ADVERTISEMENT

This Module Contains:
- Prevalence and Impact of Nonadherence
- Assessing Adherence in MTM
- Adherence Tools
- Addressing Specific Adherence Issues
- Counseling and Motivational Interviewing Techniques
- Health Literacy Issues
|
OVERVIEW: ASSESSING ADHERENCE IN MTM
Assessing patient adherence to therapy and promoting better adherence are among the chief goals of any MTM consultation. Even an ideal drug regimen becomes useless, and costly, if the patient does not use the medication. Managing adherence has become more challenging in today's healthcare environment. The variety and complexity of therapeutic options continues to expand for many medical conditions, and a greater number of patients are prescribed multiple medications. For the pharmacist conducting MTM, addressing adherence is a broad issue that must balance the goals of effective disease management, safety and tolerability, and patient lifestyle factors. The multiple factors involved in adherence were diagrammed in a World Health Organization (WHO) report (Figure 1).1
| Figure 1. Five Dimensions of Adherence1 |
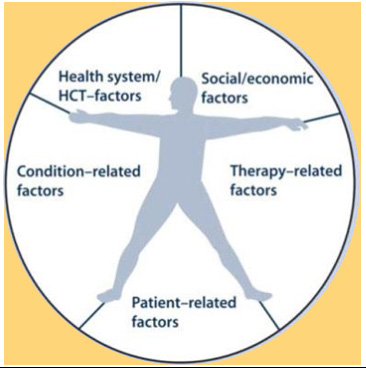 |
HCT=health care team
Reprinted with permission from: World Health Organization.
Adherence to Long-Term Therapies: Evidence for Action. |
During MTM, the goal is not for pharmacists to simply remind patients to take their medications. MTM may involve adjusting a medication regimen to fit better with that person's lifestyle, determining whether any necessary safety monitoring is needed, and helping the patient understand and adjust to the effects of a drug therapy. The term "adherence" is preferred over "compliance," because it connotes patient cooperation and buy-in for the overall therapeutic regimen, rather than obedience to the healthcare provider.2
PREVALENCE OF NONADHERENCE
Americans are a "medication-taking society." Almost half of all Americans used at least one prescription drug in the past 30 days; 24% used three or more, and 13% used five or more.3 In developed countries, adherence to therapy for any chronic disease has been estimated at approximately 50%, but many factors affect this commonly-cited figure.4 Studies comparing patient self-reports to findings from electronic dose monitoring systems show that about 80% of patients over-report their adherence.5, 6 Three quarters of patients do not take medications as directed, and less than 30% never fill their prescriptions (Figure 2).7
| Figure 2. Gap Between Written Prescription and Medication Use |
 |
IMPACT OF NONADHERENCE ON CARE OUTCOMES
Failure to use medications as directed has been described as the "single greatest detractor to efficacy" for many people with chronic illness. Undetected, nonadherence often leads to:
- Unnecessary switching and/or escalation of therapy
- Increased visits to physicians and hospitals, hospital admissions
- Increased costs of therapy, drug waste
Nonadherence accounts for 30% to 50% of all treatment failures.8 When a patient has an inadequate response to a medical therapy, many practitioners either adjust the dose of the agent if possible, or switch patients to a different drug in an effort to gain better control of the disease. A WHO report points out, "Increasing the effectiveness of adherence interventions may have a far greater impact on the health of the population than any improvement in specific medical treatments."1
PREDICTORS OF ADHERENCE TO MEDICATIONS
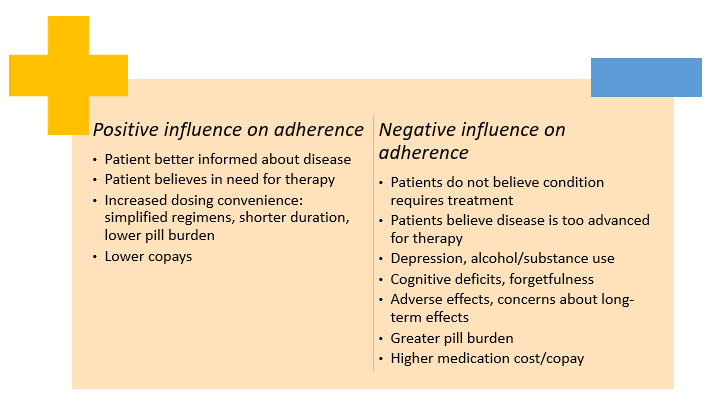
Dozens of studies have been conducted to analyze why people are nonadherent to medical therapies and to detect what factors can improve medicine-taking behaviors. The specific reasons may differ by disease type and other variables, but there are certain common issues that can be considered.9-11(Figure 3)
| Figure 3. Factors Positively and negatively Influencing Adherence9-11 |
 |
ASSESSING ADHERENCE TO MEDICATIONS IN MTM
True adherence to therapy is difficult to measure because it relies on a person's honest and accurate recounting of medication doses taken. As part of the comprehensive medication review in MTM, pharmacists can try to gain a more realistic sense of adherence, by applying some of the following strategies:
- Avoid closed-ended questions, like: "Do you take this every day?" This calls for a one-word answer. Instead, ask, "Tell me how you are taking this."
