ADVERTISEMENT

INTRODUCTION
Cardiac arrhythmias are cardiovascular emergencies that should be assessed and treated promptly to avoid decompensation into cardiac arrest. Recognizing common cardiac arrhythmias can be a useful skill for pharmacists in order to assist with early recognition and treatment of arrhythmias. In fact, several reports have noted a role for pharmacists, as the most accessible healthcare providers, in screening for arrhythmias in the outpatient setting.1,2 The purpose of this program is to provide an overview of cardiac arrhythmias and cardiac arrest to prepare practicing pharmacists to recognize cardiac arrhythmias and respond to cardiovascular emergencies.
RHYTHM IDENTIFICATION
Normal Conduction
Arrhythmias can be categorized in multiple ways, including tachyarrhythmia versus bradyarrhythmia, ventricular versus supraventricular, unstable (symptomatic) versus stable (asymptomatic), or pulseless versus with a pulse. Electrocardiogram (ECG) tracings represent the movement of electrical activity through the cardiac cycle (Figure 1).
| Figure 1. Normal Cardiac Cycle42 |
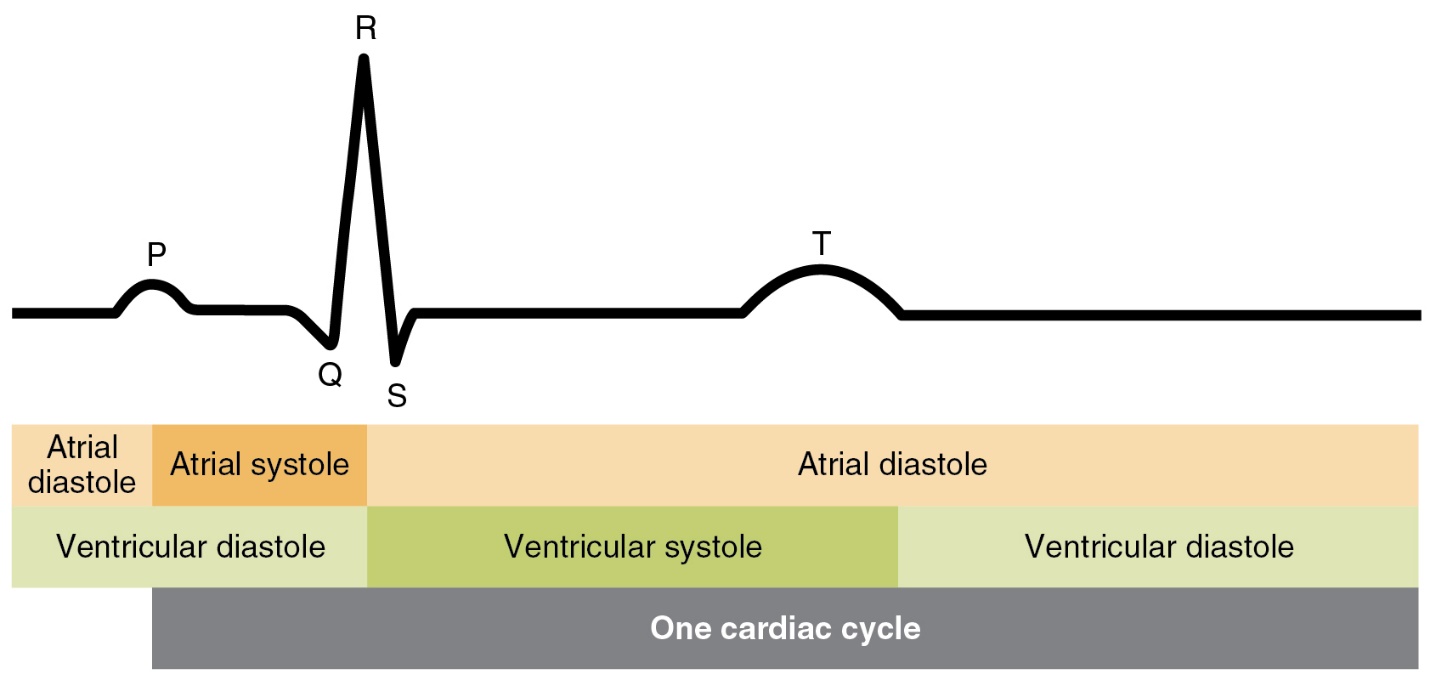 |
The P wave represents atrial depolarization, while ventricular depolarization and repolarization occur during the QRS complex and T wave, respectively. The PR interval represents the time for the electric impulse to travel from the sinoatrial (SA) node through the atrioventricular (AV) node to the ventricles.
The SA node is considered the pacemaker of the heart and is where the electrical impulse is generated, while the AV node is considered the gatekeeper and regulates the movement of electrical impulses from the atria to the ventricles to stimulate ventricular contraction.
The QT interval represents the time for ventricular depolarization and repolarization to occur, while the QTc interval is the QT interval corrected for heart rate. Finally, the R-R interval represents the time between beats and is used to calculate the heart rate. Depolarization occurs during systole, and repolarization occurs during diastole.
Electrocardiogram Evaluation
Numerous approaches have been proposed for evaluating an ECG. While no single process is preferred, it is important for clinicians to choose a stepwise approach for evaluating ECGs and to apply it consistently. One such approach is outlined in Table 1.3
| Table 1. Proposed Stepwise Approach for Evaluating an Electrocardiogram3 |
|
Step
|
Action
|
Interpretation
|
|
1
|
Assess the patient for stability (i.e., pulse, blood pressure)
|
If pulse is absent, this is a cardiovascular emergency; begin CPR immediately
|
|
2
|
Is there a P wave before each QRS complex?
|
Identifies whether the rhythm originates in the SA node
|
|
3
|
Is the R-R interval regular?
|
If no, indicates “irregularly irregular” rhythm (e.g., atrial fibrillation)
|
|
4
|
Is the rate below 60 or above 100 beats per minute?
|
Identifies bradycardia or tachycardia, respectively
|
|
5
|
Is the PR interval normal?
|
Is prolonged with various heart blocks
|
|
6
|
Is the QRS complex narrow?
|
Identifies supraventricular versus ventricular arrhythmia
|
|
7
|
Is the QT less than half the R-R interval?
|
If no, QTc is likely prolonged
|
|
8
|
Does each QRS complex look the same?
|
If no, indicates PVCs or PACs
|
|
Abbreviations: CPR, cardiopulmonary resuscitation; SA, sinoatrial; PVC, premature ventricular contraction; PAC, premature atrial contraction.
|
Recognition of Tachyarrhythmias
Tachyarrhythmias are defined as abnormal heart rhythms with ventricular rates above 100 beats per minute; rates of 150 or greater typically require treatment. Tachyarrhythmias are often symptomatic (unstable), and many can rapidly deteriorate into cardiac arrest if left untreated. Common symptoms of tachyarrhythmias include dizziness, shortness of breath, palpitations, lightheadedness, chest pain, and syncope.4 Patients presenting with tachyarrhythmias may complain of feeling that their heart is racing or that they have pounding in their chest (which is considered stable if the above symptoms are absent).
