ADVERTISEMENT

What Makes a Drug Special? Defining Specialty Medications
INTRODUCTION
Specialty medications account for less than 2% of all the prescription medications, yet make up more than 50% of all drug spending.1 There is no universal consensus on what makes a drug a specialty medication, though specialty drugs often share similar characteristics.
Before discussing the common characteristics of specialty medications, it is important to understand the two main reasons why the “specialty” designation matters. First, health plans who provide insurance to cover the cost of medications or pharmacy benefit managers (PBMs) who administer pharmacy benefits will often treat specialty medications differently than traditional, non-specialty drugs. While non-specialty medications are often grouped by whether they are a brand or a generic on a health plan’s formulary (i.e., their list of covered medications), specialty medications are often categorized on their own tier.2 This tier is often associated with a substantial cost-share responsibility (i.e., the amount the patient is responsible for paying out of their own pocket). In 2021, 49% of employer plans had specialty tiers, and patients owed an average of either a $101 copayment or 27% coinsurance.2
Beyond the coverage implications, there are also distribution implications for specialty medications that will be discussed in more detail later.
Characteristics of specialty drugs
The definition of a specialty drug is not universal. Instead, depending who you ask – the health plan or PBM, the manufacturer, or the pharmacy – a single drug may be considered specialty by some entities within the healthcare system, but not by others. Further, some health plans and PBMs may designate a medication to be a specialty drug, while other health plans and PBMs do not. Therefore, the section below will describe the most common characteristics of specialty medications (Table 1), but should not be considered an all-inclusive list nor a guide that must be followed strictly when determining specialty medication status.
| Table 1. Characteristics of Specialty Medications |
|
• Manufactured through a biotechnology process
• Special handling requirements
• Customized dosing
• Complex delivery methods
• Complex and/or rare disease target
• Clinical support essential to effective outcome
• Reimbursement complexities
• High cost |
A specialty medication does not need to meet all of these criteria in order to be considered specialty; one criterion may be enough if that characteristic is unique enough. Still, other medications may meet several of these criteria and not be considered specialty medications.
Examples will be used to illustrate the criteria described below; however, these examples are select medications and do not represent every situation that may be encountered in practice.
Manufactured through a biotechnology process
The first common characteristic of specialty medications is that they are often manufactured through a biotechnology process. Normal, everyday drugs (known as “small drug compounds”) are manufactured through a stable, predictable chemical or organic manufacturing process.3 On the other hand, biologic medications are large, complex molecules that are made from living cells and organisms.4 To put it into perspective, aspirin has a molecular weight of 180 Daltons, while a monoclonal antibody may weigh 150,000 Daltons.3 In addition, biologic medications are more unstable (i.e., they require more sensitive storage and handling conditions) and have a greater likelihood of being immunogenic (i.e., they may produce an immune response, which is undesirable in many circumstances).3
All biologic medications are considered specialty medications, but not all specialty medications are biologics. That means that small drug compounds, not produced through a biotechnology process, may also be considered specialty medications if they have other characteristics of specialty drugs.
Special Handling Requirements
Most medications are stored at room temperature without the need for much consideration for how they are handled. Some medications stored at room temperature must be administered in a more particular manner (e.g., nitroglycerin sublingual tablets must be administered in their original glass container to prevent exposure to light and moisture). Others still will require storage in a refrigerator (e.g., insulins until they are in-use) or freezer [e.g., certain vaccines, such as the live varicella (chickenpox) vaccine].5
Notably, the requirement to dispense a medication in the original packaging or store a medication in the refrigerator or freezer alone would not be enough to have that medication be considered a specialty drug. However, those storage requirements in combination with other special characteristics may lead to a specialty designation.
When the storage and handling requirements of a medication are specialized enough, however, a drug may be considered a specialty medication based on this characteristic alone. For example, Imlygic (talimogene laherparepvec), which is used for melanoma, must be stored in an ultra-low temperature freezer between -130°F to -94°F (-90°C to -70°C).5,6 Because of this specialized requirement and the lack of availability of ultra-low temperature freezers at some institutions, the manufacturer can ship this medication in its own ultra-low temperature freezer.
Another example is Kymriah (tisagenlecleucel), which is used for several types of cancer including acute lymphoblastic leukemia, diffuse large B-cell lymphoma, and follicular lymphoma. This agent must be stored in the vapor phase of liquid nitrogen at or below -184°F (-120°C) and is only stable at room temperature for up to 30 minutes after thawing.5
If either of these medications had no other characteristics of specialty drugs, these traits alone would be enough to deem these agents to be specialty medications.
Customized dosing
Drugs may also be deemed to be specialty if they are dosed in an unusual way. Specialty medications may require a simple dosing (e.g., one tablet by mouth once daily). Their dosing may even be more complex, but still not entirely unusual (e.g., dosing based on body weight or body surface area). This does not preclude them from being considered specialty drugs; however, specialty medications may be considered specialty solely based on requiring a customized dosing if the dosing instructions are unusual enough. A few examples may help illustrate this point.