- Do not make assumptions; avoid judgment
- Use the "show-me" technique for complex dosage forms
- Use multiple sources of objective evidence, including fill history, evaluation of bottles brought to appointment
It's difficult for many people to admit they do not take their medications. Given the time, effort, and money that goes into providing this treatment, some may feel they have an obligation to say they are adhering to therapy. At the same time, the reality of busy lifestyles, drug side effects, difficulties with administering the medication, and failure to understand dosage instructions present a compelling conflict. It may be easier for the person to say, "Yes, I'm using the drugs," than "No, but I can't really explain why."
Developing a personal relationship and rapport with the patient during MTM has been shown to increase adherence.12-14 Expressing a sense of empathy is often effective. When the pharmacist acknowledges that nonadherence is a very common problem, this admission can be a great relief to a person who has been hiding the problem, allowing the pharmacist to move on to possible solutions.
Tools for Measuring Adherence
Patient-reported adherence
Patient-reported adherence is often the most practical method that can be used by MTM pharmacists to assess adherence. This method is easy, fast, and inexpensive. There are various ways the pharmacist can ask patients to recall their medication-taking history. Among the validated methods are either a 3-day or 7-day recall, or use of a visual analog scale or Modified Morisky Scale (Table 1).15, 16
| Table 1. Pharmacist Tools to Measure Self-Reported Adherence17,18 |
| Visual Analog Scale |
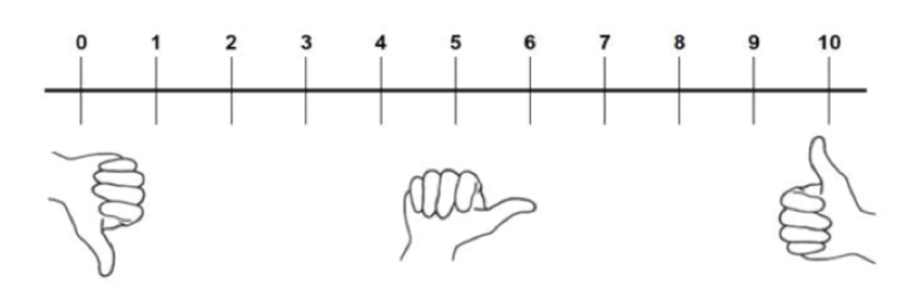 |
How much of your medication have you taken in [time period]?