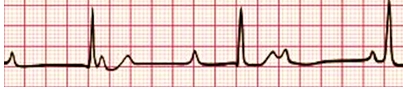
Sinus tachycardia is represented by normal cardiac conduction with a ventricular rate of more than 100 beats per minute. It often occurs as a compensatory mechanism in response to hypotension as the body increases heart rate in an attempt to maintain cardiac output and tissue perfusion (cardiac output = stroke volume X heart rate). Sinus tachycardia can also occur as a physiologic response to pain or other stress on the body, such as withdrawal, agitation, or hypovolemia. It is important to evaluate and treat the underlying cause of sinus tachycardia before initiating pharmacotherapy targeted at lowering the ventricular rate (e.g., beta-blocker, nondihydropyridine calcium channel blocker).
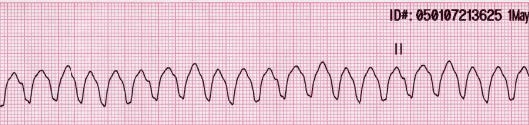
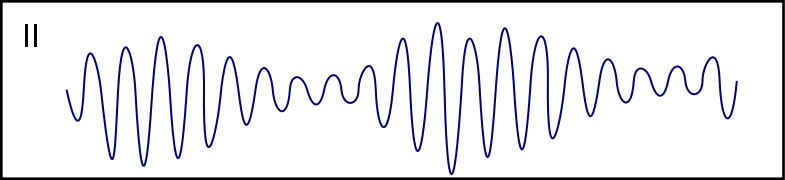
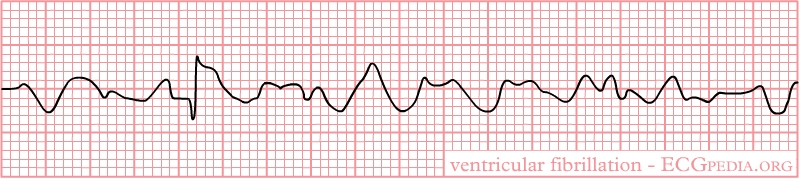
Tachyarrhythmias are often characterized as supraventricular, in which the origin of the arrhythmia is “above” the ventricles or as ventricular. Supraventricular tachyarrhythmias include supraventricular tachycardia, atrial fibrillation, and atrial flutter, and all have a narrow QRS complex. Ventricular tachyarrhythmias originate in the ventricles and include monomorphic ventricular tachycardia, polymorphic ventricular tachycardia (also known as torsades de pointes), and ventricular fibrillation. Ventricular tachycardia can occur with or without a pulse. Ventricular tachycardia with a pulse is often self-limiting, referred to as nonsustained. Sustained ventricular tachycardia can quickly decompensate into a pulseless rhythm. Ventricular fibrillation is considered a nonperfusing rhythm, meaning that it generates inadequate cardiac output to sustain life and should always be treated as cardiac arrest. Table 2 displays typical ECG tracings for each tachyarrhythmia and a description of key findings for recognizing each rhythm.
| Table 2. Recognition of Tachyarrhythmias on Electrocardiogram43-48 |
|
Type
|
Electrocardiogram
|
Key Findings
|
|
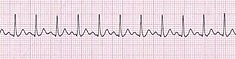
Sinus tachycardia
|
|
Normal cardiac cycle with elevated heartrate
|
|
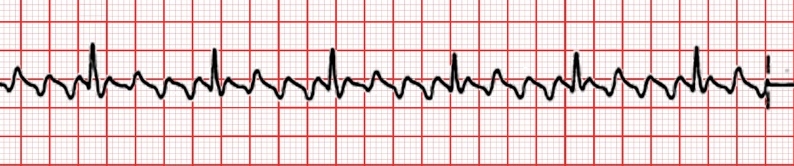
Atrial fibrillation
|
|
Irregular R-R interval; no clear P waves
|
|
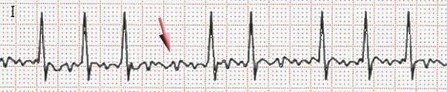
Atrial flutter
|
|
Multiple P waves before each QRS complex; 3:1 in this example
|
|
Supraventricular tachycardia
|

|
Narrow QRS; one P wave before each QRS
|
|
Monomorphic ventricular tachycardia
|
|
Wide QRS complex
|
|
Polymorphic ventricular tachycardia
|
|
Wide QRS complex; torsades de pointes (“twisting of the points”)
|
|
Ventricular fibrillation
|

|
Absence of clear P wave or QRS complex
|
Recognition of Bradyarrhythmias
Bradyarrhythmias are defined as abnormal heart rhythms with ventricular rates below 60 beats per minute. Compared with tachyarrhythmias, bradyarrhythmias are more likely to occur without symptoms. Sinus bradycardia with a heart rate of 40 to 60 beats per minute is common during sleep, in young healthy adults, and in trained athletes.5 Bradycardia also commonly occurs in response to medications that lower the heart rate, such as digoxin, beta-blockers, and nondihydropyridine calcium channel blockers. Other common causes of bradycardia include myocardial ischemia or infarction, hypoxia, and electrolyte abnormalities such as hyperkalemia.6
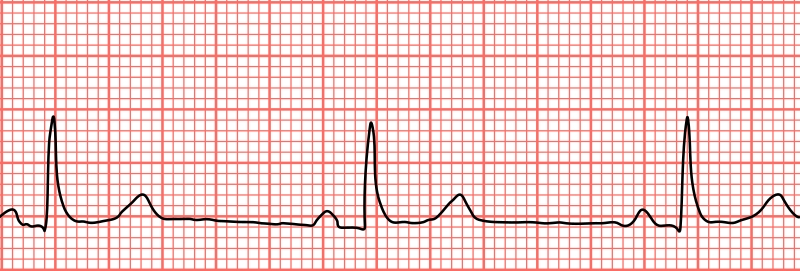
A heart block occurs when there is a disruption in the electrical impulses that control the beating of the heart. Heart blocks are categorized as first degree, second degree types I and II, and third degree.5 First-degree heart block is characterized by a prolonged PR interval, representing a protracted time for the electrical impulse generated in the SA node to travel through the AV node to the ventricles. Second-degree heart block is further characterized as second-degree type I and second-degree type II, also referred to as Mobitz I and Mobitz II, respectively.
In second-degree type I heart block, which is further delineated as Wenchebach, there is a progressive delay between atrial and ventricular contraction until a dropped ventricular beat occurs. On an ECG, the PR interval will appear progressively longer for several beats until there is a P wave (representing atrial depolarization) with no QRS complex (ventricular depolarization) following it. In second-degree type II heart block, the PR interval is consistent for each heartbeat, but there are sporadic dropped ventricular beats (i.e., P waves without a subsequent QRS complex).
