
Expired activity
Please go to the PowerPak
homepage and select a course.
Relevant Changes in the Management of Advanced Renal Cell Carcinoma: Updates and Insights for Pharmacists
Overview of Renal Cell Carcinoma
Kidney cancer is the seventh most common cancer in the United States with 18,800 new cases estimated in 2023 and 14,890 deaths; 4.2% of all cancers and 2.4% of all cancer-related deaths.1 Renal cell carcinoma (RCC) comprises 85% of kidney cancers and approximately 70% are of clear cell histology. The development of RCC may be sporadic or associated with familial or hereditary syndromes.2,3 Up to 90% of sporadic RCC is associated with the loss of function of the von Hippel-Lindau (VHL) tumor suppressor gene, located on short arm of chromosome 3 (3p25) caused by an autosomal-dominant constitutional mutation in the VHL gene that predisposes to clear cell RCC and other proliferative vascular lesions. Smoking, obesity, and hypertension are additional established risk factors for RCC development.4 The incidence of RCC has been rising on average 0.6% each year but death rates have been falling on average 0.7% each year from 2006 through 2015; 5-year survival for localized RCC has increased from 88.4% (during 1992–1995) to 92.6% (during 2007–2013) and for advanced disease from 7.3% (during 1992–1995) to 11.7% (during 2007–2013).1 Several factors influence 5-year survival including the tumor stage, grade, local extent of the tumor, presence of regional nodal metastases, and evidence of metastatic disease at presentation.4
Surgery is the only curative treatment option for localized RCC, although 20% to 30% of patients who undergo a nephrectomy will relapse.4 Local recurrences are rare with most metastases occurring at distant sites. The most widely used prognostic factor model is from the Memorial Sloan Kettering Cancer Center, which has been validated by the International mRCC Database Consortium (IMDC).5,6 Prognostic factors include 5 variables: interval from diagnosis to treatment of less than 1 year; Karnofsky performance status (PS) < 80%; serum lactate dehydrogenase (LDH) > 1.5 times the upper limit of normal (ULN); corrected serum calcium greater than the ULN; and serum hemoglobin less than the lower limit of normal (LLN). Patients considered as low risk or good prognosis do not exhibit any of these factors; those with 1 or 2 factors present are considered intermediate risk; and patients with 3 or more of the factors are considered poor risk.
The treatment landscape for advanced and relapsed disease has significantly changed over the past decade regarding targeted therapies and immunotherapies. The choice of therapy is heavily affected by risk factors, PS, and previous lines of treatment.4 Targeted therapy is now widely used in first- and second-line treatments. Checkpoint inhibitors mark a new era in the treatment of advanced RCC and several agents are safe and effective in the management of RCC in the advanced or metastatic setting. These therapies mark a new landscape in the treatment of RCC.7,8
Treatment Overview for Localized RCC
Surgical excision or radical nephrectomy are effective treatment modalities in patients with localized disease (stages I–III).4 Patients with small unilateral T1a tumors or whenever preservation of renal function is a primary issue, a partial nephrectomy is an appropriate treatment; some of these tumors may require a radical nephrectomy due to location, tumor size, and surgical expertise. In contrast, active surveillance for patients with extensive comorbidities or decreased life expectancy may be an appropriate approach to avoid excessive risk for more invasive intervention. A partial or radical nephrectomy is the standard of care for T1b tumors and has demonstrated similar outcomes.4,9,10
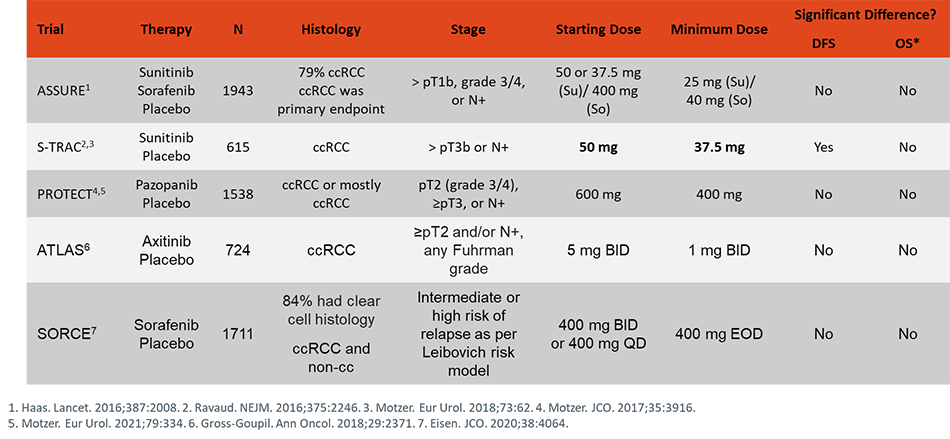
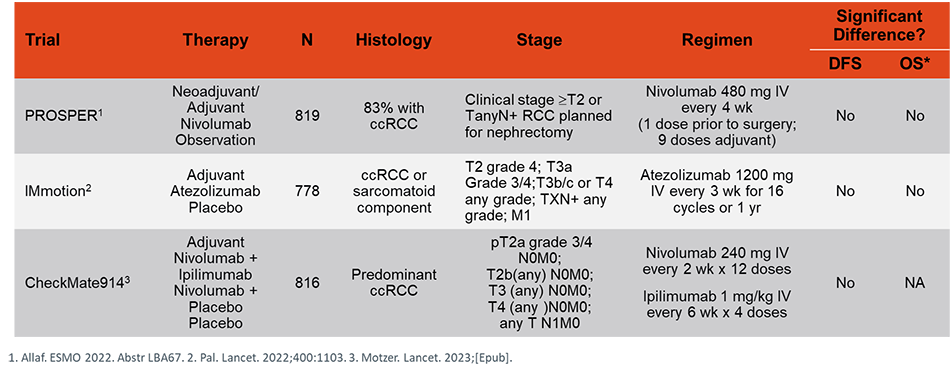
A radical nephrectomy provides a curative approach for treating locally advanced, stage II and III disease; partial nephrectomies may not resect the entirety of tumor-infiltrated tissue.4 There is no established role for adjuvant treatment following a complete nephrectomy except for patients with stage III disease, clear cell histology, and a high risk for relapse. S-TRAC, a multicenter, randomized study, evaluated 615 patients with locoregional, high-risk, clear cell cancer treated with adjuvant sunitinib (50 mg once daily; 4 weeks on, 2 weeks off) or placebo. The median duration of disease-free survival (DFS) was significantly longer in the sunitinib group than in the placebo group (6.8 years vs 5.6 years; P = .03), at a cost of a higher rate of toxic events (grade 3 or higher adverse events occurred in 63.4% of patients treated with sunitinib compared to 21.7%).11 An updated analysis demonstrated that a benefit of adjuvant sunitinib over placebo was observed across high-risk subgroups and median overall survival (OS) was not reached in either arm (hazard ratio [HR] 0.92, 95% confidence interval [CI] 0.66-1.28; P = 0.6); 67 and 74 patients died in the sunitinib and placebo arms, respectively.12 Several trials have evaluated the role of adjuvant therapy following resection using interferon alpha (IFN-α), high-dose interleukin-2 (IL-2), cytokine combinations, sunitinib or sorafenib, and pazopanib and found no benefit in DFS or improvement in OS with adjuvant therapy.13-15 Due to conflicting data, the NCCN gives adjuvant sunitinib a category 3 recommendation for patients with high risk of relapse. In KEYNOTE-564, a placebo-controlled trial, pembrolizumab demonstrated a DFS benefit in the adjuvant setting and is an FDA-approved therapeutic option for patients.16 Tables 1 and 2 highlight outcomes and ongoing clinical trials in localized RCC with targeted therapy and immunotherapy.
