
Expired activity
Please go to the PowerPak
homepage and select a course.
Chronic Rhinosinusitis with Nasal Polyps: The Role of the Pharmacist in CRSwNP
INTRODUCTION
Chronic rhinosinusitis (CRS)—a common condition that affects about 11% of people—is an annoying condition that lasts more than 12 weeks and occurs in 2 forms.1 The more common is chronic rhinosinusitis without nasal polyps (CRSsNP or type 1 CRSsNP). Less commonly encountered, chronic rhinosinusitis with nasal polyps (CRSwNP or type 2 CRSwNP) is an inflammatory disease of the nasal mucosa and paranasal sinuses that is linked to significant morbidity and reduced health-related quality of life (HRQoL).1-3 This condition is more prevalent in males and is distinctly different from noninflammatory, type 1 CRSsNP.4
Patients who have CRSwNP often appear—and feel—miserable because this condition creates almost constant difficulty breathing, loss of smell and sometimes taste, and fatigue secondary to sleep loss. Their physical and mental HRQoL is significantly lower than that seen in other conditions. It is similar to that associated with chronic obstructive pulmonary disease (COPD), asthma, and diabetes, especially if they have comorbid asthma and/or nonsteroidal anti-inflammatory drug (NSAID)-exacerbated respiratory disease (N-ERD).5-7
Patients with moderate-to-severe CRSwNP often need repeated treatment with corticosteroids or sinonasal surgery, which are both steps that lessen symptoms but do not cure the condition.3
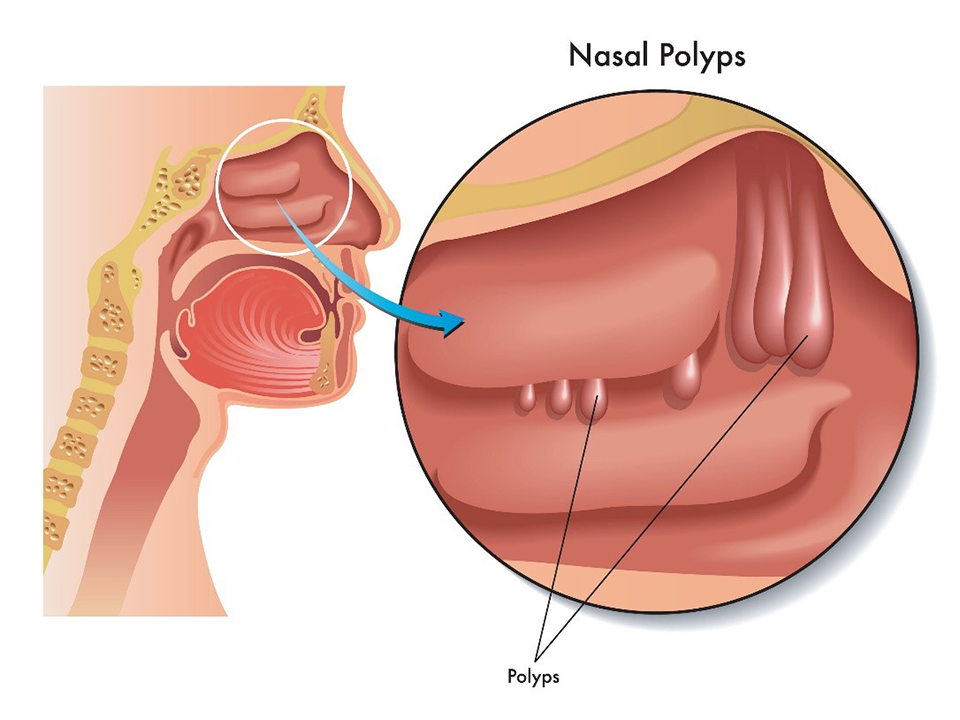
When pharmacy practitioners hear the term “nasal polyps,” they may wonder what these benign tumors look like. The visual description is usually something like this: polyps begin as teardrop-shaped soft protrusions, and as they grow, they eventually resemble peeled grapes.8 These growths block the nasal passages and, if severe, require surgery for removal. At their largest, they may be visible in the nose or protrude. Because they are soft and located on a stemlike or pedunculated base, they will move as the patient changes position, sometimes causing abrupt discomfort. FIGURE 1 shows the location of nasal polyps in the sinonasal space.8
FIGURE 1. Nasal Polyps
Nasal polyps are soft, teardrop-shaped growths located on the lining of the sinonasal passages.8 |
 |
| Credit: © Can Stock Photo/rob3000. |
CRSwNP also confers a substantial cost burden to society and individual patients. In 2019, a team of researchers from leading academic institutions and pharmaceutical companies estimated that total annual health care costs for patients with CRSwNP were $11,507, contributing to a total cost of $5.7 billion in the United States (US) per year.9 This observational, retrospective, case-control study found that indirect costs associated with CRSwNP include lost productivity and lost workdays, with a modest estimate that employees miss an average of 4.8 days of work per year (note different estimate below). Consequently, the researchers estimated direct and indirect costs at $7,182 per patient, and the total cost of CRSwNP per patient per year can exceed $15,000.9
EPIDEMIOLOGY
Experts estimate that roughly 2.1% of American adults would meet the criteria to be diagnosed with CRS,10 and in Europe, the estimates indicate that between 2.1% and 4.3% of adults are affected.11,12 Approximately 20% to 30% of patients with CRS have CRSwNP.3,13 Since technically patients would need to have nasal endoscopy (and sometimes X-rays) for reliable diagnoses, prevalence estimates for nasal polyps, which have been based on questionnaire data, may be inaccurate.14
CRSwNP usually develops in early middle age, with a peak incidence in adults in their 40s.2 Nasal symptoms tend to develop slowly, and many patients with CRSwNP simply live with the sinonasal symptoms rather than seeking treatment, even if the symptoms are severe.12 Females are affected less frequently than males but are more likely to experience severe symptoms when they have CRSwNP.3
How and why CRSwNP develops is unclear. However, clinicians use certain symptoms, described in TABLE 1, to make the diagnosis. Of note, severe symptoms vary in intensity throughout the course of the disease; they wax and wane and can be positional.15-18
| TABLE 1. Symptoms Associated With Nasal Polyps15-18 |
- Decreased (or total loss of) sense of smell and/or taste
- Facial pain, pain in the upper teeth, or headache
- Feelings of pressure over the forehead and face
- Frequent nosebleeds
- Persistent nasal stuffiness and congestion (common)
- Postnasal drip (common)
- Runny nose for at least 3 months
- Sleep disturbances
- Snoring and obstructive sleep apnea
|
CASE STUDY (PART 1)
Lou is a 45-year-old man who is in the pharmacy today to pick up decongestants and antihistamines. Yes, that’s plural—decongestants and antihistamines. The technician alerts you that he’s been in several times in the last few months and he’s complaining that nothing is helping his constant runny nose and congestion. He says he’s had a runny nose since the presidential elections in 2016—that’s 6 years! When you begin asking questions, he tells you that he is exhausted. He says that he snores, and often when his wife pokes him and he rolls over, he feels like he cannot breathe at all. He hasn’t been diagnosed with asthma, but he has 2 siblings who have it. He also says he’s missed quite a bit of work, but he hasn’t seen a doctor because he hates to miss another day.