Certain medications may be dosed based on blood levels of the therapeutic target. As an example, hemophilia is treated by replacing clotting factor XIII for hemophilia A or factor IX for hemophilia B. Factor XIII or IX in these patients is used to treat hemophilia patients acutely (i.e., during an active bleed) or prophylactically (i.e., to prevent bleeding events). To determine the appropriate prophylactic dose of factor products for these patients, the equations in Table 2 may be used.7 Note that one of the components in the calculation is the patient’s desired factor level. This means that the provider needs to know the patient’s current level to determine how much to replace (i.e., a 40% increase from the current level).
| Table 2. Hemophilia Factor Replacement Equations7 |
|
Hemophilia A factor replacement equation
Patient weight ÷ 4.4 × factor level desired = number of factor VIII units needed
Hemophilia B factor replacement equation
Patient weight ÷ 2.2 × factor level desired = number of factor IX units needed
|
Some medications may also require customized dosing based on genetic factors. Chronic Hepatitis C virus (HCV) is one of the leading causes of liver disease, liver failure, and liver cancer in the United States.8 Within the past decade, new treatment options have emerged that allow clinicians to cure HCV infections in a high percentage of patients. However, determining the appropriate medication for these patients is complex and is based on genetic factors, namely the virus’ genotype. There are 6 genotypes and numerous subtypes that have been identified.9 Not only are certain medications chosen to combat certain genotypes, but also the length of time the medication is used is often determined by the particular genotype of the patient’s virus.10
A final example of medications requiring customized dosing are those that have maximum lifetime doses. Some drugs, like doxorubicin, an anticancer medication, have a ceiling dose. If the patient receives more than that total lifetime dose, they are put at risk for adverse events. For doxorubicin, higher cumulative doses lead to an increased risk of cardiomyopathy, a disease affecting the heart muscle.11
These requirements for customized dosing would lead hemophilia factor products, HCV medications, and doxorubicin to be considered specialty medications even if no other characteristics of specialty drugs were present.
Complex delivery methods
Medications may also be deemed as specialty drugs based on how they are administered. Specialty drugs may have common delivery methods (e.g., by mouth, topically, or as a subcutaneous injection). They also may be much more complex and require significant expertise in order to properly administer. A few examples will help illustrate this point.
First, consider Spinraza (nusinersen), which is indicated for the treatment of spinal muscular atrophy (SMA), a disease that destroys nerve cells in the brain and spine.12 This medication must be administered as an intrathecal injection – directly into the spinal canal.
Next, think about drugs like Eylea (aflibercept). This medication belongs to a class of medications called vascular endothelin growth factor inhibitors, which are all used for a variety of ocular conditions like diabetic macular edema, age-related macular degeneration, and diabetic retinopathy.13 These agents must be injected directly into the intravitreal space – the jelly-like fluid in the back of the eye.
There are also medications, like Brineura (cerliponase alfa), that require intraventricular infusion. This medication is used for a rare condition called late infantile neuronal ceroid lipofuscinosis type 2 (CLN2), a brain condition.14 To ensure the medication is delivered directly to the target area, the medication is infused directly into the ventricles of the brain through a small hole in the skull.
Needless to say, these routes of administration, while effective in delivering medication to the desired site within the body, require significant expertise to ensure the best patient outcomes. For this reason, even without any other specialty characteristics, these medications and others like them would all be considered specialty drugs due to their complex administration requirements alone.
Complex and/or rare disease target
Drugs that treat rare diseases often require no other characteristics to be considered specialty medications, because expertise is required to appropriately manage patients with these conditions. But how rare is “rare?” The U.S. Food and Drug Administration (FDA) defines a rare disease as one that affects less than 200,000 persons in the U.S.15 These are also known as orphan diseases, and the drugs used to treat these conditions are referred to as orphan drugs. Over 7,000 rare diseases have been identified and affect approximately 30 million people in the U.S.15 Some examples of orphan diseases previously discussed include CLN and SMA, which both affect 1 to 9 per 100,000 live births.16,17
Interestingly, only about 5% of the 7,000 known rare diseases have effective treatments available.18 The FDA offers several programs to incentivize pharmaceutical manufacturers to research and develop treatments for these conditions, most notably granting medications for rare conditions that meet certain criteria an orphan designation.15 Orphan designation:15
- Provides tax credits for clinical research studies conducted in humans.
- Waives the Prescription Drug User Fee, valued at approximately $3 million.
- Grants a potential of up to 7 years of market exclusivity. This limits generic competition from entering the market for up to 2 years longer than new chemical entities that are approved for non-rare diseases.
Medications may be deemed as specialty drugs if they treat diseases that are more prevalent than orphan diseases, but are still uncommon. An example would be rheumatoid arthritis, which affects about 1.5 million individuals in the U.S.19 While it is an uncommon disorder, impacting less than 1% of the population, it cannot be considered an orphan disease as it does not meet the prevalence cutoff.
