ADVERTISEMENT

Risks and Benefits of Prevention and Screening in the Elderly: Keeping Your Patients Safe from the Complications of Aging
INTRODUCTION
Some preventive interventions, such as vaccinations, have minimal risks and clear public health benefits (eg, prevention of disease, reduced severity of illness, reduced risk of hospitalization).1 However, many other interventions, such as cancer screening tests impose risks and burdens on patients (eg, false positives, false negatives, overdiagnosis of symptomless cancers), complicating the decision of who should receive the intervention.2 Targeting is less important for interventions with minimal risks since many patients will benefit and few will be harmed.1 In contrast, targeting is important for preventive interventions with risks since some patients may be more likely to be harmed than helped by the intervention.1
While it is important to provide screening efforts in the elderly population, it is necessary to decide which preventive efforts will clearly produce a health benefit while keeping the patient safe from unnecessary harm. Some questions that need to be addressed by an elderly patient considering a screening should include3:
-
How likely am I to get the disease at my age?
-
Would detecting the disease early benefit my health in the long-term? For instance, is there any scientific proof that it might help me live longer?
-
What adverse effects might be associated with the screening test, with possible tests following screening, and with the treatment?
-
How common are false-positive and false-negative test results?
-
Will more tests follow if results are positive?3
Consideration of these key points is critical to making an informed decision about whether to participate in screenings and other preventive measures and is an important conversation that elderly patients should be having with health care professionals. While screening in this population may help to prevent the complications of aging, it may also produce unnecessary risks that need to be weighed against the benefits.
SCREENING AND DISEASE PREVENTION
It is often conveyed that screenings can prevent diseases. However, a screening program can only be considered to be a preventive measure if it determines and influences risk factors or detects and treats abnormal changes that could develop into a disease. For example, an endoscopy, which detects and removes intestinal polyps that could later develop into cancer.3
A disadvantage of screening is that many people have treatment even though the disease would never have developed.3 Many abnormal changes do not necessarily develop into a more serious condition or might even go back to normal without causing any health problems.3 For example, most precancerous cells will not turn into cancer.4 They are abnormal cells that could turn into cancerous cells, but which, by themselves, are not invasive or spreading.4 Overdiagnosis or treatment of preclinical cancers that would have never caused symptoms or pose a serious health threat may lead to unnecessary treatment that injures the patient.2 This does not imply that screening is inconsequential, and it is certainly relevant in cervical, colorectal, and breast cancers.2
The World Health Organization (WHO) has defined criteria for evaluating population-wide screening, which include the following3:
-
Screening should be done only for diseases with serious consequences
-
The test must be reliable and not harmful
-
There must be an effective treatment for the disease when detected at an early stage
-
There must be scientific proof that that treatment is more effective when started before symptoms arise.3
FRAMEWORK FOR INDIVIDUALIZING PREVENTION
Since few studies of preventive interventions have included the elderly, it is difficult to extrapolate the results to this population.1 Even if trials show effectiveness of an intervention, they generally do not address individual patient characteristics (eg, comorbid conditions, functional status), which may change the likelihood of receiving benefit or harm from a preventive intervention.1 This makes it especially important to individualize prevention and screening decisions in the older population considering the combination of health, function, remaining life expectancy, and values with advancing age.1 A framework has been developed to help determine patients who are most likely to benefit if they receive the intervention and patients who are more likely to be harmed and should avoid the intervention. The algorithm (ie, screening process) is described below.
Estimate Life Expectancy
Many preventive interventions expose patients to risks immediately for the promise of improved health later.1 However, older patients with a limited life expectancy may be unlikely to survive long enough to benefit from prevention. For example, finding an asymptomatic disease in a person who will die of something else before the disease becomes symptomatic does not produce benefit and may cause considerable harm. Therefore, it is important to determine life expectancy when making decisions about preventive measures in the elderly population.1
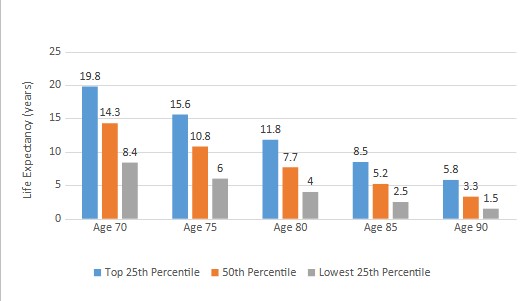
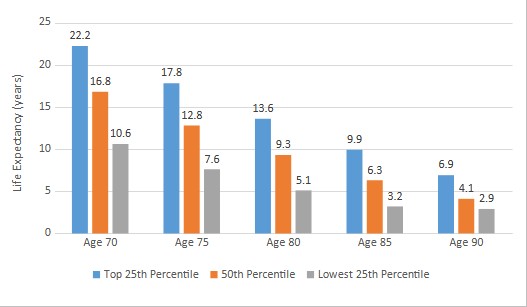
Although it is impossible to predict the exact life expectancy of an individual person, life table data can be used to estimate life expectancy for the average person at any age.5 To account for patients who may be healthier or less healthy than the average person in their age group, life tables can provide the life expectancy of the healthiest and least healthy quartile. Figures 1 and 2 provide a general idea of the distribution of life expectancies at various ages as predicted by United States (US) life table data.5
| Figure 1. Life Expectancy for Men5 |
 |
| Figure 2. Life Expectancy for Women5 |
 |
Instructions:
If you experience any of these discomforts, circle the number indicating its intensity. Please note that discomfort associated with lactose intolerance is typically experienced 30 minutes to 2 hours after eating dairy or foods containing dairy.
