
Expired activity
Please go to the PowerPak
homepage and select a course.
Practice Standards for Immunizing Adults in the Community Pharmacy
INTRODUCTION
It is an exciting time to be a pharmacy technician and the landscape is quickly changing for technician involvement in the vaccination process. The Department of Health and Human Services (HHS) recently expanded its guidance allowing pharmacy technicians to administer COVID-19 tests, COVID-19 vaccinations, and pediatric immunizations to patients 3 years of age and older.1 Technicians are now included in the Public Readiness and Emergency Preparedness (PREP) Act’s liability waiver, which provides immunity from liability to anyone who administers vaccines. Pursuant to the PREP Act, HHS now allows qualified pharmacy technicians across the country to administer pediatric and COVID-19 immunizations and COVID-19 tests under a qualified pharmacist’s supervision, provided they meet several requirements (Table 1). This new authority is time-limited to the COVID-19 public health emergency. It is unclear if Congress will extend it past the current health emergency.1
| Table 1. Immunization Requirements for Pharmacy Technicians1 |
| Requirement |
| Licensed and/or registered in accordance with state requirements (if state requirements exist) |
| Certified Pharmacy Technician (CPhT) certification from either the Pharmacy Technician Certification Board or National Healthcareer Association (in states with no state licensure or registration requirements) |
| Completion of a training program approved by the Accreditation Council for Pharmacy Education (ACPE), including hands-on injection technique and the recognition and treatment of emergency reactions to vaccines |
| Current certificate in basic cardiopulmonary resuscitation (CPR) |
| Completion of 2 hours of ACPE-approved, immunization-related continuing pharmacy education during the relevant state licensing period(s) |
Even if pharmacy technicians do not wish to administer vaccinations, technicians can provide integral support in several areas in the immunization process. Administering immunizations involves several processes, such as deciding whom to vaccinate, assessing vaccine contraindications and precautions, providing vaccine information statements, ensuring appropriate storage and handling of vaccines, and maintaining vaccine records. Pharmacists must fulfill certain responsibilities related to vaccination but pharmacy technicians will be greater assets if they understand and are aware of the vaccination process. This continuing education activity explores key areas where pharmacy technicians can assist pharmacists whether they have the appropriate credentials or personal desire to actively administer vaccinations or not.
APPROPRIATE VACCINE CANDIDATES
All health care providers should make every effort to ensure that adults receive all indicated vaccines as expeditiously as possible. When adults present at the pharmacy, the pharmacy technician is often the first point of contact. This provides a valuable opportunity to identify needed vaccinations according to the most current version of the adult immunization schedule. It may be helpful to have the Centers for Disease Control and Prevention (CDC) adult immunization schedule (found at https://www.cdc.gov/vaccines/schedules/hcp/imz/adult.html) on hand to review the recommended adult vaccinations. A more in-depth conversation will likely be necessary between patient and pharmacist, but the technician can serve as the first person to identify and educate a patient on vaccinations that would be appropriate for them to receive.
Assessing Contraindication and Precautions
Before vaccination, all patients should be screened for contraindications and precautions. A contraindication is a condition that increases the risk of a serious adverse reaction to vaccination.2 A vaccine should not be administered if a contraindication is documented. For example, a history of an anaphylactic reaction to a dose of vaccine or to a vaccine component is a contraindication for further doses. Giving a live vaccine to a severely immunocompromised person is also considered a contraindication. Because of the theoretical risk to the fetus, pregnant women generally should not receive live attenuated virus vaccines, so pregnancy is a contraindication to live vaccines. In some cases (such as pregnancy), the contraindication may be temporary, and vaccinations can often be administered later when the condition leading to a contraindication no longer exists.
A precaution is a condition that might increase the risk for a serious adverse reaction, cause diagnostic confusion, or compromise the vaccine’s ability to produce immunity.2 A precaution exists when a person might experience a more severe reaction to the vaccine than would have otherwise been expected; however, the risk for a reaction is lower than the risk expected with a contraindication. Immunizers can vaccinate people who have mild illnesses safely, and mild illnesses are not considered a precaution for immunization.3 However, the presence of a moderate or severe acute illness with or without a fever is a precaution for all vaccines. The immunizer should defer vaccination until the acute illness has improved.2 This precaution avoids causing diagnostic confusion between the underlying illness’s manifestations and the vaccine’s possible adverse effects or superimposing the vaccine’s potential adverse effects on the underlying illness.