While specialty medications are often considered to only treat rare diseases, they are also becoming increasingly available for severe or more specialized forms of common disorders. However, unless a medication has other characteristics of a specialty drug, treating a common disease target on its own will not lead to that medication being considered a specialty drug. As an example, patients with gout, a very common disease, who do not respond to conventional treatment may be prescribed Krystexxa (pegloticase). This medication is not considered a specialty drug because of the disease it is treating, but because of other characteristics – it is administered as an intravenous infusion, and as will be discussed shortly, is very expensive and requires clinical support to ensure an effective outcome.20
Another example would be high cholesterol medications, Praluent (alirocumab) and Repatha (evolocumab). These two medications are approved to reduce the risk of future cardiovascular events, including heart attack and stroke, in patients who have established atherosclerotic cardiovascular disease (ASCVD).21,22 The American Heart Association and American College of Cardiology define established ASCVD as anyone with a prior history of acute coronary syndromes (sudden reduced blood flow to the heart), myocardial infarction (heart attack), stroke, transient ischemic attack (ministroke), stable or unstable angina (chest pain), a prior arterial revascularization (a procedure to redirect or improve blood flow to the heart), or peripheral arterial disease (reduced blood flow to the limbs).23 Considering the broad definition and the fact that a heart attack occurs every 40 seconds in the U.S., this indication is not rare or uncommon.24 Still these medications have other characteristics of specialty drugs that lead to their designation as such.
Clinical Support Essential to an Effective Outcome
Given the importance of proper and timely distribution of specialty medications and the complex nature of these drugs and/or the diseases they are targeting, specialty pharmacies came into existence to ensure patients achieve the best outcomes. Specialty pharmacies focus on the proper dispensing of specialty medications and provide care beyond what a typical community pharmacy provides (Table 3).
| Table 3. Services Commonly Offered by Specialty Pharmacies25 |
- 24-hour access to pharmacists
- Benefits investigation and assistance with submitting and resolving prior authorization requirements
- Communication and follow-up with the physician
- Shipping coordination to ensure timely, accurate delivery to reduce waste
- Identifying and securing financial assistance (e.g., enrolling patients in patient assistance programs, identifying and applying copay coupons)
- Detailed, routine patient adherence and medication counseling and monitoring
- Payer and/or manufacturer reporting
- Proactive patient outreach for prescription refill and renewal
|
Any pharmacy that dispenses specialty medications may be colloquially called a “specialty pharmacy.” However, pharmacies that focus their dispensing on specialty medications are legitimized by certification from Accreditation Commission for Health Care (ACHC), URAC, or another accrediting body. In 2020, there were approximately 1,200 accredited specialty pharmacy locations, up dramatically from 2015 when there were less than 400.26 The majority of these were independently-owned (42%) and health care provider-owned (39%), which includes specialty pharmacies owned by hospitals, health systems, physician practices, and provider group purchasing organizations.26 Only 9% are owned by health plans and PBMs.26 Some of the largest specialty pharmacies include CVS Specialty, Accredo, Optum Specialty Pharmacy, AllianceRx Walgreens Prime, and Humana Specialty Pharmacy.27
While the dispensing of specialty drugs from specialty pharmacies may be considered a more high-touch, but similar dispensing model compared to that used for traditional medications (e.g. dispensing from an outpatient retail or community pharmacy or insurer- or PBM-owned mail order pharmacy), this is simply the tip of the iceberg.
Most specialty pharmacies dispense prescriptions through the mail, with very few brick and mortar specialty stores. Specialty pharmacies that are owned by large retail chains, on the other hand, may dispense medication from the specialty pharmacy to the retail entity to be picked up by the patient. This alleviates a number of challenges associated with shipping the medication directly to the patient, such as ensuring the patient is home to receive the shipment. It may create inconvenience for the patient though by relying upon them to travel to the pharmacy to obtain the medication.
As previously mentioned, specialty drugs often have distribution implications that must be considered. Not every specialty drug is available from every specialty pharmacy and not all specialty drugs require distribution from a specialty pharmacy. Sometimes specialty medications are available only from a small number of specialty pharmacies (as few as one). The availability of these so-called “limited distribution drugs” is determined by the pharmaceutical manufacturer who produces the medication.28 Health plans or PBMs may also restrict which pharmacies can fill a prescription for a given specialty medication by creating a preferred specialty pharmacy network.29 Understanding the proper location to send a prescription for a specialty medication is a challenge often encountered by health care providers as it is often unclear as to which pharmacies the manufacturer, health plan, or PBM requires the patient to use.
Bagging versus Buy-and-Bill
Four different dispensing models are used for specialty medications that are required to be administered by a health care professional (“office-administered agents”). Brown-bagging is the practice of dispensing the medication from a specialty pharmacy directly to the patient. The patient then takes the medication to their provider for administration.30 The biggest issue with brown-bagging is the risk of improper storage and handling. If a medication requires specialized handling, the medication may be ruined if it is accidentally left in the patient’s car or on the patient’s porch in the heat of summer. Specialty pharmacies help navigate this by providing patient education and coordinating shipping times to ensure the patient is home to receive the shipment. Still, these issues may occur.
White-bagging circumvents the issue of storage and handling by having the specialty pharmacy dispense the medication directly to the patient’s provider (e.g., outpatient clinic, a physician’s office).30 The medication, intended for the specific patient, is handled only by health care professionals and is administered upon the patient’s arrival to a scheduled appointment.