The intensity of discomfort is ranked 1=none, 3=mild, 5=severe |
In addition to using life tables, general mortality risk calculators have been developed and validated for older adults.1 There are numerous risk calculators specific to life-limiting conditions (eg, cancer, dementia, heart disease, lung disease).1 These mortality risk calculators have been gathered at https://eprognosis.ucsf.edu/index.php. A patient’s age, comorbidities, and functional limitations can be entered into a risk calculator to obtain an evidence-based estimate of mortality risk and life expectancy.6
Determine the Time-To-Benefit for a Preventive Intervention
For preventive interventions that expose patients to immediate risks or burdens with delayed benefits, the time-to-benefit can be defined as the time between the intervention (when harms are most likely) to the time when improved health outcomes are seen.1 Since studies generally focus on the magnitude of benefit, the time-to-benefit for many preventive interventions is unclear. Survival analyses of screening trials have estimated the time-to-benefit for a few cancer screening interventions. If survivor analyses are not available, the time-to-benefit can be estimated by reviewing Kaplan-Meier survival curves for the intervention and control groups. The Kaplan-Meier curve is the visual representation of survival that shows the probability of an event at a respective time interval. The point at which the curves last clearly separate between the intervention and control groups provides a reasonable estimate of the time-to-benefit for a preventive intervention.1
In addition, the site mentioned above (https://eprognosis.ucsf.edu/index.php) provides a time-to-benefit figure that demonstrates which interventions patients may benefit from and those that may be harmful based on the patient’s life expectancy.6
Review the Benefits of Prevention
If a patient is likely to live long enough to benefit from a preventive intervention, the next step is to consider the potential benefits.1 For example, the primary benefit of cancer screening is the reduction in cancer mortality when early-stage disease is detected and treated, which otherwise would have caused death during the remaining lifetime.
Review the Harms of Prevention
Since many preventive tests might pose harm, the potential benefits of interventions must be weighed against the potential harms.1 Harms are less acceptable when they are caused by screening tests, since screenings may only benefit a few individuals, but all individuals will be exposed to the potential harms (eg, a screening that involves x-rays).1
In addition to physical harm, the psychological distress caused by preventive interventions should be considered.1 This may include the emotional pain of the diagnosis of a disease in a person whose life was not extended by the screening or the alarm and anxiety of a false-positive test. Many older adults may have cognitive, physical, or sensory problems that make screening tests and further work-up difficult, painful, or frightening.1
Integrate the Patient's Values/Preferences Into Decision-Making
The final step is to assess how individuals value the potential harms and benefits and to integrate their preferences into the decision.1 The value placed on different health outcomes will vary. For example, some who undergo screening may value peace of mind after a negative screening result, whereas someone with dementia is not likely to receive such comfort. Clinicians should discuss the benefits and harms with the patient, allow the patient to apply their own values to the outcome, and then jointly decide whether to pursue the intervention.1
There should be a discussion prior to screening about the possible procedures and treatments that may be required after an abnormal screening result.1 Persons who would not want further workup or treatment of an abnormal result should not be screened.1
Applying the Framework
If life expectancy is more than the time-to-benefit, the patient has a substantial chance of benefit and a preventive intervention should be encouraged.1 If life expectancy is less than the time-to-benefit, the preventive intervention should not be offered. If life expectancy approximates the time-to-benefit, a patient’s values and preferences should play the dominant role in the decision whether to perform a preventive intervention or not.1
APPLYING SCREENING PRINCIPLES TO CERTAIN CANCERS
This section will review breast, colorectal, cervical, and prostate cancer screening in the elderly.
