Oncology Pharmacy Consults
Lysis Crisis:
Pharmacist's Role and Responsibility in the Management of Tumor Lysis Syndrome
Tumor Lysis Syndrome Background
Definition
Tumor lysis syndrome in an oncometabolic syndrome resulting from a rapid die-off of large numbers of cancer cells.1,4 Cancer cell death may occur spontaneously or as a result of therapy, including traditional cytotoxic chemotherapy and targeted, immuno, hormonal, and radiation therapies. Cell death releases cellular contents into the blood stream leading to hyperuricemia, hyperkalemia, hyperphosphatemia, and hypocalcemia. Electrolyte and metabolic dysregulation can progress to renal toxicity, cardiac arrhythmias, seizures, and death due to multiorgan failure.
The Cairo-Bishop criteria have been adopted as the consensus defining TLS.5 These criteria recognize clinically silent "laboratory TLS" and established "clinical TLS." Identification of laboratory TLS is based on the presence of 2 or more anomalous blood chemistry values within the 3 days before chemotherapy or 7 days after the initiation of chemotherapy in an adequately hydrated patient, who is also using a uric-acid lowering agent. Laboratory blood changes of a 25% or more increase from baseline of uric acid, potassium, or phosphorous, or a 25% or more decrease in calcium are typically used as indications of TLS. Alternatively, if baseline values are unknown, absolute values may be used (Table 1).
| Table 1. Absolute Electrolyte Levels |
| Electrolyte |
Absolute value |
| Uric acid |
≥8 mg/dL (0.47 mmol/L) |
| Potassium |
≥6 mEq/L (or 6 mmol/L) |
| Phosphorus |
≥4.5 mg/dL (1.45 mmol/L) for adults ≥6.5 mg/dL (2.1 mmol/L) for children |
| Calcium |
≤7 mg/dL (1.75 mmol/L) |
Absolute electrolyte levels indicative of a patient with TLS.
TLS = tumor lysis syndrome. |
Clinical TLS is defined as the presence of at least 1 clinical criterion – increased serum creatinine of more than 1.5 the upper limit of normal, cardiac arrhythmia, and seizures – that is not thought to be an adverse effect of chemotherapy.5 The clinical grade of TLS is based on the severity of symptoms. However, there are several limitations to the Cairo-Bishop criteria:
- The exclusion of spontaneous TLS; these criteria require that the patient be receiving, or have recently received chemotherapy;
- Creatinine clearance can be elevated in patients with chronic kidney disease, not just TLS;
- The distinction between "laboratory" and "clinical" TLS is not generally relevant, because most guidelines recommend aggressive treatment of laboratory abnormalities in order to prevent renal insufficiencies from developing;
- The Cairo-Bishop criteria outline different grades of clinical TLS; however, guidelines do not vary treatment recommendations by grade.5
In spite of these limitations, the Cairo-Bishop criteria have proven to be very effective in identifying and diagnosing patients with TLS.5
Epidemiology
Tumor lysis syndrome is a rare event in the treatment of patients with most cancer types. It is most common in patients with acute lymphocytic leukemia, AML (with a WBC count of more than 75 000), B-cell acute lymphoblastic leukemia, and Burkitt's lymphoma (Table 2).6-13 Patients with cancers that are most frequently associated with TLS are those that are large, fast-growing, and chemo-sensitive. For instance, approximately 26% of children with B-cell acute lymphoblastic leukemia will develop treatment-associated TLS.6 Spontaneous TLS, prior to therapy initiation, is reported to occur in approximately 14% of patients.7
| Table 2. Incidence of TLS |
| Risk group |
Malignancy |
Incidence (%) |
| Highs |
Acute lymphocytic leukemia |
5.2–23 |
| Acute myeloid leukemia (WBC >75 000) |
18 |
| B-cell acute lymphoblastic leukemia |
16.4 |
| Burkitt's lymphoma |
14.9 |
| Intermediate |
AML (WBC 25 000–50 000) |
6 |
| Diffuse large B-cell lymphoma |
6 |
| Low |
AML (WBC <25 000) |
1 |
| Chronic lymphocytic leukemia |
0.33 |
| Chronic myelogenous leukemia |
Case reports |
| Solid tumors |
Case reports |
Incidence of tumor lysis syndrome in various cancer types.