In general, vaccinations should be deferred when a precaution is present. However, a vaccination might be indicated in the presence of a precaution if the vaccine’s protection benefit outweighs the risk for an adverse reaction. For example, among people whose adherence to medical care is questionable, it would be necessary to weigh the benefits and risks of vaccinating in lieu of deferral. In this case, it would be up to the pharmacist or primary care provider to decide if vaccination’s benefits outweigh the estimated risk of an adverse event. The provider may decide to vaccinate the patient despite the precaution. Table 2 lists the contraindications and precautions for common adult vaccines.
| Table 2. Contraindications and Precautions for Commonly Used Vaccines in Adults2,4,5 |
| Vaccine |
Contraindication |
Precaution |
| All vaccines |
· History of anaphylactic reaction to a dose of vaccine or to a vaccine component
|
· Moderate or severe acute illness with or without fever
|
| Tetanus, diphtheria, pertussis (Tdap); Tetanus, diphtheria (Td) |
· History of encephalopathy within 7 days of a vaccine containing tetanus or diphtheria toxoid or acellular pertussis
· History of severe reaction to latex (Tdap;Td)
|
· Guillain-Barré Syndrome within 6 weeks after a previous dose of tetanus toxoid-containing vaccine
· History of Arthus-type hypersensitivity reactions after a previous dose of tetanus or diphtheria toxoid-containing vaccine
· Progressive or unstable neurologic disorder, uncontrolled seizures, or progressive encephalopathy (Tdap)
|
| Measles, mumps, rubella (MMR) |
· Severe immunodeficiency
· Pregnancy
· History of immediate hypersensitivity to gelatin or neomycin
|
· Recent receipt of blood product containing antibodies
· History of thrombocytopenia or thrombocytopenic purpura
|
| Human papillomavirus (HPV) |
· Hypersensitivity to yeast
|
· Pregnancy
|
| Varicella |
· Severe immunodeficiency
· Pregnancy
· History of immediate hypersensitivity to gelatin or neomycin
|
· Recent receipt of blood product containing antibodies
· Receipt of specific antivirals (i.e., acyclovir, famciclovir, or valacyclovir) 24 hours before vaccination
|
| Influenza, inactivated injectable |
· Severe egg allergya
|
· Guillain-Barré Syndrome within 6 weeks of previous influenza vaccination
|
| Influenza, live attenuated nasal spray |
· Severe egg allergya
· Pregnancy
· Receipt of zanamivir or oseltamivir within the previous 48 hours, peramivir within 5 days, or baloxavir within 17 days
· Immunocompromised or close contacts with severely immunosuppressed people who require a protective environment
|
· Guillain-Barré Syndrome within 6 weeks of previous influenza vaccination
· Medical conditions that might predispose to higher risk of complications attributable to influenzab
|
| Recombinant zoster vaccine (RZV) |
· History of immediate hypersensitivity to gelatin or neomycin
|
· Pregnancy and lactation
|
| Pneumococcal: polysaccharide (PPSV23), conjugate (PCV13) |
· Hypersensitivity to yeast (PCV 13)
|
· None other than listed for all vaccines
|
| Hepatitis A (HepA) |
· History of severe reaction to latex
|
· None other than listed for all vaccines
|
| Hepatitis B (HepB) |
· History of severe reaction to latex
· Hypersensitivity to yeast
|
· None other than listed for all vaccines
|
| Meningococcal (MenACWY; MenB) |
· History of severe reaction to latex (MenB)
|
· Pregnancy (MenB)
|
aHistory of severe allergic reaction (e.g., anaphylaxis) to egg is a labeled contraindication to the use of inactivated influenza vaccine and live attenuated influenza vaccine. However, CDC’s Advisory Committee on Immunization Practices recommends that the vaccine may be administered in a medical setting, under the supervision of a health care provider who is able to recognize and manage severe allergic conditions.
bCertain chronic medical conditions such as diabetes mellitus, chronic pulmonary diseases (including asthma), chronic cardiovascular diseases (except hypertension), renal, hepatic, neurologic/neuromuscular, hematologic, or metabolic disorders might predispose an individual to a higher risk of complications attributable to influenza. |
History of Immediate Hypersensitivity
A severe allergic reaction (e.g., anaphylaxis) to a previous dose of a vaccine or to one of its components is a contraindication to vaccination. While most vaccines have many components, substances to which individuals are most likely to have had a severe allergic reaction include egg protein, gelatin, neomycin, and yeast.6 People having an allergic reaction to any of these components should consider evaluation by an allergist. However, a previous severe allergic reaction to any vaccine is a contraindication for future receipt of the vaccine regardless of a dermatologic consult.