CRSwNP has been linked to absenteeism and presenteeism (going to work but performing below expectations because of illness). One study found employees who had refractory nasal polyps were absent an average of 24.6 days every year, and they were present but were unproductive on an additional 38.8 days.19 That represents 24% of the usual 260 workdays in a year. Polyps also affect individuals’ time at home. Participants in this study spent roughly 21 days annually on daily sinus care routines. Ultimately, the productivity cost averaged more than $10,000 per year in 2014, with costs increasing as the condition worsened.19
Increasingly, clinicians and researchers are soliciting patients’ input and their assessments of outcomes when looking for targets and treatments for diseases. In the case of CRSwNP, the European Forum for Research and Education in Allergy and Airway Diseases (EUFOREA) Patient Advisory Board interviewed 15 patients using semi-structured interviews.20 The results of this activity were enlightening. CRSwNP patients voiced a need for greater societal awareness, and said that physicians seemed to be unaware of, discount, or underestimate CRSwNP’s burden on social function and well-being. When asked to identify the most bothersome symptoms, patients selected poor sleep quality and psychological impact. Close to the top of their concerns was the lack of smell and taste associated with the condition. They also complained about the lack of care coordination and limited treatment options, highlighting the transient effectiveness when they used oral corticosteroids and/or had sinus surgery. EUFOREA’s statement provides novel insights on CRSwNP’s burden and the shortcomings of current care.18
Health care systems and the pharmacists who work within them can use the multiple insights made by these patients to provide better care for CRSwNP.
Like many other respiratory tract diseases, CRS is heterogeneous and presents as multiple inflammatory endotypes.21 Typically, patients with CRS will have bilateral benign edematous polyps located in areas from the paranasal sinuses to the nasal cavity. Concurrently, typical patients will have elevated levels of cytokines and mediators and intense inflammatory infiltrates.2,22 In Western countries, eosinophilic inflammation accompanies CRSwNP and is a hallmark of the disease. When patients with CRSwNP are compared to patients without nasal polyps, researchers find elevated levels of immunoglobulin E (IgE), interleukin-4 (IL-4), and IL-5.21,23,24 Further, in patients with more severe CRSwNP, researchers find polyclonal and preferential activation of T-helper type 2 cells that amplifies mucosal inflammation.25
Risk Factors
The incidence of nasal polyps seems to be increasing, and researchers are looking for risk factors. Defects in the sinonasal epithelial barrier, bacterial exposure, and immune system dysregulation may contribute.2,3,23 A unique subgroup of patients with CRSwNP are those with allergic fungal rhinosinusitis; they usually have elevated antifungal IgE, eosinophilic mucus, and unilateral CRSwNP.26
Genetics and environment are always suspected with airway disease. Nasal polyps appear to have an unspecified genetic link (meaning the location of the specific genetic mutation is not clear). A large study showed first-degree relatives of patients who have CRSwNP are 4.1 times more likely to have the condition, and second-degree relatives are 3.3 times more likely than people in a control group.27
Individuals who experience hyperimmune responses to fungus are also at increased risk.28 Bacterial colonization pursuant to impaired innate and adaptive immunity has been implicated; higher IgE levels and eosinophils in nasal polyps are also linked to Staphylococcus aureus colonization.29,30 A specific risk factor—lengthy exposure to occupational dust—has been identified in the textile industry.31
As noted, CRSwNP is linked to both local and systemic inflammation.32 Local inflammation generally manifests as a dysfunctional interaction between the sinonasal mucosa and the environment. Colonization with S aureus in the upper airway can cause biofilm formation, immune dysregulation, inflammation, and barrier dysfunction.22,33,34 Systemic immunologic crosstalk (instances in which 1 or more components of 1 signal pathway affect another) may contribute, with symptoms of CRS resulting from simultaneous irritation of the upper and lower airways.32
Some scientists have also suggested that reflexes mediated by the nervous system similar to what occurs in asthma, possibly via the nodose ganglion/vagus nerve, may influence disease development.35
Common Comorbidities
CRS has long been associated with other respiratory tract diseases such as asthma and inhalant allergy, but various studies have reported different prevalence rates of these comorbidities depending on the CRS phenotype.
In a 2018 study that enrolled 1470 participants, clinical researchers looked at comorbidities. Among the 651 patients with CRSwNP, 46.9% had comorbid asthma compared to 21.2% of patients with CRSsNP and 10% of patients in the control group. CRSwNP patients were more likely to have inhalant allergies or NSAID sensitivity.36
The Global Initiative for Asthma (GINA) and EUFOREA state these conditions are indicators of more severe disease, especially with concomitant asthma. Both stress that addressing these conditions together is essential.37,38
Inflammation explains the close association between CRSwNP and severe asthma and hypersensitivity to NSAIDs; 83% of patients with N-ERD report this correlation.5,39 For this reason, guidelines recommend asking affected individuals about salicylate intake from NSAIDs and dietary sources (eg, blueberries, apples, avocadoes, mushrooms, cauliflower, coffee, nuts [almonds, macadamia nuts, peanuts, pine nuts, pistachios]).40
One-third of patients with CRSwNP and aspirin-exacerbated respiratory disease (AERD) reported that alcohol consumption exacerbated symptoms.39 Researchers at the University of Virginia examined alcohol’s connection to N-ERD and found that red wine was more likely to aggravate symptoms than white wine or clear spirits. These findings suggest that the offending agent may not be alcohol, but polyphenols related to the process used to make red wine.41
Two diseases—Churg-Strauss syndrome (a rare genetic condition characterized by blood vessel inflammation) and cystic fibrosis (CF)—are closely associated with systemic nasal polyposis, but they are generally associated with neutrophilic (as opposed to eosinophilic) inflammation.42 Up to three-quarters of patients with Churg-Strauss syndrome develop nasal polyposis, as do roughly 45% of patients with CF. A clinical pearl for pharmacists is that nasal polyps suggest CF in undiagnosed young patients and call for screening to rule out this inherited respiratory and digestive genetic defect.43,44
Inadequate Diagnosis and Treatment
Unfortunately, diagnosis usually lags onset by approximately 5 years; patients seek health care, but health care practitioners misdiagnose this condition often and repeatedly.43 Heightened awareness of the poor care coordination, tendency not to address comorbidities, and patients’ belief that clinicians lack empathy or understanding should drive clinicians to provide better care.