In third-degree heart block, there is complete dissociation between atrial and ventricular activity. On an ECG, there will be no identifiable relationship between P wave and QRS complexes. Permanent pacemakers are commonly implanted to manage chronic heart block, especially third degree and symptomatic second degree.
Heart blocks are oftentimes challenging to differentiate on ECG. Table 3 displays typical ECG tracings for each bradyarrhythmia and a description of key findings for differentiating each rhythm.
| Table 3. Recognition of Bradyarrhythmias on Electrocardiogram49,50 |
|
Type
|
Electrocardiogram
|
Key Findings
|
|
Sinus bradycardia
|
|
Normal cardiac cycle with decreased heart rate
|
|
First-degree heart block
|

|
Prolonged PR interval
|
|
Second-degree heart block, type I
|

|
PR interval gets progressively longer prior to dropped QRS
|
|
Second-degree heart block, type II
|

|
Dropped QRS complexes, but consistent PR interval
|
|
Third-degree heart block
|
|
No relationship between P waves and QRS complexes
|
Acute Treatment of Arrhythmias
Generalized Treatment Approach
The American Heart Association (AHA) guidelines for Advanced Cardiovascular Life Support (ACLS) offer treatment algorithms for managing tachycardia and bradycardia with a pulse.6 Initial management principles for both types of arrhythmias are the same and focus on assessing and supporting the patient’s circulation, airway, and breathing (“CAB”), identifying and treating an underlying cause of the abnormal heart rate, and assessing for signs of hemodynamic instability. Blood pressure, pulse oximetry, and the patient’s ability to maintain a patent airway should be the highest priority during the initial assessment of the patient and should be supported as required. Intravenous access should be obtained, a cardiac monitor should be used to assist with rhythm identification and patient monitoring, and a 12-lead ECG should be obtained, if available. It is also advisable at this stage to consider the underlying cause of tachycardia or bradycardia, and measures should be taken to reverse this cause, if possible. For example, if pain is contributing to tachycardia, consider treating the pain. If medications have caused bradycardia, discontinue the offending agents.
Assessment of hemodynamic stability is crucial for guiding treatment decisions. Specifically, the patient should be assessed for hypotension, defined as a systolic blood pressure less than 90 mm Hg or mean arterial pressure less than 65 mm Hg; acutely altered mental status; signs of shock such as cool clammy skin, diaphoresis, or decreased urine output; ischemic chest discomfort; and acute heart failure. If any of these signs or symptoms are present, this constitutes a medical emergency, and appropriate therapy should be promptly initiated.
Acute Treatment of Tachycardia With a Pulse
Unstable tachycardia should be treated urgently with synchronized cardioversion. This nonpharmacologic intervention is similar to defibrillation, which is used in cardiac arrest, in that it delivers electrical energy through the anterior chest wall.7 The key difference is that with synchronized cardioversion, electrical shock is delivered in sync with the QRS complex. In other words, the shock is delivered at the same time as ventricular depolarization. As may be expected, this procedure is painful for the patient. Sedation should be considered before performing synchronized cardioversion. Sedation should be achieved with a single dose of short-acting analgesic and/or sedative agents. The specific choice of agent typically depends on local availability and provider preferences; agents include fentanyl, propofol, midazolam, or ketamine, and similar agents. If synchronized cardioversion is unsuccessful, it can be repeated with an increased level of energy.
Stable tachycardia must be characterized as being wide or narrow complex and as regular or irregular before determining treatment. A wide complex is defined as a QRS complex of 0.12 seconds or greater, while a narrow complex is defined as a QRS of less than 0.12 seconds. The characterization as regular or irregular is based on whether the R-R interval (i.e., the distance between two QRS complexes) is consistent (Table 4).6
Stable, narrow complex, regular tachycardias can be treated with vagal maneuvers or adenosine.6 The vagus nerve stimulates the body’s parasympathetic nervous system to slow down the body’s natural pacemaker, the SA node. Vagal maneuvers are typically performed by the Valsalva maneuver, modified Valsalva maneuver, or diving reflex.8
| Table 4. Acute Treatment Recommendations for Tachyarrhythmias Based on Patient Stability, Width of QRS Complex, and Regularity of Rhythm6 |
|
Stability
|
QRS
|
Regularity
|
Likely Rhythm
|
Treatment Options
|
|
Unstable
|
Narrow
|
Regular
|
Supraventricular tachycardia
|
-
Synchronized cardioversion
-
Can consider adenosine
|
|
Unstable
|
Narrow
|
Irregular
|
Atrial fibrillation
|
-
Synchronized cardioversion
|
|
Unstable
|
Wide
|
Regular
|
Monomorphic ventricular tachycardia
|
-
Synchronized cardioversion
|
|
Unstable
|
Wide
|
Irregular
|
Polymorphic ventricular tachycardia
|
-
Synchronized cardioversion
|
|
Stable
|
Narrow
|
Regular
|
Supraventricular tachycardia
|
-
Vagal maneuvers
-
Adenosine
|
|
Stable
|
Narrow
|
Irregular
|
Atrial fibrillation
|
-
Beta blocker
-
Nondihydropyridine calcium channel blocker
|
|
Stable
|
Wide
|
Regular and monomorphic
|
Monomorphic ventricular tachycardia
|
-
Adenosine
-
Procainamide
-
Amiodarone
-
Sotalol
|
|
Stable
|
Wide
|
Irregular or polymorphic
|
Polymorphic ventricular tachycardia
|
-
Procainamide
-
Amiodarone
-
Sotalol
|
The Valsalva maneuver can be performed in various ways but involves instructing the patient to take a deep breath and then blow out against a closed glottis while in a supine position. Practically, this can be achieved by asking a patient to blow into an empty 10-mL syringe for 10 to 15 seconds. The modified Valsalva maneuver involves the same technique as the original maneuver; however, the patient begins in an upright sitting position and is dropped to a supine position immediately when they begin to blow. At the same time, the legs are extended to a 45- to 90-degree angle, where they are held for 45 to 60 seconds.
The diving reflex involves immersing the patient’s face in a basin of cold water for as long as tolerated. Carotid sinus massage was previously used as a form of vagal maneuver but is no longer recommended due to the risk of inciting a cerebrovascular accident. Vagal maneuvers are fast and simple to perform but have an initial success rate of only 10%-40% and a rate of sustained success of only 3%-30%; therefore, alternative pharmacologic treatment is often required.9
Adenosine slows conduction through the AV node to restore normal sinus rhythm. It is rapidly metabolized in red blood cells and, therefore, should be administered with a rapid intravenous (IV) push followed immediately by a saline flush. The initial dose of adenosine is typically 6 mg. If ineffective, a 12-mg dose can be administered. Patients should be on cardiac monitoring while receiving adenosine. After administering adenosine, the electrical tracing typically displays a brief period of a flat line (i.e., asystole). If adenosine is effective, this will be followed by the restoration of normal sinus rhythm. If ineffective, this will be followed by a return to the tachyarrhythmia. Common adverse reactions include flushing, dyspnea, headache, dizziness, and gastrointestinal distress. Rarely, new cardiac arrhythmias or prolonged asystole can occur. Caution should be used in patients with asthma due to the risk of severe bronchospasm and in patients who have undergone heart transplantation, as they may experience a more profound effect from adenosine.10
In patients with extremely high heart rates, it can be difficult to differentiate supraventricular tachycardia from atrial fibrillation. Adenosine will be ineffective if the rhythm is atrial fibrillation; however, it may slow the heart rate temporarily to allow for proper rhythm identification. Beta-blockers and nondihydropyridine calcium channel blockers are the preferred therapies for atrial fibrillation and atrial flutter.6 Wide complex, stable tachycardias are typically treated with antiarrhythmic agents, including procainamide, amiodarone, or sotalol.
