ADVERTISEMENT

PHARMACIST’S GUIDE TO PATIENT SELF-MANAGEMENT OF HEART FAILURE
Individualizing Pharmacologic Treatment Approaches in Heart Failure
Chronic heart failure is a debilitating, often fatal disease that results in major health and socioeconomic consequences. The number of people with heart failure is expected to rise from the 6.2 million observed in 2016 to more than 8 million in 2030.1,2 Nearly 30% of Medicare beneficiaries do not survive 1 year following hospitalization for heart failure.1 In addition to frequent rehospitalization,3 heart failure causes significant reduction in health-related quality of life, both in psychological and physical functioning.4,5
TYPES AND CLASSIFICATION OF HEART FAILURE
Heart failure is generally grouped into two main types based on left ventricular functional abnormalities: heart failure with reduced ejection fraction (HFrEF) and heart failure with preserved ejection fraction (HFpEF).6 HFrEF is also referred to as systolic dysfunction and is characterized by thin and weakened heart muscle. In HFrEF, the heart has diminished contractility and is, therefore, unable to eject an adequate amount of blood to the body. The left ventricular ejection fraction (LVEF), which is the percentage of blood that is squeezed out of the left ventricle with each contraction, is generally defined as HFpEF, also called diastolic dysfunction, is often associated with a hypertrophic, stiffened heart muscle which leads to poor myocardial relaxation. Because the heart cannot effectively relax, it is not able to fill with and subsequently pump out a substantial amount of blood with each contraction. In HFpEF, the LVEF is normal or mildly abnormal and is usually ≥50 percent. While the benefits of many classes of medications are established for HFrEF, there are no therapies that have been proven to effectively treat HFpEF. Consequently, HFpEF treatment typically focuses on the underlying causes, such as hypertension or coronary artery disease.
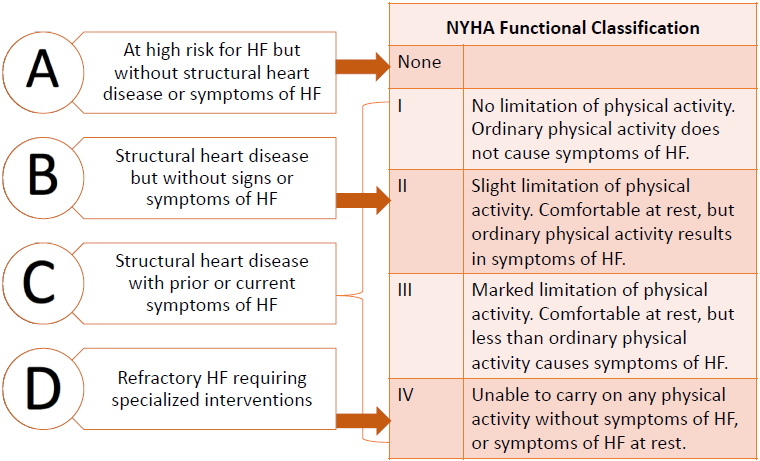
Two different but complementary systems are used to classify heart failure (Figure 1).7 One is the New York Heart Association (NYHA) Functional Classification System, which divides heart failure into four classes. The NYHA classification system has been used for decades and is commonly used in clinical trials. It focuses on exercise capacity and symptomatic status of heart failure.7
|
Figure 1. ACC/AHA heart failure stage and NYHA functional classification7
|
| Reprinted with permission from Yancy CW, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;62(16):e147-239. |
The other system for classifying heart failure was developed by the American College of Cardiology and the American Heart Association (ACC/AHA).7 The ACC/AHA system emphasizes the development and progression of heart failure and can be used to describe individuals and populations.
