
Expired activity
Please go to the PowerPak
homepage and select a course.
PHARMACIST’S GUIDE TO PATIENT SELF-MANAGEMENT OF HEART FAILURE
Addressing Adherence Challenges
BURDEN OF HEART FAILURE
Chronic heart failure is a largely self-managed disease with guidance and support provided by the heart failure team. The prevalence of chronic heart failure was 6.2 million in 2016 and is projected to increase by 46% by 2030.1 The total cost due to heart failure was estimated to be $31 billion in the United States in 2010 and is projected to increase to $70 billion by 2030.1 Of the approximately 1 million persons hospitalized with heart failure annually, nearly 30% of Medicare beneficiaries do not survive 1 year following hospitalization.1 These statistics make it clear that the magnitude of the support needed by patients with chronic heart failure is substantial and expected to increase.
Self-managing heart failure is an arduous, daily challenge faced by patients with chronic heart failure, which is often complicated by related comorbidities such as hypertension and type 2 diabetes mellitus. In addition to taking an average of 7 evidence-based medications, patients with heart failure may face diet and fluid restrictions. Daily monitoring of body weight also is often necessary. Moreover, patients with chronic heart failure experience significant reduction in health-related quality of life, both in psychological and physical functioning.2,3 Thus, the burden of heart failure affects not only patients, but includes family and caregivers, and often friends and neighbors, as well.
A factor that contributes to the burden and suboptimal outcomes faced by patients with chronic heart failure is the under use of evidence-based medications. The CHAnge the Management of Patients with Heart Failure (CHAMP-HF) registry recently reported on the use of guideline-recommended pharmacotherapy in patients with heart failure with reduced ejection fraction (HFrEF), ie, left ventricular ejection fraction £40%.4 Analysis showed that one-quarter (26.3%) of patients did not have a contraindication to renin-angiotensin-aldosterone (RAAS) inhibitor therapy, but were not treated with an angiotensin converting enzyme (ACE) inhibitor, angiotensin receptor blocker (ARB), or angiotensin receptor-neprilysin inhibitor (ARNI). Under utilization of beta-blocker and mineralocorticoid receptor antagonist (MRA) therapy also was observed, with 33% and 66%, respectively, of those without a contraindication not receiving therapy. Furthermore, among eligible patients who received evidence-based pharmacotherapy, few received the recommended doses. For example, 10.4% of eligible patients received an ACE inhibitor or ARB at the recommended dose, 1.8% an ARNI, 18.4% a beta-blocker, and 25.2% an MRA.
The CHAMP-HF results support that frequent hospital admissions and poor health-related quality of life in many patients with HFrEF is due to suboptimal use of evidence-based therapies as recommended in current guidelines.5 Suboptimal use includes lack of prescribing recommended classes of medications and targeted doses. Extensive evidence shows that the use of ACE inhibitors, ARBs, beta-blockers, and MRAs at appropriate doses results in significant reductions in the 1-year mortality rates in patients with HFrEF, with added benefit when used in combination.6-11For example, the Randomized Aldactone Evaluation Study (RALES) trial showed that the addition of the aldosterone antagonist (AA) spironolactone to an ACE inhibitor reduced the risk of death 30%.10 The addition of the beta-blocker carvedilol to the combination of an ACE inhibitor and AA reduced the risk of death 35%.11
OPTIMIZING PHARMACOTHERAPY FOR HFrEF
Recognizing that many treatment gaps exist in the care provided to patients with HFrEF , the American College of Cardiology published recommendations in 2018 regarding 10 pivotal issues related to HFrEF that remain unresolved in the 2017 ACC/AHA/HFSA Focused Update of the 2013 ACC/AHA Guideline for the Management of Heart Failure.5,12 These issues were identified by a multidisciplinary panel of heart failure stakeholders, including pharmacists.12
The Decision Pathway developed by the panel identified pharmacists as having an important role in addressing several of the 10 pivotal issues, all intended to optimize pharmacotherapy (Table 1). To achieve medication optimization across the spectrum of care, it is essential that pharmacists in different practice settings, who often perform specialized but complementary functions, collaborate with one another and other members of the heart failure team. Recommendations for collaboration between community pharmacy-based and clinic-based pharmacists to achieve medication optimization across the continuum of heart failure care were recently released by the American College of Clinical Pharmacy, the Community Pharmacy Enhanced Services Network USA, and the National Community Pharmacists Association Innovation Center.13 The four key recommendations are:
- Identify patients who are candidates for pharmacist-pharmacist collaboration
- Establish effective, secure modes of bidirectional communication
- Establish goals for pharmacist-pharmacist collaboration
- Promote shared trust, responsibility, and accountability
| Table 1. Role of the pharmacist on the heart failure team12 |
| Serve as a resource for the treating clinician and heart failure team |
| Oversee all of a patient’s medications |
| Optimize pharmacotherapy |
| Identify potential drug interactions |
| Perform medication synchronization and assess adherence |
| Provide education to improve patient adherence |
| Provide disease management programs |
| Ensure that vaccinations are current |
| Identify and navigate insurance coverage, patient assistance programs |
| Request medication price matching |
To facilitate collaboration and communication among pharmacists, a tool used at the Medical University of South Carolina is Rx Communication. This tool enables the pharmacist to enter information about the patient beginning at the time of hospital admission, irrespective of whether the patient is in the intensive care unit (ICU) or general floor. The tool also provides a mechanism for pharmacists to communicate with other pharmacists. When the patient transitions to a different unit, such as from the ICU to a general floor, the pharmacist on the general unit will see all of the information already entered. The pharmacist on the general unit continues to enter information, which is then passed on to the outpatient or community pharmacist when the patient is discharged. Sharing this information has fostered a collaborative relationship among pharmacists in different practice settings who provide care to that specific patient with heart failure. This has proved to be very helpful in optimizing care for these patients. Other benefits include:
- the ability to identify patients who may need additional education about their medications or the disease state itself.
