ADVERTISEMENT

This Module Contains:
- Patient criteria for Medicare Part D patients and non-Medicare MTM candidates
- Who qualifies for Part D-funded MTM services?
- List of core chronic conditions
- How to contact eligible patients
- Targeting patients for MTM services beyond Medicare Part D
- Definition of a high-risk, complex regimen
- Role of caregivers in MTM
|
What’s New in this Update?
- CMS updated its Targeted Beneficiary definition to include “At-risk beneficiaries.” This module explains what this means for MTM providers.
- As of January 2022 CMS requires MTM providers that offer services under Medicare Part D to provide a website with information for patients.
- The Enhanced MTM model program has concluded; reports indicated that enhanced MTM did not produce cost savings compared with regular MTM.
- New Feature: Video on pharmacist reimbursement for MTM services
- services.
|
INTRODUCTION
If you are providing MTM services to patients enrolled in Medicare Part D, those patients must meet specific selection criteria in order to have MTM services reimbursed by Medicare. However, many pharmacists also provide MTM to other groups of patients, outside of Medicare Part D, who can benefit from these services. This chapter analyzes both of those groups, to help pharmacists target the most appropriate patients for MTM services.
How patients are targeted for MTM depends much on the arrangements for reimbursement. When a pharmacist provides MTM under Medicare Part D, the services must follow particular protocols and may be constrained by limited reimbursement. Some pharmacy organizations also provide MTM services for employers that are looking to reduce healthcare costs and absentee rates among their workforces. Research on these programs has shown that for every $1 spent on MTM, the employer can save between $6 and $12 on healthcare costs.1-3 The Patient-Centered Medical Home (PCMH) is another example of a care structure with an emphasis on MTM.4 In PCMH and workplace settings, the criteria for patient selection is usually much broader than that defined by Medicare Part D. Patient criteria for MTM are outlined in Table 1.
| Table 1. Patient Criteria and MTM Structure, Medicare Part D versus Non-Medicare |
| |
Medicare Part D Patients |
Non-Medicare Part D Patients |
| Age |
Over 65 generally Medicare eligible |
Any Age |
| Referral Path |
Referred through Medicare Part D sponsor to:
• Pharmacy benefit managers (PBMs)
• Contracted MTM provider (e.g., Outcomes MTM)
• Contracted community provider Long-term care residents are included. CMS generally views long-term care residents as community dwellers (not inpatients). They are eligible for MTM in addition to the CMS-mandated monthly consultant pharmacist review. |
• Eligible state Medicaid programs
• Direct marketing
• Employer contracts
• PBMs for non-Med D insured
• Contracts with pharmacies
• Patient self-referral
• Physician referrals
• Pharmacy referrals (from non MTM providing pharmacies)
• Hospitals, care transition organizations, accountable care organization (ACO) affiliates, patient centered medical homes (PCMH).
|
| Referral Criteria |
• Enrollees meeting specified targeting criteria per CMS requirements:
o Annual drug costs >$4,696 (2022 figure)
o Minimum # drugs 2–8
o Target disease states
o Multiple chronic diseases
• Expanded criteria:
o Enrollees meeting other plan-specific criteria (agreed upon at the sponsor's application to CMS and annual review)
|
• Single chronic disease management
• Multiple chronic disease management
• Medication adherence issues
• Self-referral for any reason in self-refer model
|
| Reimbursement |
• Use of CPT codes:
o 99605
o 99606
o 99607
|
• Negotiated rates per contract with employee groups, or other groups
• Fee for service
|
| MTM Service |
• Must provide written summary in Comprehensive Medication Review (CMR) format:
1. Cover letter
2. Medication List
3. To-Do List
• Discuss concerns with drug therapy; summary of purpose and instructions for medications; review medications including non-Rx, supplements; engage beneficiaries in management of drug therapy.
• Core elements of MTM model
• May include other value- added services; however, reimbursement may be a constraint.
|
• CMS MTM CMR recommended (see left)
• Core elements of MTM model
• Additional services may include:
o adherence support
o outside consultation with other healthcare providers
o continuity of care/care transition services
o provider protocols
|
| Table provided courtesy of Demetra Antimisiaris, PharmD |
MEDICARE PART D MTM CRITERIA
Medicare Part D "sponsors" (or payers) are private insurance companies that contract with Medicare to provide drug benefits to Part D enrollees.5 Sponsors may offer their own MTM services (often provided via phone), or they may contract with pharmacies or specialized MTM organizations to provide phone or in-person MTM services. If so, sponsors will refer candidates to the pharmacy setting for MTM, based on the Medicare Part D criteria outlined below.