| Table 1. Trials of Tyrosine Kinase Inhibitors as Adjuvant Treatment in RCC |
 |
| Table 2. Trials of Immunotherapy in Nonmetastatic RCC |
 |
Treatment Overview for Advanced or Relapsed Renal Cell Carcinoma
The primary treatment modalities for advanced disease consists of systemic chemotherapy, targeted therapies, and immune checkpoint inhibition. Cytoreductive surgery before systemic therapy is recommended for resectable masses or oligometastatic sites; however, the efficacy of newer therapies is challenging this approach.4 The CARMENA phase 3 trial demonstrated that sunitinib alone was noninferior to sunitinib after nephrectomy (median OS 18.4 months vs 13.9 months, respectively [HR, 0.89; 95% CI, 0.71–1.10]), although most patients had poor risk factors that potentially confounded the results.17 Prior to the advent of tyrosine kinase inhibitors (TKIs), antivascular endothelial growth factor (VEGF) antibodies, mammalian target of rapamycin (mTOR) inhibitors, and checkpoint inhibitors, IFN-α and high-dose IL-2 were standard of care treatment options but, conversely, their use is now limited to select patients. Numerous agents are currently US Food and Drug Administration (FDA) approved for the treatment of advanced RCC as front- and subsequent-line therapies such as: sunitinib, sorafenib, pazopanib, axitinib, temsirolimus, everolimus, bevacizumab in combination with interferon, cabozantinib, and lenvatinib/everolimus.
Immune checkpoint inhibitors are the new revolution in RCC treatment options with avelumab, pembrolizumab, nivolumab, atezolizumab and ipilimumab demonstrating efficacy and safety in combination with another agent. Immune checkpoints – cytotoxic T‐lymphocyte–associated protein 4 (CTLA‐4) and programmed cell death protein and ligand 1 and 2 (PD‐1/PD‐L1/PD‐L2) – negatively regulate T‐cell immune function, and their inhibition results in increased activation of the immune system, which has revolutionized treatment options for patients with various cancer types. Cellular immunity results from tumor antigen recognition by antigen presenting cells (APCs), leading to immune activation through interactions of B7.1/B7.2 and CD28 on the cell surface of the APCs and the resting T cell.18 In contrast, CTLA‐4, often upregulated on T cells after antigen exposure, competes with CD28 with much higher affinity for binding to B7.1/B7.2, resulting in a negative signal for early T‐cell activation. Similarly, PD‐L1 binds to PD‐1, a member of the B7/CD28 family of stimulatory receptors, leading to immune inactivation mainly at tumor sites. These therapies mark a new landscape in the treatment of RCC.
Checkpoint Inhibitors for Treatment of RCC
Nivolumab
On November 23, 2015, nivolumab was granted FDA approval as the first checkpoint inhibitor for the treatment of advanced RCC in patients whose disease progressed during or after treatment with an anti-angiogenic agent.19 Nivolumab is a fully human monoclonal antibody that selectively inhibits PD‐1 activity by binding to the receptor to block the ligands PD‐L1 and PD‐L2 from binding resulting in cellular immunity against cancer cells.20 Due to limited therapeutic options at the time, the initial application for nivolumab was granted breakthrough therapy designation, fast track designation, and priority review status.
The safety and efficacy of nivolumab were established from CheckMate 025, a phase 3, randomized, open-label study, of nivolumab vs everolimus in patients with advanced RCC.21 Eligible subjects were adults aged 18 years or older with histological confirmation of advanced RCC with a clear-cell component, measurable disease define by Response Evaluation Criteria in Solid Tumors version 1.1 (RECIST v1.1), Karnofsky PS of at least 70% at the time of study entry, and who had received one or two anti-angiogenic therapies for advanced disease were eligible to participate. Patients were randomly assigned (1:1) to received nivolumab 3 mg/kg by intravenous (IV) infusion every 2 weeks (n = 406) or everolimus 10 mg orally daily (n = 397). The median OS was 25.0 months (95% CI, 21.8 to not estimable) with nivolumab and 19.6 months (95% CI, 17.6 to 23.1) with everolimus. The HR for death (from any cause) with nivolumab vs everolimus was 0.73 (98.5% CI, 0.57–0.93; P = 0.0018). The objective response rate (ORR) was also reported to be 5 times greater with nivolumab (25% vs 5%; odds ratio [OR], 5.98; 95% CI, 3.68–9.72; P < .001). The median progression-free survival (PFS) was 4.6 months (95% CI, 3.7–5.4) and 4.4 months (95% CI, 3.7–5.5) with nivolumab and everolimus, respectively (HR, 0.88; 95% CI, 0.75–1.03; P = 0.11). The study was stopped early at the planned interim analysis because the study met its primary end point, and a benefit was observed with nivolumab regardless of PD-L1 expression. Grade 3 or 4 treatment-related adverse events (TRAEs) occurred in 19% of the patients receiving nivolumab and in 37% of the patients receiving everolimus; the most common event with nivolumab was fatigue (in 3% of the patients). The most common event with everolimus was anemia (in 8% of patients).
Two follow-up analyses have been published since CheckMate 025, which were consistent and supported the use of nivolumab in advanced RCC.22,23 Cella et al demonstrated that more patients had a clinically meaningful health-related quality of life improvement with nivolumab (200 [55%] of 361 patients) vs everolimus (126 [37%] of 343 patients; P < 0·0001) with a shorter median time to improvement in patients given nivolumab (4·7 months, 95% CI 3·7–7·5) than in patients given everolimus (median not reached, NE–NE).22 Tomita et al reported that at the 3-year follow-up, the efficacy and safety results were consistent in the global and the Japanese populations.23 In the Japanese population, median OS was 45.9 months and not reached (HR 1.08; 95% CI: 0.50–2.34; P = 0.85) with nivolumab and everolimus; ORR was 43% vs 8%, respectively (OR 6.80; 95% CI: 1.60–28.91; P = 0.0035).
Nivolumab may be administered as a flat dose of 240 mg IV every 2 weeks or 480 mg IV every 4 weeks.20 Treatment is continued until disease progression or unacceptable toxicities. No dosage adjustments are required for baseline renal impairment. Baseline hepatic impairment does not require dosage adjustment, but pharmacokinetics have not been studied in patients with severe impairment. Renal impairment during treatment (serum creatinine [SCr] >1.5 to 6 × ULN) required dose interruption and initiation of steroids; SCr >6 times the ULN requires discontinuation. Patients who experience hepatic impairment during treatment, defined as an aspartate aminotransferase (AST) or alanine aminotransferase (ALT) level > 3 to 5 times the ULN or a total bilirubin level > 1.5 to 3 times the ULN, should withhold treatment and start supportive care with corticosteroids; patients with AST/ALT levels > 5 times the ULN or a total bilirubin level > 3 times the ULN should permanently discontinue therapy. There are currently no recommended dosage adjustments for patients who experience toxicities. Treatment is withheld or discontinued.