AML = acute myeloid leukemia; TLS = tumor lysis syndrome; WBC = white blood cell.
Data from Wossmann et al. Ann Hematol. 20036; Vodopivec et al. Case Rep Med. 20127; Truong et al. Cancer. 20078; Annemans et al. Leuk Lymphoma. 20039; Montesinos et al. Haematologica. 200810; Hande et al. Am J Med. 199311; Cheson et al. J Clin Oncol. 199812; Al-Kali et al. J Clin Pharm Ther. 2009.13 |
Tumor lysis syndrome in patients with solid tumors is extremely rare. It is unclear if the increasing reports of TLS in patients with solid tumors in the literature are a result of more effective treatments or increased surveillance.2,7
Pathophysiology
Therapy-induced lysis of cancer cells has the potential to release large amounts of cellular material. If this release is rapid, the normal mechanisms, which eliminate cellular waste and debris, can become overwhelmed. In particular, it is the release of nucleic acids, phosphate, and potassium that lead to the metabolic effects underlying TLS.
Chemotherapy often induces energy depletion leading to the breakdown of chemical and ion gradients across the cell membrane.14 Liberated potassium is usually taken up by the liver and muscle cells, and any excess is gradually excreted by the kidneys and gastrointestinal tract. A supraphysiological load may overwhelm potassium uptake and excretion mechanisms leading to hyperkalemia.15 This is more problematic in patients with chronic or acute renal insufficiency as potassium will clear much more slowly.
Released purine bases are metabolized under normal conditions to hypoxanthine, xanthine, and uric acid, before excretion via the kidneys (Figure 1). Unlike most mammals, humans do not have the ability to further oxidize uric acid to allantoin. High concentrations of uric acid form crystals at a pH of 5.6 or less, which is particularly problematic in the distal tubules where the pH is lower and the flow rate is slower. Urate crystal formation may block tubules and reduce glomerular filtration rate. Nonobstructive mechanisms that damage the kidneys due to hyperuricemic effects include:
- Changes in hemodynamics in the kidney
- Increased proximal and distal tubular pressures
- Increased peritubular capillary pressure
- Vasoconstriction and kidney ischemia
- Upregulated proinflammatory cytokine production16
Figure 1. Chemotherapy-Induced Cancer Cell Death
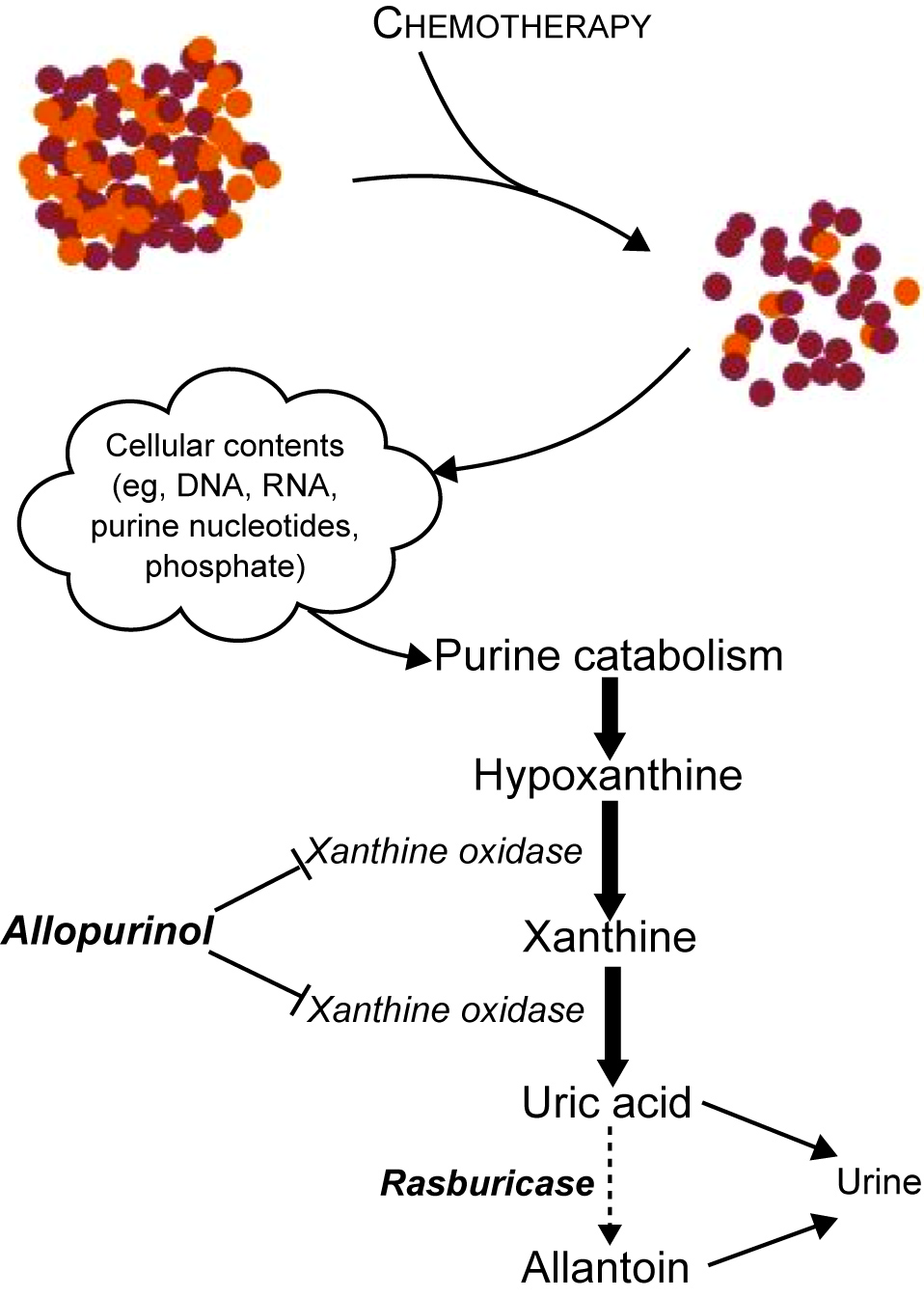
Chemotherapy-induced cancer cell death leads to increased purine catabolism and uric acid formation.
Hematologic cancer cells contain up to 4 times more intracellular phosphate than normal lymphoid cells.14 Similar to potassium, the high amounts of phosphate released from cells may overwhelm normal excretion mechanisms, particularly in patients with preexisting renal insufficiency. Hyperphosphatemia may be less common in patients with spontaneous TLS than those with TLS that's induced by chemotherapy.2
Hypocalcemia develops secondarily to hyperphosphatemia as a result of deposition of calcium phosphate crystals in soft tissues.1 Calcium phosphate crystals in the kidneys can lead to nephropathy similar to urate crystal formation. Urate crystal formation in urine potentiates calcium phosphate precipitation and vice versa.
Effects of Tumor Lysis Syndrome
Electrolyte disturbances directly contribute to the clinical manifestations of TLS. It can be difficult to identify TLS in early stages based on clinical symptoms alone. For instance, many chemotherapies induce nausea and vomiting or generalized fatigue. It is important to monitor patients closely, particularly during the first week of treatment initiation, as in some low-risk patients, TLS develops unexpectedly.5,18 Ruling out TLS in cancer patients who present with acute kidney dysfunction requires a thorough clinical history and work up.