For automatic enrollment (eligibility) in MTM based on Medicare Part D requirements, patient must meet all 3 criteria:6
- Patient with multiple chronic diseases
The sponsor may set eligibility for MTM at 2 or more chronic diseases. The sponsor can be more inclusive (e.g., they can sponsor MTM for people with 1 chronic disease as the minimum.) Sponsors cannot require patients to have more than 3 chronic diseases in order to receive MTM benefits.
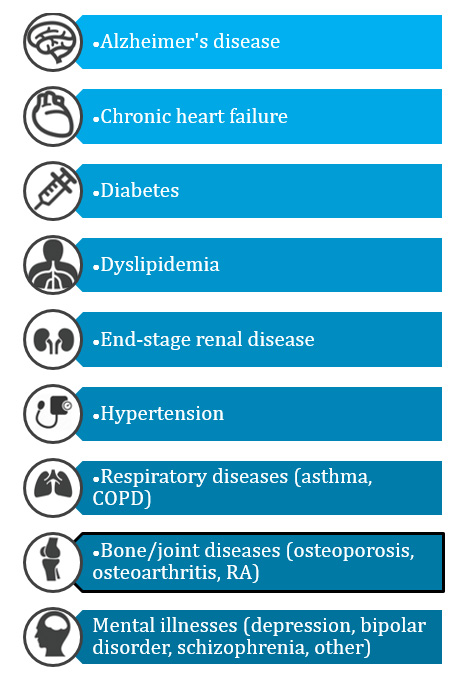
The sponsor may elect to cover MTM for any set of chronic diseases, but they must include at least 5 of the 9 "core" chronic conditions shown in Figure 1.7
- Patient taking multiple drugs covered by Medicare Part D
Each Medicare Part D sponsor determines the specific drugs covered under its formulary. The sponsor may set the minimum number of drugs required for a patient to qualify for MTM at any range between 2 and 8. That is, the sponsor may offer MTM for those taking just 1 covered drug, but they cannot require that patients be taking more than 8 drugs to receive MTM services.4
- Patient likely to incur high drug costs
CMS increases this amount each year by a margin of 11.76%. For 2022 the amount under Medicare Part D is ≥ $4,696, and for 2023 the cost threshold is $4,935. The sponsors look at first-quarter drug spending to determine the likelihood of spending this amount.7
A new requirement (CFR 423.100) implemented in January 2021 was the inclusion of “at-risk beneficiaries” who meet Overutilization Monitoring System (OMS) criteria, meaning that the patient may be at risk for adverse events or overdose of frequently abused drugs such as opioids or benzodiazepines.6 There are exemptions made for patients being medicated for active cancer pain, in hospice or palliative end-of-life care, or long-term care facilities. An example of an at-risk beneficiary would be a patient who is receiving opioids from multiple prescribers or pharmacies.6 At-risk beneficiaries do not have to meet other MTM criteria, (although there could be overlap).
| Figure 1. CMS Core Chronic Conditions7 |
 |
| Expanded criteria: Medicare Part D sponsors are encouraged by CMS to have additional expanded criteria in order to offer MTM to a wider patient base. They cannot make the criteria narrower, but they can optimize their programs, "to offer MTM to beneficiaries who will benefit the most from these services."7 |
How should eligible Medicare Part D recipients be contacted for MTM services?
Although contacting Medicare Part D candidates for MTM is done by the sponsors, pharmacists should understand the method by which patients are approached. Medicare requires that patients who meet sponsor/CMS requirements be "automatically enrolled" for MTM. This means that the patient is considered to be enrolled unless he or she specifically opts out, or declines enrollment. If a patient meets the sponsor's criteria, he or she is automatically enrolled and must be considered enrolled for that calendar year even if the person's health circumstances change.7
Sponsors are required to use more than one approach to reach eligible targeted beneficiaries for MTM, rather than using passive offers only (such as a mailed flyer). So if a letter is sent, sponsors are expected to follow up via phone if there is no response.7 Each sponsor is expected to review its patient data quarterly to target potential MTM recipients. In addition, patients enrolled in Medicare Part D can proactively contact the sponsor's pharmacy benefit manager or the medical care provider (physician) to request Medicare Part D MTM services.