In addition to the various vaccine components already listed, a severe anaphylactic reaction to latex is a contraindication to receiving certain vaccines. Although latex is not a vaccine component, some vaccines are supplied in vials or syringes that contain latex. These products are either made from natural rubber latex or synthetic rubber latex.6 Natural rubber latex contains plant proteins that can cause immediate-type allergic reactions, but synthetic rubber latex does not contain the latex proteins linked to immediate-type allergic reactions.6 Syringe plungers and vial stoppers may be made of both types of latex. The manufacturer generally notes the type of latex used in vaccine packaging in their package inserts. If a person reports a previous severe anaphylactic allergy to latex, vaccines supplied in vials or syringes that contain natural rubber latex should be avoided. Table 2 lists the vaccines that contain egg protein, gelatin, neomycin, yeast, and latex.
Pregnancy
According to CDC guidelines, live-virus vaccines are contraindicated during pregnancy because of the hypothetical risk that the vaccine virus can replicate and cause infection or have other adverse effects on the fetus. Two inactivated vaccines, Tdap vaccine and inactivated influenza vaccine, are routinely recommended for pregnant women in the United States (U.S.).7 Tdap vaccine is recommended during each pregnancy, regardless of prior vaccination status, to prevent pertussis in neonates.5 Annual influenza vaccination is recommended for all people 6 months of age and older, regardless of pregnancy status.
Immunosuppression
Immunocompetence, the ability of the body to produce a normal immune response, is a concern if it is impaired. Altered immunocompetence can be classified as primary or secondary.7 Primary immunodeficiencies generally are inherited and secondary immunodeficiency is acquired and occurs as a result of a disease process or its therapy.8 Examples of secondary immunodeficiency include HIV infection, malignancies, radiation treatment, and treatment with immunosuppressive drugs. The degree to which immunosuppressive drugs cause clinically significant immunodeficiency generally is dose related and varies by drug.
Live virus vaccines elicit an immune response by prompting the recipient’s immune system to respond to replication of the attenuated (weakened) vaccine virus. In people with compromised immune function, a virus has the potential to replicate and could lead to infection with the virus. For this reason, live virus vaccines are contraindicated for people with severe immunosuppression. Inactivated vaccines might also best be deferred during a period of altered immunocompetence because the individual may not be able to mount a response. In this case, the concern is effectiveness, not safety. Additionally, if an inactivated vaccine is administered during a period of altered immunocompetence, it might need to be readministered after immune function has improved.8 Table 2 also lists vaccines that are contraindicated in people with a compromised immune system.
VACCINE ADMINISTRATION
Intramuscular and Subcutaneous Administration Techniques
Most parenteral vaccines recommended for routine administration to adults in the U.S. are given by either the intramuscular (IM) or the subcutaneous route. An exception is the live influenza virus vaccine which is administered by the intranasal route. Table 3 lists the vaccines administered by IM or subcutaneous routes.
| Table 3. Vaccines Administered by IM versus Subcutaneous Route9 |
| IM Administration |
Subcutaneous Administration |
| Hepatitis A (HepA) |
Pneumococcal: polysaccharide (PPSV23)a |
| Hepatitis B (HepB) |
Varicella |
| Influenza vaccine, injectable |
Measles, mumps, rubella (MMR) |
| Human papillomavirus (HPV) |
|
| Meningococcal (MenACWY; MenB) |
|
| Pneumococcal: polysaccharide (PPSV23)a, conjugate (PCV13) |
|
| Tetanus, diphtheria, pertussis (Tdap); Tetanus, diphtheria (Td) |
|
| Recombinant zoster vaccine (RZV) |
|
| a Can be given both IM and subcutaneously |
An IM injection is given in the arm at the central and thickest portion of the deltoid muscle above the level of the armpit and approximately 2" below the acromion process.9 The acromion process is a bony structure that sits on the top of the scapula or shoulder blade and above the deltoid muscle. The deltoid muscle forms an upside-down triangle that starts at the acromion process with the point of the triangle at the level of the armpit. The injection should go in the center of the triangle. A good way to measure 2” is to measure 2-3 fingerbreadths below the bottom of the acromion process. To give an IM injection, the immunizer should uncover the upper arm and swab it with alcohol and allowed it to dry. At the site of injection, the immunizer stretches the muscle around the spot with the thumb and index finger. With a quick firm thrust, he or she will insert the needle into the muscle straight at a 90° angle. After pushing the vaccine out of the syringe, it’s critical to pull the needle out at exactly the same angle. If 2 separate injections are to be given, they must be separate by a minimum of 1” in the same deltoid muscle or injected in different arms. The correct needle size for an IM injection is a 22–25 gauge with a 1–1½" needle.9