Hyperkalemia is often the first observed laboratory abnormality and can occur within 6 hours of the start of chemotherapy, although it typically occurs in the first 12 to 24 hours.14,19 Normal potassium levels in the blood are 3.5 to 5.0 mEq/L, but in patients with severe hyperkalemia, it's is above 7 mEq/L. Early stage hyperkalemia may present as muscle weakness or fatigue. Cardiac dysrhythmias develop from further increases in potassium levels. Untreated, high hyperkalemia puts the patient at risk for cardiac arrhythmia and sudden death.1
Concurrent to the development of hyperkalemia, phosphate and uric acid levels build up in the blood and rise in glomerular filtrate. Elevations in blood phosphorus levels are not seen for 24 to 48 hours after the initiation of therapy, until blood levels exceed the capacity for renal excretion.
Excess phosphate binds calcium and precipitates in soft tissues including the kidneys. This contributes to kidney dysfunction and leads to the development of secondary hypocalcemia, which is primarily responsible for morbidity and mortality associated with hyperphosphatemia. Severe hypocalcemia can lead to cardiac arrhythmias, seizures, muscle twitching, tetany, hypotension, and death.1
Cells are rich with purine bases that can be metabolized to xanthine and uric acid. Sources include DNA/RNA, adenine and guanine nucleoside phosphates, and nicotinamide adenine dinucleotide. Urate precipitation in the distal renal tubules reduces urine output and further decreases a patients' ability to clear cellular waste (eg, potassium, phosphate, uric acid). Hyperuricemia usually occurs 48 to 72 hours after the initiation of therapy. Uric acid crystals are the major mechanism by which renal function is impaired in patients with TLS.1
Risk Factors
Risk factors for the development of TLS include cancer mass, cell lysis potential, patient-specific characteristics, and inadequate supportive care. Figure 2 depicts a TLS risk algorithm and is in line with the Cairo-Bishop definition of TLS.1
Figure 2. TLS Risk Assessment Algorithm
(click here for larger image)
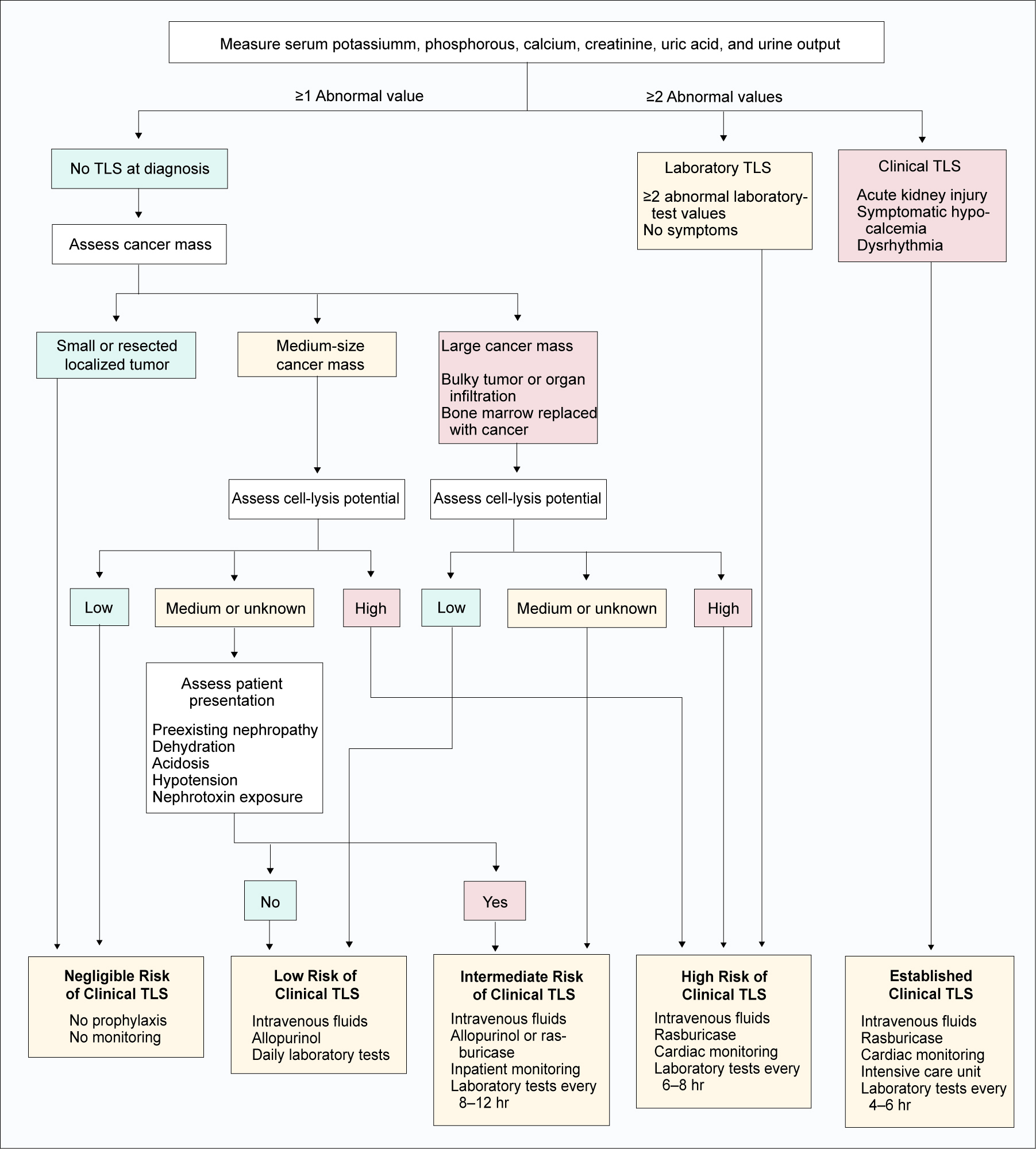
TLS = tumor lysis syndrome.
Howard et al. N Engl J Med. 2011.1 For educational purposes only.