One step further is clear-bagging (also known as gold-bagging). Clear-bagging involves a practice-owned specialty pharmacy (e.g., a specialty pharmacy owned by a health system) dispensing the medication directly to the site-of-administration, which is also owned by the practice (e.g., an outpatient infusion center owned by the same health system).30 This is similar to white-bagging, with the exception that only one entity is responsible for the dispensing and administration process.
A final option is what is called “buy-and-bill.” In this circumstance, the provider that will be administering the medication purchases and stores the medication until it is to be administered to the patient.30 There are several differences between the buy-and-bill and “bagging” models. First, with bagging, the medication is dispensed from a pharmacy for a particular patient. With buy-and-bill, the provider owns a stock of the medication that can be used for whomever is prescribed the drug. Multi-use vials can be used for different patients. Second, with bagging, providers do not seek reimbursement for the medication, only for the costs associated with the administration (e.g., professional fees, supplies, management of adverse reactions). With buy-and-bill, the provider owns the medication that they purchased (“buy”) and submits a claim to the patient’s insurance for reimbursement after administering the medication (“bill”).30
Reimbursement Complexities
Another characteristic of specialty drugs is that reimbursement may be more complex than traditional, non-specialty medications. With a traditional medication dispensed from a community pharmacy:
- The pharmacy submits a claim through the patient’s PBM;
- The PBM checks the claim against the patient’s insurance coverage;
- The PBM notifies the pharmacy of how much the pharmacy will be reimbursed and how much the patient owes (the patient’s cost-sharing responsibility);
- The pharmacy collects what the patient owes and dispenses the medication to the patient for self-administration.
This process may remain unchanged for some specialty drugs, but others may have a more complex reimbursement process. A few select examples are provided below.
There are two types of insurance – pharmacy insurance, which typically covers medications that are dispensed by a pharmacy; and medical insurance, which typically covers medical expenses, such as hospital stays, provider services, laboratory and diagnostic testing, and much more. When a traditional, non-specialty medication is dispensed, it is dispensed under the patient’s pharmacy insurance. Provider-administered medications that are dispensed through a buy-and-bill model are typically covered under the patient’s medical insurance. However, bagging may lead to confusion as the medication is dispensed by a pharmacy but administered by a health care provider. Providers may inadvertently bill the patient’s medical insurance for this medication after the pharmacy who shipped the drug billed the patient’s pharmacy insurance. This situation, known as double billing can lead to the same medication being paid for twice unless caught by the health insurance company.
A specialty drug is not universally covered under the medical or the pharmacy benefit. Certain health plans may cover a medication under the pharmacy benefit (i.e., preferring bagging), while others may cover it under the medical benefit (i.e., preferring buying-and-billing).31 This can be confusing for patients but especially for prescribers, as it is not inherently clear whether they should be sending prescriptions to a pharmacy or dispensing it from their own stock.
When a health plan determines that a medication is going to be covered under a particular benefit, this will not often impact whether any given patient will be able to receive coverage for that drug. However, challenging situations periodically arise when a patient has coverage from one health insurance company or PBM for their pharmacy insurance and a second health insurance company for their medical insurance. In these situations, if the two companies do not agree under which benefit a drug should be covered, it may leave the patient without coverage. The following illustrates this example:
- A patient is looking to fill an injectable fertility medication.
- The patient’s pharmacy insurance company deems the medication to be a medical benefit drug.
- The patient’s medical insurance company deems the medication to be a pharmacy benefit drug.
- The patient would theoretically be left without coverage by either company.
Fortunately, in these situations, payers will often work together to find a way to cover the medication for the patient.
Specialty drugs, as will be discussed in more detail below, are expensive. As such, the patient’s cost-sharing responsibility may be significantly higher for these medications – up to thousands of dollars. Since this is unaffordable to most patients, specialty pharmacies often assist with procuring copay assistance (e.g., copay coupons) to reduce the patient’s cost-sharing responsibility. In response, health insurance companies and PBMs have developed “copay maximizer” and “copay accumulator” programs that alter patients’ insurance coverage based on these medications.32 These programs may affect patient cost-sharing in convoluted ways, making it harder for patients to understand what is owed on any given prescription.
These are just a few of the challenging situations that complicate the reimbursement of specialty medications compared to traditional, non-specialty drugs.
High Cost
The final, and most important, characteristic of a drug that leads to its classification as a specialty medication is its cost. Regardless if a drug has no other characteristics previously described, if it is high cost, health plans and PBMs will consider it to be a specialty medication.
How high is “high?” While there’s no specific cost for most patients, for patients insured under Medicare, the Centers for Medicare and Medicaid Services require health plans and PBMs to consider any drug that costs more than $830 per month as a specialty drug, which is approximately $10,000 per year.33 However, specialty drugs can cost significantly more than this.