Breast Cancer
The probability that a woman will benefit from mammography depends on her risk for developing clinically significant breast cancer in her lifetime; therefore, most screening algorithms start by stratifying women into average- and increased-risk categories.7 However, the process for identifying women at increased risk for developing breast cancer differs for older women since the relative importance of risk factors changes with advancing age and consideration of life expectancy becomes more important. Observational studies favor extending screening mammography to older women who have a life expectancy of more than 10 years. Cost-effectiveness analyses similarly suggest that it is cost-effective to conduct biennial screening mammography up until a life expectancy of 9.5 years.7
Benefits of Mammography in Older Women
The benefit of mammography is finding breast cancer at an early, asymptomatic stage when treatment is expected to be more effective in reducing breast cancer mortality.7 Studies suggest the accuracy of mammography for detecting cancers increases with age. Sensitivity (ie, true positive rate) and specificity (ie, true negative rate) of mammography are highest in women older than 80 years.7
Risks of Mammography in Older Women
While the potential benefit of screening (ie, reducing breast cancer mortality) occurs on average 5 to 10 years after mammography, the potential harms of screening occur immediately.7 Harms include pain, anxiety, and complications from follow-up procedures after a false-positive mammogram or overdiagnosis. Reviews have found that cancer-specific psychological distress may persist for up to 3 years after a false-positive mammogram. In addition, some older women may have cognitive impairment and other comorbidities that make follow-up procedures more painful (eg, arthritis causing discomfort with positioning for procedures), difficult (eg, transportation challenges), or frightening (eg, agitation in women with dementia).7
Due to decreasing life expectancy and an increasing proportion of slower growing cancers, the probability of overdiagnosis increases with age.7 Detection of breast cancer that would not otherwise have clinically surfaced leads to treatments that only cause harm. Studies have suggested approximately 30% of breast cancers detected during the screening period are overdiagnosed. However, this estimate has not been calculated specifically for women 70 years of age or older. The risk of overdiagnosis is higher among screened women with less than a 5- to 10 year life expectancy because of their increased risk of dying from other causes before a screen-detected cancer can progress to symptoms.7
The benefit of screening mammography is also dependent on there being effective treatment for early-stage breast cancer in older women.7 Few clinical trials of breast cancer treatments have included women 75 years of age and older, especially those with multiple comorbidities or frailty. Therefore, the benefits of some treatments remain uncertain in this population.7 The toxicity and mortality from chemotherapy have been noted to increase with age, potentiating the risks of treatment after a positive screening.8
Approximately 20% of women 65 years of age and older experience complications from breast cancer surgery, and the risk increases with age.7 Short-term decreases in cognition may occur among older women following general anesthesia and chemotherapy. Breast radiotherapy can cause fatigue, breast pain, and edema and increase the risk of ischemic heart disease.7
Current Recommendations for Breast Cancer
Table 1 lists the recommendations for breast cancer screening in women.9-11
| Table 1. Screening Recommendations for Breast Cancer9-11 |
|
US Preventive Services Task Force (USPSTF)
|
American Cancer Society (ACS)
|
American College of Obstetricians and Gynecologists (ACOG)
|
|
Biennial screening of all women 50-74 years of age; current evidence is insufficient to assess the balance of benefits and harms of screening mammography in women aged 75 years or older
|
Annual screening for women 45-54 years of age; biennial screening for women >55 years of age with life expectancy >10 years
|
Annual or biennial screening for women 40-75 years of age; screening beyond 75 years of age should be a shared decision based on a woman’s health status/longevity
|
Based on available data, screening for breast cancer is not recommended if a woman has an estimated life expectancy of less than 10 years.1 The ePrognosis Cancer Screening guide available at http://cancerscreening.eprognosis.org/ allows for comparisons of a patient’s life expectancy with the time-to-benefit for screening mammography to help clinicians determine whether mammography is likely to benefit a patient.
Colorectal Cancer
In the US, colorectal cancer is most common in adults aged 65 to 74 years.12 Screening detects polyps, which are precancerous growths on the tissue in the colon and rectum wall. Overall, only 5% of these precancerous polyps will develop into cancer, which typically takes 7 to 10 or more years.13
Several screening tests have been developed to identify colorectal cancer. Table 2 lists the US Preventive Services Task Force (USPSTF) recommended screening tests for colorectal cancer.12
| Table 2. USPSTF Recommended Screening Tests for Colorectal Cancer12 |
|
Test
|
Description
|
|
Stool testa
|
Testing is done at home with a kit that checks for blood in the stool that cannot be seen visually
|
|
Sigmoidoscopy
|
Rectum and sigmoid colonb are examined using a sigmoidoscopec
|
|
Colonoscopy
|
Rectum and entire colon are examined using a colonoscoped
|
|
CT colonography (virtual colonoscopy)
|
Uses a CT scan to produce a series of pictures of the colon and the rectum from outside the body
|
Abbreviations: CT, computed tomography; USPSTF, US Preventive Services Task Force.
a Three (3) types of stool tests are FDA-approved: guaiac fecal occult blood test (gFOBT); the fecal immunochemical test (FIT); and multitargeted stool DNA testing (FIT-DNA).
b Lower one-third of the colon.
c Flexible lighted tube with a lens for viewing and a tool for removing polyps.
d Longer tube versus the sigmoidoscope.