Acute Treatment of Bradycardia With a Pulse
For patients experiencing asymptomatic bradycardia, AHA guidelines recommend monitoring and observing the patient.6 In many cases, the bradycardia will resolve. If the patient becomes symptomatic, then pharmacologic treatment can be initiated. The first line therapy for symptomatic bradycardia is atropine, which blocks acetylcholine at parasympathetic sites, thereby increasing firing of the SA node. It can be repeated every 3 to 5 minutes for up to 3 doses.
When atropine is ineffective, second-line therapies include dopamine or epinephrine administered as a continuous IV infusion or transcutaneous pacing. Both dopamine and epinephrine exert their therapeutic effect in treating bradycardia through their activity at β1 receptors in the heart. Transcutaneous pacing is a temporary measure in which small pulses of electrical current are delivered through the chest to stimulate cardiac contraction. It can be used until the underlying cause of bradycardia is resolved or until a permanent pacemaker can be placed.
Evidence is limited comparing the alternative therapies for symptomatic bradycardia, and all have a similar strength of recommendation in guidelines.6 PrePACE was a feasibility trial that randomized 82 patients with symptomatic bradycardia who failed to respond to atropine to receive either dopamine or transcutaneous pacing. No difference was observed in 30-day mortality; however, 1,380 patients would be needed to detect a 10% relative mortality difference, so this finding is not surprising given the intent of the study to determine feasibility.11
Typical dosing of medications used to manage tachyarrhythmias and bradyarrhythmia is summarized in Table 5.
| Table 5. Dosing of Medications Used for Tachyarrhythmias, Bradyarrhythmias, and Cardiac Arrest6 |
|
Adult Cardiac Arrest
|
Adult Tachycardia With Pulse
|
Adult Bradycardia With Pulse
|
Epinephrine IV/IO
-
1 mg every 3 to 5 minutes
|
Adenosine IV
-
First dose: 6 mg rapid IV push
-
Second dose: 12 mg
-
Always follow with NS flush
|
Atropine IV
-
1 mg bolus every 3–5 minutes
-
Maximum: 3 mg
|
Amiodarone IV/IO
-
First dose: 300 mg bolus
-
Second dose: 150 mg bolus
|
Procainamide IV
-
Initially 20–50 mg/min
-
Maintenance infusion: 1–4 mg/min
-
Maximum: 17 mg/kg
-
Avoid if prolonged QT or congestive heart failure
|
Dopamine IV
-
5–20 mcg/kg per minute
-
Titrate to patient response; taper slowly
|
Lidocaine IV/IO
-
First dose: 1–1.5 mg/kg
-
Second dose: 0.5–0.75 mg/kg
|
Amiodarone IV
-
First dose: 150 mg over 10 minutes
-
Maintenance infusion: 1 mg/min for first 6 hours
|
Epinephrine IV
-
2-10 mcg per minute
-
Titrate to patient response
|
|
Sotalol IV
-
100 mg (1.5 mg/kg) over 5 minutes.
-
Avoid if prolonged QT
|
|
Cardiac Arrest
Cardiac arrest is defined as the cessation of cardiac mechanical activity and is ultimately confirmed by the absence of circulation.12 An estimated 300,000 or more Americans experience an out-of-hospital cardiac arrest (OHCA) each year, with an incidence of approximately 92 per 100,000 people.12 Only about 7% of patients who experience OHCA survive to hospital discharge, and asystole is the most common presenting rhythm.12 The incidence of in-hospital cardiac arrest (IHCA) is approximately 10 per 1,000 hospital admissions, with a higher survival-to-discharge rate of 23%. While outcomes following IHCA have improved over the last decade, the rate of return of spontaneous circulation (ROSC) following OHCA has been essentially unchanged since 2012.13 In 2020, sudden cardiac arrest was reported as the underlying cause of mortality in about 20,000 Americans.
The primary focus in the treatment of adult cardiac arrest is prompt recognition of a cardiovascular event, immediate initiation of cardiopulmonary resuscitation (CPR), and defibrillation in the case of shockable rhythms. While the resuscitation process may vary for OHCA and IHCA, quick response remains critical. Furthermore, the probability of a patient’s survival with a favorable neurologic outcome is markedly increased with immediate CPR and the use of an automated external defibrillator (AED).14,15
In OHCA, the patient’s care is largely dependent upon community members and their responses. When OHCA is witnessed, the chance of survival to hospital discharge can triple if the presenting rhythm is shockable.12 For every minute that passes after arrest, the chance of survival from ventricular fibrillation declines by 7%-10% without bystander CPR. Bystander intervention allows for a more gradual decline in the chance of survival by about 3%-4% per minute.16 lay rescuer can assume cardiac arrest if the person is unconscious or unresponsive with absent or abnormal breathing (slow, irregular gasps).
Upon recognition of cardiac arrest, community members should call 911 or a local emergency response number, immediately perform CPR, and use an AED. There is overwhelming evidence that hands-only (chest compression only) CPR in the OHCA setting is associated with better patient outcomes than compressions with breaths.17-19 Hands-only CPR limits interruptions in chest compressions to give breaths (which are often inadequate) and reduces the reluctance of bystanders to participate.17 Additionally, studies have shown there is little risk of injury if CPR is performed on a person later found not to have cardiac arrest.20 The benefit of initiation of CPR outweighs the risk of providing chest compressions to someone who is not in cardiac arrest.6,20
In IHCA, clinical deterioration often precedes cardiac arrest, which is why recognition of early warning signs and prevention is the first link in the AHA IHCA Chain of Survival (Figure 2). Nonshockable rhythms (i.e., pulseless electrical activity and asystole) are the most common rhythms identified during IHCA, accounting for approximately 81% of cases.21
| Figure 2. American Heart Association Chain of Survival for Cardiac Arrest6 |
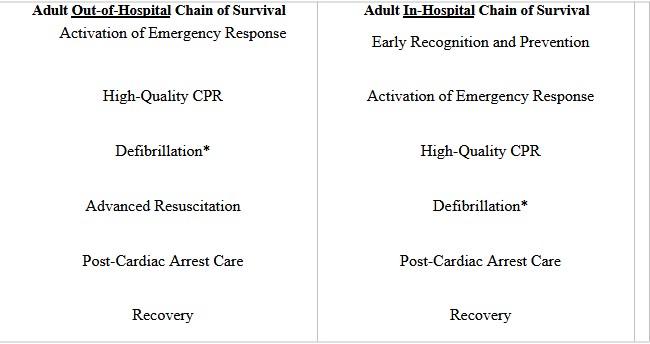 |
Adapted from AHA 2020 Adult BLS and ACLS Guidelines6
*In the out-of-hospital setting, defibrillation may be initiated during bystander CPR through the use of an automated external defibrillator (AED). When emergency medical services or other healthcare providers are performing CPR, defibrillation is typically delivered through a manual defibrillator based on the healthcare providers assessment of the cardiac arrest rhythm.