On average, specialty medications cost approximately $79,000 per year.34 They make up over half of all drug spending, which, when considering that a characteristic of specialty drugs is that they typically treat rare or uncommon conditions, is quite an astonishing statistic.1 In 2021, it was estimated that of the top 10 drugs by projected total revenue, 8 were considered specialty medications.35 Specialty medications may also be significantly more expensive than the $79,000 per year average (Table 4).
| Table 4. Top 5 Most Expensive Medications in the U.S.36 |
| Rank |
Generic Name |
Brand Name |
Use |
Annual Cost of Therapy |
| 1 |
Onasemnogene abeparvovec |
Zolgensma |
Spinal muscular atrophy |
$2,125,000 |
| 2 |
Lonafarnib |
Zokinvy |
Hutchinson-Gilford progeria syndrome |
$1,073,760 |
| 3 |
Naxitamab-gqgk |
Danyelza |
Neuroblastoma |
$1,011,882 |
| 4 |
Tebentafusp-tebn |
Kimmtrak |
Uveal Melanoma |
$975,520 |
| 5 |
Metreleptin |
Myalept |
Lipodystrophy |
$929,951 |
Where We Are and Where We Go from Here
Over the past several years, the FDA has continued to approve a significant number of drugs that are classified as new chemical entities (drugs in which the main chemical has never been approved by the FDA in the past). Of these agents, most of them have been for orphan diseases or can be classified as specialty medications based on the other characteristics previously discussed (Figure 1).
| Figure 1. New Chemical Entity Approvals 2015-202137-43 |
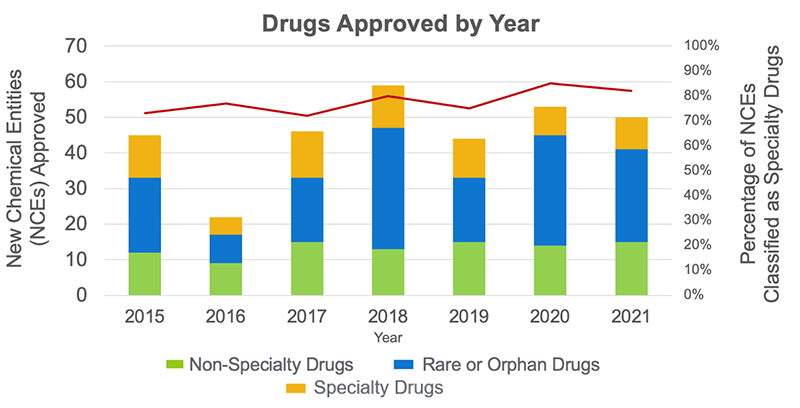 |
Out of the 269 total medications approved from 2015 through 2020, 208 are either rare or orphan drugs or other specialty drugs. That’s 77% of all the new chemical entities approved in the past 6 years. This has been consistent from one year to the next, with between 72% and 85% of approved new chemical entities being able to be classified as specialty agents.
With more than 7 out of every 10 drugs approved over the past 6 years being specialty medications, health care providers and patients have an unprecedented new opportunity to deliver and receive care that was previously not possible. If, however, the most common characteristic of specialty drugs is high cost, this has the potential to create an affordability issue for patients and payers. Fortunately, biosimilars promise some relief for exorbitant drug spending.
A biosimilar, as the name implies, is not a copy of the original biologic product (also known as the “originator” or “reference” product), but instead is a compound deemed to be “highly similar” to the originator product.3,4 Biosimilars are often thought of “generic biologic drugs” though they are not simply copies of the reference product as traditional generic medications are.
The fact that small drug compounds (normal, everyday drugs) are manufactured through a straightforward manufacturing process makes them very easy to copy, which allows for generic manufacturers to develop identical compounds that are expected to produce equivalent therapeutic outcomes. Conversely, the size and complexity of biologic medications and their manufacturing processes makes them very difficult to copy. A small change in the biologic’s manufacturing process may lead to structural differences in the compound, which can impact the drug’s safety and efficacy.3
In order to gain approval by the FDA, pharmaceutical manufacturers of biosimilar medications must prove that there are no clinically meaningful differences in safety, purity, and potency (how well the drug works) from an existing FDA-approved reference product.44 In order to gain approval by the FDA, manufacturers of generic medications only need to show bioequivalence to the original product; that is, that the generic medication becomes available to the site of action in the body in a similar manner when administered at the same dose compared to the original product.45 In addition to bioequivalence, manufacturers of biosimilars must conduct clinical studies to demonstrate that the biological product has no major pharmacokinetic (how the drug moves within the body) or pharmacodynamic (how the drug works within the body) differences compared to the originator product. Animal studies to assess safety must also be conducted.46
As of August 2022, there have been 37 biosimilars approved by the FDA for use in the U.S. (Tables 5 through 7). The entry of biosimilars to the market promises billions of dollars of savings on health care spending and will help in curbing the spend on specialty drugs.47