BENEFITS OF PHARMACOTHERAPY IN HEART FAILURE WITH REDUCED EJECTION FRACTION
The mortality benefits of several classes of medications for HFrEF are well established. Angiotensin-converting enzyme (ACE) inhibitor therapy has been shown to reduce all-cause mortality by 16% (mean 41.4 months)8 and angiotensin receptor blocker (ARB) therapy by 12%; median 40 months.9 Mortality reductions are greater with beta-blocker10,11 (34%) and mineralocorticoid receptor antagonist (MRA) (30%) therapy in patients on background therapy of diuretics and renin-angiotensin-aldosterone system (RAAS) inhibitor therapy.12,13 Moreover, the mortality benefit from adding a MRA to an ACE inhibitor is greater than with an ACE inhibitor alone.13 Mortality risk is further reduced with the addition of a beta-blocker to an ACE inhibitor and MRA.14,15 More recently, angiotensin receptor-neprilysin inhibitor (ARNI) therapy has been shown to reduce the risk of death and hospitalization in patients with HFrEF.15
SUBOPTIMAL USE OF PHARMACOTHERAPY IN HEART FAILURE WITH REDUCED EJECTION FRACTION
Recent evidence from the CHAnge the Management of Patients with Heart Failure (CHAMP-HF) registry showed that pharmacologic treatment of patients with HFrEF is suboptimal (Table 1).16 A key finding from the registry was that a quarter (26.2%) of the patients did not have a contraindication to RAAS inhibitor therapy, yet did not receive an ACE inhibitor, ARB, or ARNI. Additionally, one-third (32.9%) did not receive a beta-blocker, with even fewer receiving an evidence-based beta-blocker (bisoprolol, carvedilol, or metoprolol succinate). Similarly, about two-thirds (65.9%) of the patients were not on an MRA.
|
Table 1. CHAMP-HF Registry16
Objective: To characterize the patterns and factors associated with the use and dose of medications used for HFrEF
Methods:
- Registry of outpatients in the United States with chronic HFrEF receiving at least 1 oral medication for heart failure management
- Patients (N=3518)
- Adults with chronic heart failure and LVEF £40%
- Medications: angiotensin-converting enzyme inhibitor, angiotensin receptor blocker, angiotensin receptor-neprilysin inhibitor, beta-blocker, mineralocorticoid receptor antagonist, antihypertensives, vasoactive/inotropic agents, other
|
The findings from the CHAMP-HF registry are especially concerning for a number of reasons. First, as noted earlier, several classes of medications have been shown to reduce mortality, with the greatest benefit from treatment with combination therapy as recommended in current guidelines.17 Despite guideline recommendations and evidence indicating mortality benefit, these medications are still being greatly underutilized in practice. Second, the natural history of heart failure suggests that once patient function begins to deteriorate, as in patients with NYHA class III, improvement to NYHA class I or II is unlikely, and further disease progression is common.18 This observation underscores the importance of treating patients early and aggressively with guideline-directed medical therapy.