|
Common Causes of Cardiac Arrest
Cardiac arrest in specific patient populations requires rapid identification of potential causes and immediate treatment. The most common causes of sudden OHCA in adults are myocardial infarction and electrolyte disturbances.6 Identifying and treating reversible underlying causes is an integral aspect of the AHA ACLS Adult Cardiac Arrest Algorithm in the presence of both shockable and nonshockable rhythms.
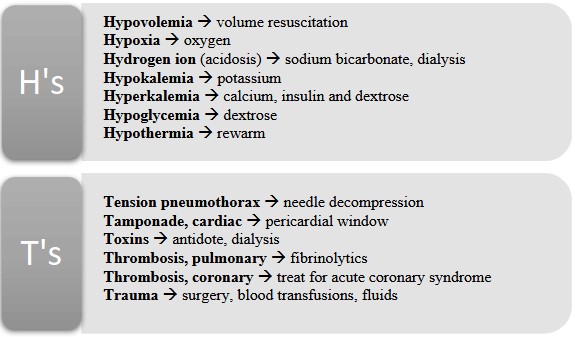
Common reversible causes are listed in Figure 3. These are especially important considerations in the event of cardiac arrest without cardiac origin (e.g., respiratory arrest, pulmonary embolism, drowning, opioid overdose) and in the presence of a nonshockable rhythm. The recent exponential rise of opioid-associated OHCA correlated with the ongoing opioid epidemic necessitates careful evaluation, and patients should be treated appropriately with naloxone when an overdose is suspected.22 As with other medications administered during cardiac arrest resuscitation, CPR should not be delayed for medication administration; rather, naloxone can be administered while CPR is underway.
| Figure 3. Assessment and Potential Treatments of Reversible Causes of Cardiac Arrest6 |
 |
High-Quality Cardiopulmonary Resuscitation
For patients in cardiac arrest, high-quality CPR is the most important intervention for survival.23 Whenever cardiac arrest is identified, CPR should be initiated immediately regardless of the arrest rhythm. High-quality CPR includes a rate of 100 to 120 compressions per minute, a depth of 2 to 2.4 inches (5.1 to 6.1 cm) in adults, full chest recoil, minimization of interruptions, and avoidance of excessive ventilation. Utilization of the rate of 100 to 120 compressions per minute has been associated with increased survival to hospital discharge following out-of-hospital cardiac arrest compared to both faster and slower rates of chest compressions.23 During a rhythm check or defibrillation, the pause of chest compressions should be no more than 10 seconds, and CPR should be immediately resumed if no pulse is found or once a shock is delivered.6 In an effort to increase the quality of chest compressions, guidelines recommend switching the compressor approximately every 2 minutes if more than one rescuer is available.
For real-time optimization of CPR quality, audiovisual feedback devices may be incorporated. These devices can give feedback on compression rate, depth, and chest wall recoil and have been associated with an increase in survival to hospital discharge.24 Feedback is essential in the provision of high-quality CPR, and the use of devices with various feedback mechanisms is encouraged by the AHA, especially as rescuers become fatigued.6
Recommendations have recently changed to emphasize the importance of immediate chest compressions and minimization of any interruptions because the impact of ventilation and oxygenation remains less clear.20 In patients without an advanced airway (i.e., without an endotracheal tube or supraglottic device), breaths can be delivered by mouth or bag-mask ventilation with just enough volume to produce visible chest rise.6 Healthcare personnel must ensure an open airway for proper ventilation and oxygenation during CPR with rescue breaths. When no head or neck injury is suspected, a trained rescuer should open the airway using the head tilt-chin lift maneuver and provide a compression-to-breath ratio of 30:2. Lay rescuers who are untrained or unwilling to provide respirations should continue with chest compression-only CPR until another provider is able to administer breaths. Once emergency medical service (EMS) personnel arrive, they may place an advanced airway and use a ventilation rate of 1 breath every 6 seconds during continuous chest compressions.
Rhythm Classification Determines Treatment
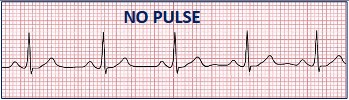
After recognition of cardiac arrest and initiation of CPR, the first decision point in the AHA ACLS algorithm is whether or not the rhythm observed is shockable. Shockable rhythms include ventricular fibrillation (VF) and pulseless ventricular tachycardia (pVT), and nonshockable rhythms include asystole and pulseless electrical activity (PEA). PEA represents electrical activity with no mechanical activity or cardiac output. It is recognized on ECG by any organized appearing rhythm (other than VT or VF) in the absence of a pulse. In other words, PEA may appear like sinus tachycardia (or any other rhythm) on an ECG, but no pulse is present. Identifying a shockable versus nonshockable arrest rhythm is a crucial decision point for the provider, as the treatment course varies depending on the rhythm observed at each rhythm check. An overview of cardiac arrest rhythms can be found in Table 6.
| Table 6. Recognition of Cardiac Arrest Rhythms47,48,51-53 |
|
Rhythm
|
Electrocardiogram
|
Shockable
|
|
Asystole
|

|
Nonshockable
|
|
Pulseless electrical activity
|
|
Nonshockable
|
|
Monomorphic pulseless ventricular tachycardia
|

|
Shockable
|
|
Polymorphic pulseless ventricular tachycardia
|
|
Shockable
|
|
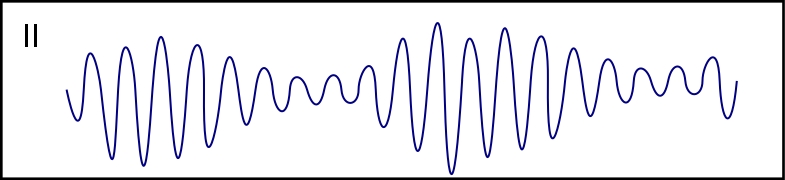
Ventricular fibrillation
|
|
Shockable
|
When resuscitation from cardiac arrest is performed in the community setting by emergency medical personnel or in the hospital setting by other healthcare providers, a manual cardiac monitor/defibrillator is used. The provider is tasked with recognizing the arrest rhythm and determining whether it is shockable or nonshockable, then programming the manual defibrillator to deliver a shock, if indicated.