0 = None; 5 = About half; 10 = Every dose |
| Morisky Scale (Yes = 0, No = 1) |
1. Do you ever forget to take your medicine?
2. Are you careless at times about taking your medicine?
3. When you feel better, do you sometimes stop taking your medicine?
4. Sometimes if you feel worse when you take the medicine, do you stop taking it? |
0 = lowest level of adherence; 4 = highest level of adherence
Patients scoring 0 or 1 would benefit most from pharmacist intervention |
Measuring patient adherence is now a part of quality measures used to rate healthcare delivery and sometimes to determine payment levels, as in pay-for-performance (P4P) models. A P4P model offers bonus payments to providers (including pharmacists in some areas) when Pharmacy Quality Alliance (PQA) measures are met in the treatment of patients receiving Medicare Part D benefits. Categories in the current updated PQA measures include:17
- Medication safety (young children, older adults)
- Appropriate medication use (diabetes, statins, opioids
- Adherence measures (medication fills for certain drug classes such as diabetes, cardiac conditions, anticoagulation, COPD)
Proportion of Days Covered (PDC) requires access to claims data, and is the preferred adherence measurement method for PQA. PDC can be used to calculate adherence to chronic therapies in populations, but it is not useful for measuring adherence to acute therapies.18 Another method using claims data is Medication Possession Ratio (MPR). These calculations are summarized in Table 2.19
| Table 2. Calculating PDC and MPR Adherence Measures19 |
| Proportion of Days Covered (PDC) |
Medication Possession Ratio (MPR) |
|
# of days in time period
"covered" by medication
÷
# of days in period
(Value of 1 = 100% adherence)
|
# of days drug was supplied
within refill period
÷
# of days in refill period
(Value of 1 = 100% adherence)
|
|
· Examines each day in period to determine if the patient has the drug on hand
· Provides more conservative estimate of adherence compared with MPR when patients are switching drugs or using dual-therapy in a class
· More complex to calculate than MPR
|
· May overestimate adherence, because the ratio would be artificially high for patients who refill medications early or overlap on refills. "Medication possession" data reveal whether patients have refilled medications, but not whether they actually took the medications.
|
Addressing Specific Adherence Issues in MTM
Once the conversation has been started, the pharmacist should attempt to identify any potential barriers that affect that individual. Addressing adherence problems during MTM is challenging and highly patient-specific. Some common barriers and proposed pharmacist interventions are outlined in Table 3.
| Table 3. Common Barriers to Adherence and Proposed Interventions |
| Barriers |
Pharmacist interventions |
| Forgetfulness |
Distinguish between forgetfulness vs. motivation. Address situations where forgetfulness is most likely. Tailor reminders to patient's lifestyle/preferences. |
| Fear of long-term effects |
Explore concerns and understanding of medication effects Discuss risk-benefit analysis of therapy |
| Occurrence of adverse effects |
Manage when possible; suggest change in therapy if needed |
| Unclear about instructions |
Evaluate health literacy, utilize teach-back method.
Address questions; refer questions to prescriber when necessary |
| Perceived lack of efficacy |
Explore understanding of condition and treatment; Explain to patient why the medication is being taken; discuss expectations, impact on symptoms, how the drug works. |
| Cost |
Recommend lower cost alternatives, generic programs, patient or co- pay assistance programs |
Forgetfulness
Forgetfulness is a major cause of nonadherence. This affects people with impaired memory, but also those with unpredictable schedules, such as parents of young children.
Perceived lack of efficacy ("I really don't need this drug" or "It's not working for me")
Perceived lack of efficacy is one of the most commonly cited reasons for missing doses and discontinuing therapy.9 People may not "feel" the effects of the disease they are treating (a classic example is hypertension), and may not necessarily notice the effects of treatment. Unrealistic expectations are highly predictive of premature discontinuation.23
Difficult medication regimen (e.g., injectable administration)
Adherence rates drop when a medication regimen is more complex and increase when the regimen is simplified.20 Difficult regimens may include injectable or inhaled therapies. Fear of self-injection is a significant reason for nonadherence for many patients. Even a patch can be a complex regimen for some patients, if it involves site rotation or needing to remove the patch at a certain time. Does the relative ease of taking a pill overcome adherence problems? Not necessarily. Adherence to oral therapies is low among people with chronic conditions and tends to decrease with time. Even when an oral drug has the potential to noticeably reduce symptoms or would yield nearly 99% efficacy (such as with oral contraceptives), adherence tends to be low.20
Early discontinuation from therapy
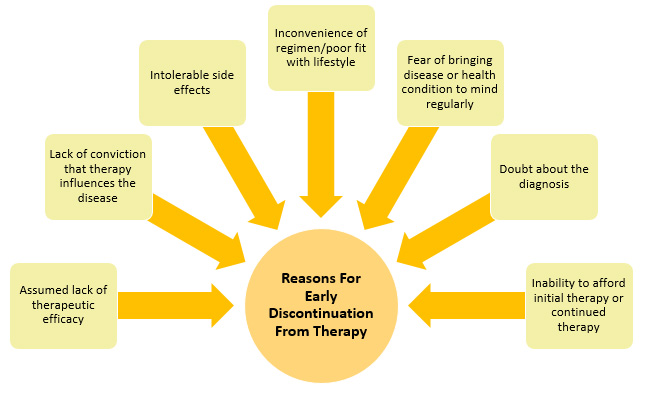
Prescription "abandonment" occurs often. This is a particular problem during care transitions such as discharge from a hospital and for drugs with high copays.20 People who discontinue treatment tend to do so within the first 12 months of therapy.21 Adverse effects are a major reason given by both patients and physicians for why people stop therapy (Figure 4).