The injection site for a subcutaneous injection is the fatty tissue over the triceps.9 Injection sites are located on the back of the upper arm. Before injecting, the immunizer should cleanse the site with alcohol and allow it to dry. The immunizer will pinch the injection site between the index finger and thumb to ensure medication goes into the fatty tissue and to prevent injection into the muscle. In this technique, immunizers insert the needle at a 45° angle to the skin. After pushing the vaccine out of the syringe, they pull the needle out at exactly the same angle. On the very rare occasion that a patient needs 2 injections in the same area, they will separate them by a minimum of 1". The correct needle size for a subcutaneous injection is a 23–25 gauge with a 5/8" needle.9
Syncope Precautions
Syncope (fainting) may follow vaccination, especially in adolescents and young adults. In 2005, the Vaccine Adverse Event Reporting System (VAERS) began detecting a trend of increasing syncope reports that coincided with the licensure of 3 vaccines for adolescents: human papillomavirus (HPV), meningococcal conjugate or MenACWY, and Tdap.10 The risk for serious secondary injuries, including skull fracture and cerebral hemorrhage, are of particular concern and such injuries have been documented. Many falls due to fainting can be prevented by having the patient sit or lie down during vaccination and experts recommend this precaution be taken during vaccine administration. Since most reported syncope reactions occur within 15 minutes of vaccine administration, pharmacy staff should observe patients for 15 minutes after vaccination.10 Patients who faint after vaccination generally recover within a few minutes. If a patient faints after a vaccination, the pharmacist should observe until the patient regains consciousness so that further treatment needs can be determined. If the patient does not recover immediately, pharmacy staff should call local emergency medical services.10
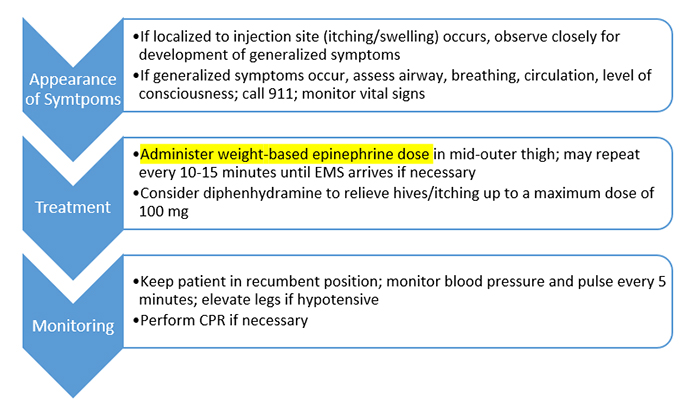
Anaphylaxis Precautions
Vaccine providers should know how to recognize allergic reactions, including anaphylaxis, a rare complication of vaccination. Pharmacies need to have and rehearse a plan to handle anaphylaxis and ensure supplies are available. Table 4 lists signs and symptoms of anaphylaxis and Table 5 lists select emergency supplies that should be available in community settings. Figure 1 shows the emergency medical protocol for handling anaphylactic reactions in adults that is recommended by the Immunization Action Coalition, an organization that works in conjunction with CDC to educate health care professionals about vaccine safety and efficacy.
| Table 4. Signs and Symptoms of Anaphylaxis11 |
| Organ System |
Signs/Symptoms |
| Skin |
Hives, itching, flushing |
| Mucosal |
Swelling of lips, face, throat, eyes |
| Respiratory |
Nasal congestion, change in voice, sensation of throat closing, shortness of breath, wheezing, cough |
| Gastrointestinal |
Nausea, vomiting, diarrhea, cramping abdominal pain |
| Cardiovascular |
Fainting, dizziness, tachycardia, hypotension |
| Table 5. Supplies for Managing Anaphylaxis in a Community Setting11 |
| Medication |
Additional Supplies |
| Epinephrine in prefilled autoinjector or prefilled syringe (0.3 mg); at least 3 doses should be available onsite |
Blood pressure measuring device/stethoscope with adult-sized and extra-large cuffs |
| Diphenhydramine oral, 12.5 mg/5 mL liquid; 25 or 50 mg tabletsa |
Tongue depressors |
| |
Light with extra batteries (for examination of the mouth and throat) |
| |
A timing device for checking pulse |
| |
Cell phone or access to onsite phone |
| aDiphenhydramine relieves itching and hives only; it will not relieve upper or lower airway obstruction, hypotension, or shock. |
| Figure 1. Emergency Protocol for Management of Anaphylactic Reactions in a Community Setting11 |
 |
After every anaphylactic reaction that occurs, the pharmacist should notify the patient’s primary care physician and report the incident to VAERS.11 Two recent CDC safety studies confirmed post-vaccination anaphylaxis is rare. In a 25-year review of VAERS data , reports of anaphylaxis among adults most often followed influenza vaccine. In a Vaccine Safety Datalink study, the estimated incidence of anaphylaxis was 1.3 per million vaccine doses administered for all vaccines and 1.6 per million doses for IIV3 (trivalent) influenza vaccine.12 While the risk of anaphylaxis is considered very low, every pharmacy that administers vaccinations must have an emergency plan and proper supplies in case an anaphylactic reaction occurs.