| Table 5. Biosimilars Approved in the U.S. for Cancer-Related Indications48 |
| Trade name (biosimilar name) |
Date of FDA-Approval |
Originator Trade Name (generic) |
| Fylnetra (pegfilgrastim-pbbk) |
May 2022 |
Neulasta (pegfilgrastim) |
| Alymsys (bevacizumab-maly) |
April 2022 |
Avastin (bevacizumab) |
| Releuko (filgrastim-ayow) |
February 2022 |
Neupogen (filgrastim) |
| Riabni (rituximab-arrx) |
December 2020 |
Rituxan (rituximab) |
| Nyvepria (pegfilgrastim-apgf) |
June 2020 |
Neulasta (pegfilgrastim) |
| Ziextenzo (pegfilgrastim-bmez) |
November 2019 |
Neulasta (pegfilgrastim) |
| Ruxience (rituximab-pvvr) |
July 2019 |
Rituxan (rituximab) |
| Zirabev (bevacizumab-bvzr) |
June 2019 |
Avastin (bevacizumab) |
| Kanjinti (trastuzumab-anns) |
June 2019 |
Herceptin (trastuzumab) |
| Trazimera (trastuzumab-qyyp) |
March 2019 |
Herceptin (trastuzumab) |
| Ontruzant (trastuzumab-dttb) |
January 2019 |
Herceptin (trastuzumab) |
| Herzuma (trastuzumab-pkrb) |
December 2018 |
Herceptin (trastuzumab) |
| Truxima (rituximab-abbs) |
November 2018 |
Rituxan (rituximab) |
| Udenyca (pegfilgrastim-cbqv) |
November 2018 |
Neulasta (pegfilgrastim) |
| Nivestym (filgrastim-aafi) |
July 2018 |
Neupogen (filgrastim) |
| Fulphila (pegfilgrastim-jmdb) |
June 2018 |
Neulasta (pegfilgrastim) |
| Retacrit (epoetin alfa-epbx) |
May 2018 |
Epogen (epoetin-alfa) |
| Ogivri (trastuzumab-dkst) |
December 2017 |
Herceptin (trastuzumab) |
| Mvasi (Bevacizumab-awwb) |
September 2017 |
Avastin (bevacizumab) |
| Zarxio (Filgrastim-sndz) |
March 2015 |
Neupogen (filgrastim) |
| Table 6. Biosimilars Approved in the U.S. for Inflammatory Conditions48,49 |
| Trade name (biosimilar name) |
Date of FDA-Approval* |
Originator Trade Name (generic) |
| Amjevita (Adalimumab -atto) |
September 2016 |
Humira (adalimumab) |
| Cyltezo (Adalimumab-adbm) |
August 2017 |
Humira (adalimumab) |
| Yusimry (adalimumab-aqvh) |
December 2021 |
Humira (adalimumab) |
| Hulio (adalimumab-fkjp) |
July 2020 |
Humira (adalimumab) |
| Abrilada (adalimumab-afzb) |
November 2019 |
Humira (adalimumab) |
| Hadlima (adalimumab-bwwd) |
July 2019 |
Humira (adalimumab) |
| Eticovo (etanercept-ykro) |
April 2019 |
Enbrel (etanercept) |
| Hyrimoz (adalimumab-adaz) |
October 2018 |
Humira (adalimumab) |
| Ixifi (infliximab-qbtx) |
December 2017 |
Remicade (infliximab) |
| Renflexis (Infliximab-abda) |
May 2017 |
Remicade (infliximab) |
| Avsola (infliximab-axxq) |
December 2019 |
Remicade (infliximab) |
| Erelzi (Etanercept-szzs) |
August 2016 |
Enbrel (etanercept) |
| Inflectra (Infliximab-dyyb) |
April 2016 |
Remicade (infliximab) |
| *Inflammatory conditions include diseases like rheumatoid arthritis, juvenile idiopathic arthritis, plaque psoriasis, psoriatic arthritis, Crohn’s disease, ulcerative colitis, and ankylosing spondylitis. Not all of these products are indicated for all of these conditions. |
| Table 7. Other Biosimilars Approved in the U.S. for Indications Other than Cancer or Inflammatory Conditions48,49 |
| Trade name (biosimilar name) |
Date of FDA-Approval |
Originator Trade Name (generic) |
Indication |
| Rezvoglar (insulin glargine-aglr) |
December 2021 |
Lantus (insulin glargine) |
Type 1 and Type 2 Diabetes Mellitus |
| Semglee (Insulin glargine-yfgn) |
July 2021 |
Lantus (Insulin glargine) |
Type 1 and Type 2 Diabetes Mellitus |
| Byooviz (ranibizumab-nuna) |
September 2021 |
Lucentis (ranibizumab) |
Ocular disorders* |
| Cimerli (ranibizumab-eqrn) |
August 2022 |
Lucentis (ranibizumab) |
Ocular disorders* |
| *Both ranibizumab biosimilars are indicated for various ocular disorders including neovascular (wet) age-related macular degeneration, macular edema following retinal vein occlusion, and myopic choroidal neovascularization. Ranibizumab-eqrn is also FDA-approved for diabetic macular edema and diabetic retinopathy. |
Conclusion
The characteristics of specialty drugs are defined by each individual organization, but have shared characteristics across the industry. A medication being designated as a specialty drug has important implications on distribution and reimbursement. Still, the inconsistency between organizations in designating drugs as specialty medications may lead to patient and provider confusion. Pharmacy technicians can play a role in helping patients understand what specialty medications are and by connecting patients prescribed specialty drugs to sources of additional information (e.g., health insurance companies’ or PBMs’ customer service lines or manufacturer patient information resources).