|
Benefits of Colorectal Cancer Screening
Colorectal cancer screening reduces mortality. This is mainly attributable to the reduction of cancer incidence by the removal of polyps and, to a lesser degree, early detection and treatment of cancer.14
Harms of Colorectal Cancer Screening
Bleeding and perforations are the most common adverse events for sigmoidoscopy and colonoscopy.14 Complications may be higher if polypectomy (ie, removal of polyp) is performed or if persons are in poor health.1 Physical discomfort during these tests may occur (eg, muscle spasms, stomach pain), and many older adults may experience substantial distress from the bowel preparation including dizziness, nausea, and fecal incontinence. Approximately 1 in 10 older adults who submit a stool test will have a false-positive result, which leads to anxiety and additional unnecessary testing.1 The precise risk of overdiagnosis with colorectal cancer screening is currently unknown.14
Current Recommendations for Colorectal Cancer
Based on the information presented in the guidelines listed in Table 3, colorectal cancer screening may be most appropriate for persons with a life expectancy greater than 10 years.9,15,16
| Table 3. Screening Recommendations for Colorectal Cancer9,15,16 |
|
Guideline
|
Recommendation
|
Testing/Frequency
|
|
US Preventive Services Task Force
|
Screen all adults 45-75 years of age; individualize decisions in those 76-85 years of age based on health status, prior screening status, and individual preferences.; screening is not recommended for adults >85 years of age
|
-
gFOBT or FIT every year
-
FIT-DNA every 1-3 years
-
CT colonography every 5 years
-
Sigmoidoscopy every 5 years
-
Sigmoidoscopy every 10 years + FIT every year
-
Colonoscopy every 10 years
|
|
American Cancer Society
|
Screen all adults 45-75 years of age if life expectancy >10 years; individualize decisions in adults 76-85 years of age based on preferences, life expectancy, health status, and prior screening history; discourage screening in adults >85 years of age
|
-
FIT or gFOBT every year
-
FIT-DNA every 3 years
-
CT colonography every 5 years
-
Sigmoidoscopy every 5 years
-
Colonoscopy every 10 years
|
|
American College of Physicians
|
Screen all adults 50-75 years of age; persons with life expectancy ≤10 years should not be screened
|
-
FIT or gFOBT every 2 years
-
Colonoscopy every 10 years
-
Sigmoidoscopy every 10 years + FIT every 2 years
|
| Abbreviations: CT, computed tomography; FIT, fecal immunochemical test; FIT-DNA, multitargeted stool DNA testing; gFOBT, guaiac fecal occult blood test. |
Cervical Cancer
Cervical cancer is almost exclusively attributed to infection with human papillomavirus (HPV).17 HPV is acquired through genital skin-to-skin contact with an infected partner, usually but not necessarily, during sexual intercourse. HPV infection can progress to cancer if untreated over a period of several years to decades.17
The HPV test and the Papanicolaou (Pap) test are both screening tools to detect cervical cancer.17 A Pap test can detect mild structural changes in cervical epithelium associated with early HPV infections. HPV tests detect HPV RNA or HPV DNA depending on the type of test used to indicate the presence of HPV. If abnormalities are detected on these tests, women may be referred for a colposcopy, which may include a cervical biopsy.17
Benefits of Cervical Cancer Screening
Routine cervical cancer screening is very effective for preventing cervical cancer and deaths. Since screening with Pap tests was initiated, population studies in the US show a 20% to 60% decline in mortality rates from cervical cancer.1
Harms of Cervical Cancer Screening
False positives are common among older postmenopausal women, leading to unwarranted patient concern and invasive procedures (eg, colposcopy, cervical biopsy).1 In addition, discomfort and anxiety during Pap tests can occur along with the identification and treatment of clinically unimportant cervical lesions given its slow growing nature and the possibility of regression of cervical lesions. There are no data about the time-to-benefit for cervical cancer screening in women 65 years and older.1
Current Recommendations for Cervical Cancer
The main consideration to continue cervical cancer screening is whether an older woman has received regular screening during her reproductive years.1 The likelihood an older woman will die of cervical cancer is remote if she has had normal screens in the past. Decision models suggest that older women who have had repeated normal Pap tests during their reproductive years do not benefit from continued Pap testing beyond age 65.1 Table 4 lists the screening recommendations for cervical cancer. Of note, the American College of Obstetricians and Gynecologists (ACOG) has endorsed the USPSTF Guidelines.18
| Table 4. Screening Recommendations for Cervical Cancer9, 19 |
|
Guideline
|
Recommendation
|
Testing/Frequency
|
|
US Preventive Services Task Force
|
Screening in women 21-65 years of age; discontinue at age 65 if adequate prior screeninga,b
|
-
Every 3 years with Pap test in women aged 21-29 years
-
For women aged 30 65 years, screening every 3 years with Pap test alone, every 5 years with HPV test alone, or every 5 years with HPV/Pap combination
|
|
American Cancer Society
|
Screening in women 25-65 years of age; discontinue at age 65 if regular screening in the past 10 years with normal results
|
-
Primary HPV testc every 5 years
-
If primary HPV testing is not available, screening may be done with either HPV/Pap test combination every 5 years or a Pap test alone every 3 years
|
Abbreviations: HPV, human papillomavirus; Pap, Papanicolaou.
a Three (3) consecutive negative cytology results or 2 consecutive co-occurring negative HPV/Pap test results within 10 years are required before stopping screening, with the most recent test occurring within 5 years.
b Screening may be indicated if there is an inadequate/unknown screening history or in those who are at high risk of developing cervical cancer.