Nivolumab and Ipilimumab
On April 16, 2018, the FDA granted nivolumab a second indication in combination with ipilimumab for the treatment of intermediate or poor risk, previously untreated advanced RCC.19 Ipilimumab is a recombinant human IgG1 immunoglobulin monoclonal antibody that binds to the CTLA-4 allowing for enhanced T-cell activation and proliferation. Combining ipilimumab (anti-CTLA-4) with nivolumab (anti-PD-1) results in enhanced T-cell function that is greater than that of either antibody alone, resulting in improved antitumor responses in advanced RCC.24
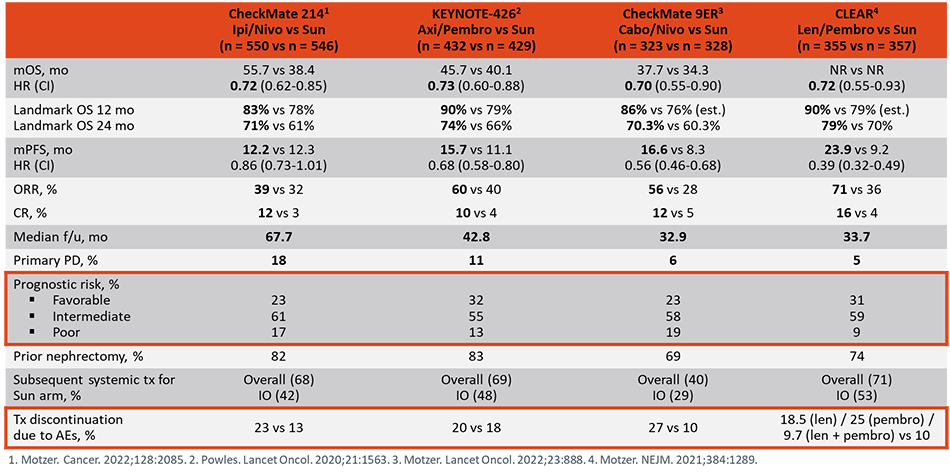
CheckMate 214, a randomized, open-label, phase 3 trial, compared nivolumab (3 mg/kg body weight) plus ipilimumab (1 mg/kg) IV every 3 weeks for 4 doses followed by nivolumab monotherapy (3 mg/kg) every 2 weeks vs sunitinib monotherapy 50 mg orally (4 weeks on and 2 weeks off schedule) in patients with advanced RCC.25 Eligible patients were 18 years or older with previously untreated advanced RCC with clear cell histology, had measurable disease defined by RECIST v1.1, and a Karnofsky PS of at least 70. A total of 1096 patients were randomized (1:1) to nivolumab plus ipilimumab or sunitinib monotherapy; 425 and 422 treated patients, respectively, had intermediate or poor-risk disease. The combination of nivolumab plus ipilimumab had a higher ORR compared to sunitinib monotherapy (42% vs 27%, P < .001), and a higher complete response rate (9% vs 1%, P < .001) in the intermediate- and poor-risk patients. The 18-month OS rate was 75% (95% CI, 70–78) with nivolumab plus ipilimumab and 60% with sunitinib (95% CI, 55–65) at a median follow-up of 25.2 months in intermediate- and poor-risk patients. The median PFS (11.6 months vs 8.4 months; HR, .82; P = .03) was not significant per the prespecified 0.009 P-value threshold. It is important to note that data are conflicting for front-line treatment with nivolumab plus ipilimumab in patients with favorable-risk disease per the exploratory analysis from Checkmate 214 demonstrating lower ORR, OS, and PFS; in contrast, the phase 1 CheckMate 016 demonstrated favorable outcomes in all patient groups.25,26 TRAEs occurred in 93% of patients in the nivolumab plus ipilimumab group and 97% in the sunitinib group; grade 3 or 4 events occurred in 250 patients (46%) and 335 patients (63%), respectively.25 TRAEs led to discontinuation in 22% and 12% of patients, respectively. Patient-reported outcomes were evaluated by Cella et al who concluded that nivolumab plus ipilimumab led to fewer symptoms and better health-related quality of life than sunitinib in patients at intermediate or poor risk with advanced RCC.27 Table 3 highlights updated date from Checkmate 214.
Dosing of the combination treatment is nivolumab 3 mg/kg and ipilimumab 1 mg/kg once every 3 weeks for 4 combination doses, followed by nivolumab (flat dose) 240 mg once every 2 weeks or 480 mg once every 4 weeks as monotherapy until disease progression or unacceptable toxicity.20,24 Toxicity management for nivolumab should be handled as mentioned previously. No dosage adjustments are required for baseline renal impairment with ipilimumab.24 Baseline hepatic impairment does not require dosage adjustment, but pharmacokinetics have not been studied in patients with moderate to severe impairment. Patients who experience grade 2 or 3 renal impairment or grade 2 hepatic impairment should have a treatment interruption and may require steroids. Grade 4 renal impairment and/or grade 3 or 4 hepatic impairment require permanent discontinuation. There are currently no recommended dosage adjustments for patients who experience toxicities. Treatment is withheld or discontinued. As both agents enhance the immune system effects, treatment interruption and delays are often simultaneous for both agents. The NCCN panel gives the combination nivolumab plus ipilimumab a category 1, preferred treatment option recommendation for first-line treatment of intermediate- and poor-risk patients with previously untreated, relapsed or medically unresectable, clear cell, stage IV RCC; category 2A, other recommended option in patients with favorable-risk disease.4
Pembrolizumab and Axitinib
On April 19, 2019, the FDA approved pembrolizumab plus axitinib for the first-line treatment of patients with advanced RCC.19 Pembrolizumab is a highly selective anti-PD-1 humanized monoclonal antibody that inhibits PD-1 activity by binding to the PD-1 receptor on T cells to block PD-L1 and PD-L2 from binding inhibiting the negative immune regulation caused by PD-1 receptor signaling and inducing antitumor responses.28 Axitinib is an oral, selective second-generation TKI that blocks angiogenesis and tumor growth by inhibiting VEGFR-1, VEGFR-2, and VEGFR-3.29 As monotherapy, axitinib is FDA-approved and given an NCCN category 1 recommendation for the treatment of advance RCC following one prior therapy as it has demonstrated greater ORR and longer median PFS compared with those treated with sorafenib.4,19,30,31 The difference in PFS between patients treated with axitinib vs sorafenib in the front-line setting is not statistically significant and, thus, it is a category 2B recommendation for use under certain circumstances.4,32 The rationale from combined checkpoint inhibition with anti-VEGF therapy is thought to have complementary mechanisms from the immunomodulatory effects with anti-VEGF therapies, including enhanced tumor infiltration of immune cells and reduced immunosuppressive effects of myeloid-derived suppressor cells.33
Keynote 426 was an open-label, phase 3 trial that randomly assigned patients in a 1:1 ratio to receive pembrolizumab 200 mg IV every 3 weeks plus axitinib 5 mg orally twice daily or sunitinib 50 mg orally daily for the first 4 weeks of each 6-week cycle.34 The dose of axitinib could be increased to 7 mg, then 10 mg (twice daily if safety criteria were met) and reduced to 3 mg, then 2 mg (twice daily to manage toxic effects); the sunitinib dose could be reduced to 37.5 mg, then 25 mg, for the first 4 weeks of each 6-week cycle to manage toxic effects. Eligible patients were 18 years or older, had newly diagnosed or recurrent stage IV clear cell RCC, had received no previous systemic therapy for advanced disease, had a Karnofsky PS score of 70 or more, had at least one measurable lesion as evaluated according to RECIST v1.1, and had an available tumor sample for biomarker assessment. The main efficacy measures were OS and PFS by blinded independent central review. The trial demonstrated a statistically significant improvement in OS in a prespecified interim analysis for patients on the pembrolizumab plus axitinib arm (HR 0.53; 95% CI: 0.38, 0.74; P < 0.0001). With deaths reported in 18% of patients, the median OS was not reached in either arm. The 12-month OS rate was 90% in the pembrolizumab plus axitinib arm and 78% for those treated with sunitinib. Median PFS was 15.1 and 11.1 months for those receiving pembrolizumab plus axitinib vs sunitinib (HR 0.69; 95% CI: 0.57–0.84; P = 0.0001), respectively. The ORR was 59.3% (95% CI, 54.5–63.9) in the pembrolizumab plus axitinib group and 35.7% (95% CI, 31.1–40.4) in the sunitinib group (P < 0.001). The benefit of pembrolizumab plus axitinib was observed across favorable, intermediate, and poor risk groups and regardless of PD-L1 expression. The most common adverse reactions in > 20% of patients who received pembrolizumab plus axitinib were diarrhea, fatigue/asthenia, hypertension, hypothyroidism, decreased appetite, hepatotoxicity, palmar-plantar erythrodysesthesia, nausea, stomatitis/mucosal inflammation, dysphonia, rash, cough, and constipation. Grade ≥ 3 adverse events of any cause occurred in 75.8% of patients in the pembrolizumab–axitinib group and in 70.6% in the sunitinib group. Grade ≥ 3 hepatotoxicity occurred in 20% of patients and resulted in permanent discontinuation of pembrolizumab or axitinib in 13% of patients.