When a layperson in the community setting performs CPR, AEDs should be used whenever available, as they provide the fundamental step of assessing the cardiac arrest rhythm. Operating an AED requires 2 simple steps: (1) turn on the AED and (2) follow the step-by-step voice instructions. The AED will prompt the operator to position the electrode pads on the victim’s bare chest. The AED then automatically analyzes the person’s heart rhythm and announces whether a shock is indicated. If needed, the AED will prompt the operator to remain clear from the patient and then press a button (usually identified by a flashing light) to deploy the shock. After the shock is delivered, the AED will instruct the operator to resume chest compressions. The process of analyzing the rhythm and shocking, if indicated, will automatically repeat every 2 minutes. Pharmacists working in the community or outpatient setting should familiarize themselves with the location and operating principles of AEDs so that they are prepared to respond to a cardiac arrest event.
Nonshockable Rhythms
If the patient is found to be in a nonshockable rhythm (asystole or PEA), epinephrine 1 mg intravenous push should be administered as quickly as possible, and CPR should continue with rhythm checks every 2 minutes (Figure 4). In OHCA, epinephrine has been found to increase the achievement of ROSC, survival to hospital admission, and 3-month survival, and early administration has been associated with improved patient outcomes.25 It is also crucial to consider reversible causes, as treatment of asystole and PEA depends heavily on identifying and correcting the underlying cause.
| Figure 4. Overview of Cardiac Arrest Treatment Strategies6 |
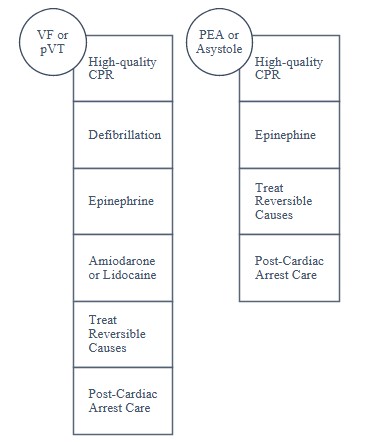 |
Shockable Rhythms
Shockable rhythms (pVT or VF) should be approached with immediate defibrillation while still maintaining minimal interruptions in CPR due to evidence of increased survival.6,16 Defibrillation serves to terminate pVT/VF resulting in a perfusing cardiac rhythm, and it is often necessary to restore a sinus rhythm.17 Optimizing patient outcomes in the community setting with early defibrillation using AEDs is a critical aspect of managing OHCA because of the possibility of shockable rhythms. Additionally, epinephrine administration in pVT/VF is recommended in the event that initial defibrillation attempts have failed, and sequential administration of amiodarone or lidocaine can be considered.
Antiarrhythmic agents such as amiodarone and lidocaine prevent the recurrence of pVT/VF, but evidence showing improved survival to hospital discharge is lacking.17 The 2020 AHA ACLS guidelines recommend that either amiodarone or lidocaine be administered during cardiac arrest with shockable rhythms, with no preference given to either agent. A retrospective cohort study published in 2023, however, included over 14,000 patients receiving either amiodarone or lidocaine for VT/VF IHCA and found that, compared to amiodarone, lidocaine was associated with higher odds of ROSC, 24-hour survival, survival to hospital discharge, and favorable neurologic outcome at hospital discharge.26
When performing defibrillation, a biphasic waveform defibrillator with a single shock strategy is recommended. Depending on the skillset of the operator in the healthcare setting, the defibrillator may be used in manual mode to eliminate the hands-off time for rhythm analysis that AEDs require (note that a brief hand-off time will still be required to deliver the shock).6 After the shock is administered, whether via manual defibrillation or AED, chest compressions should be immediately resumed. It is preferable to resume chest compressions and not perform a rhythm or pulse check because of the improvement in the chest compression fraction during resuscitation. This increased hands-on time has been associated with improved survival to hospital discharge in VF.27,28
Routes of Drug Administration
Providers should first attempt to establish IV access for drug administration.6 However, this can be challenging based on patient characteristics or provider experience.
If the provider is unable to place a peripheral IV, alternatives can be considered: intraosseous (IO), endotracheal (ET), intracardiac, and central venous routes. IO and ET access may be established in the prehospital setting by EMS; the intracardiac and central venous routes are reserved for the hospital setting. Notably, IO is the preferred alternative and is established as a reasonable option if IV attempts are unsuccessful.6 IO access is obtained by placing a hollow bore needle through the cortex of a bone into the medullary space. The preferred sites for IO access in adults are the proximal tibia, humeral head, and sternum. IO access kits include specialized needles and a drill (e.g., EZ-IO) are readily available to EMS and hospital staff and can be used to quickly obtain IO access with high success rates.29 Medications traditionally given via the IV route can be administered IO at the same dose and frequency. The intracardiac route is not preferred because of the highly invasive nature requiring a specialized skill set and because of the high potential for morbidity.30Appropriately trained healthcare providers may attempt central venous access if IV and IO access are unsuccessful because of the potential for interruptions and morbidity.
The ET route can be considered only when other access routes are not available and is the least preferred route of administration because of unpredictable drug concentrations and lower rates of survival.31,32 The ET route is obtained via endotracheal intubation and medications are administered directly into the endotracheal tube. When the ET route is used, the dose administered should typically be 2 to 2.5 times that of the typical IV dose (e.g., epinephrine 2–3 mg ET versus epinephrine 1 mg IV). The acronym NAVEL is used to describe ACLS medications that can be administered by the ET route: naloxone, atropine, vasopressin (or Valium [diazepam]), epinephrine, lidocaine. Given the accessibility of IO access kits and the ease of their use, the ET route is rarely used.
CARE AFTER Cardiac Arrest
Return of Spontaneous Circulation
ROSC can be identified by the presence of blood pressure and a pulse, or an abrupt sustained increase in end-tidal carbon dioxide (ETCO2), typically 40 mm Hg or higher. There are 2 main phases to post-cardiac arrest care: (1) the initial stabilization phase and (2) continued management and additional emergent activities. The AHA emphasizes that once ROSC is achieved, resuscitation continues and requires a comprehensive, multidisciplinary system of care. When ROSC is achieved in the prehospital setting, the stabilization phase of post–cardiac arrest care should be performed. The patient should be transported to the nearest hospital with intensive care and cardiac intervention services.
Initial Stabilization Phase
In the immediate post-ROSC phase, healthcare providers should focus on the management of the patient’s airway, breathing, and circulation. These interventions may occur simultaneously. Airway management should be obtained through the placement of an endotracheal tube if necessary, and confirming its placement with waveform capnography. Respiratory parameters include maintaining SpO2 (oxygen saturation) at 92%–98%, starting at 10 breaths per minute, while titrating to PaCO2 (arterial partial pressure of carbon dioxide) of 35–45 mm Hg. Healthcare providers should then administer crystalloid and/or vasopressors or inotrope to avoid hypotension and reach a goal systolic blood pressure of >90 mm Hg or mean arterial pressure of >65 mm Hg.