- facilitating bidirectional communication so that the entire team understands and is working toward the same goals established for a specific patient.
|
Case Study #1
KD is a 59-year-old woman readmitted for symptoms of worsening heart failure over the past 3 days. She has been hospitalized 3 times over the past 13 months for similar episodes. The attending cardiologist asks you to provide a comprehensive medication review and provide your recommendations.
1. What do we want to look for in the medication review?
2. How can her risk for heart failure hospitalization be reduced?
|
Medication Therapy Review
According to the Centers for Medicare & Medicaid Services, a comprehensive medication review is14:
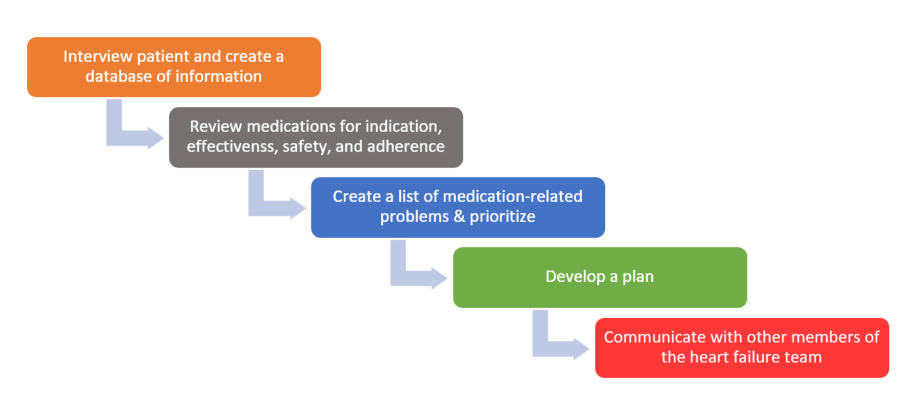
“a systematic process of collecting patient-specific information, assessing medication therapies to identity medication-related problems, developing a prioritized list of medication-related problems and creating a plan to resolve them with the patient, caregiver and/or the prescriber.”
One suggested stepwise approach to medication therapy review in collaboration with the patient while hospitalized is shown in Figure 1.14 There are several key points to keep in mind in conducting the medication therapy review. One is that active involvement of the patient is critical so that the patient’s medication history is clear and fully understood. Moreover, patients who are engaged in their treatment discussions and decisions are generally more willing and able to adhere to the treatment plan. The patient interview should be conducted in a quiet and private setting, if possible. In addition, a time for the interview should be scheduled in advance to occur at a time when the patient is not rushed so that they are able to focus and engage in the review. The patient should be invited to include a family member, caregiver, and/or other person(s) who might be involved in providing support to the patient.
|
Figure 1. Stepwise approach to medication therapy review14
|
Establishing a positive tone for collaboration at the beginning of the medication therapy review is essential and can be facilitated by offering the patient understanding and support. Identifying and resolving patient barriers and concerns is a key goal of the medication therapy review. Thus, assessing whether or not the patient is achieving the desired benefits from treatment, as well as experiencing side effects or other issues that might serve as a barrier to adherence is vital. One common barrier is affordability, so talking with the patient about affordability of medications is important. If the patient has not recently contacted their insurance provider, it can be helpful to submit a test claim to clarify current coverage and out-of-pocket cost. The community pharmacist might be contacted to identify if there’s a coupon card or assistance program such as through the state or manufacturer. The discussion about affordability also should include the goals of treatment and the expected benefits of each medication such as reduction in mortality and improved health-related quality of life as this will help the patient make a more informed decision.
If a treatment barrier is identified, the focus should be to collaborate with the patient to find a solution that is acceptable to the patient and that the patient is able to implement. Furthermore, patient agreement to the action plan is important. The medication therapy review also should determine if the patient is receiving medications and doses consistent with current guideline recommendations. Similarly, the medication therapy review is an opportune time to streamline the treatment plan and to eliminate medications that serve no clear purpose. In addition to talking with the heart failure team, this may require consultation with the patient’s primary care provider or other prescribers.