Pembrolizumab is administered as a flat dose of 200 mg IV every 3 weeks (or 400 mg every 6 weeks) with axitinib 5 mg orally twice daily.28,29 Treatment is continued until disease progression or unacceptable toxicities. No dosage adjustments are required for baseline renal impairment. Baseline hepatic impairment does not require dosage adjustment, but pharmacokinetics have not been studied in patients with moderate to severe impairment. Patients who experience grade 2 renal impairment should have a treatment interruption and may require steroids. Grade 3 or 4 renal impairment requires discontinuation. Patients who experience hepatic impairment during treatment, defined as an AST or ALT level > 3 to 5 times the ULN but less than 10 times ULN without concurrent total bilirubin at least 2 times ULN, should withhold treatment and start supportive care with corticosteroids; patients with AST/ALT levels > 5 times the ULN or a total bilirubin level > 3 times the ULN with concurrent total bilirubin at least 2 times ULN or ALT or AST at least 10 times ULN, should permanently discontinue therapy. There are currently no recommended dosage adjustments for patients who experience toxicities. Pembrolizumab plus axitinib, as a front-line option, is a category 1 for patients with favorable risk disease and for intermediate/poor risk.4 It is also a 2A recommendation as a subsequent treatment option for those who are immunotherapy naïve.
Avelumab and Axitinib
On May 14, 2019, the FDA approved avelumab in combination with axitinib for first-line treatment of patients with advanced RCC.19 Avelumab is a fully human monoclonal antibody that binds to PD-L1 to selectively prevent the interaction between the PD-1 and B7.1 receptors.35
JAVELIN Renal 101, a randomized, multicenter, open-label trial, evaluated the role of avelumab plus axitinib in 886 patients with untreated advanced RCC regardless of tumor PD-L1 expression.36 Eligible patients were 18 years or older, had previously untreated advanced RCC with a clear cell component, had at least 1 measurable lesion according to the RECIST v1.1, Eastern Cooperative Oncology Group PS score of 0 or 1, a fresh or archival tumor specimen, and adequate renal, cardiac, and hepatic function. Patients were randomized to receive either avelumab 10 mg/kg IV every 2 weeks plus axitinib 5 mg orally twice daily or sunitinib 50 mg orally once daily for 4 weeks followed by 2 weeks off until disease progression or unacceptable toxicity. Dose escalations and reductions of axitinib and dose reductions of sunitinib were permitted, but no dose adjustments were permitted for avelumab. The main efficacy end points were PFS assessed by blinded independent central review and OS in patients with PD-L1 positive tumors. Of the 560 patients with PD-L1 positive tumors (63.2%), the median PFS was 13.8 months with avelumab plus axitinib and 7.2 months with sunitinib (HR, 0.61; 95% CI, 0.47–0.79; P < 0.001). In the overall population, the median PFS was 13.8 months and 8.4 months, respectively (HR, 0.69; 95% CI, 0.56–0.84; P < 0.001). At 19 months, the median OS data were immature with 27% deaths in the intent-to-treat (ITT) population. Adverse events during treatment occurred in 99.5%, and 99.3% of patients in the avelumab plus axitinib group and sunitinib group, respectively; grade ≥ 3 was observed in 71.2% and 71.5% of the patients.
The recommended dose of avelumab is a flat 800 mg IV every 2 weeks with axitinib 5 mg orally twice daily.29,35 Patient should receive premedications with an antihistamine and acetaminophen prior to the first 4 infusions; consideration of premedication for subsequent infusions should be based on clinical judgment and the presence or severity of infusion-related reactions with previous infusions. There are no dosage adjustments for baseline renal and hepatic impairment, and no clinically relevant pharmacokinetic differences were observed in patients with a creatinine clearance of 15–89 mL/minute, bilirubin level ≤ ULN and AST level > ULN, or bilirubin level 1–1.5 times the ULN, or bilirubin level 1.5–3 times the ULN. Patients who experience renal or hepatic toxicity, defined as a serum SCr > 1.5 to 6 times ULN, or AST/ALT level > 3 to 5 times the ULN or a total bilirubin level > 1.5 to 3 times the ULN, while receiving therapy should withhold treatment and start corticosteroids until recovered to grade 0 or 1. Therapy should be discontinued if patients experience any of the following while receiving treatment: SCr > 6 times the ULN, AST or ALT level > 5 times the ULN, or total bilirubin level > 3 times the ULN. At the time of this publication, this treatment combination was not yet incorporated in the NCCN guidelines (v1.2024) but a discussion update was in progress.4
Atezolizumab and Bevacizumab
Another notable treatment combination is atezolizumab plus bevacizumab as a treatment option for patients with untreated, advanced clear cell RCC. This treatment combination is not FDA-approved and has not been incorporated in the NCCN guidelines at the time of this publication. The emergence of the phase 3 trial resulted from the phase 2 trial that demonstrated improved PFS with atezolizumab plus bevacizumab vs sunitinib in patients with metastatic RCC who express PD-L1.37 Atezolizumab is a humanized monoclonal antibody immune checkpoint inhibitor that binds to PD-L1 to selectively prevent the interaction between the PD-1 and B7.1 receptors, while still allowing interaction between PD-L2 and PD-1 restoring antitumor t-cell function.38 Bevacizumab is a recombinant, humanized monoclonal antibody that binds to, and neutralizes, VEGF, preventing its association with endothelial receptors retarding the growth of all tissues.39
IMmotion 151, a randomized, multicenter, open-label, phase 3 controlled trial assigned (1:1) patients to receive atezolizumab 1200 mg IV plus bevacizumab 15 mg/kg IV once every 3 weeks vs sunitinib 50 mg orally once daily for 4 weeks, followed by 2 weeks off.40 Eligible patients were aged 18 years or older with unresectable locally advanced or metastatic RCC with any component of clear cell or sarcomatoid histology, measurable disease according to RECIST v1.1, Karnofsky PS 70% or higher, adequate hematological and end-organ function, and tumor tissue available for PD-L1 testing. Median follow-up was 15 months at the primary progression-free survival analysis and 24 months at the OS interim analysis. In the PD-L1 positive population, the median PFS was 11.2 months in the atezolizumab plus bevacizumab group vs 7.7 months in the sunitinib group (HR, 0.74, 95% CI, 0.57–0.96, P = 0.0217). In the ITT population, median OS did not cross the significance boundary at the interim analysis (HR, 0.93, 0.76–1.14). Grade ≥ 3 TRAEs were observed in 40% and 54 % in the atezolizumab plus bevacizumab group and sunitinib group, respectively. All grade TRAEs leading to discontinuation were observed in 5% in the atezolizumab plus bevacizumab group and 8% in the sunitinib group.