c Primary HPV tests have higher sensitivity to detect precancerous lesions and better reassurance with a negative test resulting in a need for less frequent screening.20
|
Prostate Cancer
The likelihood of having prostate cancer increases as the prostate-specific antigen (PSA) level increases, although there is no set cutoff point for identifying the presence of prostate cancer.21 Many specialists recommend a PSA level of 4 ng/mL or higher when deciding if a patient might need further testing. Men with a PSA level between 4 to 10 ng/mL have about a 1-in-4 chance of having prostate cancer. If the PSA is more than 10, the chance of having prostate cancer is over 50%.21
An elevated PSA level may be caused by prostate cancer but can also be caused by benign prostatic hyperplasia (BPH) and prostatitis, leading to false-positive results.22 A digital rectal examination (DRE) is not recommended as a screening test because of lack evidence of benefits.22
Benefits of Prostate Cancer Screening
The overall benefit of PSA-based screening for prostate cancer is sensitive to the values of individual men.22 The magnitude of net benefit of PSA-based screening depends on how each man weighs the potential benefits and harms of screening, diagnosis, and treatment.22
Risks of Prostate Cancer Screening
Potential harms of screening include frequent false-positive results and psychological distress.22 Harms of a prostate biopsy include pain, hematospermia (ie, blood in semen or ejaculate), and infection. The false-positive and complication rates from biopsy are higher in older men. Additionally, follow-up of large, randomized trials suggests that 20% to 50% of men diagnosed with prostate cancer through screening may be overdiagnosed, resulting in treatment without benefits and consequential adverse effects (eg, erectile dysfunction, urinary incontinence, bowel urgency, fecal incontinence).22
Current Recommendations for Prostate Cancer
Adequate evidence shows that the harms of screening in men 70 years of age and older are at least moderate and greater than in younger men because of increased false-positive results and adverse effects from diagnostic biopsy and treatment.22 Table 5 lists the screening recommendations for prostate cancer.22-24
| Table 5. Screening Recommendation for Prostate Cancer22-24 |
|
Guideline
|
Recommendations
|
Test/Frequency
|
|
US Preventive Services Task Force
|
-
Individualized decision making in men 55-69 years of age
-
Consider family history, race/ethnicity, comorbid medical conditions, patient values, benefits versus risks
-
Do not screen in men ≥70 years of age
|
-
PSA-based screening frequency not provided
|
|
American Cancer Society
|
-
Men ≥50 years of age with a life expectancy >10 years can consider screening after discussion about the risks, benefits, and uncertainties of PSA screening
|
-
Biennial screening if PSA is <2.5 ng/mL
-
Annual screening if PSA is ≥2.5 ng/mL
|
|
American Urological Association
|
-
Shared decision making for men 55-69 years of age based on patient’s values and preferences
-
Do not screen in men ≥70 years of age
-
Do not screen in any man with <10-15 year life expectancy
|
-
PSA screening interval of 2 years or more
|
| Abbreviation: PSA, prostate-specific antigen. |
TREATMENT OF ASYMPTOMATIC CHRONIC CONDITIONS
Treatment of asymptomatic chronic conditions also impose immediate risks and burdens on patients for the promise of delayed benefits.1 Table 6 lists the estimated time-to-benefit for treating hypertension, diabetes, and hyperlipidemia.5
| Table 6. Estimated Time-to-Benefit for Treatment of Asymptomatic Chronic Conditions5 |
|
Disease
|
Time-to-Benefit (years)
|
Intervention
|
|
Diabetes
|
10
|
Intensive glycemic control
|
|
Hypertension
|
1-2
|
Primary prevention
|
|
Hyperlipidemia
|
2-5
|
Primary prevention with statins
|
Treatment for asymptomatic conditions can be viewed as preventive because there are potential risks and a time-to-benefit from drug therapy.1 Therefore, treatment of these asymptomatic conditions should be targeted to older adults whose life expectancy exceeds the time-to-benefit.1 Time-to-benefit from intensive hypertension control (defined as <120/80 mmHg), intensive glycemic control (defined as HbA1C <7%), and using statins for primary prevention with respect to individual patient characteristics can be determined at https://eprognosis.ucsf.edu/index.php.
Intensive Blood Pressure Control
Orthostatic hypotension, falls, fractures, syncope, electrolyte abnormalities, and acute kidney injury have been reported with intensive blood pressure treatment in older adults.1,25 It remains unclear whether intensive blood pressure lowering is well-tolerated and if its effects are uniform across the age spectrum.26 Clinical judgment, patient preference, and an assessment of risk versus benefits is recommended for decisions regarding intensity of blood pressure lowering for older adults.25
Intensive Glycemic Control
The risk of hypoglycemia as a result of intensive glucose control is even greater in older adults who have defective glucose counterregulation, multiple comorbidities, and polypharmacy.27 Hypoglycemia is associated with an increased risk of myocardial infarction, heart failure, stroke, cardiovascular death, falls, fracture, and dementia.27
In frail older adults with medical comorbidities and whose life expectancy is <10 years, it may be advisable to target a HbA1C ≤8%.28 In those with severe comorbidities and/or cognitive and functional disability, glycemic goals may be even higher (eg, HbA1C <8.5%). Treatment should be individualized, with efforts made to preserve quality of life and to avoid hypoglycemia and related complications.28
Statins for Primary Prevention
The risks of overtreating with a statin in the absence of an indication may include myopathy, new-onset diabetes, and hepatoxicity. The USPSTF has provided recommendations for using statins in primary prevention of cardiovascular disease (Table 7).29
| Table 7. USPSTF Recommendations for Statin Use in Primary Prevention29 |
|
Population
|
Recommendation
|
|
Adults aged 40-75 years of age with ≥1 CVD risk factora and an estimated 10-year CVD risk of ≥10%
|
Initiate a statin
|
|
For adults aged 40-75 years with ≥1 CVD risk factora and an estimated 10-year CVD risk of 7.5% to <10%
|
Selectively offer a statin
|
|
For adults 76 years or older
|
Evidence is insufficient to recommend for or against starting a statin
|
Abbreviations: CVD, cardiovascular; USPSTF, US Preventive Services Task Force.