Guidelines for the management of heart failure were published in 20137 and subsequently updated in 2017 following the 2015 approvals of ivabradine and sacubitril/valsartan in the United States.19 In 2018, the American College of Cardiology published a decision pathway for optimizing the treatment of patients with NYHA stage C HFrEF.17 A key recommendation is that all patients with stage C HFrEF should be treated initially with the combination of RAAS inhibitor therapy, specifically an ACE inhibitor or ARB, and a beta-blocker (Figure 2). In addition, a diuretic should be added for patients with symptoms of fluid overload.
Figure 2. Guideline-directed medical therapy for Stage C HFrEF17
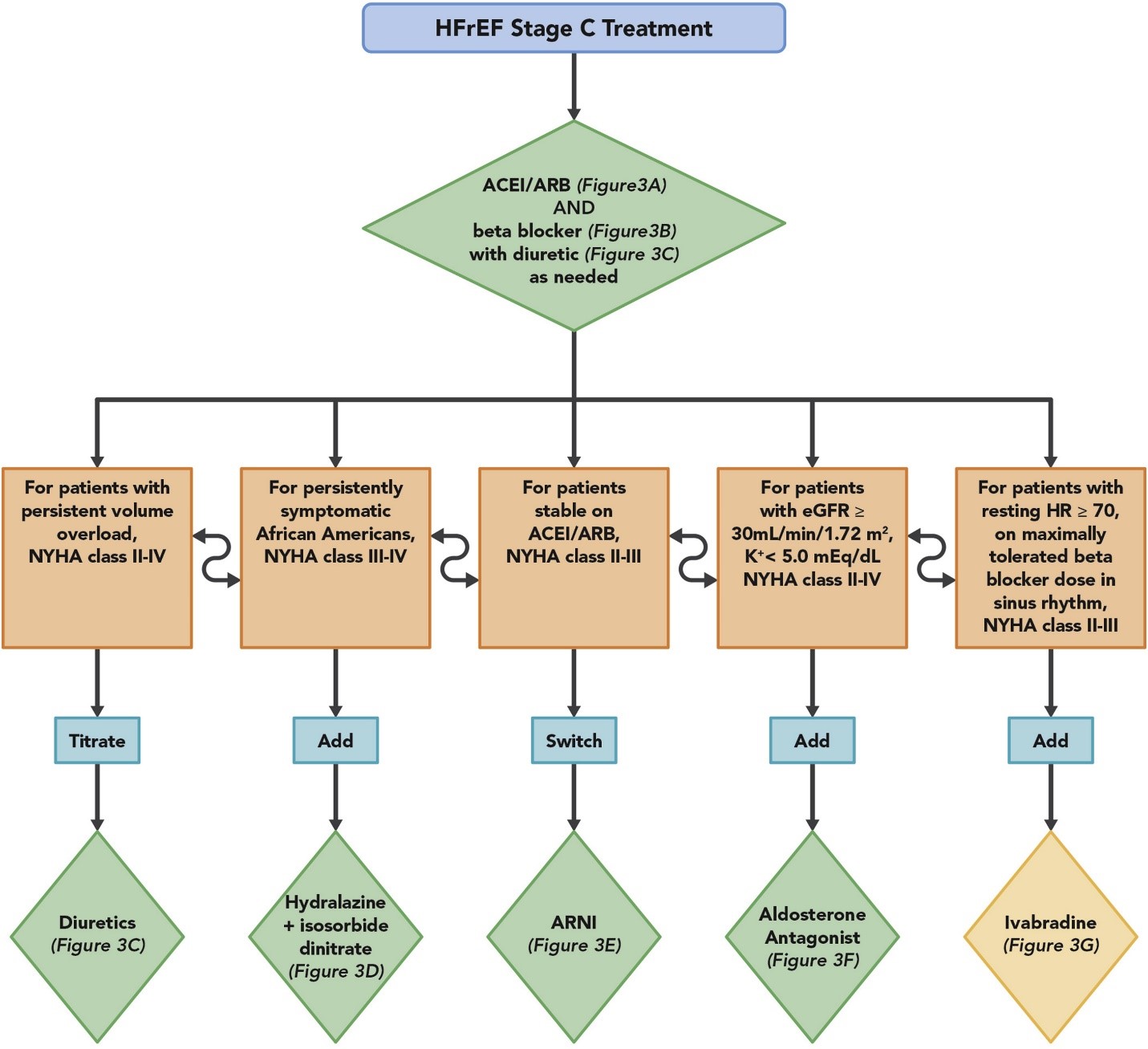 |
| Green diamonds indicate Class I guideline recommendations, while the yellow diamond indicates a Class II recommendation. ACEI, angiotensin-converting enzyme inhibitors; ARB, angiotensin receptor blockers; ARNI, angiotensin receptor-neprilysin inhibitor; eGFR, estimated glomerular filtration rate; HFrEF, heart failure with reduced ejection fraction; HR, heart rate; NYHA, New York Heart Association. |
| Reprinted with permission from Yancy CW, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;62(16):e147-239. |
Subsequent treatment is individualized based on patient characteristics. If the patient has persistent volume overload, adjusting the dose of the diuretic is the appropriate treatment. For an African-American patient who has persistent symptoms of HFrEF, using either the fixed-dose combination of isosorbide dinitrate and hydralazine or using the two components individually would be appropriate. For patients who have adequate renal function and normal serum potassium, adding an MRA is recommended. Patients stable on ACEI/ARB can be switched to sacubitril/valsartan. For patients who have a resting heart rate Digoxin may be considered as initial therapy in patients with severe symptoms or in patients with persistent symptoms of HFrEF.7
Case Study
RW is a 57-year-old male diagnosed 7 months ago during a hospitalization with NYHA class II, AHA/ACC stage C HFrEF. Doppler echocardiography revealed an ejection fraction of 30% to 35%. During his hospitalization, RW was started on an ACEI, beta-blocker, and loop diuretic. Medication doses were titrated over the subsequent 3 months.
· Past medical history: hypertension (poorly controlled with HCTZ 25 mg/day). No other comorbidities.
· Current medications:
· Lisinopril 20 mg once daily
· Metoprolol succinate 200 mg once daily
· Furosemide 80 mg once daily
At a follow-up visit 4 months ago, his serum creatinine (1.0 mg/dL) and serum potassium level (4.0 mEq/L), as well as other laboratory values were within normal limits. Spironolactone 25 mg once daily was started.
A recheck 1 month later revealed serum creatinine 1.1 mg/dL and serum potassium 4.3 mEq/L.
He remained symptomatic with 2+ pedal edema with cool extremities; coarse crackles could be heard bilaterally in posterior lung bases.
· Vital signs: BP 142/86 mmHg; pulse 88 bpm, regular
· Body weight 208 lbs (body mass index 30.8 kg/m2)
The dose of furosemide was increased to 80 mg twice daily.