Website requirements
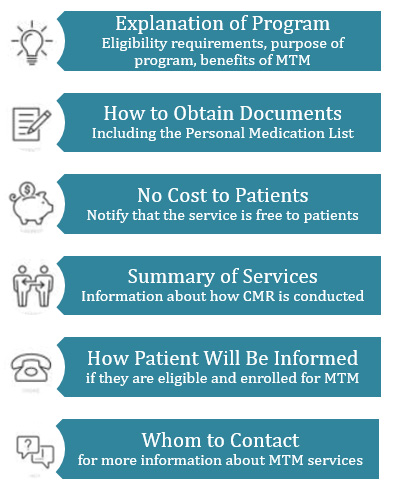
As of January 2022, CMS requires that MTM sponsors provide a website for patients with information about the MTM services it provides. The new ruling recommends that the site be accessible “by clicking through a maximum of two links” and that the website’s URL be kept accurate and functioning. Required elements for the sponsor’s MTM website are outlined in Figure 2.6
Figure 2. MTM Sponsor Website Elements6
A new ruling by CMS requires MTM sponsors to provide patients with access to a website containing the following: |
 |
How can pharmacists who provide MTM receive referrals for Medicare patients?
One way to receive referrals to provide MTM for this set of patients is to contact local providers of Medicare prescription drug coverage, including:
- Prescription Drug Plan–Part D (PDPs)
- Medicare Advantage–Part C
A listing of these providers can be found on the CMS.gov website:
http://www.cms.gov/Medicare/Prescription-Drug-Coverage/PrescriptionDrugCovContra/PartDContacts.html
In the video clip, two MTM experts discuss the issue of pharmacist reimbursement for MTM services and how that concept is evolving.
Third-Party MTM Organizations (e.g., Outcomes MTM)
Pharmacists who are MTM providers can also access eligible Medicare Part D enrollees through MTM provider companies like Outcomes MTM®. These companies act as third-party intermediaries between the health plan or payer and the pharmacy. The company provides names of identified patients to the pharmacy and assists with documentation and billing by providing software and other services.
Enhanced MTM Model Program For Specific Regions8
In 2017, CMS initiated a pilot program for "enhanced" MTM in 11 states to determine how expanded MTM services would influence costs and quality of care. Enhanced MTM encouraged more individualized interventions and engaged pharmacists more extensively in the MTM process. For example, pharmacists were asked to identify at-risk patients, optimize medication use, mediate communication with prescribers, and share information prior to office visits, such as comprehensive medication review (CMR) reports. The enhanced program also increased payments for more extensive MTM interventions.
After four years of implementation, the Enhanced MTM Model Program concluded in 2020. An analysis of the findings showed that Enhanced MTM services did not significantly reduce the cost of medical care (gross Medicare expenditures), including care of medically complex patients such as those with diabetes.8
TARGETING PATIENTS FOR MTM: BEYOND MEDICARE PART D
Clearly, there is a vast population of patients apart from those enrolled in Medicare who can benefit from MTM services, and for whom cost savings can be recognized. As shown in Table 1, this includes patients who are younger than 65, who may have only one chronic health condition, and who may be dealing with a common problem such as nonadherence.
If a pharmacy organization has an MTM program that serves employers, community groups, or individual pharmacy patrons, the criteria for patients to receive MTM may extend beyond the criteria outlined by Medicare Part D. Potential situations may include:
- Medicaid MTM programs required by states
As of 2022, states where MTM services can be reimbursed through the state’s Medicaid program include Colorado, Florida, Louisiana, Michigan, Minnesota, North Dakota, Tennessee, West Virginia, Wisconsin.9 Some states require face-to-face MTM, leading to local pharmacist opportunities and impact to those communities.
- Patients who are nonadherent to medications or medical therapies
Approximately 50% of patients with chronic diseases are nonadherent to medical therapies.10 Nonadherence may be identified via pharmacy records (failure to fill or refill prescriptions), from physician referral, or from lab records. Specific guidance on how to address adherence problems through MTM services are provided in Module 5.
- Recent care transition
Approximately 60% of medication-related errors in patient records occur during care transitions.7Hospital admissions and discharges, as well as changes in medical provider or care setting, are ideal opportunities for MTM. Accountable Care Organizations (ACOs) are groups that partner with pharmacists to offer MTM at the time of care transitions to reduce rehospitalization and promote safe and effective medication use.