| Figure 4. Reasons for Early Discontinuation from Therapy |
 |
Patient Case: Adherence to a Daily Oral Medication
A 42-year-old mother of 3 young children has had variable adherence to daily oral levothyroxine (T4) therapy. Soon after an endocrinologist visit, her adherence level is high, but it tends to drop after a few months. Based on her chart, the pharmacist notes that she has been significantly hypothyroid at times, with detrimental effects on her life and health. The patient agrees that the therapy is important, but just can't seem to make it part of her routine.
Instead of simply telling the patient that it is important to take the medication daily (which her physician has done), the pharmacist needs to determine her specific barriers to adherence.
Pharmacist: "Tell me about some of the issues that you think prevent you from using this medicine regularly."
Patient responds she is supposed to take her medicine first thing in the morning on an empty stomach, then wait 30 minutes. She sometimes doesn't remember it until breakfast time, so she skips that dose in order to eat breakfast. This occurs 1 or 2 times per week. Asked about her morning routine, she adds that she brews a pot of coffee first thing in morning "so I can function."
Pharmacist: "What I am hearing you saying, is that you are concerned about how eating and drinking might affect the way the drug works."
The pharmacist discusses data on thyroid medications and timing of food absorption. One solution is to take the pill at night, but the patient reports that evenings are "even crazier than mornings." Since it usually takes her about 30 minutes to get her youngest children dressed, another plan is suggested:
Pharmacist: Can you keep a glass of water by your bedside, and take the thyroid pill right when you wake up? Then, promise yourself will not start brewing the coffee unless the pill has been taken."
The patient agrees that this plan fits well with her lifestyle. She will try this approach and have her thyroid levels rechecked after 3 months. Because she sometimes has misplaced the lab forms. The pharmacist may be able to facilitate the use of electronic lab orders.
The pharmacist has offered solutions that are easy to implement and fit well with the patient's lifestyle, short-term do-able goals for the patient, and a longer-term goal and follow-up plan.
Because the patient has young children, the pharmacist asks the patient about medication storage, and suggests a convenient cupboard lock sold at the pharmacy to ensure safe storage of her medication.
|
MOTIVATIONAL TIPS TO ACHIEVE CHANGE IN ADHERENCE BEHAVIORS
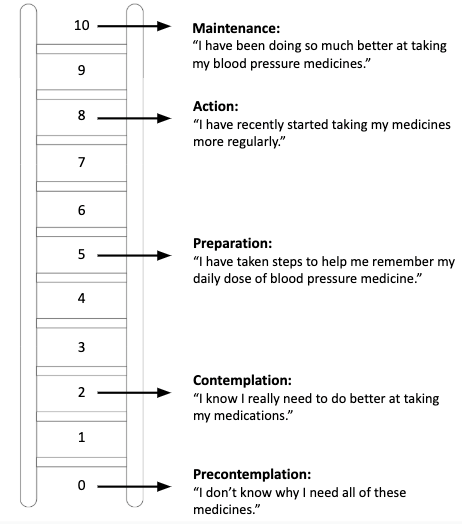
Pharmacists are regarded as the health professionals with a high degree of knowledge and expertise in addressing adherence issues. However, it is unrealistic to expect that one MTM encounter is going to change a person's long-term behavior patterns. The MTM pharmacist can utilize a "Contemplation Ladder" to determine the patient's degree of motivation for improving adherence (Figure 5).22
| Figure 5. Contemplation Ladder for Changing Adherence Behavior22 |
 |
An MTM pharmacist can take proactive steps to counsel patients on adherence (Table 4).
| Table 4. Tips for Counseling Patients About Adherence |
| Step |
What to Consider |
|
1. Learn the patient's belief set
|
· Does the patient understand significance of his/her condition?