The rapid lysis of large masses of cancer cells have the potential to precipitate TLS: the more cancer cells, the higher the risk of TLS.1 Patients with small or resected localized tumors, or medium-sized tumors with a low potential for rapid cell lysis, have a very low risk of TLS. Patients with large tumors, medium-sized tumors with intermediate or high risk of rapid cell lysis, or hematological cancers have a risk of TLS that needs to be defined before the start of therapy. Hematological cancers frequently have replaced most bone marrow by the time treatment ensues, and as a result, constitute bulky diseases. Similarly, metastases and organ infiltration, particularly hepatomegaly, splenomegaly, and nephromegaly, typically represent a larger tumor burden. Patients with cancers that infiltrate the kidneys or obstruct urine outflow may predispose them to TLS.
Patient-specific characteristics, such as preexisting nephropathy, renal insufficiency, or dehydration, can predispose patients to TLS. Reduced flow rate, coupled with increased uric acid and/or phosphorus levels, increases the risk of crystal formation and nephropathy. Hypotension increases the risk of TLS by 2 mechanisms: reduced urine flow and nephropathy independent of TLS. Glomerular filtration and urine flow rates are decreased in hypotensive patients which increases the risk of TLS. Hypotension itself can lead to nephropathy in the absence of TLS. Uric acid crystals or microcrystals are usually present in the renal tubules of hypotensive patients with acidic urine and hyperuricemia. Lastly, exposure to nephrotoxins (eg, some antibiotics [vancomycin, aminoglycosides] and imaging contrast agents) also increases the risk of TLS.
Remember, clinical TLS is brought on by:
- High tumor burden
- High sensitivity to cell lysis during treatment
- Inefficient ability to clear lysed cell by-products
- Failure to adequately manage early symptoms1

Postgraduate Healthcare Education, LLC (PHE) is the source of PowerPak continuing education for health care
professionals. Our accredited programs assist in meeting the requirements of licensure. PHE provides continuing
education for the broad spectrum of health care professionals. This site features a searchable database of accredited
PowerPak courses on important topics for today's health care professionals.
PHE customizes PowerPak online for each visitor by creating a personal participant profile. Registered participants
may update their contact information, take an exam, receive instant grading, view their exam history, and print certificates
for successfully completed programs at any time. Monthly notifications will be sent to participants notifying you of new
courses available on the site.