a Dyslipidemia, diabetes, hypertension, and smoking. |
IMMUNIZATIONS
In contrast to screening interventions, the risks associated with immunizations are much lower than the benefits.1 Thus, nearly all older adults should receive the recommended vaccinations. Table 8 lists the adult immunization schedule.30
| Table 8. Adult Immunization Schedule for Those 65 Years of Age and Older30 |
|
Vaccine
|
Recommendation
|
|
COVID-19
|
2- or 3- dose primary series and booster
|
|
Influenza inactivated (IIV4) or influenza recombinant (RIV4)
|
1 dose annually
|
|
Tetanus, diphtheria, pertussis (Tdap or Td)
|
1 dose Tdap, then Td or Tdap booster every 10 years
|
|
Varicella (VAR)
|
2 dosesa
|
|
Zoster recombinant (RZV)
|
2 doses
|
|
Pneumococcal (PCV15, PCV20, PPSV23)
|
1 dose PCV15 (followed by a dose of PPSV23 1 year later) or 1 dose PCV20b
|
|
Hepatitis Ac (HepA)
|
2, 3, or 4 doses depending on vaccine
|
|
Hepatitis Bc (HepB)
|
2, 3, or 4 doses depending on vaccine or condition
|
|
Meningococcal A, C, W, Yc (MenACWY)
|
1 or 2 doses depending on indication
|
|
Meningococcal Bc (MenB)
|
2 or 3 doses depending on vaccine and indication
|
|
Haemophilus influenzae type bc (Hib)
|
1 or 3 doses depending on indication
|
a If no evidence of immunity to varicella.
b For those who have not previously received a dose of PCV13, PCV15, or PCV20, or whose previous vaccination history is unknown.
c Recommended vaccination for adults with an additional risk factor or another indication. |
BEHAVIORS TO MAINTAIN HEALTH
Healthy behaviors have few, if any, adverse outcomes, and should be recommended to nearly all older adults. Proper nutrition, adequate physical activity, and social connection are all important in maintaining a healthy lifestyle in the elderly.31-34
Nutrition
The elderly often face a reduction in appetite and a reduced ability and motivation to purchase and prepare food.31 Lean body mass and total body weight typically decrease, resulting in an increased risk of muscle atrophy, osteoporosis, frailty, falls, fractures, and infection. After the age of 65, the risk of malnutrition increases, leading to an increase in morbidity and mortality and a decrease in quality of life.31
The same nutrition considerations for the general US population apply to older adults.32 However, this age group also has some special nutritional needs. Consuming enough protein is important to prevent the loss of lean muscle mass, and older adults should be encouraged to choose from a wide variety of protein sources (eg, seafood, meats, poultry, eggs, nuts, seeds, beans, peas, lentils). The ability to absorb vitamin B12 can decrease with age. By meeting recommendations for protein foods, a common source of vitamin B12, and including foods fortified with vitamin B12, such as breakfast cereals, individuals can maintain an adequate level. Maintaining adequate fluid intake to prevent dehydration and aid in the digestion of food should be encouraged. In addition to water, choosing unsweetened beverages such as 100% fruit or vegetable juice and low-fat or fat-free milk can support fluid intake to prevent dehydration.32
Some strategies to increased food intake in the elderly include31,32:
-
Sharing meals with friends/family
-
Altering palatability of food with flavor enhancers
-
Identify textures that can alleviate chewing/swallowing difficulty
-
Obtaining adequate calories/protein through liquid supplements
-
Home-delivered meals.31,32
Physical Activity
Physical activity can help prevent or delay the onset of coronary artery disease, type 2 diabetes mellitus, osteoporosis, obesity, and cognitive impairment; protect against the development of functional decline; improve mood; and reduce stress.1 In addition, activities that improve endurance, strength, and flexibility will delay impairments in mobility and may preserve the ability to perform tasks of daily living.1 The Physical Activity Guidelines for Americans recommend at least 150 to 300 minutes per week of moderate-intensity aerobic activity or 75 to 150 minutes per week of vigorous aerobic activity (or an equivalent combination of both), combined with moderate- to high-intensity, muscle-strengthening activity (eg, resistance/weight training) at least 2 days per week for most individuals.33 In addition, older adults are encouraged to do balance training activities as part of their weekly physical activity.33
Social Connection
Social isolation and loneliness have a serious impact on longevity, physical and mental health, and quality of life.34 Hearing, functional, or cognitive impairments can be a barrier to social interaction.1 Clinicians can facilitate social connections by identifying and addressing impairments and asking if individuals would like more social contact, what types of contact they prefer, and connecting individuals to programs to enhance social connections or support.1
CASE EXAMPLE
An 80-year-old female presents with hypertension, hyperlipidemia, diabetes, chronic obstructive lung disease (COPD), and painful osteoarthritis. Her blood pressure is 120/75 mmHg and her latest HbA1C was 7.2%. She is a former smoker and is having difficulty walking several blocks and bathing independently. She rates her overall health as good and has not been hospitalized in the past year. Her physician ranks her in the 50th percentile as compared to others the same age. She is wondering whether she should be screened for colorectal cancer and if she can stop any of her medications.