TREATMENT OPTIONS
Experts recommend 4 treatment goals for patients with CRSwNP45:
- Control inflammation
- Maintain sinus ventilation and drainage
- Treat colonizing or infecting microorganisms
- Reduce exacerbations.45
Currently, a standard algorithm guides clinicians through several steps in a rational manner based on the patient’s response.46 Some treatment approaches can alleviate symptoms in patients with mild-to-moderate disease. In patients who have allergies or experience watery discharge, antihistamines can provide symptomatic relief. Two simple interventions include saline irrigation and intranasal glucocorticoids (INCS).40,47
Saline irrigation, although lacking research evidence, sometimes soothes congestion and pain.40 High-volume, low-pressure nasal saline irrigations—which are inexpensive—may decrease antigen, biofilm, and inflammatory mediators.48
Intranasal glucocorticoids (eg, budesonide, fluticasone, mometasone and others, often used off-label) may reduce polyp size and rhinorrhea and partially or completely restore the patient’s sense of smell.46,47 Yet clinicians tend to under-prescribe INCS or prescribe INCS at doses too low to be effective for nasal polyps. Boosting the dose can deliver better responses. Once-daily dosing is insufficient for patients with CRSwNP; increasing the dose to 2 actuations twice-daily provides the recommended dose and can be up to 4 actuations twice daily for fluticasone.45,48 Patients also tend to underuse these products when they are prescribed, which creates a situation where monitoring at the pharmacy can be helpful.45
The 2021 International Consensus Statement on Allergy and Rhinology: Rhinosinusitis indicates intranasal products vary in cost but tend to be inexpensive or of moderate cost. Common adverse effects include epistaxis (nosebleeds), local irritation, and headache.43
CASE STUDY (PART 2)
Lou finally decides your advice to see the doctor is good, and that it could lead to relief. His primary care provider could see polyps and referred him to an otolaryngologist, who conducted several tests and ordered a CT scan. Lou is here to start on a nasal corticosteroid inhaler. He also has directions for nasal irrigation. He asks you if you have information on how to do the irrigation. He also has concerns about how much time these treatments will take and if they will work.
Increasingly, researchers are looking for intranasal delivery methods that are more effective, especially when polyps enlarge, because large polyps obstruct uniform medication delivery. Delivery methods that are sometimes used (and might be off-label) and being explored include47,49:
- A breath-activated fluticasone spray in which exhalation through a connected mouthpiece generates pressure to spray steroid into the nasal passage
- Corticosteroid injection directly into the sinonasal tissue or the polyp
- Corticosteroid-releasing stents placed surgically that slowly release corticosteroid into the nose and sinuses over 30 days or more
- Synthetic polyurethane nasal dressing or corticosteroid-treated bioresorbable gel-type nasal dressing
- Off-label, corticosteroid-infused materials (but note the risks of unpredictable pharmacological properties, variable nasal dressings saturation and release onto the sinonasal mucosa, and inconsistent amounts of topical corticosteroids at the targeted site).48,50
Patients with moderate-to-severe symptoms will find better relief if they switch from intranasal sprays to topical drops or solutions.40 Research has determined that large volume nasal steroid rinses administered using plastic squeeze bottles are superior to traditional steroid sprays because they reach areas of the nasal structures that spray cannot, although the cost increases.50,43,46
The leukotriene receptor antagonist montelukast may also provide some relief, but the few studies that have looked at its use in CRSwNP have produced conflicting results.43,51 It seems to be approximately as effective as intranasal glucocorticoids and can be used alone or in combination with intranasal glucocorticoids.43
Frequently, topical treatment fails to produce acceptable relief in 4 to 6 weeks. Short-course (2 to 3 weeks) oral glucocorticoids may reduce polyp size, alleviate symptoms, and improve quality of life (QoL). After 3 to 6 months, patients may report that their symptoms are back and need another course of systemic glucocorticoids.34,53,53
The 2021 International Consensus Statement on Allergy and Rhinology: Rhinosinusitis indicates that administering systemic oral steroids for 8 to 12 weeks can provide substantial benefit if monitored closely. Adverse effects include increased bone turnover, insomnia, gastrointestinal irritation, and transient adrenal suppression. Chronic oral steroids are ill-advised, and patients should receive only 2 or 3 short courses of oral steroids annually.55 If patients respond to systemic steroids, they should return to inhaled or topical corticosteroids when they finish the oral steroids, with the goal of maintaining control.46
If these medical treatments fail, traditionally the next step has been endoscopic surgery, but it is not curative.56 Its primary purpose is to restore sinus ventilation, improve topical medications’ ability to penetrate the mucosa, and debulk severe polyposis (multiple polyps).43 Experts have not defined which specific treatments need to be tried or their treatment durations before considering surgery, so clinicians understandably vary in their approaches. Surgical delay has been associated with a greater likelihood of asthma later in life.56
Many patients will need another surgery (called surgical revision) if polyps recur.57 Complications, although rare, include bleeding, cerebrospinal fluid leak, infection, intracranial injury, hyposmia/anosmia, lacrimal system injury, orbital injury, scarring, septal perforation, vascular injury, and vision changes or blindness.43
A few weeks after surgery, aspirin desensitization can help patients with adequate pulmonary function to prevent polyp recurrence. Many patients report improved QoL and less reliance on systemic steroids. Aspirin desensitization may also reduce the likelihood of revision surgery. Desensitization starts with gradually increasing doses of aspirin administered orally or intranasally. Once patients reach the highest dose of aspirin that fails to trigger symptoms, they continue to take a maintenance dose. Aspirin’s well-known adverse effects (eg, gastric bleeding or pain, impaired renal function, nausea, and anticoagulation) are problems for many patients, and approximately 50% of patients cannot persist for more than a few months.43,46
Clinicians should have a high index of suspicion for S aureus. It is unclear if staph infection causes or exacerbates nasal polyps. If it appears that the infection is bothersome, clinicians can employ methylprednisolone to decrease inflammation and/or a 3-week course of doxycycline.58,59
BIOLOGICS
Medical researchers, noting that approximately 80% of patients with CRSwNP have a type 2 eosinophilic inflammation, have targeted this fact to develop biologics.54 Elevated IL-4, IL-5, and IL-13 levels may aggravate nasal polyps and are current biologic targets. The US Food and Drug Administration (FDA) approved dupilumab for this condition in 2019, omalizumab in 2020, and mepolizumab in 2021. All decrease polyp burden and improve symptoms.23,38,60
In 2021, EUFOREA established 5 standards that are considered necessary when considering biologics in CRSwNP patients: 1) evidence of type 2 inflammation (ie, biological biomarker); 2) need for systemic corticosteroids in the past 2 years; 3) significant impairment of QoL; 4) pronounced anosmia; and 5) diagnosis of comorbid asthma.38,61
Dupilumab
Dupilumab (Dupixent) inhibits IL-4 and IL-13 signaling. Dupilumab’s approval was based on 2 pivotal trials, both of which enrolled high numbers of participants who had comorbid asthma (59%) and N-ERD (28%).62
The first and smaller phase 3, randomized, placebo-controlled LIBERTY NP SINUS-24 trial enrolled 276 participants.63 Patients had severe, poorly controlled nasal polyps despite surgery with or without subsequent nasal steroids. A majority of patients had previous surgeries, and 15% had 3 or more surgeries. Approximately three-quarters of patients had taken short courses of systemic steroids in the 2 years before enrollment. Participants in the active treatment arm received dupilumab 300 mg subcutaneously (SC) every 2 weeks for 1 year, followed by 300 mg every 2 weeks for 24 weeks. The other arm employed a placebo.63
The randomized, placebo-controlled LIBERTY NP SINUS-52 trial enrolled 448 participants.63 To assess safety and efficacy, the researchers used 2 primary endpoints63:
- Changes from baseline to week 24 in nasal polyp score (NPS, an unvalidated score to measure polyp size with 0 = no blockage on 1 side and 4 meaning total blockage on 1 side [total possible score is 8, indicating complete blockage on both sides]), nasal congestion, or obstruction
- Sinus Lund-Mackay CT scores, done in an intention-to-treat (ITT) population.