1. Is RW being treated with guideline-directed medical therapy?
2. What changes, if any, do you recommend?
|
RW remains symptomatic despite treatment with three classes of guideline-directed medications. However, his dose of lisinopril is at the low end of the target dose of 20 to 40 mg/day. In addition, his blood pressure remains elevated and he has obesity, both of which require further consideration for treatment. Of greatest concern is that his pulse remains elevated at 88 beats per minute despite treatment with the guideline-directed target dose of metoprolol succinate.
IVABRADINE
SHIFT Trial
Having an elevated heart rate is a known risk factor for cardiovascular death in patients with heart failure. The Systolic Heart failure treatment with the If inhibitor ivabradine Trial (SHIFT) (Table 2) assessed the effect of heart rate reduction with ivabradine in patients with HFrEF.20 SHIFT showed that patients with a heart rate ≥87 beats per minute were at more than two-fold higher risk for the primary composite endpoint of cardiovascular death or heart failure hospitalization than patients with heart rate 70 to <72 beats per minute.21 The risk of the primary composite endpoint increased 3% for every 1 beat per minute increase in baseline heart rate. Of key importance is that in patients treated with ivabradine, Analysis revealed that the benefits observed with ivabradine resulted from pure heart rate reduction, which is consistent with ivabradine’s known pharmacologic effects.22
|
Table 2. SHIFT Trial20
Objective: To assess the effect of heart rate reduction with ivabradine on outcomes in adults with HFrEF
Methods:
- Randomized, double-blind, placebo-controlled, parallel-group, multicenter, phase 3
- Patients (N=6558)
- Adults with symptomatic heart failure and LVEF £35%
- HR ≥70 bpm, normal sinus rhythm
- Heart failure hospitalization within previous year
- Stable treatment with a beta-blocker, if tolerated
- Run-in phase to confirm inclusion/exclusion criteria
- Randomized to ivabradine 5 mg twice daily or placebo
- Ivabradine dose titrated based on heart rate after 14 days
Primary endpoint: composite of CV death or heart failure hospitalization
Median follow-up: 22.9 months
|
In the SHIFT trial, the significant reduction in the composite endpoint observed with ivabradine was driven by heart failure hospitalization as the difference in cardiovascular death was not significantly different between the ivabradine and placebo groups.20 Other significant reductions observed with ivabradine vs placebo included cardiovascular hospitalization, all-cause hospitalization, and heart failure mortality, but not all-cause death.
Ivabradine proved to be well tolerated in the SHIFT trial, with similar adverse event rates in the ivabradine and placebo groups. An adverse event of any grade was experienced by 75% in the ivabradine group and 74% in the placebo group. The adverse events of any grade that occurred significantly more frequently in the ivabradine group, all in <10% of patients, included bradycardia (both symptomatic and asymptomatic), hypertension, increased incidence of atrial fibrillation, and phosphenes (transient enhanced brightness in a restricted area of the visual field.) There was no significant difference between the 2 groups in the occurrence of an adverse event that led to drug withdrawal.
The SHIFT trial showed that ivabradine is a safe, effective medication in patients with stable, symptomatic chronic heart failure with LVEF ≤35%, who are in sinus rhythm with resting heart rate ≥70 bpm and either are on maximally tolerated doses of beta-blockers or have a contraindication to beta-blocker therapy.
Approved Indications for Use
Ivabradine is approved to reduce the risk of hospitalizations for worsening heart failure in adults with stable, symptomatic, chronic HFrEF. Ivabradine is also approved for the treatment of stable, symptomatic heart failure due to dilated cardiomyopathy in children age ≥6 months. Adults who are appropriate candidates for ivabradine therapy mirror the inclusion criteria for the SHIFT trial, ie, adults with NYHA class II or III symptoms, left ventricular ejection fraction £35%, in sinus rhythm with a resting heart rate ≥70 beats per minute, and who are taking a maximally-tolerated dose of beta-blocker unless contraindicated. This last requirement that beta-blocker therapy must be optimized prior to initiating ivabradine is especially important.
Contraindications and Other Considerations for Use
Ivabradine should be avoided in patients with acute decompensated heart failure, clinically significant hypotension, sick sinus syndrome, sinoatrial block, or third-degree AV block unless a functioning demand pacemaker is present, clinically significant bradycardia, severe hepatic impairment, or heart rate maintained exclusively by a pacemaker. In addition, ivabradine is contraindicated in combination with strong CYP3A4 inhibitors eg, clarithromycin, diltiazem, verapamil, itraconazole, ketoconazole, and ritonavir.