While a well-conducted medication therapy review can take considerable time, the benefits to the patient, and the impact on the rest of the heart failure team, can be substantial.
|
Case Study #2
The patient is a 54-year-old African-American woman with a history of diabetes admitted overnight for worsening heart failure. Her condition has been stabilized, but this is her third heart failure admission over the past 10 months. The patient exhibits good adherence to her treatment plan.
The medical resident suggests that some new diabetes medications may be beneficial in patients with heart failure and wants to know whether one might be right for this patient.
Past medical history:
· HFrEF x 3 years
· Hypertension x 8 years
· T2DM x 11 years
Vital signs: BP 126/76 mmHg; pulse 68 bpm, regular
Body mass index: 33.8 kg/m2
Labs:
· Electrolytes within normal limits
· eGFR 62 mL/min/1.73 m2
· A1C 7.8% (3 weeks ago)
· Left ventricular ejection fraction 30%
Current medications:
· Valsartan 120 mg twice daily
· Furosemide 40 mg once daily
· Spironolactone 25 mg once daily
· Hydralazine 50 mg three times daily
· Isosorbide dinitrate 40 mg three times daily
· Metformin 1 g twice daily
· Glimepiride 6 mg once daily
What changes, if any, do you recommend?
|
Modifying the Treatment Plan
One notable finding is that the patient in case study #2 is not being treated with a beta-blocker. Evidence-based beta-blockers for HFrEF, ie, bisoprolol, carvedilol, or metoprolol succinate, should be initiated in this patient unless a contraindication exists.5 Discontinuing valsartan and switching to sacubitril/valsartan is also a guideline-recommended option as it may serve to reduce morbidity and mortality.15 The addition of ivabradine would be a future consideration if her heart rate were >70 beats per minute despite optimized beta-blocker therapy.
The physician providing care to this 54-year-old woman with T2DM is specifically interested in possible use of diabetes medications that might be helpful for patients with heart failure. Results of cardiovascular outcome trials with 3 classes of medications used for the treatment of patients with T2DM has shown that some of the glucagon-like peptide-1 receptor agonists (GLP-1RAs) and sodium glucose cotransporter-2 inhibitors (SGLT-2is) reduce cardiovascular risk compared to placebo as part of standard therapy.16 In patients with established HFrEF, the SGLT-2is canagliflozin, dapagliflozin, and empagliflozin (but not ertugliflozin) are preferred over a GLP-1RA for patients who do not achieve adequate glycemic control with the combination of lifestyle management and metformin.17
Greater insight into the benefit of SGLT-2i therapy in patients with HFrEF is provided by the DAPA-HF trial (Table 2).18 Whereas all other cardiovascular outcome trials included only patients with T2DM, only 42% of patients in the DAPA-HF trial had T2DM. In addition, all patients in the DAPA-HF trial had HFrEF. Results showed a 16.3% reduction in the primary endpoint with dapagliflozin vs 21.2% for placebo, showing a 26% relative reduction with dapagliflozin (hazard ratio (HR) 0.74; 95% confidence interval (CI) 0.65-0.85; P<0.001). Of key importance is that the reduction in the primary composite endpoint with dapagliflozin was similar in patients with T2DM (25%) and without T2DM (27%), suggesting that the benefits of dapagliflozin in HFrEF involve nonglycemic mechanisms.
|
Table 2. DAPA-HF Trial18
Objective: To evaluate the efficacy and safety of dapagliflozin in patients with HFrEF and with or without T2DM
Methods:
- Randomized, double-blind, placebo-controlled, parallel-group, multicenter, phase 3
- Patients (N=4744)
- Adults with NYHA class II, III, or IV symptoms and LVEF £40%
- NT-proBNP ≥600 pg/mL; if hospitalized for heart failure within previous 12 months: NT-proBNP ≥400 pg/mL; if atrial fibrillation or atrial flutter: NT-proBNP ≥900 pg/mL
- Implantable cardioverter-defibrillator and/or cardiac resynchronization therapy
- ACEI, ARB, or sacubitril/valsartan + b-blocker, if tolerated
- Screening period to confirm inclusion/exclusion criteria
- Randomized to dapagliflozin 10 mg or placebo once daily plus standard care
Primary endpoint(s): composite of worsening heart failure or CV death
Median follow-up: 18.2 months
|
Significant reductions also were observed with dapagliflozin for hospitalization or urgent visit for heart failure (30% reduction), hospitalization for heart failure (30% reduction), urgent visit for heart failure (57% reduction), and CV death or hospitalization for heart failure (25% reduction). Dapagliflozin was well-tolerated. The frequency of adverse events related to volume depletion, renal dysfunction, and hypoglycemia did not differ between the dapagliflozin and placebo groups. In general, patients treated with an SGLT-2i must practice good urogenital hygiene. Patients should also be educated about the need to avoid hypovolemia.