Emergency Cardiac Intervention
A 12-lead ECG should be obtained as soon as possible after ROSC is achieved to identify an ST-segment elevation myocardial infarction (STEMI). This serves to support the decision of emergent cardiac intervention when STEMI or unstable cardiogenic shock is present. The AHA recommends coronary angiography to be performed on all patients with suspected cardiac cause of arrest and STEMI on ECG. Revascularization via percutaneous coronary intervention (PCI) may be necessary.
Targeted Temperature Management
Following the stabilization phase, all patients should receive a neurologic exam. Further workup of patients who are comatose should include a computed tomography scan of the head and electroencephalogram (EEG) monitoring. The 2020 AHA ACLS guidelines recommend targeted temperature management (TTM) for any patient who does not follow commands after ROSC. Even in an intubated patient, the ability to follow commands can be assessed by simple directives such as, “squeeze my hand” or “wiggle your toes.” When TTM is used, it has been associated with favorable neurologic outcomes in some studies.33,34
According to AHA guidelines, TTM includes maintenance of body temperature at 32°C to 36°C for at least 24 hours.6 Adjunctive therapies during TTM include deep analgesia and sedation to maintain a Richmond Agitation Sedation Scale (RASS) score of –4 or –5; deep sedation with or without neuromuscular blocking agents to treat and prevent shivering; EEG monitoring and treatment of seizures if indicated; and frequent monitoring and repletion of electrolytes (especially potassium, magnesium, and phosphate) and blood glucose.
Despite guideline recommendations in support of TTM, its utility following cardiac arrest is an area of controversy due to clinical trials with conflicting results. Notable trials that demonstrated the benefit of TTM include HACA (2002) and HYPERION (2019), which found favorable neurologic outcomes and increased survival in the groups randomized to hypothermia.33,35 The TTM Trial (2013) failed to show a benefit of TTM.36 These studies were criticized, however, due to inclusion of patient populations that limit external generalizability, allowance of hyperthermia in some control groups, and baseline differences between study groups that could impact outcomes.37,38
Most recently, the TTM2 trial, published in 2021, was the largest randomized controlled trial of TTM in cardiac arrest to date. TTM2 included 1,900 patients following OHCA who were randomized to undergo targeted hypothermia at 33°C, followed by controlled rewarming, or targeted normothermia with early treatment of fever (body temperature, ≥37.8°C). Among the 1,850 participants who were evaluated for a primary outcome of death from any cause at 6 months, the difference between the groups was not significant (50% in the TTM group and 48% in the normothermia group, P = 0.37).39
Of note, landmark trials related to TTM in cardiac arrest have had major differences in their inclusion criteria related to out-of-hospital versus in-hospital arrest and shockable versus nonshockable rhythms. Differences in study protocols also exist, particularly related to the degree of temperature control in the “normothermia” group. One school of thought is that targeting normothermia instead of hypothermia (i.e., using cooling measures to avoid fever) may exert the greatest therapeutic benefits. Others believe that specific patient populations may benefit from targeted hypothermia, but these specific subgroups have yet to be clearly identified in the literature. Guideline recommendations from the AHA, the European Resuscitation Council, and the Australian and New Zealand Committee on Resuscitation all recommend TTM targeting hypothermia, but all were updated before the publication of TTM2.6,40,41 It will be interesting to see the impact of TTM2 on guideline recommendations in the future.
Conclusion
Cardiovascular emergencies are common, and prompt recognition and treatment can minimize morbidity and mortality. Whether in a community or ambulatory setting, as a witness to an OHCA, or happening to be present when an AED is needed, pharmacists are well-positioned to use their CPR training and knowledge of cardiovascular therapy to optimize a victim’s chance of survival. The AHA provides a list of the top 10 take-home messages for adult cardiovascular life support, as summarized here6:
REFERENCES
1. Adam L. Potential benefits of pharmacist intervention in the detection and therapy of atrial fibrillation. Can Pharm J (Ott). 2021;154:240-241.
2. Al-Arkee S, Mason J, Lindenmeyer A, Jalal Z. Pharmacist management of atrial fibrillation in UK primary care: a qualitative study. J Pharm Pol Pract. 2022;15:98.
3. Metkus TS. A focused step-wise guide to ECG interpretation. ECG Rounds. New York, NY: McGraw-Hill Education; 2016.
4. Gopinathannair R, Olshansky B. Management of tachycardia. F1000Prime Rep. 2015;7:60.
5. Sidhu S, Marine JE. Evaluating and managing bradycardia. Trends Cardiovasc Med. 2020;30:265-272.
6. Panchal AR, Bartos JA, Cabanas JG, et al. Part 3: Adult basic and advanced life support: 2020 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2020;142:S366-S468.
7. Goyal A, Sciammarella JC, Chhabra L, Singhal M. Synchronized electrical cardioversion. StatPearls. Treasure Island (FL): StatPearls Publishing LLC; 2023.
8. Niehues LJ, Klovenski V. Vagal maneuver. StatPearls. Treasure Island (FL): StatPearls Publishing LLC; 2023.
9. Ceylan E, Ozpolat C, Onur O, Akoglu H, Denizbasi A. Initial and sustained response effects of 3 vagal maneuvers in supraventricular tachycardia: a randomized, clinical trial. J Emerg Med. 2019;57:299-305.
10. Singh S, McKintosh R. Adenosine. StatPearls. Treasure Island (FL): StatPearls Publishing LLC; 2023.
11. Morrison LJ, Long J, Vermeulen M, et al. A randomized controlled feasibility trial comparing safety and effectiveness of prehospital pacing versus conventional treatment: 'PrePACE'. Resuscitation. 2008;76:341-349.
12. Tsao CW, Aday AW, Almarzooq ZI, et al. Heart disease and stroke statistics—2023 update: a report from the American Heart Association. Circulation. 2023;147:e93-e621.
13. Virani SS, Alonso A, Benjamin EJ, et al. Heart disease and stroke statistics—2020 update: a report from the American Heart Association. Circulation. 2020;141:e139-e596.
14. Komori A, Iriyama H, Abe T. Impact of defibrillation with automated external defibrillator by bystander before defibrillation by emergency medical system personnel on neurological outcome of out-of-hospital cardiac arrest with non-cardiac etiology. Resusc Plus. 2023;13:100363.
15. Brooks SC, Clegg GR, Bray J, et al. Optimizing outcomes after out-of-hospital cardiac arrest with innovative approaches to public-access defibrillation: a scientific statement from the International Liaison Committee on Resuscitation. Resuscitation. 2022;172:204-228.
16. Larsen MP, Eisenberg MS, Cummins RO, Hallstrom AP. Predicting survival from out-of-hospital cardiac arrest: a graphic model. Ann Emerg Med. 1993;22:1652-1658.