Atezolizumab is approved in other indications and administered as a flat dose of 1200 mg IV every 3 weeks.38 Treatment is continued until disease progression or unacceptable toxicities. No dosage adjustments are required for renal impairment; however, it is important to note that pharmacokinetics have not been studied in patients with a glomerular filtration rate (GFR) < 29 mL/minute. Baseline hepatic impairment does not require dosage adjustment, but pharmacokinetics has not been studied in patients with severe impairment. Patients who experience hepatic impairment during treatment, defined as an AST or ALT level > 3 to 5 times the ULN or a total bilirubin level > 1.5 to 3 times the ULN, should withhold treatment and start supportive care with corticosteroids; patients with AST/ALT levels > 5 times the ULN or a total bilirubin level > 3 times the ULN should permanently discontinue therapy. There are currently no recommended dosage adjustments for patients who experience toxicities. Treatment is withheld or discontinued.
Cabozantinib and Nivolumab
On January 22, 2021, the FDA approved the combination of nivolumab and cabozantinib as first-line treatment for patients with advanced RCC.19
Efficacy was evaluated in CHECKMATE-9ER, a randomized, open-label trial in patients with previously untreated advanced RCC.41 Patients were randomized to receive either nivolumab 240 mg over 30 minutes every 2 weeks in combination with cabozantinib 40 mg orally once daily (n = 323) or sunitinib 50 mg orally daily for the first 4 weeks of a 6-week cycle (4 weeks on treatment followed by 2 weeks off [n = 328]).
The trial demonstrated a statistically significant improvement in PFS, OS, and confirmed ORR for patients treated with nivolumab plus cabozantinib compared with those who received sunitinib. Median PFS per blinded independent central review (BICR) was 16.6 months vs 8.3 months; HR 0.51 (95% CI: 0.41, 0.64; P = 0.001). Median OS was not reached in either arm; HR 0.60 (95% CI: 0.40, 0.89). Confirmed ORR per BICR was 55.7% and 27.1% in the nivolumab plus cabozantinib and sunitinib arms, respectively.
The most common adverse reactions (≥ 20%) in patients receiving the combination of nivolumab and cabozantinib were diarrhea, fatigue, hepatotoxicity, palmar-plantar erythrodysaesthesia syndrome, stomatitis, rash, hypertension, hypothyroidism, musculoskeletal pain, decreased appetite, nausea, dysgeusia, abdominal pain, cough, and upper respiratory tract infection.
The recommended dose is nivolumab 240 mg every 2 weeks (or 480 mg every 4 weeks) in combination with cabozantinib 40 mg orally once daily without food until disease progression or unacceptable toxicity.
| Table 3. Frontline IO/VEG-F Combination Trials |
 |
Choice of Therapy
The speed with which the immuno-oncology market is evolving is at unprecedented rates, with new data and/or approvals being announced often. The lack of market maturity may create challenges to making an access decision today (ie, preferring one product over another). The treatment for advanced RCC has significantly changed with the advent of TKIs, anti-VEGF antibodies, and mTOR inhibitors, and immunotherapies have provided new therapeutic modalities.
It is evident that checkpoint blockade has demonstrated effective management for patients with RCC. Treatment selection utilizing immune checkpoint inhibitors for patients with advanced disease should put into consideration disease-specific risk factors, patient comorbidities, patient preference of a completely oral regimen vs infusion, prior lines of therapy, and any underlying autoimmune diseases. At times, the choice of therapy becomes challenging for providers, as survival benefit, long-term analysis, budget impact, adverse event cost, and sequencing studies are all limited.
Several ongoing clinical trials are aimed at further defining the role of immunotherapy, combination chemo-immunotherapy, and combination target therapy with immunotherapy.
Pharmacist Considerations in Patient Management
As a class, the spectrum of adverse effects associated with immune checkpoint inhibitors is very different than other systemic anticancer agents. Immune-related adverse events (irAEs) commonly affect skin, GI tract, and lungs, as well as endocrine, thyroid, adrenal, pituitary, musculoskeletal, renal, nervous, hematologic, cardiovascular, and ocular systems.42,43 Due to the unpredictable nature of irAEs, there should be a high level of suspicion that any changes in the patient's symptoms or quality of life are treatment-related.
A major practical difference in AEs associated with chemotherapy vs those associated with immunotherapy is that traditional cytotoxic chemotherapy often results in acute-onset emetic and myelosuppressive effects, while irAEs tend to be relatively delayed-onset and inflammatory or autoimmune in nature. Accordingly, close follow up of patients and timely management is critical to minimize morbidity. In each case, the health care provider is charged with determining answers to a set of basic clinical decisions including: (1) assessing whether it is autoimmune etiology or another cause; (2) whether to hold or continue treatment; (3) the timing of steroid initiation; (4) the starting dose of steroid and duration of treatment; (5) the route of administration of steroids (oral vs IV); (6) whether it can be handled as an inpatient vs outpatient; and (7) when to initiate second-line immunosuppressive therapy.44
| Figure 2. Onset of Immune Checkpoint Inhibitor-Associated Toxicities |
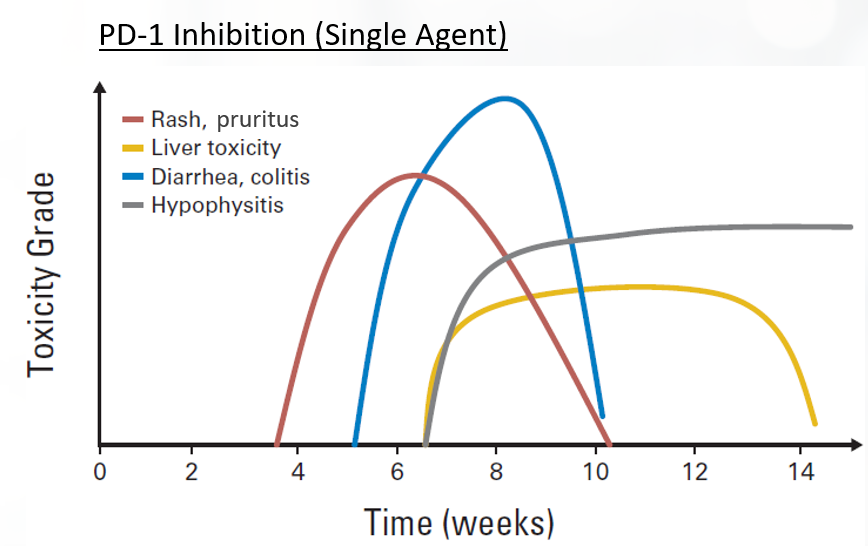 |
irAEs are typically inflammatory or autoimmune in nature.45-47 There is a trend toward higher incidence of irAEs when these agents are used in combination therapy (ie, dual immune checkpoint inhibitor or with targeted chemotherapies).42,45 Toxicities affect all organ systems, including the GI tract (colitis, diarrhea), lung (pneumonitis), endocrine system (hypophysitis, thyroiditis), liver (hepatitis), and skin (rash, pruritus), among others. irAEs do not necessarily appear concurrently. For instance, skin and GI events usually appear within 1 to 2 cycles of dual blockade, while hepatitis, pneumonitis, and endocrine side effects appear later.