- Change in health status
Improved patient education is needed for individuals who have undergone a recent change in health status. This may include patients who have received a new diagnosis for a chronic condition such as diabetes. Other circumstances include:
- Adverse events stemming from medication use or medication error
- Need for change in therapy, increased dosage of medication
- Progression of disease
- Laboratory values outside of normal range
- Patients using high-risk medications or complex medication regimens
According to the Institute of Medicine, gaps in medication knowledge can lead to medication errors. Patients may not understand how to use a drug, especially if its dosage and administration instructions are complex.11
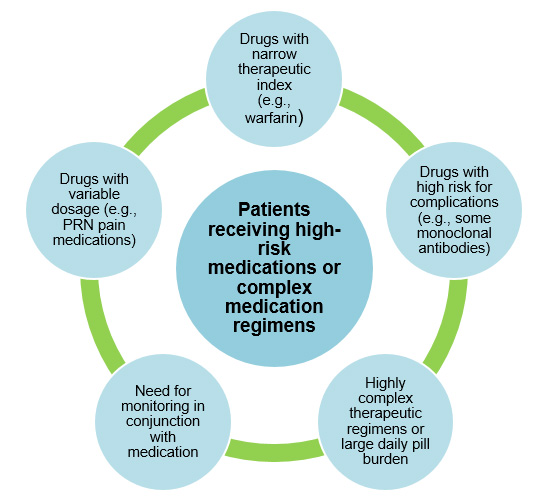
Through MTM, pharmacists provide an important service in addressing these patient education gaps. Patients using a device (such as an inhaler) may receive insufficient instructions in the physician's office, and often have forgotten the instructions by the time the prescription is filled.11 Situations that may be amenable to MTM are outlined in Figure 3.
| Figure 3. High-Risk/Complex Regimens Warranting MTM |
 |
- Request originating from healthcare provider or payer
Physicians and other healthcare providers often lack the time to provide thorough patient education, medication reconciliation, and adherence follow-up. These functions may be designated to a pharmacist who receives reimbursement for these services. Examples of such systems might include the Patient-Centered Medical Home (PCMH, defined in the sidebar) and Collaborative Practice Agreements (described in Module 16, Communication With Physicians and Other Healthcare Providers.
Payers may review utilization databases to identify patients who are frequently hospitalized or seek emergency care in order to identify patients who are candidates for MTM. This may be Medicare-eligible patients, but also other patients who are high utilizers of services.
- Patient self-referral for MTM services
Self-referral for MTM services probably does not happen often in the current healthcare environment. In theory, a pharmacist could provide MTM services on an individual basis for a fee, and the patient would realize cost savings in other ways such as fewer drugs or medical visits.12 This reflects a pharmacy trend where sole "product" is the pharmacist's health management knowledge. Some situations that might warrant one-on-one counseling with a pharmacist include:
- Wellness initiatives such as smoking cessation
- A need to reduce patients' out-of-pocket medication costs or medical costs
MTM SERVICES INVOLVING CAREGIVERS
There are many scenarios where MTM services should be delivered in the company of the patient as well as a close relative or caregiver.
If a patient is cognitively impaired or has a severe mental illness, MTM services may be provided directly to the caregiver/s, without the patient present. These decisions are made in conjunction with a healthcare provider such as the patient's physician. If a pharmacist providing MTM service believes that the patient is unable to understand or is unlikely to follow the instructions, this should be documented and shared with the healthcare provider. At that point, a healthcare proxy should determine who can legally make decisions on the patient's behalf and receive education about his or her care. CMS’s current requirements state, “The flexibility to perform the CMR with an individual other than the beneficiary. . .does not apply to situations where the sponsor is unable to reach the beneficiary (such as no response by mail, no response after one or more phone attempts, or lack of phone number or address), if there is no evidence of cognitive impairment, or where the beneficiary declines the CMR offer.”13
Some patients may elect to bring in a spouse, adult son or daughter, or other caregiver to participate in MTM. State laws vary as to how a third party may participate in medical decision-making; this information is usually available from the state's Department of Health. For MTM, this may involve just having the patient provide informal consent for a relative to sit in, a basic HIPAA form, or having paperwork prepared for a healthcare surrogate or power of attorney. Some of these situations might include:
- An elderly person who wants an adult son/daughter to participate in MTM;
- A person with a condition that may involve caregiver assistance (e.g., assistance with injections);
- Patient with a condition that renders them unable to help themselves in certain circumstances (e.g., a person with epilepsy or severe asthma, or a treatment that may cause mental cloudiness);
- A family member or friend who is a healthcare professional with medical knowledge that may help guide decision making
- Patients in long-term care settings
|
Definitions Used in Module 2
Medicare Part D Sponsor
Private insurance companies or payers that contract with Medicare to provide drug benefits to Medicare Part D enrollees.