The researchers randomized participants randomly (1:1:1) to dupilumab 300 mg every 2 weeks for 52 weeks, dupilumab every 2 weeks for 24 weeks and then every 4 weeks for the remaining 28 weeks, or placebo every 2 weeks for 52 weeks.63
In both LIBERTY NP SINUS-24 and LIBERTY NP SINUS-52, dupilumab significantly improved the endpoints within as early as 4 weeks of treatment.64 Dupilumab-treated participants’ NPS scores fell by 2 points (95% CI, -2.43 to -1.69; P < .0001) in SINUS-24 and 1.8 points (-2.10 to -1.51; P < .0001) in SINUS-52 compared with those treated with placebo. In LIBERTY NP SINUS-24, polyps tended to recur when treatment was withdrawn. Patient-reported outcomes improved significantly, and surgical intervention was reduced by 83%.63
The most common adverse events included nasopharyngitis, worsening of nasal polyps and asthma, headache, epistaxis, and injection-site erythema. Patients in the placebo arm were more likely to experience these adverse events.63
Dupilumab’s labeling of common adverse reactions is similar. It lists injection site reactions, eosinophilia, insomnia, toothache, gastritis, arthralgia, and conjunctivitis.62
Omalizumab
Researchers explored anti-IgE antibody omalizumab’s (Xolair) safety and efficacy in the POLYP 1 (n = 138) and POLYP 2 (n = 127) trials.65 They enrolled adults with CRSwNP who had inadequate responses to INCS, randomizing patients 1:1 to omalizumab or placebo and intranasal mometasone for 24 weeks. The POLYP trials used 2 primary endpoints: 1) NPS change from baseline to week 24 and 2) Nasal Congestion Score. Secondary endpoints included a patient- reported outcome measure, the Sino-Nasal Outcome Test-22 (SNOT-22).65
In both trials, participants had severe CRSwNP and substantially impaired QoL (mean NPS higher than 6 and patient-reported outcome measure scores of approximately 60).65 Approximately 60% of patients had had previous surgeries, and between 12% and 29% of patients had used systemic steroids in the previous year. Up to 61% of participants had comorbid asthma, and up to 38% had N-ERD.65
Both studies met the coprimary endpoints, with changes in NPS of 1 to 2 points.51 At the trials’ end, omalizumab-treated participants had better patient-reported outcome measures, sense of smell, postnasal drip, and runny nose than placebo-treated patients. In both trials, the mean changes from baseline at week 24 for omalizumab compared to placebo were as follows: NPS, -1.08 versus 0.06 (P < .0001) and -0.90 versus -0.31 (P = .0140); NPS, -0.89 versus -0.35 (P = .0004) and -0.70 versus -0.20 (P = .0017); and patient-reported outcomes measure, -24.7 versus -8.6 (P < .0001) and -21.6 versus -6.6 (P < .0001).65
Adverse events were similar between groups. Again, placebo-treated patients were more likely to report adverse events than omalizumab-treated patients. In general, the researchers graded adverse events as mild to moderate.65
Omalizumab’s labeling indicates that in patients with nasal polyps, common adverse reactions (at least 3% of patients) include headache, injection site reaction, arthralgia, upper abdominal pain, and dizziness.66 This product has a boxed warning concerning potential anaphylaxis (bronchospasm, hypotension, syncope, urticaria, and/or angioedema of the throat or tongue).66
Mepolizumab
In July 2021, the FDA approved mepolizumab (Nucala), an IL-5 antagonist, to treat CRSwNP. It blocks the growth, differentiation, recruitment, activation, and survival of eosinophils.26
The randomized, double-blind, placebo-controlled, phase 3 SYNAPSE trial (N = 407) enrolled adults with recurrent, refractory, severe, bilateral nasal polyp symptoms (nasal obstruction symptom visual analogue scale [VAS] score >5).67 Participants were also eligible for repeat nasal surgery despite standard of care treatment and had at least 1 nasal surgery in the past 10 years—and 33% had 3 or more previous surgeries. The number of participants with asthma and NSAID-exacerbated disease was also high (71% and 26%, respectively). Researchers randomized participants 1:1 to receive either 100 mg mepolizumab subcutaneously or placebo once every 4 weeks plus the necessary standard of care for 52 weeks. The trial’s endpoints were change from baseline in total endoscopic nasal polyp score at week 52 and change in mean nasal obstruction VAS score during weeks 49 to 52.67
At week 52, mepolizumab-treated participants’ (n = 206) total endoscopic NPS significantly improved compared with placebo-treated participants’ (n = 201) scores (adjusted difference in medians -0.73; 95% CI, -1.11 to -0.34; P < .0001).67 Similarly, nasal obstruction VAS score measured in weeks 49 to 52 also significantly improved (-3.14; -4.09 to -2·.8; P < .0001).67
Adverse events were reported in 15% of mepolizumab-treated patients and 9% of placebo-treated patients. Six percent of participants in both arms experienced on-treatment serious adverse events, but none were mepolizumab related. Researchers associated treatment with a 50% reduction in the need for surgery and 42% less systemic steroid use. They concluded mepolizumab treatment improved nasal polyp size and nasal obstruction compared better than placebo. The researchers identified no new safety concerns in the population.67
The recommended adult dose of mepolizumab is 100 mg SC once every 4 weeks.67
Investigational Biologics
Benralizumab (Fasenra), a monoclonal anti-IL-5 receptor alpha (anti-IL5Ra) antibody,33 is currently being studied in 2 phase 3 trials, OSTRO and ORCHID, for CRSwNP. One trial is completed, and the other is ongoing.14
The Onset of Effect and Impact on Health-Related Quality of Life, Exacerbation Rate, Lung Function, and Nasal Polyposis Symptoms for Patients with Severe Eosinophilic Asthma Treated with Benralizumab (called the ANDHI trial) was a randomized, controlled, double-blind, parallel-group, placebo-controlled phase 3b trial.55 The trial assessed benralizumab’s efficacy, onset of effect, impact on HRQoL, exacerbation rate, lung function, and nasal polyposis symptoms. The researchers reported early clinical responses in patient-reported outcomes, HRQoL, pulmonary function, and nasal polyposis symptoms.68
Additionally, tezepelumab (Tezspire), a thymic stromal lymphopoietin (TSLP) blocker and immunoglobulin G2 (IgG2) antibody, is being studied in a phase 3 trial for use in CRSwNP.69
PHARMACIST SUPPORT IN CRSwNP
Pharmacists in all practice locations will need to educate patients in a stark reality—they will need to manage their CRSwNP indefinitely because it is a manifestation of chronic inflammation and airway lining dysfunction. It is not a resolvable infection or a passing problem. This disease is chronic and incurable and needs to be managed accordingly. The treatment goals for CRSwNP go hand-in-hand with current treatment strategy40:
- Treatment should improve upper and lower airway, rhinologic, and extra-nasal rhinologic symptoms
- Treatment should also improve topical medical therapy delivery and efficacy.