Medications
Hypertension: lisinopril, chlorthalidone
Hyperlipidemia: simvastatin
Diabetes: glipizide, metformin
Discussion
From Figure 2, her life expectancy can be estimated to be 9.3 years. Colorectal cancer screening is not recommended for those with a life expectancy of ≤10 years.15,16 Therefore, this patient should be advised that colorectal cancer screening is more likely to harm than help and screening should be discouraged. The benefits of more intensive blood pressure control in older patients can be realized in 1 to 2 years. Given the patient’s life expectancy of 9.3 years, continuing more intensive blood pressure control is likely to decrease the mortality risk and should be recommended. In older adults with medical comorbidities and whose life expectancy is <10 years, it is advisable to target a HbA1C ≤8%.28 Based on the patient’s life expectancy and desire to eliminate one of her medications, decreasing or discontinuing glipizide may be a reasonable recommendation. The time-to-benefit for primary prevention of cardiovascular events in patients with hyperlipidemia varies from 2 to 5 years; therefore, the patient can benefit from hyperlipidemia treatment, which should be continued.
CONCLUSION
Preventive interventions may avert some of the complications associated with aging (eg, cancer, chronic diseases). However, prevention can also harm older patients if conditions that are unlikely to cause symptoms in the patient’s lifetime are identified and treated. For this reason, a framework for individualized decision-making for preventive medical interventions can be used to help identify older patients who are most likely to benefit (and most likely to be harmed) by such interventions.
REFERENCES
-
Kotwal AA, Lee SJ. Chapter 11: Prevention and screening. In: Halter JB, Ouslander JG, Studenski S, et al, eds. Hazzard’s Geriatric Medicine and Gerontology, 8e. McGraw Hill; 2022.
-
World Health Organization (WHO). Cancer—Screening and early detection. May 16, 2010. Accessed February 27, 2023. https://www.who.int/europe/news-room/fact-sheets/item/cancer-screening-and-early-detection-of-cancer
-
InformedHealth.org [Internet]. Benefits and risks of screening tests. Institute for Quality and Efficiency in Health Care (IQWiG); 2006-2019. Updated December 17, 2019. Accessed February 27, 2023. https://www.ncbi.nlm.nih.gov/books/NBK279418/
-
Eldridge L. What it means if you have precancerous cells. Verywell Health. Updated May 17, 2022. Accessed February 27, 2023. https://www.verywellhealth.com/what-are-precancerous-cells-2248796
-
Lee SJ, Kim CM. Individualizing prevention for older adults. J Am Geriatr Soc. 2018;66(2):229-234. doi:10.1111/jgs.15216
-
ePrognosis. University of California San Francisco (UCSF). Accessed February 27, 2023. https://eprognosis.ucsf.edu/index.php
-
Walter LC, Schonberg MA. Screening mammography in older women: a review. JAMA. 2014;311(13):1336-1347. doi:10.1001/jama.2014.2834
-
Muss HB, Woolf S, Berry D, Cirrincione C, Weiss RB, et al. Adjuvant chemotherapy in older and younger women with lymph node-positive breast cancer. JAMA. 2005;293(9):1073-1081. doi:10.1001/jama.293.9.1073
-
US Preventive Services Task Force (USPSTF). A & B recommendations. Accessed February 28, 2023. https://uspreventiveservicestaskforce.org/uspstf/recommendation-topics/uspstf-a-and-b-recommendations
-
American Cancer Society (ACS). American Cancer Society recommendations for the early detection of breast cancer. January 14, 2022. Accessed February 28, 2023. https://www.cancer.org/cancer/breast-cancer/screening-tests-and-early-detection/american-cancer-society-recommendations-for-the-early-detection-of-breast-cancer.html
-
American College of Obstetricians and Gynecologists (ACOG).Breast cancer risk assessment and screening in average-risk women. July 2017. Accessed February 28, 2023. https://www.acog.org/clinical/clinical-guidance/practice-bulletin/articles/2017/07/breast-cancer-risk-assessment-and-screening-in-average-risk-women
-
National Cancer Institute (NCI). Screening tests to detect colorectal cancer and polyps. August 2, 2021. Accessed February 28, 2023. https://www.cancer.gov/types/colorectal/screening-fact-sheet
-
Harvard Health Publishing. They found colon polyps: now what? February 2, 2022. Accessed February 28, 2023. https://www.health.harvard.edu/diseases-and-conditions/they-found-colon-polyps-now-what
-
Helsingen LM, Kalager M. Colorectal cancer screening—approach, evidence, and future directions. NEJM Evid. 2022;1(1). January 10, 2022. Accessed February 28, 2023. https://evidence.nejm.org/doi/pdf/10.1056/EVIDra2100035
-
ACS. American Cancer Society guideline for colorectal cancer screening. November 17, 2020. Accessed March 1, 2023. https://www.cancer.org/cancer/colon-rectal-cancer/detection-diagnosis-staging/acs-recommendations.html
-
Qaseem A, Crandall CJ, Mustafa RA, Hicks LA, Wilt TJ, et al. Screening for colorectal cancer in asymptomatic average-risk adults: a guidance statement from the American College of Physicians. Ann Intern Med. 2019;171(9):643-654. doi:10.7326/M19-0642
-
Berman T, Smith JA. Chapter 33: Cervical cancer. In: O’Connell MB, Smith JA, eds. Women's Health Across the Lifespan, 2e. McGraw Hill; 2019.