During treatment with ivabradine, heart rate should be monitored closely, especially for symptoms of bradycardia and atrial fibrillation. Ivabradine is not recommended in patients with second-degree AV block. Female patients should use effective contraception when taking ivabradine.
Dosing
Before initiating treatment with ivabradine, beta-blocker therapy must be optimized (unless contraindicated) to ensure an adequate blood pressure, ie, ≥90/50 mmHg, and patient tolerability. In adults, the usual initial dose is 5 mg twice a day, taken with food. In vulnerable adults in whom bradycardia could cause hemodynamic compromise, the recommended initial dose is 2.5 mg twice a day. The dose can be adjusted after two weeks based on the heart rate. If the heart rate is <50 beats per minute or if the patient experiences symptoms of bradycardia, the dose should be reduced by 2.5 mg twice a day. If the patient is already on a dose of 2.5 mg twice a day, ivabradine should be discontinued. If the heart rate is 50 to 60 beats per minute, the dose should be maintained, with appropriate heart rate monitoring. If the heart rate is >60 beats per minute, the dose can be increased by 2.5 mg twice a day, until a maximum dose of 7.5 mg twice a day is achieved.
Summary
In summary, heart rate reduction with ivabradine in patients with symptomatic HFrEF results in a significant reduction in heart failure hospitalization. The magnitude of this effect increases with increasing heart rate prior to initiating ivabradine. Safety considerations include patients who have hypertension, bradycardia or other conduction abnormality, or atrial fibrillation.
Case Study (cont)
RW returned to clinic 4 months later. Physical examination revealed:
· Vital signs: BP 136/80 mmHg; pulse 78 bpm, regular
· Body weight 201 lbs (BMI 30.0 kg/m2
· Jugular venous pressure 10 cm; carotids full
· Lungs: fine inspiratory crackles; mildly short of breath
· Cool extremities
Current medications:
· Lisinopril 20 mg once daily
· Metoprolol succinate 200 mg once daily
· Furosemide 80 mg twice daily
· Spironolactone 25 mg once daily
· Ivabradine 7.5 mg twice daily
What changes, if any, do you recommend?
|
RW still exhibits symptoms of fluid overload, thus increasing his dose of furosemide to 120 mg twice daily is reasonable. The furosemide dose should be reevaluated in a few days based upon his response. His pulse remains above the ideal range of 60 to 70 beats per minute, but he is being treated with the recommended doses of metoprolol succinate and ivabradine. Another change to consider is switching RW from his ACE inhibitor lisinopril to the ARNI sacubitril/valsartan to further reduce morbidity and mortality as suggested in the 2017 ACC Consensus Decision Pathway.17 Stopping an ACE inhibitor at least 36 hours prior to initiating sacubitril/valsartan is required.
SACUBITRIL/VALSARTAN
Sacubitril/valsartan is a combination medication containing a neprilysin inhibitor (sacubitril) and an ARB (valsartan). Valsartan inhibits the effects of angiotensin II by selectively blocking the angiotensin II type 1 receptor, as well as inhibiting angiotensin II-dependent aldosterone release. Sacubitril blocks the effects of neprilysin, an enzyme that breaks down endogenous peptides that promote vasodilation and diuresis, as well as reduce myocardial fibrosis and hypertrophy. It is this dual mechanism of action of sacubitril/valsartan of simultaneously reducing aldosterone levels and preventing the breakdown of endogenous peptides that cause vasodilation that produces the beneficial effects in patients with HFrEF.
PARADIGM-HF Trial
The Prospective Comparison of ARNI with ACEI to Determine Impact on Global Mortality and Morbidity in Heart Failure (PARADIGM-HF) trial was conducted to assess the efficacy and safety of sacubitril/valsartan vs an active control, enalapril, in the outpatient setting (Table 3).15 The primary outcome of the study was a composite of death from cardiovascular causes or heart failure hospitalization.