Helping patients stay treatment adherent is probably the most important area for pharmacist involvement.48,49 This is especially true for patients with comorbid lower airway disease. Pharmacists and others on the team must stress the relationship between upper and lower airway inflammation and explain the concept of unified airway disease. Some specialists describe this condition to patients using the term “asthma of the nose.”70 It emphasizes that nasal polyps, like asthma, are chronic.
Patients may be unfamiliar with or reluctant to use nasal irrigation. Prescribers generally recommend a neti pot, a squeeze bottle, or a bulb syringe.71 Patients should use sterile water, which they can make by boiling water and allowing it to cool, if they mix their own saline solutions. They administer irrigation solutions by standing over a sink or in the shower, tilting the head to 1 side, and squeezing or pouring the solution into the upper nostril. The solution will drain out of the lower nostril.
Patients should breathe from their mouths during the process and repeat the process on the other side. It takes trial and error to determine the best position so that the irrigation solution does not run into the throat. Once they have irrigated both sides, patients should blow their noses gently; if they had recent surgery, the surgeon would likely tell them to skip this step for up to a week.72 Patients can find demonstration videos on various video sites like YouTube.
Some otolaryngologists order preparations that add medication that addresses the inflammatory process within the sinuses to nasal saline irrigations, which require compounding.48 If the patient’s regular pharmacy does not provide compounding services, patients will need referrals to appropriate pharmacies.
Redundant counseling for patients who use inhalers on technique is also important. Patient technique often declines with time, so reassessing technique periodically is wise. Epistaxis is a common adverse effect in patients who have CRSwNP, and good counseling can also help patients develop a technique that reduces its occurance.45
CASE STUDY (PART 3)
Lou returns to the pharmacy and reports he started on a biologic 4 months ago. He reports he’s feeling better and anxious to stop using the intranasal corticosteroids and irrigation. He says, “Those treatments take time, and now, I am all set. Biologics are the best thing ever.” This is a typical problem. Many patients don’t realize that when they start a biologic, they still need to continue their usual care. You’re now in the position that you need to gently educate him about lifelong management of nasal polyps. What will you say about what to expect, the need for adherence, and future treatment options?
Managing Expectations: Systemic Steroids and Surgery
Short-course corticosteroids are often employed. Patients need to know that it is possible to see significant improvements in HRQoL and symptom severity, but the benefit usually disappears within 3 months.72,73 In addition, guidelines agree that 3 short courses of corticosteroids annually is the absolute limit for this intervention.43,45 This recommendation is probably based on a longitudinal observational study that enrolled patients with asthma. Receiving more than 2.5 short courses of oral corticosteroids annually was associated with a significantly greater loss of bone marrow density (BMD) than the BMD loss in patients who received 2.5 courses or fewer per year.74
As noted throughout this continuing education activity, it is common for patients to progress to the point of needing surgery. Patients should not expect a cure pursuant to surgery and may need additional surgeries later. Managing expectations around the time of surgery is critical, as polyps recur in 40% to 60% of postsurgical patients; this is especially true among asthma and N-ERD patients.14,17
Patients will continue to need oral and nasal medications after surgery to slow recurrence.17 Accordingly, EUFOREA and the American Academy of Allergy, Asthma & Immunology (AAAAI) recommend patients who have moderate-to-severe asthma or steroid-dependent asthma and who want to avoid surgery or are not eligible for surgery should be directly considered for a biologic agent.38,61,75
If patients begin treatment with biologics, the pharmacist should discuss adherence pointedly during counseling and ensure that patients know they will need to continue the biologic for at least 6 months before the prescriber can assess its effectiveness.38 Additionally, they should remind patients not to discontinue corticosteroids abruptly once they start a biologic. Dupilumab’s labeling includes patient information, and reviewing that information with patients can guide comprehensive discussion. This biologic is administered SC (300 mg every other week), and patients need education on injection technique.62
Omalizumab’s dosing is 75 to 600 mg SC every 2 or 4 weeks, with the dose and dosing frequency calculated based on total serum IgE level and body weight. For omalizumab, the FDA requires health care providers to give patients a Medication Guide before starting treatment and before each subsequent treatment, and the Medication Guide is included in its approved labeling.66
Mepolizumab’s dose in CRSwNP is 100 mg SC every 4 weeks.67 Its labeling includes patient information as well. Patients should also know researchers have not yet been able to demonstrate that the approved biologics have disease-modifying effects, so polyps may return if patients stop the biologics.45
Pharmacists may be able to provide some insight to prescribers when they have difficulty selecting therapies for specific patients. Pharmacists should encourage prescribers to consider patient preference and dexterity. Some patients may be unable to irrigate their sinuses without help, for example, and different types of inhalers have various features that require different levels of eyesight, dexterity, breath, and coordination.45
Large polyps, because they cause blockage, decrease the effectiveness of INCS, and pharmacists should have a high index of suspicion when patients complain that inhalers do not work despite good technique and adherence.17 Often, patients with concurrent asthma or N-ERD will require maximum doses of INCS for disease management. Additionally, saline spray or irrigation is necessary for all types of CRS and should be used daily.17
Experts recommend using second-generation intranasal corticosteroids (eg, budesonide, fluticasone propionate, mometasone) rather than first-generation (eg, beclomethasone, flunisolide, triamcinolone) for CRSwNP because patients usually need long-term treatment; second-generation intranasal corticosteroids are less likely to cause systemic adverse effects.45
The ability to pay can represent a barrier to biologic access, so pharmacists can find patient assistance programs.
Assessing comorbidities can occasionally suggest that 1 biologic might be better than another. In addition to add-on maintenance treatment in adult patients with inadequately controlled CRSwNP, the FDA has approved dupilumab for moderate-to-severe atopic dermatitis and moderate-to-severe asthma aged 12 years and older with an eosinophilic phenotype or with oral corticosteroid-dependent asthma.62
The FDA has approved omalizumab for moderate-to-severe persistent asthma in patients 6 years of age and older with a positive skin test or in vitro reactivity to a perennial aeroallergen and symptoms that are inadequately controlled with inhaled corticosteroids (atopic asthma) and chronic idiopathic urticaria.66 Mepolizumab’s indications include severe asthma in patients older than 6 years and eosinophilic granulomatosis with polyangiitis adult patients.76 If a patient’s CRSwNP does not respond to a specific biologic, switching to the another biologic is rational.