There is concern that the administration of immune-activating agents may exacerbate pre-existing autoimmune disease.42 Data on the toxicity of immune checkpoint inhibitors in patients with preexisting autoimmune disease or prior irAEs is generally lacking due to exclusion of these populations from the registry clinical trials leading to FDA approval. However, based on limited data from smaller retrospective studies, immune checkpoint inhibitors appear to have a similar efficacy in these patient groups, as in the general population. A retrospective records analysis of patients with NSCLC and a history of an autoimmune disorder (AID) found that checkpoint inhibitor therapy did not significantly aggravate the AID for most patients and that irAE rates were like those reported in clinical trials that excluded AIDs.48
It is important to note that shared adverse events may present between IO therapy and VEG-F-targeted therapies. These may include transaminase elevation, endocrinopathies, GI side effects, and skin toxicities. It is important for clinicians to be aware of this in the management strategy of the adverse event.
Close consultation with disease-specific subspecialists is encouraged during irAE management.42 Routine premedication with corticosteroids is not recommended.
- Infusion-related reactions (IRRs) are uncommon and mild. IRRs are associated with low-grade fever, chills, headache, or nausea. Mild IRRs do not require infusion interruption or other interventions. For moderate IRRs, the infusion rate should be slowed or held, and antihistamines, acetaminophen, NSAIDS, narcotics, or IV fluids may be required. Severe IRRs are often more prolonged with limited responsiveness to intervention or infusion interruption and can recur following initial improvement
- Dermatological toxicities are the most common irAE and typically present within the first 2 cycles of therapy. Maculopapular rash, pruritus, vitiligo, alopecia, hair repigmentation, and eczematous, lichenoid, psoriasiform, and bullous dermatitis have been observed. The reported incidences of all-grade dermatologic toxicity range from 37% to 70% for ipilimumab and 17% to 40% for PD-1/PD-L1 inhibitors, with a similar 1% to 3% of patients experiencing high-grade dermatological toxicity across all immune checkpoint inhibitors. In general, short-term use of higher potency topical corticosteroids is preferred over longer-term use of a lower-potency agent
- Gastrointestinal toxicity may present as diarrhea or colitis, typically 6 to 8 weeks after therapy initiation. The incidence is highest in patients receiving dual nivolumab/ipilimumab therapy, high in patients receiving anti-CTLA-4 therapy, and least common in patients receiving anti-PD-L1 and anti-PD-1 therapies (13.6%, 9.1%, 1.3%, respectively). Corticosteroids will resolve GI toxicity in 40% to 60% of patients
- Hepatic toxicity is rare and typically mild, but it can be fatal. The incidence is estimated at 3% to 9% for ipilimumab and 0.7% to 1.8% for anti-PD-L1 and anti-PD-1 therapies. Autoimmune hepatitis and drug-induced hepatitis can be difficult to distinguish but may be differentiated by distinct histologic features and imaging
- Pancreatic toxicity is common and associated with elevated amylase and/or lipase levels, but it does not typically require intervention. Acute pancreatitis is rare and treated with standard medical care, including hospital admission, aggressive fluid resuscitation, and pain control. Gastroenterology consultation and immunosuppression are warranted if clinical assessment and/or imaging findings support moderate to severe acute pancreatitis
- Endocrine dysfunction typically involves the thyroid, pituitary, adrenal glands, and pancreas and is associated with hypothyroidism, hyperthyroidism, hypophysitis, type 1 diabetes, and primary adrenal insufficiency. Endocrine toxicity is very challenging to distinguish from other treatment- and disease-related causes. Median time to onset of moderate to severe endocrinopathy has ranged from 1.75 months to 5 months for ipilimumab and 1.4 months to 4.9 months with PD-1 inhibitor monotherapy. Life-long hormone replacement therapy may be required for some patients
- Pneumonitis is rare (<5% all-grade, ≥1% high-grade) but may be fatal. The median time to irAE onset has been reported at 2.5 months (earlier for combination vs monotherapy)
- Nervous system toxicity is moderately common (3.8% for CTLA-4 inhibitors, 6% with PD-1 inhibitors, and 12% for combination therapy) and may be fatal, despite aggressive treatment. Neurologic irAEs include numerous conditions such as myasthenia gravis, Guillain-Barré Syndrome (GBS)-like syndrome, central and/or peripheral neuropathy, aseptic meningitis, encephalitis, and transverse myelitis. Fatalities were more commonly associated with encephalitis and myasthenia gravis. Prompt treatment is critical for reducing long-term morbidity and mortality. Resolution is typically <8 weeks with treatment
- Cardiovascular toxicities, including myocarditis, cardiomyopathy, cardiac fibrosis, heart failure, and cardiac arrest, are uncommon but may be fatal. Prevalence has been estimated to be 1.1% (but may be underestimated), with a median onset of 34 days from initiation of treatment. Patients with suspected cardiotoxicity should have a full cardiac work up and receive corticosteroids until cardiac function returns to normal, with a 4- to 6-week taper.
- Musculoskeletal toxicities include inflammatory arthritis, myositis, and myalgias. Myositis can be fatal and is more commonly observed in patients receiving anti-PD-1/PD-L1 therapy than anti-CTLA-4 therapy. The incidence is up to 7%.
The NCCN, American Society of Clinical Oncology (ASCO), and European Society for Medical Oncology (ESMO released a clinical practice guideline for the management of irAEs in patients treated with immune checkpoint inhibitor therapy.42,43,49 These organizations recognized the need for greater awareness and guidance on the management of irAEs. They have provided grading and management. The recommendations include:
- Patient and family caregivers should receive education about immunotherapies and irAEs prior to initiating therapy and throughout treatment and survivorship
- There should be a high level of suspicion that new symptoms are treatment related
- In general, therapy should be continued with close monitoring for grade 1 toxicities, with the exception of some neurologic, hematologic, and cardiac toxicities
- Hold treatment for most grade 2 toxicities; resume when symptoms revert to grade 1 or less. Corticosteroids may be administered
- Hold for grade 3 toxicities and initiate high-dose corticosteroids. Taper corticosteroids over 4 to 6 weeks. Infliximab (anti-TNFα) may be offered if symptoms do not improve in 2 to 3 days. Use caution when resuming after resolution of symptoms to grade ≤1; do not adjust dose
- Permanent discontinuation for grade 4 toxicities, except for select endocrinopathies (ie, hypothyroidism controlled with levothyroxine supplementation).