It is important to note that the thiazolidinedione medications pioglitazone and rosiglitazone, as well as the dipeptidyl peptidase-4 inhibitor saxagliptin, are not recommended for use in patients with heart failure.19
INTERVENTIONS TO ASSESS AND IMPROVE ADHERENCE
The addition of one or more medications to the treatment plan is likely to impact treatment adherence, particularly in a patient who is taking multiple medications. One recent investigation found that approximately one-half of insured U.S. adults age 18 to 64 years with newly diagnosed heart failure exhibited poor adherence to their heart failure medications.20 A key finding is that patients with poor adherence were approximately 15% more likely than patients with good adherence to have a preventable hospitalization within 3 to 5 years after their initial diagnosis. Good adherence was defined as the percentage of days covered ≥80%, while poor adherence was defined as the percentage of days covered <40%.
The Adherence Estimator
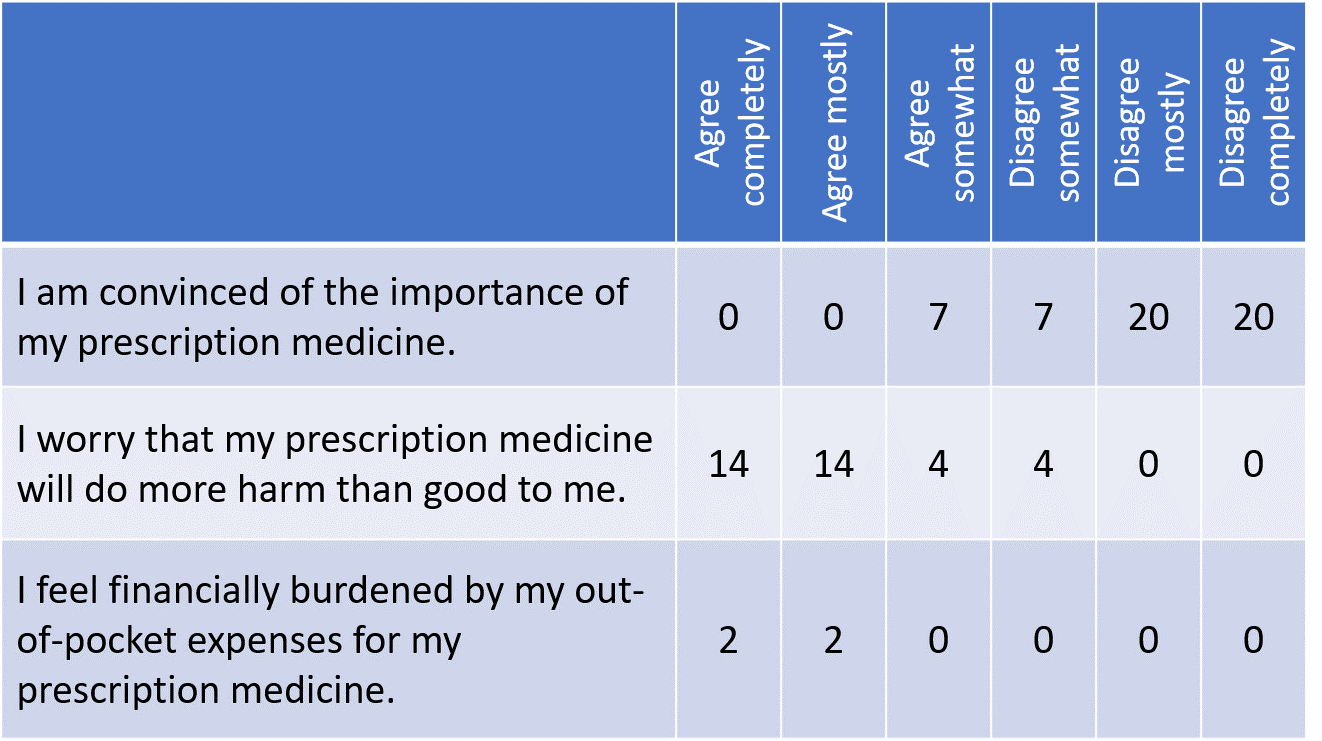
One tool that has been validated to assess adherence to oral medications in select chronic conditions, such as hypertension and hyperlipidemia, is the Adherence Estimator.21 It has not been specificallytested in the heart failure population. The Adherence Estimator consists of 3 items to assess perceived concerns about predications, perceived need for medications, and perceived affordability of medications (Figure 2). By simple summation of the weights assigned to the categorical responses of the 3 items, a total score is obtained that identifies patients as low, medium, or high risk for non-adherence.
|
Figure 2. The Adherence Estimator21
|
Strategies to Improve Adherence
Several points should be kept in mind when developing strategies to improve patient adherence. As noted earlier, the patient plays a central role in identifying and resolving suboptimal adherence. It is important to realize that adherence is a multifactorial issue and it is likely that more than 1 barrier contributes to suboptimal patient adherence. Collaborating with the patient to identify the root causes contributing to suboptimal medication adherence is a key role for the pharmacist. Providing understanding that treatment adherence is difficult for most patients with several chronic diseases, including heart failure, and expressing the desire to help the patient improve their quality of life can help the patient feel comfortable to be open and honest. Once the root causes are identified, the role of the pharmacist is to suggest possible solutions for the patient to consider, with the patient selecting the solution(s) that they are willing and able to implement. Successful implementation often requires ongoing patient education and support from the pharmacist and other members of the heart failure team. Clear and timely communication with other team members is critical so that all team members provide consistent and individualized support. For patients who are hospitalized, changes to the treatment plan, particularly if a new medication is started, are best implemented well in advance of discharge as this provides greater opportunity to provide the extra education and support often needed. Finally, adherence should be assessed at every visit, whether it is in clinic or when the patient picks up a prescription. Ongoing support and encouragement are of great benefit, even in patients who exhibit good adherence.