TABLE 2 lists key counseling points to stress for patients who have nasal polyps.40,77
| TABLE 2. Counseling Points: Talking to Patients Who Have Nasal Polyps40,78 |
- Manage allergies and asthma. If asthma and allergy symptoms continue despite good adherence, consider modifying the treatment plan
- Use a nasal rinse, OTC saline sprays or nasal wash kits with devices, or distilled or sterile water. Clean the irrigation devices thoroughly after each use
- Use inhalers properly and as prescribed. Be certain to talk to your prescriber or pharmacist if you find an inhaler difficult to use. Consider increasing the dose or frequency if the response is not acceptable
- Avoid nasal irritants. Allergens, chemical fumes, fine dust and debris, and tobacco smoke will exacerbate symptoms
- Practice good hygiene. Wash hands often and well to protect against bacterial and viral infections and keep hands away from your face and nose.
- Use room humidifiers to hydrate the nasal passages, improve mucus flow, and help prevent blockages and inflammation. Clean humidifiers as recommended by the manufacturer.
|
| Abbreviation: OTC, over-the-counter. |
Interplay With Health Systems
Beyond patient-level support, pharmacists can improve care at the systems level. They must recognize the burden of disease on HRQoL by developing and implementing evidence-based clinical programs, which include access to specialists and biologics. Obviously, systems need pharmacy benefits that manage quality of care and cost-effectiveness. But if the systems in which pharmacists work create health care inequalities and limited access to novel treatments, pharmacists can advocate for simple, more empathetic, and easily navigable prior authorization processes.
One area where pharmacists have considerable impact is in the development of medication distribution and education practices to ensure patient safety and optimal use of biologics. Communicating and collaborating with patients, prescribers, and payors can minimize delays in therapy and increase access. It can also create a better relationship between patients and clinicians.
CONCLUSION
CRSwNP is not just a runny nose or nasal congestion. It is a serious condition that causes substantial distress. Researchers are narrowing down the biologic mechanisms that cause this condition, and several biologics are approved or under study. Regardless, at this point, CRSwNP is incurable, meaning pharmacists and other health care providers need to educate patients about lifelong management.
REFERENCES
- Hastan D, Fokkens WJ, Bachert C, et al. Chronic rhinosinusitis in Europe—an underestimated disease. A GA2 LEN study. Allergy. 2011;66(9):1216-1223. doi:10.1111/j.1398-9995.2011.02646.x
- Alobid I, Antón E, Armengot M, et al. SEAIC-SEORL. Consensus document on nasal polyposis. POLINA project. J Investig Allergol Clin Immunol. 2011;21(suppl 1):1-58.
- Stevens WW, Schleimer RP, Kern RC. Chronic rhinosinusitis with nasal polyps. J Allergy Clin Immunol Pract. 2016;4(4):565-572. doi:10.1016/j.jaip.2016.04.012
- Chen S, Zhou A, Emmanuel B, Thomas K, Guiang H. Systematic literature review of the epidemiology and clinical burden of chronic rhinosinusitis with nasal polyposis. Curr Med Res Opin. 2020;36(11):1897-1911. doi:10.1080/03007995.2020.1815682
- Khan A, Huynh TMT, Vandeplas G, et al. The GALEN rhinosinusitis cohort: chronic rhinosinusitis with nasal polyps affects health-related quality of life. Rhinology. 2019;57(5):343-351. doi:10.4193/Rhin19.158
- van Agthoven M, Fokkens WJ, van de Merwe JP, et al. Quality of life of patients with refractory chronic rhinosinusitis: effects of filgrastim treatment. Am J Rhinol. 2001;15(4):231-237. https://doi.org/10.1177/194589240101500403
- Wensing M, Vingerhoets E, Grol R. Functional status, health problems, age and comorbidity in primary care patients. Qual Life Res. 2001;10(2):141-148. doi:10.1023/A:1016705615207
- Fried MP. Nasal polyps. Merck Manual Professional Version. Revised December 2021. Accessed July 7, 2022. https://www.merckmanuals.com/professional/ear,-nose,-and-throat-disorders/nose-and-paranasal-sinus-disorders/nasal-polyps
- Bhattacharyya N, Villeneuve S, Joish VN, et al. Cost burden and resource utilization in patients with chronic rhinosinusitis and nasal polyps. Laryngoscope. 2019;129(9):1969-1975. doi:10.1002/lary.27852
- Bhattacharyya N, Gilani S. Prevalence of potential adult chronic rhinosinusitis symptoms in the United States. Otolaryngol Head Neck Surg. 2018;159(3):522-525. doi:10.1177/0194599818774006
- Hedman J, Kaprio J, Poussa T, Nieminen MM. Prevalence of asthma, aspirin intolerance, nasal polyposis and chronic obstructive pulmonary disease in a population-based study. Int J Epidemiol. 1999;28(4):717-722. doi:10.1093/ije/28.4.717
- Klossek JM, Neukirch F, Pribil C, et al. Prevalence of nasal polyposis in France: a cross-sectional, case-control study. Allergy. 2005;60(2):233-237. doi:10.1111/j.1398-9995.2005.00688.x
- Benjamin MR, Stevens WW, Li N, et al. Clinical characteristics of patients with chronic rhinosinusitis without nasal polyps in an academic setting. J Allergy Clin Immunol Pract. 2019;7(3):1010-1016. doi:10.1016/j.jaip.2018.10.014
- Bachert C, Van Bruaene N, Toskala E, et al. Important research questions in allergy and related diseases: 3-chronic rhinosinusitis and nasal polyposis - a GALEN study. Allergy. 2009;64(4):520-533. doi:10.1111/j.1398-9995.2009.01964.x
- Fokkens WJ, Lund V, Bachert C, et al. EUFOREA consensus on biologics for CRSwNP with or without asthma. Allergy. 2019;74(12):2312-2319. doi:10.1111/all.13875
- Kim DW, Cho SH. Emerging endotypes of chronic rhinosinusitis and its application to precision medicine. Allergy Asthma Immunol Res. 2017;9(4):299-306. doi:10.4168/aair.2017.9.4.299
- Fokkens WJ, Lund VJ, Hopkins C, et al. European position paper on rhinosinusitis and nasal polyps 2020. Rhinology. 2020;58(suppl S29):1-464. doi:10.4193/Rhin20.600
- Alobid I, Cardelus S, Benítez P, et al. Persistent asthma has an accumulative impact on the loss of smell in patients with nasal polyposis. Rhinology. 2011;49(5):519-524. doi:10.4193/Rhino10.295