|
Table 3. PARADIGM-HF Trial15
Objective: To examine whether the long-term effects of sacubitril/valsartan on morbidity and mortality were superior to those of ACE inhibition with enalapril
Methods:
- Randomized, double-blind, active-controlled, parallel-group, multicenter, phase 3
- Patients (N=8399)
- Adults with NYHA class II, III, or IV symptoms and LVEF £35%
- BNP level ≥150 pg/mL or NT-proBNP level ≥600 pg/mL; if hospitalized for heart failure within previous 12 months: BNP ≥100 pg/mL or NT-proBNP ≥400 pg/mL
- If taking ACEI or ARB, required to take a stable dose of beta-blocker and ACEI (or ARB) equivalent to at least 10 mg enalapril daily
- Screening period, single-blind run-in period during which all patients received enalapril, followed by a single-blind run-in period during which all patients received sacubitril/valsartan
- Randomized to sacubitril/valsartan 97 mg/103 mg twice daily or enalapril 10 mg twice daily
Primary endpoint(s): composite of CV death or heart failure hospitalization
Median follow-up: 27 months
|
PARADIGM-HF was stopped early because the boundary for overwhelming benefit with sacubitril/valsartan was crossed after a median follow-up of 27 months. At the time the study was stopped, the primary outcome had occurred in 21.8% and 26.5% of sacubitril/valsartan and enalapril patients, respectively (hazard ratio (HR) 0.80; 95% confidence interval (CI) 0.73-0.87; P<0.001). There were significant reductions in the individual components of the primary outcome, as well as all-cause death, favoring sacubitril/valsartan vs enalapril.
The PARADIGM-HF trial showed sacubitril/valsartan to be well tolerated vs enalapril.15 A similar percentage of patients in the sacubitril/valsartan and enalapril groups experienced an adverse event (81.4% vs 82.8%, respectively), although significantly more patients in the enalapril group withdrew from the trial due to an adverse event (12.3% vs 10.7%, respectively). There was no significant difference in the first occurrence of decline in renal function or in new-onset atrial fibrillation between the two groups. Angioedema occurred in a small and similar percentage of patients in both groups. Symptomatic hypotension was significantly more common in the patients who received sacubitril/valsartan. Interestingly, significantly more patients treated with enalapril experienced renal impairment, serum potassium >6.0 mEq/L, and cough.
A pre-specified analysis of the PARADIGM study focused on non-fatal clinical deterioration.23 In comparison with the enalapril group, fewer sacubitril/valsartan-treated patients required intensification of medical treatment for heart failure (HR 0.84; 95% CI 0.74-0.94; P=0.003) or an emergency department visit for worsening heart failure (HR 0.66; 95% CI 0.52-0.85; P=0.001). Patients in the sacubitril/valsartan group had 23% fewer hospitalizations for worsening heart failure and were significantly less likely to require intensive care or to receive intravenous positive inotropic agents. The reduction in heart failure hospitalization with sacubitril/valsartan was evident after the first 30 days after randomization.
PIONEER-HF Trial
The PARADIGM-HF trial did not address the safety and efficacy of sacubitril/valsartan in the inpatient setting including patients with decompensated HFrEF. This was the population targeted by the Comparison of Sacubitril-Valsartan versus Enalapril on Effect on NT-proBNP in Patients Stabilized from an Acute Heart Failure Episode (PIONEER-HF) trial (Table 4).24 In this trial, the biomarker N-terminal pro-B-type natriuretic peptide (NT-proBNP) was used as a surrogate for efficacy, as it is a validated biomarker for neurohormonal activation, hemodynamic stress, and subsequent cardiovascular events. Treatment with sacubitril/valsartan vs enalapril resulted in a significantly greater time-averaged reduction in the NT-proBNP concentration at weeks 4 and 8 (ratio of change 0.71; 95% CI 0.63-0.81; P<0.001). The rates of worsening renal function, hyperkalemia, symptomatic hypotension, and angioedema did not differ significantly between the 2 groups. The results of the PIONEER-HF trial showed that the benefits of sacubitril/valsartan extend to the inpatient setting in patients with acute decompensated heart failure following hemodynamic stabilization.
|
Table 4. PIONEER-HF Trial24
Objective: To assess the efficacy and safety of sacubitril/valsartan compared with enalapril after hemodynamic stabilization in patients hospitalized for acute decompensated heart failure
Methods:
- Randomized, double-blind, active-controlled, parallel-group, multicenter, phase 3
- Patients (N=881)
- Adults with acute decompensated heart failure and LVEF £40%
- NT-proBNP ≥1600 pg/mL or BNP ≥400 pg/mL
- Randomized to sacubitril/valsartan 24 mg/26 mg or 49 mg/51 mg twice daily or enalapril 2.5 mg or 5 mg twice daily based on systolic blood pressure
Primary endpoint: time-averaged proportional change in the NT-proBNP level from baseline through weeks 4 and 8
Study duration: 8 weeks
|
Approved Indications for Use
Sacubitril/valsartan is approved to reduce the risk of cardiovascular death and hospitalization for heart failure in patients with chronic NYHA class II-IV HFrEF. It is usually administered in conjunction with other heart failure therapies, in place of an ACE inhibitor or ARB. Sacubitril/valsartan is also approved for treatment of symptomatic heart failure with systemic left ventricular systolic dysfunction in children age ≥1 year.