The 2017 ACC Expert Consensus Decision Pathway for Optimization of Heart Failure Treatment: Answers to 10 Pivotal Issues About Heart Failure With Reduced Ejection Fraction: A Report of the American College of Cardiology Task Force on Expert Consensus Decision Pathways provides 10 considerations for interventions to improve patient adherence to therapy (Table 3).12 Implementation of these interventions requires a collaborative approach among the heart failure team, including pharmacists who practice in different settings. Effective communication among team members is essential.
| Table 3. Ten considerations to improve adherence12 |
| 1 |
Capitalize on opportunities when patients are most disposed to adherence
· In-hospital/pre-discharge initiation following decompensation |
| 2 |
Consider the patient’s perspective
· Start with the goals of therapy (feeling better and living longer) and then discuss how specific actions (medication initiation, intensification, monitoring, and adherence) support those goals
· Use decision aids when available
· Ask patient how they learn best and provide education accordingly |
| 3 |
Simplify medication regimens when possible |
| 4 |
Consider costs and access
· Become familiar with and advocate for systems that help make cost sharing automatic, immediate, and transparent
· Prescribe lower-cost medications if of similar efficacy
· Facilitate access to copay assistance
· Discuss out-of-pocket copays proactively
· Prescribe 90-day quantities for refills |
| 5 |
Communicate with other clinicians involved in care, ideally facilitated by electronic health records |
| 6 |
Educate using practical, patient-friendly information
· Provide a written explanation of the purpose of each medication prescribed
· Plan pharmacist visits for complex medication regimens
· Use the “teach back” principle to reinforce education |
| 7 |
Recommend tools that support adherence in real time
· Pill boxes to be filled by patient or caregiver a week at a time
· Alarms for each time of the day medications are due
· Smartphone M-Health applications that provide an interactive platform for education, reminders, warnings, and adherence tracking |
| 8 |
Consider behavioral supports
· Motivational interviewing
· Participate in engaged benefit designs |
| 9 |
Anticipate problems
· Communicate common side effects
· Provide instructions on when to call for refills or problems |
| 10 |
Monitor adherence and target patients at risk
· Ask patients directly (eg, “How many times in a week do you miss taking your medications?” “Have you run out of your medications recently?”)
· Carry out medicine reconciliation at visits, with focus on discrepancies
· Assess remaining dosage units (ie, count excess remaining tablets)
· Monitor pharmacy fills, using available databases (eg, https://www.colorado.gov/pacific/dora/PDMP) or automated alerts for failed fills and refills
· Review available drug levels (eg, digoxin, INR) or concentrations of BNP/NT-proBNP
· Plan home-based nursing visits for appropriate patients |
| BNP, B-type natriuretic peptide; INR, international normalized ratio; NT-proBNP, N-terminal pro-B-type natriuretic peptide |
Polypharmacy
|
Case Study #3
A 72-year-old man comes into the pharmacy to pick up a new prescription for sacubitril/valsartan. He seems bothered starting yet another medication and is confused about which ones he should continue or discontinue.
Current medications:
· Lisinopril 30 mg once daily
· Metoprolol succinate 200 mg once daily
· Furosemide 80 mg once daily
· Spironolactone 25 mg once daily
1. What are the benefits of adding sacubitril/valsartan?
2. Are there any drug interactions to consider?
3. What other precautions should be considered before the patient takes sacubitril/valsartan?
|
Patients may not fully understand why changes are being made to their treatment plan, especially when a new medication has been added. This is a reminder of the importance of providing ongoing education and asking patients at each encounter if they have any questions. When a new medication is started, the patient should be asked to explain their understanding as to why the new medication is being started and its expected effect on heart failure prognosis, as well as its name, dosage, frequency, and common adverse events as their response can help direct the education and support the patient needs.
The use of the ARNI sacubitril/valsartan is recommended in the current guidelines for patients with chronic symptomatic NYHA class II or II HFrEF who tolerate an ACE inhibitor or ARB. Switching to the ARNI was shown to further reduce morbidity and mortality in the Prospective Comparison of ARNI with ACEI to Determine Impact on Global Mortality and Morbidity in Heart Failure (PARADIGM-HF) trial.15 Specifically, patients treated with sacubitril/valsartan showed significant reductions in hospitalizations and mortality compared with the ACE inhibitor enalapril.
Since sacubitril/valsartan includes an ARB, it would replace existing ACE inhibitor or ARB therapy; in this case study, lisinopril. To minimize the risk of angioedema, a 36-hour washout period is needed following discontinuation of an ACE inhibitor and initiation of sacubitril/valsartan.