REQUIRED DOCUMENTATION
The National Childhood Injury Act of 1986 created the National Vaccine Injury Compensation Program (VICP). The VICP was established after lawsuits against vaccine manufacturers and health care providers threatened to cause vaccine shortages and reduce vaccination rates.13 To protect vaccine manufacturers and health care providers, the government enacted this legislation. The VICP is a no-fault alternative to the traditional legal system for resolving vaccine injury petitions and offers no-fault compensation to patients if injury occurs. This program applies to any routinely recommended childhood vaccination, even if many or most doses of the vaccine are administered to adults (e.g., influenza vaccine). The National Childhood Vaccine Injury Act require health care providers who administer vaccines covered by VICP to document vaccinations appropriately and maintain a system of permanent recordkeeping. The VICP requires the following documentation14:
- Date vaccine administered
- Vaccine manufacturer
- Vaccine lot number
- Name, address, and title of person administering the vaccine
- Edition date printed on the Vaccine Information Sheet (VIS)
- Date the VIS is given to the patient or the patient’s legal representative
The Advisory Committee on Immunization Practices (ACIP), medical and public health experts that make vaccine recommendations to CDC, recommends keeping this information for all vaccines, not just for those required by the Act.14 It is also wise to document the vaccine injection site and while a signature or signed consent is not required by federal law, it is a good idea to obtain some form of acknowledgment that the patient received the VIS and were asked if they had any questions. The pharmacy’s computer system may be able to document this signature at the time payment is collected or as part of the prescription process.
Immunization information systems (IISs; formerly called immunization registries) are confidential, population-based, computerized information systems that collect and consolidate vaccination data from multiple health care providers within a geographic area.15 These systems are critical tools that can increase and sustain vaccination coverage by consolidating vaccination records from multiple providers and assessing vaccination coverage within a defined geographic area. Most IISs have additional capabilities, such as vaccine management, adverse event reporting, maintenance of birth-to-death vaccination histories, and interoperability with other health information systems. These systems can provide CDC with accurate data to make informed vaccination decisions. Providers should be aware of state and/or regional immunization information systems and reporting requirements.
VACCINE ADVERSE EVENT REPORTING
Before FDA licenses vaccines, it requires vaccine evaluation in 3 phases of clinical trials. Small phase 1 trials provide the first safety evaluation to identify common adverse events. In phase 2 trials, the vaccine is given to people who have characteristics like those for whom the new vaccine is intended. Vaccines that appear promising are evaluated in phase 3 trials, which typically involve several hundred to several thousand volunteers and are generally designed to demonstrate vaccine efficacy and provide additional information on vaccine safety.16 Although FDA requires extensive studies for licensure of new vaccines, post-marketing research and surveillance identify safety issues that may only be detected following vaccination of a much larger, more diverse population. After licensure, several mechanisms assess a vaccine’s safety including VAERS and the Vaccine Safety Datalink project.
Vaccine Adverse Event Reporting System
CDC and FDA manage VAERS—a safety surveillance system that collects reports of adverse events associated with vaccines currently licensed in the U.S.—jointly.17 It accepts reports of adverse events that may be associated with licensed vaccines from health care providers, manufacturers, and the public. FDA and CDC continually monitor VAERS reports for any unexpected patterns or changes in adverse event rates. The report of an adverse event to VAERS is not proof that a vaccine caused the event. It is usually impossible to determine whether an adverse event resulted from a concurrent condition or from a vaccination from VAERS data alone even when the event occurs soon after vaccination. However, CDC and FDA encourage reporting of adverse events whether it is the provider’s belief that the vaccination was the cause or not. If VAERS data suggests a possible link between an adverse event and vaccination, CDC and FDA personnel may study the relationship further in a controlled fashion.17
In addition to analyzing individual reports, CDC and FDA also analyze patterns of reporting associated with vaccine lots. Many complex factors are important when comparing different vaccine lots. Larger lots may generate more reports as opposed to smaller lots simply because more people will be vaccinated with doses from larger lots. Similarly, if a lot that has been in use for a long time, it is more likely to be associated with reports than newer lots. CDC and FDA analyze the data continually to look for lots associated with death reports or more serious adverse effects than would be expected based on such factors as time in use and chance variation. If they detect such a lot, they investigate further to determine if the lot is safe for use, or if additional FDA actions are needed.17
There are 2 ways to submit a report to VAERS: (1) online reporting or (2) downloading a PDF and then uploading the completed form. The online submission is the preferred option and can be accessed at https://vaers.hhs.gov/esub/index.jsp. The VAERS form asks for the following information18 :
- type of vaccine received