-
ACOG. Updated cervical cancer screening guidelines. April 2021. Accessed March 1, 2023. https://www.acog.org/clinical/clinical-guidance/practice-advisory/articles/2021/04/updated-cervical-cancer-screening-guidelines
-
ACS. The American Cancer Society guidelines for the prevention and early detection of cervical cancer. April 22, 2021. Accessed March 1, 2023. https://www.cancer.org/cancer/cervical-cancer/detection-diagnosis-staging/cervical-cancer-screening-guidelines.html
-
Bhatla N, Singhal S. Primary HPV screening for cervical cancer. Best Pract Res Clin Obstet Gynaecol. 2020;65:98-108. doi:10.1016/j.bpobgyn.2020.02.008
-
ACS. Screening tests for prostate cancer. January 4, 2021. Accessed March 2, 2023. https://www.cancer.org/cancer/prostate-cancer/detection-diagnosis-staging/tests.html
-
USPSTF. Prostate cancer: screening. May 8, 2018. Accessed March 2, 2023. https://www.uspreventiveservicestaskforce.org/uspstf/document/RecommendationStatementFinal/prostate-cancer-screening
-
ACS. American Cancer Society recommendations for prostate cancer early detection. February 24, 2023. Accessed March 2, 2023. https://www.cancer.org/cancer/prostate-cancer/detection-diagnosis-staging/acs-recommendations.html
-
American Urological Association (AUA). Early detection of prostate cancer (2018). Accessed March 2, 2023. https://www.auanet.org/guidelines-and-quality/guidelines/prostate-cancer-early-detection-guideline
-
Chen T, Shao F, Chen K, Wang Y, Wu Z, et al. Time to clinical benefit of intensive blood pressure lowering in patients 60 years and older with hypertension: a secondary analysis of randomized clinical trials. JAMA Intern Med. 2022;182(6):660-667. doi:10.1001/jamainternmed.2022.1657
-
Camafort M, Redón J, Pyun WB, Coca A. Intensive blood pressure lowering: a practical review. Clin Hypertens. 2020;26(1):21. doi: 10.1186/s40885-020-00153-z
-
Arnold SV, Lipska KJ, Wang J, Seman L, Mehta SN, et al. Use of intensive glycemic management in older adults with diabetes mellitus. J Am Geriatr Soc. 2018;66(6):1190-1194. doi: 10.1111/jgs.15335
-
Munhi M. Treatment of type 2 diabetes mellitus in the older patient. UpToDate. Updated February 1, 2023. Accessed March 3, 2023. https://www.uptodate.com/contents/treatment-of-type-2-diabetes-mellitus-in-the-older-patient
-
USPSTF. Statin use for the primary prevention of cardiovascular disease in adults: preventive medication. August 23, 2022. Accessed March 3, 2023. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/statin-use-in-adults-preventive-medication
-
Centers for Disease Control and Prevention (CDC). Recommended adult immunization schedule for ages 19 years or older, United States, 2023. February 17, 2023. Accessed March 3, 2023. https://www.cdc.gov/vaccines/schedules/downloads/adult/adult-combined-schedule.pdf
-
Clegg ME, Williams EA. Optimizing nutrition in older people. Maturitas. 2018;112:34-38. doi:10.1016/j.maturitas.2018.04.001
-
US Department of Agriculture. Dietary Guidelines for Americans 2020-2025. 9th ed. December 2020. Accessed March 3, 2023.
https://www.dietaryguidelines.gov/sites/default/files/2021-03/Dietary_Guidelines_for_Americans-2020-2025.pdf
-
US Department of Health and Human Services (HHS). Executive Summary:Physical Activity Guidelines for Americans, 2nd edition. HHS; 2019. Accessed March 3, 2023. https://health.gov/sites/default/files/2019-10/PAG_ExecutiveSummary.pdf
-
WHO. Reducing social isolation and loneliness among older people. Accessed March 3, 2023. https://www.who.int/activities/reducing-social-isolation-and-loneliness-among-older-people