- Rudmik L, Smith TL, Schlosser RJ, et al. Productivity costs in patients with refractory chronic rhinosinusitis. Laryngoscope. 2014;124(9):2007-2012. doi:10.1002/lary.24630
- Claeys N, Teeling MT, Legrand P, et al. Patients unmet needs in chronic rhinosinusitis with nasal polyps care: a patient advisory board statement of EUFOREA [published correction appears in Front Allergy. 2021 Oct 29;2:789425]. Front Allergy. 2021;2:761388. doi:10.3389/falgy.2021.761388
- Tomassen P, Vandeplas G, Van Zele T, et al. Inflammatory endotypes of chronic rhinosinusitis based on cluster analysis of biomarkers. J Allergy Clin Immunol. 2016;137(5):1449-1456.e1444. doi:10.1016/j.jaci.2015.12.1324
- Bachert C, Gevaert P, Holtappels G, et al. Total and specific IgE in nasal polyps is related to local eosinophilic inflammation. J Allergy Clin Immunol. 2001;107(4):607-614. doi:10.1067/mai.2001.112374
- Chaaban MR, Walsh EM, Woodworth BA. Epidemiology and differential diagnosis of nasal polyps. Am J Rhinol Allergy. 2013;27(6):473-478. doi:10.2500/ajra.2013.27.3981
- Dietz de Loos DAE, Hopkins C, Fokkens WJ. Symptoms in chronic rhinosinusitis with and without nasal polyps. Laryngoscope. 2013;123(1):57-63. doi:10.1002/lary.23671
- Bachert C, Claeys SE, Tomassen P, et al. Rhinosinusitis and asthma: a link for asthma severity. Curr Allergy Asthma Rep. 2010;10(3):194-201. doi:10.1007/s11882-010-0096-0
- Dykewicz MS, Rodrigues JM, Slavin RG. Allergic fungal rhinosinusitis. J Allergy Clin Immunol. 2018;142(2):341-351. doi:10.1016/j.jaci.2018.06.023
- Oakley GM, Curtin K, Orb Q, et al. Familial risk of chronic rhinosinusitis with and without nasal polyposis: genetics or environment. Int Forum Allergy Rhinol. 2015;5(4):276-282. https://doi.org/10.1002/alr.21469
- Cohen NA, Widelitz JS, Chiu AG, et al. Familial aggregation of sinonasal polyps correlates with severity of disease. Otolaryngol Head Neck Surg.2006;134(4):601-604. doi:10.1016/j.otohns.2005.11.042
- Song WJ, Lee JH, Won HK, Bachert C. Chronic rhinosinusitis with nasal polyps in older adults: clinical presentation, pathophysiology, and comorbidity. Curr Allergy Asthma Rep. 2019;19(10):46. doi:10.1007/s11882-019-0880-4
- Hulse KE, Stevens WW, Tan BK, Schleimer RP. Pathogenesis of nasal polyposis. Clin Exp Allergy. 2015;45(2):328-346. doi:10.1111/cea.12472
- Veloso-Teles R, Cerejeira R, Roque-Farinha R, von Buchwald C. Higher prevalence of nasal polyposis among textile workers: an endoscopic based and controlled study. Rhinology. 2018;56(2):99-105. doi:10.4193/Rhin17.228
- Rudmik L, Smith TL, Schlosser RJ, et al. Productivity costs in patients with refractory chronic rhinosinusitis. Laryngoscope. 2014;124(9):2007-2012. doi:10.1002/lary.24630
- Suh JD, Ramakrishnan V, Palmer JN. Biofilms. Otolaryngol Clin North Am. 2010;43(3):521-530, viii. doi:10.1016/j.otc.2010.02.010
- Van Zele T, Gevaert P, Watelet JB, et al. Staphylococcus aureus colonization and IgE antibody formation to enterotoxins is increased in nasal polyposis. J Allergy Clin Immunol. 2004;114(4):981-983. doi:10.1016/j.jaci.2004.07.013
- Mazzone SB, Undem BJ. Vagal afferent innervation of the airways in health and disease. Physiol Rev. 2016;96(3):975-1024. doi:10.1152/physrev.00039.2015
- Philpott CM, Erskine S, Hopkins C, et al. Prevalence of asthma, aspirin sensitivity and allergy in chronic rhinosinusitis: data from the UK National Chronic Rhinosinusitis Epidemiology Study. Respir Res. 2018;19(1):129. doi:10.1186/s12931-018-0823-y
- Global Strategy for Asthma Management and Prevention (2021 update). Global Initiative for Asthma. Accessed July 7, 2022. https://ginasthma.org/wp-content/uploads/2021/05/GINA-Main-Report-2021-V2-WMS.pdf
- Bachert C, Han JK, Wagenmann M, et al. EUFOREA expert board meeting on uncontrolled severe chronic rhinosinusitis with nasal polyps (CRSwNP) and biologics: definitions and management [published correction appears in J Allergy Clin Immunol. 2021;147(5):1981-1982]. J Allergy Clin Immunol. 2021;147(1):29-36. doi:10.1016/j.jaci.2020.11.013
- De Schryver E, Derycke L, Campo P, et al. Alcohol hyper-responsiveness in chronic rhinosinusitis with nasal polyps. Clin Exp Allergy. 2017;47(2):245-253. doi:10.1111/cea.12836
- Hopkins C. Chronic rhinosinusitis with nasal polyps. N Engl J Med. 2019;381:55-63. doi:10.1056/NEJMcp1800215
- Eschenbacher W, Kim M, Mattos J, Lawrence M, Payne S, Borish L. Activation of platelet-adherent basophils in chronic rhinosinusitis with alcohol hypersensitivity. Ann Allergy Asthma Immunol. 2022;128(4):443-450. doi:10.1016/j.anai.2022.01.013
- Chaaban MR, Walsh EM, Woodworth BA. Epidemiology and differential diagnosis of nasal polyps. Am J Rhinol Allergy. 2013;27(6):473-478. doi:10.2500/ajra.2013.27.3981
- Orlandi RR, Kingdom TT, Smith TL, et al. International consensus statement on allergy and rhinology: rhinosinusitis 2021. Int Forum Allergy Rhinol. 2021;11(3):213-739. doi:10.1002/alr.22741
- Brihaye P, Clement PA, Dab I, et al. Pathological changes of the lateral nasal wall in patients with cystic fibrosis (mucoviscidosis). Int J Pediatr Otorhinolaryngol 1994;28(2-3):141-147. doi:10.1016/0165-5876(94)90005-1
- Ranford D, Hopkins C. Safety review of current systemic treatments for severe chronic rhinosinusitis with nasal polyps and future directions. Expert Opin Drug Saf. 2021;20(10):1177-1189. doi:10.1080/14740338.2021.1926981
- Naclerio R, Baroody F, Bachert C, et al. Clinical research needs for the management of chronic rhinosinusitis with nasal polyps in the new era of biologics: a National Institute of Allergy and Infectious Diseases workshop. J Allergy Clin Immunol Pract. 2020;8(5):1532-1549.e1. doi:10.1016/j.jaip.2020.02.023
- Chong LY, Head K, Hopkins C, Philpott C, Burton MJ, Schilder AG. Different types of intranasal steroids for chronic rhinosinusitis. Cochrane Database Syst Rev. 2016;4(4):CD011993. doi:10.1002/14651858.CD011993.pub2
- Dhringa PL, Dhingra S. Diseases of the Ear, Nose and Throat & Head and Neck Surgery. 7th ed. Elsevier India; 2017.