- the timing of vaccination
- the adverse event’s time of onset
- recipient’s current illnesses or medications, history of adverse events following vaccination, allergies to medications, food or other products, and demographic characteristics
A reportable events table lists conditions believed to be caused by vaccines and is available at https://vaers.hhs.gov/docs/VAERS_Table_of_Reportable_Events_Following_Vaccination.pdf. Health care providers are required by law to report any conditions on the table to VAERS and are strongly encouraged to report clinically significant or unexpected events following vaccination.18
Vaccine Safety Datalink
While VAERS provides useful information on vaccine safety, this passive reporting system has important limitations. Events following vaccination are merely reported; the system cannot assess whether a given type of event occurs more often than expected after vaccination. A second limitation is that event reporting is incomplete and biased toward events believed to be more likely to be due to vaccination and that occur relatively soon after vaccination. To obtain more systematic information on adverse events, the Vaccine Safety Datalink (VSD) project was initiated in 1990.19 Directed by CDC, this project includes 9 managed-care organizations across the country. Member databases include information on immunizations, medical conditions, demographics, laboratory results, and prescription medications. The VSD objectives include conducting safety studies suggested by the medical literature or VAERS, monitoring adverse events from new vaccines or subsequent to new vaccine recommendations, and providing information for making national vaccine recommendations.19
STORAGE AND HANDLING
Failure to store and handle vaccines properly can result in a significant financial burden to the pharmacy. Perhaps more importantly from a patient perspective, administration of improperly-stored vaccines may elicit an inadequate immune response resulting in ineffective vaccination. To improve the standard of vaccine storage and handling practices, CDC has published detailed guidance to be used by all vaccine providers.19 The following section discusses these recommendations.
Vaccine Cold Chain
A cold chain is a temperature-controlled supply chain that includes all vaccine-related equipment and procedures. The cold chain begins with the cold storage unit at the manufacturing plant, extends to the transport and delivery of the vaccine and correct storage at the provider facility, and ends with administration of the vaccine to the patient.20 Vaccines must be stored properly from the time they are manufactured to the time they are administered. A single break in the chain means an irreversible loss of potency. ACIP’s general best practice recommendations state that if a vaccine is exposed to inappropriate temperatures and inadvertently given to a patient, the vaccine must be repeated.14 This means extra doses for the patients and an increased cost to providers.
Storage and Temperature Monitoring Equipment
The pharmacy must have and maintain proper storage and monitoring equipment appropriately. CDC recommends using purpose-built or pharmaceutical-grade units designed specifically to either refrigerate or freeze vaccines. These purpose-built units have microprocessor-based temperature controls with digital thermometers and fan-forced air circulation or multiple cool air vents to maintain uniform temperatures. They are specifically designed for fast recovery from an out-of-range temperature.20 A household-grade unit can be an acceptable alternative to pharmaceutical-grade vaccine storage units but only for refrigerated vaccines. If a household-grade unit is used, a separate freezer unit is necessary for frozen vaccines. Vaccines should never be stored in a dormitory-style or bar-style combined refrigerator/freezer unit under any circumstances.
Refrigerators should maintain temperatures between 36°F and 46°F and freezers should maintain temperatures between -58°F and +5°F.20 CDC recommends a specific temperature monitoring device called a “digital data logger” (DDL).20 A DDL provides the most accurate storage unit temperature information including details on how long a unit has operated outside the recommended temperature range. Temperature monitoring devices can experience a drift over time and CDC recommends calibrating a DDL every 2 to 3 years or according to the manufacturer’s specifications to ensure the device is still functioning properly.20 Pharmacy staff should monitor and record temperatures at the start and end of each workday and keep records for 3 years in a readily retrievable file. They should record the following information:
- Minimum/maximum temperature
- Date
- Time
- Name of person who checked and recorded the temperature
- Actions taken if a temperature excursion occurred
Quick Tip: Post “DO NOT UNPLUG” warning signs at outlets and label fuses and circuit breakers to alert people not to turn off power to a storage unit.
Organizing and Storing Vaccine
To confirm vaccines are stored correctly and to minimize the risk of administration errors, CDC recommends the following best practices20:
- Store each type of vaccine or diluent in its original packaging
- Position vaccines and diluents 2 to 3 inches from the unit’s walls, ceiling, floor, and door
- Avoid storing similar named products or adult and pediatric vaccines on the same shelf
- Store diluent with the corresponding refrigerated vaccine
- If other medications and biologics must be stored in the same unit as vaccines, mark them clearly marked and store them in separate containers
- Arrange vaccines and diluents in rows and allow space between them to promote air circulation
Quick Tip: Food and beverages should never be stored in the unit with vaccines.