Patient-Centered Medical Home (PCMH)
A model or philosophy of primary care that is patient-centered, coordinated, team-based, accessible, and focused on quality and safety. A philosophy of healthcare delivery that encourages providers/care teams to meet patients where they are; treat patients with respect, dignity, and compassion; and enable trusting relationships with providers and staff.
Collaborative Practice Agreement
An agreement that defines a formal relationship between pharmacists and physicians or other providers to allow for expanded patient-care services from the pharmacist and document the collaboration and cooperation of the provider.
Accountable Care Organization
As defined by CMS, ACOs are "groups of doctors, hospitals, and other healthcare providers, who come together voluntarily to give coordinated high-quality care to their Medicare patients."
|
REFERENCES
- Isetts BJ, Schondelmeyer SW, Artz MB, et al. Clinical and economic outcomes of medication therapy management services: the Minnesota experience. J Am Pharm Assoc (2003). Mar-Apr 2008;48(2):203-214.
- Lin HW, Lin CH, Chang CK, et al. Economic outcomes of pharmacist-physician medication therapy management for polypharmacy elderly: A prospective, randomized, controlled trial. J Formos Med Assoc. Mar 2018;117(3):235-243.
- Schultz BG, Tilton J, Jun J, Scott-Horton T, Quach D, Touchette DR. Cost-Effectiveness Analysis of a Pharmacist-Led Medication Therapy Management Program: Hypertension Management. Value Health. Apr 2021;24(4):522-529.
- National Committee for Quality Assurance (NCQA). Benefits of NCQA Patient-Centered Medical Home Recognition: Latest Evidence. June 2019. Available at: https://www.ncqa.org/wp-content/uploads/2019/09/20190926_PCMH_Evidence_Report.pdf.
- Office of the Inspector General, Department of Health and Human Services. Medicare Part D Sponsors. OEI-02-07-00460, Oct 2007.
- Centers for Medicare & Medicaid Services (CMS). 2021 Part D Drug Management Program Guidance. December 23, 2020. Available at: https://www.cms.gov/files/document/cy-2021-part-d-dmp-guidance-memo-december-22-2020.pdf.
- Centers for Medicare & Medicaid Services (CMS). Contract Year 2023 Medication Therapy Management Program Information and Submission Instructions. April 15, 2022. Available at: https://www.cms.gov/files/document/memo-contract-year-2023-medication-therapy-management-mtm-program-submission-v041522.pdf
- Acumen LLC. Evaluation of the Part D Enhanced Medication Therapy Management (MTM) Model: Fourth Evaluation Report. April 2022. Available at: https://innovation.cms.gov/data-and-reports/2022/mtm-fourth-evalrept.
- National Board of Medication Therapy Management. (2022). State Medicaid Requirements for CMRs and TMRs. Available at: https://www.nbmtm.org/mtm-reference/state-medicaid-requirements-cmrs-tmrs/.
- Brown MT, Bussell JK. Medication adherence: WHO cares? Mayo Clin Proc. Apr 2011;86(4):304-314.
- Aspden P, Wolcott J, Bootman JL, et al (Eds). Preventing Medication Errors. Institute of Medicine, Committee on Identifying and Preventing Medication Errors. National Academies Press, 2007.
- Wittayanukorn S, Westrick SC, Hansen RA, et al. Evaluation of medication therapy management services for patients with cardiovascular disease in a self-insured employer health plan. J Manag Care Pharm. Jun 2013;19(5):385-395.
- Centers for Medicare & Medicaid Services. 2021 Part D Drug Management Program Guidance. December 23, 2020. Available at: https://www.cms.gov/files/document/cy-2021-part-d-dmp-guidance-memo-december-22-2020.pdf.