· Is the person motivated to take any medication for the condition?
· Does patient believe pros of taking medication outweigh the cons?
· Has patient lost motivation to treat the disease (e.g., he/she is feeling good, he/she doesn't believe the medication is helping)?
|
|
2. Inquire about goals
|
· Is there anything the disease is preventing that the patient would like to do again?
|
|
3. Become familiar with family history, priorities, and cultural beliefs
|
· Is the person motivated to remain healthy for a child or other family member?
· Does the person have a family member whose condition worsened because of failure to take a medication?
|
|
4. Give the patient a sense of collaboration into decision-making process
|
· Work together to select a medication that the person will have a genuine "interest" in taking
· Maintain independence for a longer time
· Reduce the risk of having frequent relapses
|
|
5. Learn the patient's attitudes about taking medications in general
|
· Past negative experiences
· Patterns of taking medications in the past; schedules that work best
|
|
6. Understand the patient's reimbursement status
|
· High copayments
· Fixed income
· Qualified for special programs (low-income subsidy if Part D)
|
IMPACT OF LOW LITERACY AND HEALTH LITERACY ON MEDICATION ADHERENCE
Many people who have low literacy are skillful at hiding this fact from healthcare providers. According to the National Assessment of Adult Literacy (NAAL), about 14% of Americans have a literacy level "below basic prose," meaning that they can understand only simple, straightforward content from a short piece of text.23 Generally speaking, this would rule out most medication information or instructions. The NAAL further reports that approximately 22% have below basic quantitative literacy (understanding only simple numeric concepts; unlikely to understand numbers embedded in printed materials).23
There are many excellent tools available to pharmacists to assess written literacy and health literacy. Some of the best-validated screening tools include the REALM-SF (Rapid Estimate of Adult Literacy in Medicine–Short Form) and the SILS (Single-item Literacy Screener).24 Organizations such as NAAL and the Agency for Healthcare Research and Quality (AHRQ) provide guidelines and tools for evaluating literacy and health literacy in the pharmacy. It is essential to avoid belittling patients or making them feel ashamed about poor reading skills. A set of health pictograms is available for free download from the U.S. Pharmacopeial Convention.25 Use of these pictograms has been shown to improve medication adherence.
Health literacy is different concept than prose or quantitative (number) literacy. Even a highly educated and literate person may have very low health literacy. Many drug names sound the same, and similar drug names are frequently confused. Many consumers have limited ability to distinguish between the brand names and generic names of the agents they are using. Evaluating and addressing a patient's health literacy are important in the process of MTM. The AHRQ's Health Literacy Toolkit includes a number of useful resources toward this goal, including:30
- Pharmacy Health Literacy Assessment Tool and User's Guide
- Training Program for Pharmacy Staff on Communication
- Guide on How to Create a Pill Card
- Telephone Reminder Tool to Help Refill Medicines on Time
SUMMARY AND CONCLUSIONS
A basic tenet of adherence is that a person's perceived need for a medication must outweigh the downsides, such as inconvenience, cost, and possible adverse effects.26 This is truer now than ever before, with a greater variety of therapies available and a greater need to balance the risks and benefits of drug therapies. Pharmacists must be aware of the importance of adherence in making therapeutic decisions, considering safety risks, and evaluating the potential efficacy of an agent.
REFERENCES
- World Health Organization (WHO). Adherence to Long-term Therapies: Evidence for Action. Geneva, Switzerland: WHO, 2003.
- Bell JS, Airaksinen MS, Lyles A, Chen TF, Aslani P. Concordance is not synonymous with compliance or adherence. Br J Clin Pharmacol. Nov 2007;64(5):710-711; author reply 711-713.
- Centers for Disease Control and Prevention (CDC). Therapeutic Drug Use. Updated October 20, 2021. Available at: https://www.cdc.gov/nchs/fastats/drug-use-therapeutic.htm.
- Mathes T, Pieper D, Antoine SL, Eikermann M. 50% adherence of patients suffering chronic conditions--where is the evidence? Ger Med Sci. 2012;10:Doc16.