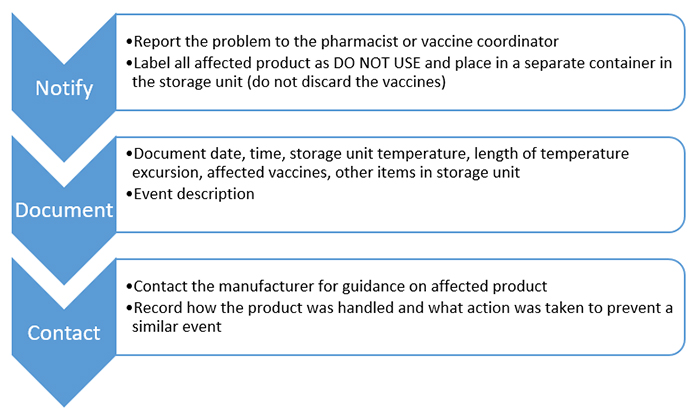
Handling a Temperature Excursion
Any temperature reading outside ranges recommended in the manufacturer’s package inserts is considered a temperature excursion.20 Pharmacy staff should follow this CDC recommended action plan immediately after a temperature excursion occurs (Figure 2).
| Figure 2. Steps for Handling a Temperature Excursion20 |
 |
Quick Tip: If the temperature alarm sounds repeatedly, first do basic checks of the unit door, power supply, and thermostat settings. Consider contacting a repair technician to determine the need for repair or replacement.
Vaccine Preparation
Vaccine preparation is the final step in the cold chain prior to administration. Vaccines should only be drawn up at the time of administration and prepared in a designated area away from any space that could lead to contamination of the vaccine product. If vaccines must be drawn up in advance, best practice states that each person administering vaccines should draw up no more than 1 multi-dose vial or 10 doses at one time and store them at the recommended temperatures.20 Any remaining pre-drawn syringes should be discarded at the end of the workday. As an alternative to pre-drawing vaccines, pharmacies can consider using manufacturer-filled syringes that are prepared and sealed under sterile conditions at the point of manufacture.
Vaccines can be supplied in single-dose vials or multidose vials. Single-dose vial do not contain preservatives and should never be used more than once. Multidose vials can be entered or punctured more than once because they contain a preservative to prevent microorganism growth. Only the number of doses indicated in the manufacturer’s package insert should be withdrawn from the vial. After the maximum number of doses has been withdrawn, the vial should be discarded, even if there is residual vaccine or the expiration date has not been reached. It is never recommended to use partial doses from 2 different vials to obtain a single lots of a vaccine. Some vaccines need to be reconstituted before administration and the manufacturer usually supplies a a diluent. Diluents are specifically designed for each vaccine and are designed to meet the volume, pH balance, and chemical requirements of their corresponding vaccines.19 Diluents should never be substituted for one another and even if the supplied diluent is sterile water or saline, use only the diluent supplied with the vaccine to reconstitute it.
Quick Tip: Always check expiration dates on both diluents and vaccines before reconstituting them.
CDC recommends designating a vaccine coordinator responsible for ensuring all vaccines are stored and handled correctly and supervising the pharmacy’s storage and handling operating procedures. The coordinator’s responsibilities would include things such as managing inventory, organizing storage units, tracking temperature monitoring devices, responding to temperature excursions, maintaining required documentation, and training staff. This is an excellent position to be filled by a pharmacy technician who has appropriate training.
CONCLUSION
Proper vaccine administration is critical to ensure that vaccinations are safe and effective. This begins with appropriate patient assessment to determine what vaccines are required and possible precautions or contraindications. The pharmacy technician can begin this process by assessing vaccination history and using CDC adult immunization schedules to determine what the patient immunization gaps. In addition, technicians can begin to gather the necessary information to identify contraindications or precautions such as a history of immediate hypersensitivity to any vaccine or the presence of allergies to egg protein, gelatin, neomycin, yeast, or latex. Technicians can also screen for pregnancy. The pharmacist will then be able to use this information to decide if the patient is an appropriate candidate for vaccination.
Some pharmacy technicians decide not to become certified to administer vaccines. Regardless, technicians can be valuable participants in many steps in the immunization process. These designated tasks may include vaccine dose preparation, proper storage and inventory maintenance, and assisting with VCIP-required documentation and other record keeping. Pharmacy technicians can provide integral support, streamline workflow, and increase operational and technologic oversight of pharmacy-administered vaccinations to ultimately improve the patient care process related to immunizations.