REFERENCES
- Evernorth By the numbers. Accessed on August 2, 2022. Available at: https://www.evernorth.com/drug-trend-report/utilization-and-costs
- Kaiser Family Foundation. 2021 employer health benefits survey. Section 9: Prescription drug benefits. Accessed on August 2, 2022. Available at: https://www.kff.org/report-section/ehbs-2021-section-9-prescription-drug-benefits/
- Li E, Ramanan S, Green L. Pharmacist substitution of biological products: Issues and considerations. J Manag Care Spec Pharm. 2015;21(7):532-539.
- Kusti M. Overview and manufacturing of biologics. Am J Manag Care. 2020. Available at: https://www.ajmc.com/view/overview-and-manufacturing-of-biologics
- Drug Facts and Comparisons. 2022. Wolters Kluwer Health, Inc. Accessed August 2, 2022.
- Imlygic has special operations and handling requirements. Accessed on August 2, 2022. Available at: https://www.imlygichcp.com/operations-and-handling
- The Hemophilia, von Willebrand Disease & Platelet Disorders Handbook. Calculating the dose. Accessed on August 2, 2022. Available at: https://www.hog.org/handbook/article/3/29/calculating-the-dose
- Khullar V, Firpi RJ. Hepatitis C cirrhosis: New perspectives for diagnosis and treatment. World J Hepatol. 2015;7(14):1843-55.
- Dhawan VK. Hepatitis C. Accessed on August 2, 2022. Medscape. Available at: https://www.medscape.com/answers/177792-3826/what-are-the-most-common-hepatitis-c-virus-hcv-genotypes
- AASLD-IDSA. Recommendations for testing, managing, and treating hepatitis C. Accessed on August 2, 2022. Available at: http://www.hcvguidelines.org
Doxorubicin hydrochloride [package insert]. Memphis, TN: Northstar Rx LLC; July 2022. Available at: https://dailymed.nlm.nih.gov/dailymed/fda/fdaDrugXsl.cfm?setid=ddf55319-bf62-4ec7-8be2-ef97188837c4&type=display
- Spinraza [package insert]. Cambridge, MA: Biogen; June 2020. Available at: https://www.spinraza.com/content/dam/commercial/spinraza/caregiver/en_us/pdf/spinraza-prescribing-information.pdf
- Eylea [package insert]. Tarrytown, NY: Regeneron Pharmaceuticals, Inc.; June 2021. Available at: https://www.regeneron.com/downloads/eylea_fpi.pdf
- Brineura [package insert]. Novato, CA: BioMarin Pharmaceutical Inc.; March 2020. Available at: https://www.brineura.com/wp-content/themes/jupiter-child/assets/pdfs/resources/Brineura-Prescribing-Information.pdf
- S. Food & Drug Administration. Rare diseases at FDA. Accessed August 2, 2022. Available at: https://www.fda.gov/patients/rare-diseases-fda
- Neuronal ceroid lipofuscinosis. Accessed August 2, 2022. Available at: https://www.orpha.net/consor/cgi-bin/OC_Exp.php?lng=EN&Expert=216
- Proximal spinal muscular atrophy. Accessed August 2, 2022. Available at: https://www.orpha.net/consor/cgi-bin/Disease_Search.php?lng=EN&data_id=633
- Kaufmann P, Pariser AR, Austin C. From scientific discovery to treatments for rare diseases - the view from the National Center for Advancing Translational Sciences - Office of Rare Diseases Research. Orphanet J Rare Dis. 2018;13(1):196.
- Arthritis Foundation. Arthritis by the numbers. 2019. Accessed August 8, 2022. Available at: https://www.arthritis.org/getmedia/e1256607-fa87-4593-aa8a-8db4f291072a/2019-abtn-final-march-2019.p
- Krystexxa [package insert]. Deerfield, IL: Horizon Therapeutics USA, Inc.; July 2022. Available at: https://www.hzndocs.com/KRYSTEXXA-Prescribing-Information.pdf
- Praluent [package insert]. Tarrytown, NY: Regeneron Pharmaceuticals, Inc.; April 2021. Available at: https://www.regeneron.com/downloads/praluent_pi.pdf
- Repatha [package insert]. Thousand Oaks, California: Amgen Inc.; September 2021. Available at: https://www.pi.amgen.com/-/media/Project/Amgen/Repository/pi-amgen-com/Repatha/repatha_pi_hcp_english.pdf
- Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;140(11):e596-e646.
- Yu B, Akushevich I, Yashkin AP, Kravchenko J. Epidemiology of geographic disparities of myocardial infarction among older adults in the United States: Analysis of 2000-2017 Medicare data. Front Cardiovasc Med. 2021;8:707102.
- Hagerman J, Freed S, Rice G. Specialty pharmacy: A unique and growing industry. Pharmacy Today. 2013: 19(7); 39.