- Zeller A, Ramseier E, Teagtmeyer A, Battegay E. Patients' self-reported adherence to cardiovascular medication using electronic monitors as comparators. Hypertens Res. Nov 2008;31(11):2037-2043.
- Chan A, De Simoni A, Wileman V, et al. Digital interventions to improve adherence to maintenance medication in asthma. Cochrane Database Syst Rev. Jun 13 2022;6(6):Cd013030.
- National Consumers League. Script Your Future. 2019. Available at: https://www.scriptyourfuture.org/about/.
- Kleinsinger F. The Unmet Challenge of Medication Nonadherence. Perm J. 2018;22:18-033.
- Curkendall SM, Thomas N, Bell KF, Juneau PL, Weiss AJ. Predictors of medication adherence in patients with type 2 diabetes mellitus. Curr Med Res Opin. Oct 2013;29(10):1275-1286.
- Al-Qerem W, Jarab AS, Badinjki M, Hyassat D, Qarqaz R. Exploring variables associated with medication non-adherence in patients with type 2 diabetes mellitus. PLoS One. 2021;16(8):e0256666.
- Nieuwlaat R, Wilczynski N, Navarro T, et al. Interventions for enhancing medication adherence. Cochrane Database Syst Rev. Nov 20 2014;2014(11):Cd000011.
- Snyder ME, Zillich AJ, Primack BA, et al. Exploring successful community pharmacist-physician collaborative working relationships using mixed methods. Res Social Adm Pharm. Dec 2010;6(4):307-323.
- Wellman BR, Frail CK, Zillich AJ, Snyder ME. Pharmacists' experiences with a telephonic medication therapy management program for home health care patients. Consult Pharm. Mar 2015;30(3):163-174.
- Keshishian F, Colodny N, Boone RT. Physician-patient and pharmacist-patient communication: geriatrics' perceptions and opinions. Patient Educ Couns. May 2008;71(2):265-284.
- Sayner R, Carpenter DM, Blalock SJ, et al. Accuracy of Patient-reported Adherence to Glaucoma Medications on a Visual Analog Scale Compared With Electronic Monitors. Clin Ther. Sep 1 2015;37(9):1975-1985.
- Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. Jan 1986;24(1):67-74.
- Pharmacy Quality Alliance. PQA Adherence Measures. August 28, 2018. Available at: https://www.pqaalliance.org/adherence-measures.
- Loucks J, Zuckerman AD, Berni A, Saulles A, Thomas G, Alonzo A. Proportion of days covered as a measure of medication adherence. Am J Health Syst Pharm. Mar 7 2022;79(6):492-496.
- Lam WY, Fresco P. Medication Adherence Measures: An Overview. Biomed Res Int. 2015;2015:217047.
- Halpern V, Lopez LM, Grimes DA, Stockton LL, Gallo MF. Strategies to improve adherence and acceptability of hormonal methods of contraception. Cochrane Database Syst Rev. Oct 26 2013;(10):Cd004317.
- Stout RL, Braciszewski JM, Subbaraman MS, Kranzler HR, O'Malley SS, Falk D. What happens when people discontinue taking medications? Lessons from COMBINE. Addiction. Dec 2014;109(12):2044-2052.
- DiClemente CC, Corno CM, Graydon MM, Wiprovnick AE, Knoblach DJ. Motivational interviewing, enhancement, and brief interventions over the last decade: A review of reviews of efficacy and effectiveness. Psychol Addict Behav. Dec 2017;31(8):862-887.
- National Assessment of Adult Literacy (NAAL). A nationally representative and continuing assessment of English language literacy skills of American adults. U.S. Department of Education. Available at: http://nces.ed.gov/naal/kf_demographics.asp.
- Agency for Healthcare Research and Quality. Health Literacy Measurement Tools. Updated November 2019. Available at: http://www.ahrq.gov/professionals/quality-patient-safety/quality-resources/tools/literacy/index.html. .
- U.S. Pharmacopeial Convention. USP Pictogram Library. Available at: http://www.usp.org/usp-healthcare-professionals/related-topics-resources/usp-pictograms. .
- McQuaid EL, Landier W. Cultural Issues in Medication Adherence: Disparities and Directions. J Gen Intern Med. Feb 2018;33(2):200-206.