17. Barletta JF. Cardiopulmonary arrest. In: DiPiro JT, Yee GC, Haines ST, Nolin TD, Ellingrod VL, Posey LM, eds. DiPiro’s Pharmacotherapy: A Pathophysiologic Approach, 12e. New York, NY: McGraw Hill; 2023.
18. Sayre MR, Berg RA, Cave DM, et al. Hands-only (compression-only) cardiopulmonary resuscitation: a call to action for bystander response to adults who experience out-of-hospital sudden cardiac arrest: a science advisory for the public from the American Heart Association Emergency Cardiovascular Care Committee. Circulation. 2008;117:2162-2167.
19. Cabrini L, Biondi-Zoccai G, Landoni G, et al. Bystander-initiated chest compression-only CPR is better than standard CPR in out-of-hospital cardiac arrest. HSR Proc Intensive Care Cardiovasc Anesth. 2010;2:279-285.
20. Olasveengen TM, Mancini ME, Perkins GD, et al. Adult basic life support: 2020 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Circulation. 2020;142:S41-S91.
21. Andersen LW, Holmberg MJ, Berg KM, Donnino MW, Granfeldt A. In-hospital cardiac arrest: a review. JAMA. 2019;321:1200-1210.
22. Dezfulian C, Orkin AM, Maron BA, et al. Opioid-associated out-of-hospital cardiac arrest: distinctive clinical features and implications for health care and public responses: a scientific statement from the American Heart Association. Circulation. 2021;143:e836-e870.
23. Idris AH, Guffey D, Pepe PE, et al. Chest compression rates and survival following out-of-hospital cardiac arrest. Crit Care Med. 2015;43:840-848.
24. Berg RA, Hemphill R, Abella BS, et al. Part 5: adult basic life support: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010;122:S685-S705.
25. Holmberg MJ, Issa MS, Moskowitz A, et al. Vasopressors during adult cardiac arrest: a systematic review and meta-analysis. Resuscitation. 2019;139:106-121.
26. Wagner D, Kronick SL, Nawer H, Cranford JA, Bradley SM, Neumar RW. Comparative effectiveness of amiodarone and lidocaine for the treatment of in-hospital cardiac arrest. Chest. 2023;163:1109-1119.
27. Cheskes S, Schmicker RH, Christenson J, et al. Perishock pause: an independent predictor of survival from out-of-hospital shockable cardiac arrest. Circulation. 2011;124:58-66.
28. Rea TD, Helbock M, Perry S, et al. Increasing use of cardiopulmonary resuscitation during out-of-hospital ventricular fibrillation arrest: survival implications of guideline changes. Circulation. 2006;114:2760-2765.
29. Luck RP, Haines C, Mull CC. Intraosseous access. J Emerg Med. 2010;39:468-475.
30. Guidelines 2000 for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Part 6: advanced cardiovascular life support: section 6: pharmacology II: agents to optimize cardiac output and blood pressure. The American Heart Association in collaboration with the International Liaison Committee on Resuscitation. Circulation. 2000;102:I129-I135.
31. Neumar RW, Otto CW, Link MS, et al. Part 8: Adult advanced cardiovascular life support: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010;122:S729-S767.
32. Niemann JT, Stratton SJ, Cruz B, Lewis RJ. Endotracheal drug administration during out-of-hospital resuscitation: where are the survivors? Resuscitation. 2002;53:153-157.
33. Lascarrou J-B, Merdji H, Le Gouge A, et al. Targeted temperature management for cardiac arrest with nonshockable rhythm. N Engl J Med. 2019;381:2327-2337.
34. The Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346:549-556.
35. Lascarrou J-B, Merdji H, Le Gouge A, et al. Targeted temperature management for cardiac arrest with nonshockable rhythm. N Engl J Med. 2019;381:2327-2337.
36. Nielsen N, Wetterslev J, Cronberg T, et al. Targeted temperature management at 33°C versus 36°C after cardiac arrest. N Engl J Med. 2013;369:2197-2206.
37. Zeiner A, Holzer M, Sterz F, et al. Hyperthermia after cardiac arrest is associated with an unfavorable neurologic outcome. Arch Intern Med. 2001;161:2007-2012.
38. Cocchi MN, Boone MD, Giberson B, et al. Fever after rewarming: incidence of pyrexia in postcardiac arrest patients who have undergone mild therapeutic hypothermia. J Intens Care Med. 2014;29:365-369.
39. Dankiewicz J, Cronberg T, Lilja G, et al. Hypothermia versus normothermia after out-of-hospital cardiac arrest. N Engl J Med. 2021;384:2283-2294.
40. Soar J, Böttiger BW, Carli P, et al. European Resuscitation Council Guidelines 2021: adult advanced life support. Resuscitation. 2021;161:115-151.
41. ANZCOR. ANZCOR guideline 11.8 - targeted temperature management (TTM) after cardiac arrest. 2016.
42. "File:2028 cardiac cycle vs electrocardiogram.jpg," by OpenStax College is licensed under CC BY 3.0. To view a copy of this license, visit https://creativecommons.org/licenses/by/3.0?ref=openverse.
43. "Sinus tachycardia unlabeled." To view a copy of this license, visit https://creativecommons.org/licenses/by-sa/3.0/?ref=openverse.
44. "Afib_ecg." To view a copy of this license, visit https://creativecommons.org/licenses/by/3.0?ref=openverse.
45. "Tachykardie_supraventrikulaer.jpg," by Kalumet, selbst erstellt is licensed under CC BY 30. To view a copy of this license, visit https://creativecommons.org/licenses/by/3.0?ref=openverse.
46. "File:E24 (CardioNetworks ECGpedia).jpg." To view a copy of this license, visit https://creativecommons.org/licenses/by-sa/3.0/?ref=openverse.
47. "Lead_II_rhythm_ventricular_tachycardia_Vtach_VT.JPG," by Glenlarson is licensed under CC BY-SA 30 To view a copy of this license, visit https://creativecommons.org/licenses/by-sa/3.0/?ref=openverse.
48. "Tdp small (CardioNetworks ECGpedia).svg." To view a copy of this license, visit https://creativecommons.org/licenses/by-sa/3.0/?ref=openverse.
49. "Sinus Bradycardia." To view a copy of this license, visit https://creativecommons.org/licenses/by-sa/3.0/?ref=openverse.
50. "Heart block." To view a copy of this license, visit https://creativecommons.org/licenses/by-sa/4.0/?ref=openverse.
51. "File:EKG Asystole.jpg." To view a copy of this license, visit https://creativecommons.org/licenses/by-sa/3.0/?ref=openverse.
52. "Normal Sinus Rhythm Unlabeled." To view a copy of this license, visit https://creativecommons.org/licenses/by-sa/3.0/?ref=openverse.
53. "File:Ventricular fibrillation.png." To view a copy of this license, visit https://creativecommons.org/licenses/by-sa/3.0/?ref=openverse..