| Table 4. Management of Immune-Related Toxicities Associated With Checkpoint Inhibitors50 |
|
irAE
|
ICI Therapy
|
Immunosuppressants
|
Other Treatment
|
| Grade 1 |
Discontinue if hypophysitis, pneumonitis, and/or sarcoidosis;
consider holding if renal;
hold if neurologic, aplastic anemia, acquired hemophilia; continue for all others |
Prednisone 0.5-1 mg/kg/d if acquired hemophilia |
Topical steroids a, oral antihistamines b, topical emollients if dermatologic |
| Loperamide if gastrointestinal c |
| Thyroid hormone supplementation d if hypothyroidism |
| Beta-blockers for symptomatic hyperthyroidism e; insulin therapy if hyperglycemia |
| Oral fluids, loperamide, hormone replacement therapy f if hypophysitis |
| Consider artificial tears if ocular |
| Analgesics g if rheumatologic |
| Grade 2 |
Considering holding if dermatologic, rheumatologic, or lymphopenia; hold for all others. |
Prednisone 0.5-1 mg/kg/d h
Prednisone 1-2 mg/kg/d if hypophysitis i
Prednisone 2 mg/kg/d if transverse myelitis k
|
In addition to the above, consider: adding infliximab if gastrointestinal j |
| Empiric antibiotics if pulmonary |
| Prednisone 2 mg/kg/d if transverse myelitis k |
| Adding ATG and cyclosporine if aplastic anemia |
| Adding GABA agonistl or duloxetine for pain if peripheral neuropathy; adding ophthalmic prednisone if ocular |
| Grade 3 |
Discontinue if hepatitis, renal, ocular, neurologic, cardiovascular, rheumatologic, and/or hematologic; hold for all others |
Prednisone 1-2 mg/kg/d; prednisone 2-4 mg/kg/d if peripheral neuropathy or GBS; consider plasmapheresis, intravenous immunoglobulin therapy, methotrexate, azathioprine, or mycophenolate mofetil through grade 4 if myositis; consider methotrexate or tocilizumab through grade 4 if steroid refractory; consider rituximab or cyclophosphamide if acquired hemophilia |
In addition to the above, consider:
adding omalizumab, GABA agonist l if pruritis;
plasmapheresis or immunoglobulin if neurologic;
pyridostigmine m if myasthenia gravis;
antirheumatic drugsn, methotrexate, infliximab or tocilizumab if refractory arthritis or polymyalgia-like syndrome;
infliximab, mycophenolate mofetil, intravenous immunoglobulin if pulmonary or renal;
rituximab if autoimmune; encephalopathy
infliximab if cardiovascular o
|
| Grade 4 |
Discontinue |
Prednisone 2-4 mg/kg/d |
In addition to the above, consider adding mycophenolate mofetil if hepatitis; empiric antivirals if aseptic meningitis and/or encephalitis; rituximab if acquired TTP;
rituximab or cyclophosphamide if acquired hemophilia;
rituximab, intravenous immunoglobulin, cyclosporine A, or mycophenolate mofetil if autoimmune hemolytic anemia; eculizaumab if hemolytic uremic syndrome;
intravenous immunoglobulin, rituximab, or thrombopoietin receptor agonists if immune thrombocytopenia
|
Update: December 18, 2023 |
- New drug approvals or black box warnings
- On December 14, 2023, the FDA granted approval for belzutifan for patients with advanced renal cell carcinoma following programmed cell death receptor-1 (PD-1) or programmed cell death-ligand 1 (PD-L1) inhibitor and a vascular endothelial growth factor tyrosine kinase inhibitor (VEGF-TKI). Belzutifan is an inhibitor of hypoxia-inducible factor 2 alpha.
- New safety labeling changes
- On September 6, 2023, warnings and precautions were updated to describe immune-mediated pneumonitis, colitis, hepatitis, endocrinopathies, diabetes, nephritis, dermatologic reactions of avelumab and infusion-related reactions.
- New clinical trial data
- On November 14, 2023, the 43-month follow-up results of the KEYNOTE-426 trial were published in the European Urology. In this study, advanced clear cell renal carcinoma patients were randomized to receive pembrolizumab 200 mg IV q 3 weeks + axitinib 5 mg po BID or sunitinib 50 mg po once daily x 4 weeks of a 6-week cycle
- Benefit of overall survival and PFS were maintained (hazard ratio [HR] 0.73, 95% confidence interval [CI], 0.60-0.88) and (HR, 0.68, 95% CI, 0.58-0.80)
- ORR was 60% vs 40%
- Median duration of response, 24 months (1.4+ to43+) vs 15 months (2.3-43+)
- No new safety signals
|
References
- Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17-48. doi: 10.3322/caac.21763
- Dutcher JP. Recent developments in the treatment of renal cell carcinoma. Ther Adv Urol. 2013;5(6):338-353. doi: 10.1177/1756287213505672
- Pecuchet N, Fournier LS, Oudard S. New insights into the management of renal cell cancer. Oncology. 2013;84(1):22-31. doi: 10.1159/000342962
- NCCN. The NCCN Clinical Practical Guidelines in Oncology Kidney Cancer (Version 1.2024). 2023. www.NCCN.org. https://www.nccn.org/professionals/physician_gls/pdf/kidney.pdf.
- Motzer RJ, Bacik J, Murphy BA, et al. Interferon-alfa as a comparative treatment for clinical trials of new therapies against advanced renal cell carcinoma. J Clin Oncol. 2002;20:289-296. doi: 10.1200/JCO.2002.20.1.289
- Mekhail TM, Abou-Jawde RM, Boumerhi G, et al. Validation and extension of the Memorial Sloan-Kettering prognostic factors model for survival in patients with previously untreated metastatic renal cell carcinoma. J Clin Oncol. 2005;23:832-841. doi: 10.1200/JCO.2005.05.179
- Hanna KS. A review of immune checkpoint inhibitors for the management of locally advanced or metastatic urothelial carcinoma. Pharmacotherapy. 2017;37(11):1391-1405. doi: 10.1002/phar.2033
- Hanna KS. Updates and novel treatments in urothelial carcinoma. J Oncol Pharm Pract. 2019;25(3):648-656. doi: 10.1177/1078155218805141
- Simmons MN, Weight CJ, Gill IS. Laparoscopic radical versus partial nephrectomy for tumors >4 cm: intermediate-term oncologic and functional outcomes. Urology. 2009;73:1077-1082. doi: 10.1016/j.urology.2008.11.059
- Peycelon M, Hupertan V, Comperat E, et al. Long-term outcomes after nephron sparing surgery for renal cell carcinoma larger than 4 cm. J Urol. 2009;181:35-41. doi: 10.1016/j.juro.2008.09.025
- Ravaud A, Motzer RJ, Pandha HS, et al. Adjuvant sunitinib in high-risk renal-cell carcinoma after nephrectomy. N Engl J Med. 2016;375:2246-2254. doi: 10.1056/NEJMoa1611406
- Motzer RJ, Ravaud A, Patard JJ, et al. Adjuvant sunitinib for high-risk renal cell carcinoma after nephrectomy: subgroup analyses and updated overall survival results. Eur Urol. 2018;73:62-68. doi: 10.1016/j.eururo.2017.09.008
- Smaldone MC, Fung C, Uzzo RG, Haas NB. Adjuvant and neoadjuvant therapies in high-risk renal cell carcinoma. Hematol Oncol Clin North Am. 2011;25:765-791. doi: 10.1016/j.hoc.2011.06.002
- Haas NB, Manola J, Uzzo RG, et al. Adjuvant sunitinib or sorafenib for high-risk, non-metastatic renal-cell carcinoma (ECOG-ACRIN E2805): a double-blind, placebo-controlled, randomised, phase 3 trial. Lancet. 2016;387:2008-2016. doi: 10.1016/S0140-6736(16)00559-6
- Motzer RJ, Haas NB, Donskov F, et al. Randomized phase III trial of adjuvant pazopanib versus placebo after nephrectomy in patients with localized or locally advanced renal cell carcinoma. J Clin Oncol. 2017;35:3916-3923. doi: 10.1200/JCO.2017.73.5324
- Powles T, Tomczak P, Park SH, et al. Pembrolizumab versus placebo as post-nephrectomy adjuvant therapy for clear cell renal cell carcinoma (KEYNOTE-564): 30-month follow-up analysis of a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2022;23(9):1133-1144. doi: 10.1016/S1470-2045(22)00487-9
- Mejean A, Ravaud A, Thezenas S, et al. Sunitinib alone or after nephrectomy in metastatic renal-cell carcinoma. N Engl J Med. 2018;379:417-427. doi: 10.1056/NEJMoa1803675
- Keir ME, Butte MJ, Freeman GJ, et al. PD‐1 and its ligands in tolerance and immunity. Annu Rev Immunol. 2008;26:677-704. doi: 10.1146/annurev.immunol.26.021607.090331
- FDA. Hematology/Oncology (Cancer) Approvals & Safety Notifications; 2023. www.fda.gov. Accessed August 28, 2023. https://www.fda.gov/drugs/informationondrugs/approveddrugs/ucm279174.htm.