Contraindications and Other Considerations for Use
Patients treated with sacubitril/valsartan must be closely monitored for signs and symptoms of angioedema and hypotension. Renal function and serum potassium also must be monitored in susceptible patients. Contraindications for sacubitril/valsartan include history of angioedema related to previous administration of an ACE inhibitor or an ARB, concomitant use with an ACE inhibitor or ARB, and, in patients with diabetes, concomitant use with aliskiren. Sacubitril/valsartan is not recommended in women who are breastfeeding or in patients with severe hepatic impairment.
Possible drug-drug interactions include concomitant use of aliskiren in patients with an estimated glomerular filtration rate <60 mL/min/1.73 m2 or those treated with a potassium-sparing diuretic such as spironolactone. Since spironolactone is frequently used in patients with HFrEF, close monitoring of the serum potassium is important if sacubitril/valsartan and spironolactone are used concomitantly. The risk of renal impairment with the combined use of sacubitril/valsartan and a nonsteroidal anti-inflammatory drug (NSAID) is even greater than with an NSAID alone. Additionally, the use of sacubitril/valsartan in a patient taking lithium may increase the risk of lithium toxicity.
Dosing
A 36 hour-washout period is critical if switching a patient from an ACE inhibitor to sacubitril/valsartan. Since sacubitril/valsartan lowers blood pressure, it is important to ensure that the patient has adequate blood pressure and renal function, ie, eGFR The recommended initial dose is 49/51 mg twice a day in adults. If tolerated, the dose is doubled after 2 to 4 weeks to the target maintenance dose of 97/103 mg twice daily. If there is concern about a patient having adequate blood pressure, initiating treatment at the lower dose of 24/26 mg twice a day should be considered. Blood pressure, electrolytes, and renal function should be monitored.
Summary
Results of the PARADIGM-HF and PIONEER-HF trials provide extensive data to support the use of sacubitril/valsartan in patients with HFrEF. Benefits observed with sacubitril/valsartan in patients with HFrEF include a reduction in cardiovascular death and heart failure hospitalization as well as all-cause mortality.
HYPERTENSION
Hypertension is a common risk factor for chronic heart failure.25 In the CHAMP-HF registry, 82% of patients had a history of hypertension.
In patients with heart failure and blood pressure 130-139/80-89 mmHg, monotherapy with 1 first-line medication is recommended.26 If the blood pressure is higher, dual therapy with 2 first-line medications is recommended. The choice of monotherapy vs dual therapy is based on the higher of the systolic or diastolic pressure. For example, a patient with blood pressure 144/84 mmHg would require initiation of dual therapy. Since patients with HFrEF are generally receiving treatment with an ACE inhibitor/ARB and a beta-blocker, the initial step is to ensure treatment with the highest recommended doses, if tolerated.
DIABETES MELLITUS
Heart failure is very common in people with type 2 diabetes mellitus (T2DM). In fact, people with T2DM have over twice the risk of heart failure than people without T2DM.3,27,28 In the CHAMP-HF registry, approximately 41% of patients had a history of T2DM.16
Over the past decade, more than 20 randomized clinical trials have been conducted to assess the safety of newer classes of medications for T2DM. These trials have shown that all of the dipeptidyl peptidase-4 inhibitors (DPP-4is), glucagon-like peptide-1 receptor agonists (GLP-1RAs), and sodium glucose cotransporter-2 inhibitors (SGLT-2is) (Tables 5-8) currently available are non-inferior to placebo as part of standard therapy in terms of cardiovascular safety.29 Moreover, some of the GLP-1RA and SGLT-2i medications have been shown to reduce one or more cardiovascular events.29 Based upon this evidence, the American Diabetes Association (ADA) has substantially modified its treatment recommendations for patients with established atherosclerotic cardiovascular disease, heart failure, or chronic kidney disease who have not achieved adequate glycemic control with optimized lifestyle management and metformin.30
|
Table 6. DECLARE-TIMI 58 Trial32
Objective: To evaluate the effects of dapagliflozin on CV and renal outcomes in a broad population of patients who had or were at risk for atherosclerotic CV disease
Methods:
- Randomized, double-blind, placebo-controlled, parallel-group, multicenter, phase 3