It is important to review the medication guide of sacubitril/valsartan with the patient to discuss common adverse events, eg, hypotension, hyperkalemia, cough, dizziness, and renal failure, how to monitor for these, and what to do should one occur. Patients should be advised about drug interactions and their list of current medications (prescription, non-prescription, and complementary and alternative medications) verified. Patients should also be advised about the importance of avoiding the use of medications that can exacerbate heart failure, as well as nonsteroidal anti-inflammatory medications, which may increase the risk of renal impairment. Patients should be reminded of the importance of daily monitoring of their vital signs and body weight. Finally, follow up communication with the prescriber is recommended.
Health Literacy
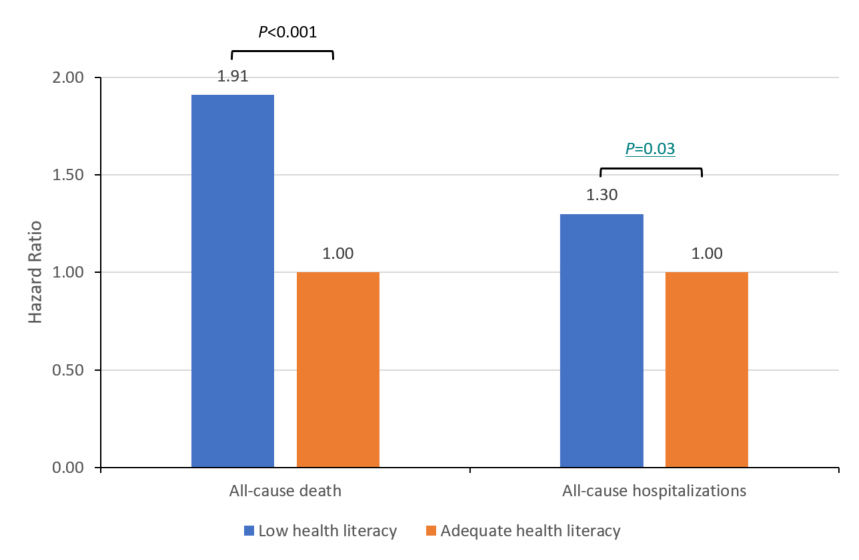
Patient health literacy is well established as having a significant impact on patient adherence and outcomes.22-24 A recent survey was conducted to measure health literacy among 2487 patients with heart failure.25 Using the Brief Health Literacy Screen (BHLS) (described below), the survey showed that 11% had low health literacy. Over a mean follow up of 16 months, patients with low health literacy were significantly more likely to die (hazard ratio (HR) 1.91; 95% confidence interval (CI) 1.38-2.65; P<0.001) and be hospitalized (HR 1.30; 95% CI 1.02-1.66; P=0.03) (Figure 3). These results underscore the importance of educating patients about their disease state and treatment plan.
|
Figure 3. Impact of health literacy on heart failure outcomes25
|
|
N=2487
Adjusted for age, sex, education, marital status, and Charlson Comorbidity Index
Health literacy defined as: low: <8 (n=261); adequate ≥8 (n=2226).
Health literacy assessed as a composite of 3 questions (5-point scale each): 1) How confident are you filling out forms by yourself?; 2) How often do you have someone help you read hospital materials?; and 3) How often do you have problems learning about your medical condition because of difficulty reading hospital materials?
|
| Reprinted with permission from Fabbri M, et al. Health literacy and outcomes in patients with heart failure: A prospective community study. Mayo Clin Proc. 2018;93(1):9-15 |
Numerous tests have been validated to assess the health literacy of patients. Characteristics of 3 of those commonly used are shown in Table 4.26-28 The Short Test of Functional Health Literacy in Adults (S-TOFHLA) requires the patient to read 2 passages, one at the 4th grade level and the other at the 10th grade level. S-TOFHLA assesses sentence completion rather than functional understanding. Numeracy is not tested. Health literacy is categorized as inadequate, marginal, or adequate. The Rapid Estimate of Adult Literacy in Medicine (REALM) test measures a person’s ability to pronounce 66 common medical words and lay terms for body parts and illnesses. Several versions are available. The BHLS consists of 3 items on a 5-point response scale that is read aloud to the patient; completion takes <2 minutes.
| Table 4. Health literacy screening tools |
| Measure |
Population |
Format |
# Questions |
| Short Test of Functional Health Literacy in Adults26 |
18-64 y |
Written
Face-to-face |
40
(12-minute cut-off) |
| Rapid Estimate of Adult Literacy in Medicine27 |
Several versions based on age, disease |
Face-to-face |
66
(2½ minutes) |
| Brief Health Literacy Screen28 |
18-64 y |
Face-to-face |
3
(1½ minutes) |
The Agency for Healthcare Research and Quality (AHRQ) also provides access to health literacy assessment tools. One is the Short Assessment of Health Literacy- Spanish and English which tests the patient’s comprehension and pronunciation of health-related terms.29 Administration of the test takes 2 to 3 minutes.