- Fein AJ. The specialty pharmacy accreditation boom slows: DCI’s exclusive update on the U.S. market. Drug Channels Institute. 2021. Accessed August 5, 2022. Available at: https://www.drugchannels.net/2021/05/the-specialty-pharmacy-accreditation.html
- Fein AJ. DCI’s top 15 specialty pharmacies of 2021–and three factors that will reshape 2022. Drug Channels Institute. 2022. Accessed August 5, 2022. Available at: https://www.drugchannels.net/2022/05/dcis-top-15-specialty-pharmacies-of.html
- Karas L, Shermock KM, Proctor C, Socal M, Anderson GF. Limited distribution networks stifle competition in the generic and biosimilar drug industries. Am J Manag Care. 2018: 24(4).
- The management of specialty drugs. Accessed August 5, 2022. Available at: https://www.spcma.org/wp-content/uploads/2016/06/sPCMA_The_Management_of_Specialty_Drugs.pdf
- Fein AJ. White bagging update: PBMs’ specialty pharmacies keep gaining on buy-and-bill oncology channels. Drug Channels Institute. 2021. Accessed August 5, 2022. Available at: https://www.drugchannels.net/2021/10/white-bagging-update-pbms-specialty.html
- EMD Serono. Specialty Digest – 13th 2017.
- Fein AJ. Four reasons why PBMs gain as maximizers overtake copay accumulators. Drug Channels Institute. 2022. Accessed August 5, 2022. Available at: https://www.drugchannels.net/2022/02/four-reasons-why-pbms-gain-as.html
- Centers for Medicare & Medicare Services. Contract year (CY) 2023 final Part D bidding instructions. 2022. Accessed August 5, 2022. Available at: https://www.cms.gov/files/document/2023partdbiddinginstructions.pdf
- Bunis D. Specialty drug prices soar to nearly $79,000 a Year. AARP. 2019. Accessed August 5, 2022. Available at: https://www.aarp.org/politics-society/advocacy/info-2019/specialty-drug-prices-rise.html
- Expected best selling pharmaceutical products (drugs) in 2021. 2021. Accessed August 5, 2022. Available at: https://www.ipharmacenter.com/post/expected-best-selling-pharmaceutical-products-drugs-in-2021
- McQueen H. The 10 most expensive drugs in the U.S., period. GoodRx. 2022. Accessed August 5, 2022. Available at: https://www.goodrx.com/healthcare-access/drug-cost-and-savings/most-expensive-drugs-period
- Center for Drug Evaluation and Research. Advancing health through innovation: New drug therapy approvals 2021. U.S. Food & Drug Administration. 2022. Accessed August 5, 2022. Available at: https://www.fda.gov/media/155227/download
- Center for Drug Evaluation and Research. Advancing health through innovation: New drug therapy approvals 2020. U.S. Food & Drug Administration. 2021. Accessed August 5, 2022. Available at: https://www.fda.gov/media/144982/download
- Center for Drug Evaluation and Research. Advancing health through innovation: New drug therapy approvals 2019. U.S. Food & Drug Administration. 2020. Accessed August 5, 2022. Available at: https://www.fda.gov/media/134493/download
- Center for Drug Evaluation and Research. Advancing health through innovation: New drug therapy approvals 2018. U.S. Food & Drug Administration. 2019. Accessed August 5, 2022. Available at: https://www.fda.gov/media/120357/download
- Center for Drug Evaluation and Research. Advancing health through innovation: New drug therapy approvals 2017. U.S. Food & Drug Administration. 2018. Accessed August 5, 2022. Available at: https://www.fda.gov/media/110526/download
- S. Food & Drug Administration. 2016 Novel Drugs Summary. 2017. Accessed August 5, 2022. Available at: https://www.fda.gov/media/102618/download
- S. Food & Drug Administration. 2015 Novel Drugs Summary. 2016. Accessed August 5, 2022. Available at: https://www.fda.gov/media/95661/download
- S. Food & Drug Administration. Biosimilar development, review, and approval. 2017. Accessed August 5, 2022. Available at: https://www.fda.gov/drugs/biosimilars/biosimilar-development-review-and-approval
- Chow SC. Bioavailability and bioequivalence in drug development. Wiley Interdiscip Rev Comput Stat. 2014;6(4):304-312.
- Christl L. FDA’s overview of the regulatory guidance for the development and approval of biosimilar products in the US. U.S. Food & Drug Administration. Accessed August 5, 2022. Available at: https://www.fda.gov/files/drugs/published/FDA’s-Overview-of-the-Regulatory-Guidance-for-the-Development-and-Approval-of-Biosimilar-Products-in-the-US.pdf
- Mulcahy A, Buttorff C, Finegold K, et al. Projected US savings from biosimilars, 2021-2025. Am J Manag Care. 2022;28(7):329-335.
- S. Food & Drug Administration. Biosimilar product information. 2022. Accessed August 5, 2022. Available at: https://www.fda.gov/drugs/biosimilars/biosimilar-product-information
- AJMC Center for Biosimilars. FDA approves Coherus’ Cimerli as interchangeable biosimilar to ranibizumab. 2022. Accessed August 5, 2022. Available at: https://www.centerforbiosimilars.com/view/fda-approves-coherus-cimerli-as-interchangeable-biosimilar-to-ranibizumab
Back to Top