- Opdivo (nivolumab). Prescribing information. Bristol‐Myers Squibb; 2023.
- Motzer RJ, Escudier B, Mcdermott DF, et al. Nivolumab versus everolimus in advanced renal-cell carcinoma. N Engl J Med. 2015;373(19):1803-1813. doi: 10.1056/NEJMoa1510665
- Cella D, Grünwald V, Nathan P, et al. Quality of life in patients with advanced renal cell carcinoma given nivolumab versus everolimus in CheckMate 025: a randomised, open-label, phase 3 trial. Lancet Oncol. 2016;17(7):994-1003. doi: 10.1016/S1470-2045(16)30125-5
- Tomita Y, Fukasawa S, Shinohara N, et al. Nivolumab versus everolimus in advanced renal cell carcinoma: Japanese subgroup 3-year follow-up analysis from the Phase III CheckMate 025 study. JpnJ Clin Oncol. 2019;49(6):506-514. doi: 10.1093/jjco/hyz026.
- Yervoy (ipilimumab). Prescribing information. Bristol‐Myers Squibb; 2023.
- Motzer RJ, Tannir NM, McDermott DF, et al. Nivolumab plus ipilimumab versus sunitinib in advanced renal-cell carcinoma. N Engl J Med. 2018;378:1277-1290. doi: 10.1056/NEJMoa1712126
- Hammers HJ, Plimack ER, Infante JR, et al. Safety and efficacy of nivolumab in combination with ipilimumab in metastatic renal cell carcinoma: the CheckMate 016 study. J Clin Oncol. 2017;35:3851-3858. doi: 10.1200/JCO.2016.72.1985
- Cella D, Grünwald V, Escudier B, et al. Patient-reported outcomes of patients with advanced renal cell carcinoma treated with nivolumab plus ipilimumab versus sunitinib (CheckMate 214): a randomised, phase 3 trial. Lancet Oncol. 2019;20(2):297-310. doi: 10.1016/S1470-2045(18)30778-2
- Keytruda (pembrolizumab). Prescribing information. Merck & Co Inc; 2022.
- Inlyta (axitinib). Prescribing information. Pfizer Inc; 2018.
- Rini BI, Escudier B, Tomczak P, et al. Comparative effectiveness of axitinib versus sorafenib in advanced renal cell carcinoma (AXIS): a randomised phase 3 trial. Lancet. 2011;378:1931-1939. doi: 10.1016/S0140-6736(11)61613-9
- Motzer RJ, Escudier B, Tomczak P, et al. Axitinib versus sorafenib as second-line treatment for advanced renal cell carcinoma: overall survival analysis and updated results from a randomised phase 3 trial. Lancet Oncol. 2013;14:552-562. doi: 10.1016/S1470-2045(13)70093-7
- Hutson TE, Lesovoy V, Al-Shukri S, et al. Axitinib versus sorafenib as first-line therapy in patients with metastatic renal-cell carcinoma: a randomised open-label phase 3 trial. Lancet Oncol. 2013;14:1287-1294. doi: 10.1016/S1470-2045(13)70465-0
- Roland CL, Lynn KD, Toombs JE, Dineen SP, Udugamasooriya DG, Brekken RA. Cytokine levels correlate with immune cell infiltration after anti-VEGF therapy in preclinical mouse models of breast cancer. PLoS One. 2009;4(11):e7669. doi: 10.1371/journal.pone.0007669
- Rini BI, Plimack ER, Stus V, et al. Pembrolizumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2019;380(12):1116-1127. doi: 10.1056/NEJMoa1816714
- Bavencio (avelumab). Prescribing information. EMD Serono Inc; 2019.
- Motzer RJ, Penkov K, Haanen J, et al. Avelumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med, 2019;380(12):1103-1115. doi: 10.1056/NEJMoa1816047
- McDermott DF, Huseni MA, Atkins MB, et al. Clinical activity and molecular correlates of response to atezolizumab alone or in combination with bevacizumab versus sunitinib in renal cell carcinoma. Nat Med. 2018;24(6):749-757. doi: 10.1038/s41591-018-0053-3
- Tecentriq (atezolizumab). Prescribing information. Genentech, Inc; 2019.
- Avastin (bevacizumab). Prescribing information. Genentech, Inc; 2023.
- Rini BI, Powles T, Atkins MB, et al. Atezolizumab plus bevacizumab versus sunitinib in patients with previously untreated metastatic renal cell carcinoma (IMmotion151): a multicentre, open-label, phase 3, randomised controlled trial. Lancet. 2019. doi: 10.1016/S0140-6736(19)30723-8
- Choueiri TK, Powles T, Burotto M, et al. Nivolumab plus cabozantinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2021;384(9):829-841. doi: 10.1056/NEJMoa2026982
- National Comprehensive Cancer Network. NCCN Guidelines Version 2.2023, Management of Immunotherapy-Related Toxicities. https://www.nccn.org/professionals/physician_gls/pdf/immunotherapy.pdf.
- Brahmer JR, Lacchetti C, Schneider BJ, et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: American Society of Clinical Oncology Clinical Practice Guideline. J Clin Oncol. 2018;36(17):1714-1768. doi: 10.1200/JCO.2017.77.6385
- Sznol M. Immunotherapy for melanoma: management of adverse events. Personal Communication and Presentation at: PER’s 11th Annual International Symposium on Melanoma and Other Cutaneous Malignancies. March 7, 2015.
- Kyi C, Postow MA. Immune checkpoint inhibitor combinations in solid tumors: opportunities and challenges. Immunotherapy. 2016;8(7):821-837. doi: 10.2217/imt-2016-0002
- Marrone KA, Ying W, Naidoo J. Immune-related adverse events from immune checkpoint inhibitors. Clin Pharmacol Ther. 2016;100(3):242-251. doi: 10.1002/cpt.394
- Postow MA, Sidlow R, Hellmann M. Immune-related adverse events associated with immune checkpoint blockade. N Engl J Med. 2018;378:158-168. doi: 10.1056/NEJMra1703481
- Leonardi GC, Gainor JF, Altan M, et al. Safety of programmed death-1 pathway inhibitors among patients with non-small cell lung cancer and preexisting autoimmune disorders. J Clin Oncol. 2018;36(19):1905-1912. doi: 10.1200/JCO.2017.77.0305
- Haanen J, Obeid M, Spain L, et al. Management of toxicities from immunotherapy: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2022;33(12):1217-1238. doi: 10.1016/j.annonc.2022.10.001
- Trinh S, Le A, Gowani S, La-Beck NM. Management of immune-related adverse events associated with immune checkpoint inhibitor therapy: a minireview of current clinical guidelines. Asia Pac J Oncol Nurs. 2019;6(2):154-160. doi: 10.4103/apjon.apjon_3_19
Back to Top