AHRQ also provides 7 health literacy tools for pharmacists and a set of curricular tools for pharmacy faculty.30 These tools are:
- Pharmacy health literacy assessment tool & user’s guide
- Training program for pharmacy staff on communication
- Guide on how to create a pill card
- Telephone reminder tool to help refill medicines on time
- Explicit and standardized prescription medicine instructions
- How to conduct a post-discharge follow-up phone call
- Health literacy tools to improve communication for providers of medication therapy management
The purpose of these 7 literacy tools is to: 1) see if pharmacists and pharmacy staff are meeting patient needs; 2) detect potential barriers for patients with limited literacy skills to comprehending pharmacy information; and 3) identify opportunities to improve customer service provided by pharmacists and pharmacy staff.
PATIENT HEART FAILURE EDUCATION RESOURCES
There are several excellent resources that the pharmacist can be used to provide patient education (Table 5). All provide information about the disease state and its treatment.
The American Association of Heart Failure Nurses provides a variety of patient tip sheets. There is a section on self-care, and another on functional, physical, and sexual activity.
CardioSmart by the American College of Cardiology offers numerous downloads for patients. Several are patient checklists such as a general action plan and tips about heart failure medication. A section on medication adherence provides patients with advice on how to achieve the greatest benefit from their medications and why it’s important. There’s also a section and resources for caregivers. There are many decision aids and discussion guides to assist clinicians in communicating and collaborating with their patients. One is to guide the selection of renin-angiotensin-aldosterone inhibitor therapy. Also available through the American College of Cardiology website is ‘TreatHF’, an application for use by clinicians to help guide and optimize pharmacological therapy for patients with chronic stage C HFrEF. TreatHF can be used online or downloaded for use on a smartphone.
The American Heart Association provides a wide variety of resources for patients, as well as for clinicians. Many of the patient resources are designed to be downloaded; some are in Spanish. The HF Guide is a 48-page brochure that covers numerous topics from the disease state and its consequences, lifestyle management, pharmacological and surgical treatment, and tips for living well with heart failure. The HF Path is an interactive tool for use online or on a smartphone that is designed to help patients achieve a better quality of life through symptom management, treatment adherence, and social support. There also is an online patient support network, including a blog and survivor stories. For clinicians, several resources are designed to identify high-risk heart failure patients and apply the latest, evidence-based treatment guidelines.
The Heart Failure Society of American (HFSA) also provides a wide variety of useful tools for patients with heart failure on their patient hub. A series of 11 modules covering a wide range of topics, with each module including questions patients should ask their heart failure team. A series of podcasts feature interviews with patients, caregivers, and clinicians to help patients live a healthy life. A webinar series features information from clinicians about critical topics in heart failure treatment, prevention, and risk management. A risk assessment toolkit helps clinicians educate patients about heart failure risk and prevention. There also is a list of patient assistance programs. The HFSA website also includes extensive information and education for clinicians, including upcoming heart failure meetings.
MedlinePlus provides extensive disease state information, as well as links to numerous other websites, including information about heart failure in children and older adults. Information about heart failure clinical trials is also available on MedlinePlus, as well as on the National Institutes of Health (NIH) website.
SUMMARY
Pharmacists are identified in current heart failure guidelines as providing key roles in the ongoing management of patients with heart failure. Key roles for pharmacists are to identify concerns and barriers patients with heart failure may be experiencing, particularly related to medications, and to collaborate with patients to resolve these issues so that they are optimally treated with guideline-directed medications. To do this effectively requires that pharmacists understand the disease burden experienced by patients with heart failure every day ranging from weighing themselves, adhering to the treatment plan, getting to appointments, refilling prescriptions, adhering to dietary restrictions, and maintaining as normal a life as possible. In addition to education, a key role for pharmacists is to provide encouragement. Patients need positive feedback that they’re doing well. There is a wide variety of resources available to help pharmacists educate patients and for patients to better self-manage their heart failure. As pharmacists contribute to the care of patients with heart failure, it is important that they work collaboratively with pharmacists in other practice settings, as well as other healthcare professionals, and that their activities be appropriately communicated to the heart failure team.
REFERENCES
- Virani SS, Alonso A, Benjamin EJ, et al. Heart Disease and Stroke Statistics-2020 Update: A Report From the American Heart Association. Circulation. 2020;141(9):e139-e596.
- Heo S, Doering LV, Widener J, Moser DK. Predictors and effect of physical symptom status on health-related quality of life in patients with heart failure. Am J Crit Care. 2008;17(2):124-132.
- Lesman-Leegte I, Jaarsma T, Coyne JC, Hillege HL, Van Veldhuisen DJ, Sanderman R. Quality of life and depressive symptoms in the elderly: a comparison between patients with heart failure and age- and gender-matched community controls. J Card Fail. 2009;15(1):17-23.
- Greene SJ, Butler J, Albert NM, et al. Medical therapy for heart failure with reduced ejection fraction: The CHAMP-HF registry. J Am Coll Cardiol. 2018;72(4):351-366.
- Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation. 2017;136(6):e137-e161.
- Yusuf S, Pitt B, Davis CE, Hood WB, Cohn JN. Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. N Engl J Med. 1991;325(5):293-302.
- Young JB, Dunlap ME, Pfeffer MA, et al. Mortality and morbidity reduction with candesartan in patients with chronic heart failure and left ventricular systolic dysfunction: results of the CHARM low-left ventricular ejection fraction trials. Circulation. 2004;110(17):2618-2626.
- CIBIS-II Investigators and Committees. The Cardiac Insufficiency Bisoprolol Study II (CIBIS-II): a randomised trial. Lancet. 1999;353(9146):9-13.
- Zannad F, McMurray JJ, Krum H, et al. Eplerenone in patients with systolic heart failure and mild symptoms. N Engl J Med. 2011;364(1):11-21.
- Pitt B, Zannad F, Remme WJ, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. Randomized Aldactone Evaluation Study Investigators. N Engl J Med. 1999;341(10):709-717.
- Packer M, Coats AJ, Fowler MB, et al. Effect of carvedilol on survival in severe chronic heart failure. N Engl J Med. 2001;344(22):1651-1658.
- Yancy CW, Januzzi JL, Jr., Allen LA, et al. 2017 ACC Expert Consensus Decision Pathway for Optimization of Heart Failure Treatment: Answers to 10 Pivotal Issues About Heart Failure With Reduced Ejection Fraction: A Report of the American College of Cardiology Task Force on Expert Consensus Decision Pathways. J Am Coll Cardiol. 2018;71(2):201-230.
- Anon. Collaboration between community pharmacy-based and clinic-based pharmacists to achieve medication optimization: Consensus guiding statements from ACCP, CPESN USA, and NCPA Innovation Center. J Am Coll Clin Pharm. 2019;2:447-448.
- Centers for Medicare & Medicaid Services. CY 2020 Medication Therapy Management Program Guidance and Submission Instructions. April 5, 2019. https://www.cms.gov/Medicare/Prescription-Drug-Coverage/PrescriptionDrugCovContra/Downloads/Memo-Contract-Year-2020-Medication-Therapy-Management-MTM-Program-Submission-v-041019-.pdf. Accessed July 29, 2020.
- McMurray JJ, Packer M, Desai AS, et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014;371(11):993-1004.
- American Diabetes Association. 10. Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes-2020. Diabetes Care. 2020;43(Suppl 1):S111-S134.
- American Diabetes Association. 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes-2020. Diabetes Care. 2020;43(Suppl 1):S98-S110.
- McMurray JJV, Solomon SD, Inzucchi SE, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019;381(21):1995-2008.
- American Diabetes Association. 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes-2019. Diabetes Care. 2019;42(Suppl 1):S90-S102.
- Chang TE, Park S, Yang Q, Loustalot F, Butler J, Ritchey MD. Association between long-term adherence to class-I recommended medications and risk for potentially preventable heart failure hospitalizations among younger adults. PLoS One. 2019;14(9):e0222868.
- McHorney CA. The Adherence Estimator: a brief, proximal screener for patient propensity to adhere to prescription medications for chronic disease. Curr Med Res Opin. 2009;25(1):215-238.
- Cox SR, Liebl MG, McComb MN, et al. Association between health literacy and 30-day healthcare use after hospital discharge in the heart failure population. Res Social Adm Pharm. 2017;13(4):754-758.
- Wu JR, Moser DK, DeWalt DA, Rayens MK, Dracup K. Health literacy mediates the relationship between age and health outcomes in patients with heart failure. Circ Heart Fail. 2016;9(1):e002250.
- Cajita MI, Cajita TR, Han HR. Health literacy and heart failure: A systematic review. J Cardiovasc Nurs. 2016;31(2):121-130.
- Fabbri M, Yost K, Finney Rutten LJ, et al. Health literacy and outcomes in patients with heart failure: A prospective community study. Mayo Clin Proc. 2018;93(1):9-15.
- Baker DW, Williams MV, Parker RM, Gazmararian JA, Nurss J. Development of a brief test to measure functional health literacy. Patient Educ Couns. 1999;38(1):33-42.
- Davis TC, Long SW, Jackson RH, et al. Rapid estimate of adult literacy in medicine: a shortened screening instrument. Fam Med. 1993;25(6):391-395.
- Wallston KA, Cawthon C, McNaughton CD, Rothman RL, Osborn CY, Kripalani S. Psychometric properties of the brief health literacy screen in clinical practice. J Gen Intern Med. 2014;29(1):119-126.
- Lee SY, Stucky BD, Lee JY, Rozier RG, Bender DE. Short Assessment of Health Literacy-Spanish and English: a comparable test of health literacy for Spanish and English speakers. Health Serv Res. 2010;45(4):1105-1120.
- Agency for Healthcare Research and Quality. AHRQ health literacy tools for use in pharmacies. 2018. https://www.ahrq.gov/health-literacy/pharmhealthlit/tools.html. Accessed July 30, 2020.
Back to Top