- Lelegren MJ, Bloch RA, Lam KK. Intraoperative applications of topical corticosteroid therapy for chronic rhinosinusitis. Ear Nose Throat J. 2021;100(5):320-328. doi:10.1177/0145561320970100
- Nasal polyps. American Academy of Allergy, Asthma, & Immunology (AAAAI). Reviewed June 28, 2019. Accessed July 8, 2022. https://www.aaaai.org/conditions-and-treatments/library/allergy-library/nasal-polyps
- Smith TL, Sautter NB. Is montelukast indicated for treatment of chronic rhinosinusitis with polyposis? Laryngoscope. 2014;124(8):1735-1736. doi:10.1002/lary.24477
- Martinez-Devesa P, Patiar S. Oral steroids for nasal polyps. Cochrane Database Syst Rev. 2011;(7):CD005232. doi:10.1002/14651858.CD005232.pub3
- Kirtsreesakul V, Wongsritrang K, Ruttanaphol S. Clinical efficacy of a short course of systemic steroids in nasal polyposis. Rhinology. 2011;49(5):525-532. doi: 10.4193/Rhino11.140
- Ta NH. Will we ever cure nasal polyps? Ann R Coll Surg Engl. 2019;101(1):35-39. doi:10.1308/rcsann.2018.0149
- Ernst FR, Imhoff RJ, DeConde A, Manes RP. Budget impact of a steroid-eluting sinus implant versus sinus surgery for adult chronic sinusitis patients with nasal polyps. J Manag Care Spec Pharm. 2019;25(8):941-950. doi:10.18553/jmcp.2019.18285
- Benninger MS, Sindwani R, Holy CE, Hopkins C. Impact of medically recalcitrant chronic rhinosinusitis on incidence of asthma. Int Forum Allergy Rhinol. 2016;6(2):124-129. doi:10.1002/alr.21652
- DeConde AS, Mace JC, Levy JM, et al. Prevalence of polyp recurrence after endoscopic sinus surgery for chronic rhinosinusitis with nasal polyposis. Laryngoscope. 2017;127(3):550-555. doi:10.1002/lary.26391
- Van Zele T, Gevaert P, Holtappels G, et al. Oral steroids and doxycycline: two different approaches to treat nasal polyps. J Allergy Clin Immunol. 2010;125(5):1069-1076. doi:10.1016/j.jaci.2010.02.020
- Ou J, Wang J, Xu Y, et al. Staphylococcus aureus superantigens are associated with chronic rhinosinusitis with nasal polyps: a meta-analysis. Eur Arch Otorhinolaryngol. 2014;271:2729-2736. doi: 10.1007/s00405-014-2955-0
- Laidlaw TM, Buchheit KM. Biologics in chronic rhinosinusitis with nasal polyposis. Ann Allergy Asthma Immunol. 2020;124(4):326-332. doi:10.1016/j.anai.2019.12.001
- Han JK, Bosso JV, Cho SH, et al. Multidisciplinary consensus on a stepwise treatment algorithm for management of chronic rhinosinusitis with nasal polyps. Int Forum Allergy Rhinol. 2021;11(10):1407-1416. doi:10.1002/alr.22851
- Dupixent (dupilumab) prescribing information. sanofi-aventis US; June 2022.
- Bachert C, Han JK, Desrosiers M, et al. Efficacy and safety of dupilumab in patients with severe chronic rhinosinusitis with nasal polyps (LIBERTY NP SINUS-24 and LIBERTY NP SINUS-52): results from two multicentre, randomised, double-blind, placebo-controlled, parallel-group phase 3 trials [published correction appears in Lancet. 2019;394(10209):1618]. Lancet. 2019;394(10209):1638-1650. doi:10.1016/S0140-6736(19)31881-1
- SINUS-24 trial results. Trial Site News. February 25, 2019. Accessed July 7, 2022. https://trialsitenews.com/sinus-24-trial-results/
- Gevaert P, Omachi TA, Corren J, et al. Efficacy and safety of omalizumab in nasal polyposis: 2 randomized phase 3 trials [published correction appears in J Allergy Clin Immunol. 2021;147(1):416]. J Allergy Clin Immunol. 2020;146(3):595-605. doi:10.1016/j.jaci.2020.05.032
- Xolair (omalizumab) prescribing information. Genentech USA, Inc; July 2021.
- Han JK, Bachert C, Fokkens W, et al. Mepolizumab for chronic rhinosinusitis with nasal polyps (SYNAPSE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Respir Med. 2021;9(10):1141-1153. doi:10.1016/S2213-2600(21)00097-7
- Harrison TW, Chanez P, Menzella F, et al. Onset of effect and impact on health-related quality of life, exacerbation rate, lung function, and nasal polyposis symptoms for patients with severe eosinophilic asthma treated with benralizumab (ANDHI): a randomised, controlled, phase 3b trial [published correction appears in Lancet Respir Med. 2021;9(3):e29]. Lancet Respir Med. 2021;9(3):260-274. doi:10.1016/S2213-2600(20)30414-8
- Tezspire (tezepelumab-ekko) prescribing information. Amgen Inc; December 2021.
- ‘Asthma of the nose’—tackling allergic rhinitis and its symptoms. The Medical Independent. March 14, 2017.
- Cafasso J. How to do a sinus flush at home. Healthline. January 28, 2019. Accessed July 5, 2022. https://www.healthline.com/health/sinus-flush#how-to
- Head K, Chong LY, Hopkins C, et al. Short-course oral steroids alone for chronic rhinosinusitis. Cochrane Database Syst Rev. 2016;4(4):CD011991. doi:10.1002/14651858.CD011991.pub2
- Head K, Chong LY, Hopkins C, et al. Short-course oral steroids as an adjunct therapy for chronic rhinosinusitis. Cochrane Database Syst Rev. 2016;4(4):CD0011992. doi:10.1002/14651858.CD011992.pub2
- Matsumoto H, Ishihara K, Hasegawa T, et al. Effects of inhaled corticosteroid and short courses of oral corticosteroids on bone mineral density in asthmatic patients: a 4-year longitudinal study. Chest. 2001;120(5):1468-1473. doi:10.1378/chest.120.5.1468
- Nucala (mepolizumab) prescribing information. GlaxoSmithKline; January 2022.
- Patel GB, Peters AT. The role of biologics in chronic rhinosinusitis with nasal polyps. Ear Nose Throat J. 2021;100(1):44-47. doi:10.1177/0145561320964653
- Nasal polyps. Mayo Clinic. Accessed July 5, 2022. https://www.mayoclinic.org/diseases-conditions/nasal-polyps/symptoms-causes/syc-20351888
Back to Top