REFERENCES
- American Society of Health-System Pharmacists. HHS Authorizes Pharmacy Technician and Pharmacy Intern Administration of COVID-19 Tests and Vaccines. Accessed March 22, 2021. https://www.ashp.org/Advocacy-and-Issues/Key-Issues/Other-Issues/HHS-Authorizes-Pharmacy-Tech-and-Intern-Administration-of-COVID-19-Tests-and-Vaccines?loginreturnUrl=SSOCheckOnly
- General Best Practice Guidelines for Immunization: Best Practices Guidance of the Advisory Committee on Immunization Practices (ACIP). Contraindications and Precautions. Centers for Disease Control and Prevention. Accessed March 23, 2021. https://www.cdc.gov/vaccines/hcp/acip-recs/general-recs/contraindications.html
- Halsey N, Boulos R, Mode F, et al. Response to measles vaccine in Haitian infants 6 to 12 months old. Influence of maternal antibodies, malnutrition, and concurrent illnesses. N Engl J Med. 1985;313(9):544-549.
- Guide to contraindications and precautions to commonly used vaccines in adults. Immunization Action Coalition. Accessed March 23, 2021. https://immunize.org/catg.d/p3072.pdf
- Latex in vaccine packaging. 2020. Centers for Disease Control and Prevention. Accessed March 23, 2021. https://www.cdc.gov/vaccines/pubs/pinkbook/downloads/appendices/b/latex-table.pdf
- General Best Practice Guidelines for Immunization: Best Practices Guidance of the Advisory Committee on Immunization Practices (ACIP). Preventing and Managing Adverse Reactions. Centers for Disease Control and Prevention. Accessed March 23, 2021. https://www.cdc.gov/vaccines/hcp/acip-recs/general-recs/adverse-reactions.html
- Vaccines during and after pregnancy. Centers for Disease Control and Prevention. Accessed March 23, 2021. https://www.cdc.gov/vaccines/pregnancy/vacc-during-after.html
- Altered immunocompetence. Centers for Disease Control and Prevention. Accessed March 23, 2021. https://www.cdc.gov/vaccines/hcp/acip-recs/general-recs/immunocompetence.html
- Immunization Action Coalition. How to administer intramuscular and subcutaneous vaccine injections to adults. Accessed March 23, 2021. https://www.immunize.org/catg.d/p2020a.pdf
- Syncope after vaccination—United States, January 2005-July 2007. MMWR Morb Mortal Wkly Rep. 2008;57(17):457-460.
- Medical management of vaccine reactions in adults in a community setting. Immunization Action Coalition. Accessed March 24, 2021. https://immunize.org/catg.d/p3082.pdf
- McNeil M. Vaccine-associated anaphylaxis. Curr Treat Options Allergy. 2019;6(3):297-308.
- About the National Vaccine Injury Compensation Program. Health Resources and Services Administration. Accessed April 14, 2021. https://www.hrsa.gov/vaccine-compensation/about/index.html.
- General Best Practice Guidelines for Immunization: Best Practices Guidance of the Advisory Committee on Immunization Practices (ACIP). Vaccination Records. Accessed March 24, 2021. Centers for Disease Control and Prevention. https://www.cdc.gov/vaccines/hcp/acip-recs/general-recs/records.html
- Murthy N, Rodgers L, Pabst L et al. Progress in childhood vaccination data in immunization Information systems–United States, 2013-2016.MMWR Morb Mortal Wkly Rep. 2017;66:1178-1181.
- Vaccine testing and approval process. Accessed March 25, 2021. Centers for Disease Control and Prevention. https://www.cdc.gov/vaccines/basics/test-approve.html
- Vaccine adverse events. U.S. Food and Drug Administration. Accessed March 24, 2021. https://www.fda.gov/vaccines-blood-biologics/report-problem-center-biologics-evaluation-research/vaccine-adverse-events
- Vaccine Adverse Event Reporting System (VAERS). Centers for Disease Control and Prevention. Accessed March 25, 2021. https://www.cdc.gov/vaccinesafety/ensuringsafety/monitoring/vaers/index.html.
- Vaccine Safety Datalink. Centers for Disease Control and Prevention. Accessed March 25, 2021. https://www.cdc.gov/vaccinesafety/ensuringsafety/monitoring/vsd/index.html.
- Vaccine storage and handling toolkit. 2021. Centers for Disease Control and Prevention. Accessed March 25, 2021. https://www.cdc.gov/vaccines/hcp/admin/storage/toolkit/storage-handling-toolkit.pdf.
Back to Top