- Patients (N=17,160)
- Adults age ≥40 years with T2DM, A1C ≥6.5% and <12.0%, and creatinine clearance ≥60 mL/min
- Multiple risk factors for atherosclerotic CV disease or established CV disease
- Screening period to confirm eligibility
- Randomized to dapagliflozin 10 mg or placebo once daily plus standard care
Primary endpoint(s): composite of CV death, nonfatal myocardial infarction, nonfatal stroke; composite of CV death or hospitalization for heart failure
Median follow-up: 4.2 years
|
|
Table 8. VERTIS-CV Trial39
Objectives:
- To demonstrate non-inferiority of ertugliflozin versus placebo on major adverse cardiovascular events
- To demonstrate superiority of ertugliflozin versus placebo on time to: 1) the composite of CV death or heart failure hospitalization; 2) CV death; and 3) the composite of renal death, dialysis/transplant, or doubling of serum creatinine from baseline
Methods:
- Randomized, double-blind, placebo-controlled, parallel-group, multicenter, phase 3
- Patients (N=8252)
- Adults age ≥40 years with T2DM and A1C ≥7.0% and £5%
- Stable, established atherosclerotic cardiovascular disease
- BMI ≥18 kg/m2
- eGFR ≥30 mL/min/1.73 m2
Primary endpoint(s): time to the first event of CV death, nonfatal MI, or nonfatal stroke
Median follow-up: –
|
For patients with established heart failure and inadequate glycemic control with lifestyle management and metformin, the ADA recommends an SGLT-2i as first-line. Alternatively, a GLP-1RA with proven cardiovascular benefit can be used if an SGLT-2i is not tolerated or contraindicated or if renal function is not adequate.30 All 4 of the SGLT-2is have been shown to reduce heart failure hospitalization: canagliflozin 33%, dapagliflozin 17%, empagliflozin 35%, and ertugliflozin 30%. For example, in the CANVAS trial (Table 5), canagliflozin reduced heart failure death or hospitalization for heart failure by 30% compared with placebo.35 There was no clear difference in effects on HFrEF vs HFpEF events, although this was not the primary outcome for the study. Additionally, sub-analyses of the EMPA-REG OUTCOME trial with empagliflozin (Table 7) showed significant reduction in hospitalization for heart failure in patients with or without prior myocardial infarction or stroke or prevalent kidney disease at baseline.36,37
|
Table 5. CANVAS Trial31
Objective: To assess the cardiovascular safety and efficacy of canagliflozin and to evaluate the balance between any potential benefits of canagliflozin and the risks associated with it
Methods:
- Randomized, double-blind, placebo-controlled, parallel-group, multicenter, phase 3
- Patients (N=4330)
- Adults with T2DM and glycated hemoglobin ≥7.0% and £5%
- eGFR >30 mL/min/1.73 m2
- Age ≥30 years with symptomatic ASCVD or ≥50 years with ≥2 of the following:
- T2DM duration ≥10 years
- Systolic blood pressure >140 mmHg despite treatment
- Current smoking
- Microalbuminuria or macroalbuminuria
- High-density lipoprotein cholesterol £39 mg/dL
- Single-blind, placebo run-in period
- Randomized to canagliflozin 100 mg or 300 mg or placebo once daily plus standard care
Primary endpoint(s): composite of CV death, nonfatal myocardial infarction, nonfatal stroke
Median follow-up: 188.2 weeks
|
|
Table 7. EMPA-REG OUTCOME Trial33
Objective: To examine the effects of empagliflozin as compared with placebo on cardiovascular morbidity and mortality in patients with T2DM and established CV disease
Methods:
- Randomized, double-blind, placebo-controlled, parallel-group, multicenter, phase 3
- Patients (N=7020)
- Adults with T2DM and
- No glucose-lowering agents for ≥12 weeks before randomization with A1C ≥7.0% and £0% or
- Stable glucose-lowering therapy for ≥12 weeks before randomized and A1C ≥7.0% and £10%
- Established CV disease
- BMI £45 kg/m2
- eGFR ≥30 mL/min/1.73 m2
- Randomized to empagliflozin 10 mg or 25 mg or placebo once daily plus standard care
Primary endpoint(s): composite of CV death, nonfatal MI, or nonfatal stroke
Median follow-up: 3.1 years
|
DAPA-HF Trial
The DAPA-HF trial is different from the cardiovascular outcome trials previously discussed in that DAPA-HF focused on the use of dapagliflozin in HFrEF; fewer than half (42%) of the patients had T2DM (Table 9).38 The results showed a 26% reduction with dapagliflozin vs placebo in the primary composite endpoint of worsening heart failure or cardiovascular death (HR 0.74; 95% CI 0.65-0.85; P<0.001). Significant reductions were also observed with dapagliflozin for hospitalization or urgent visit for heart failure (30% reduction), hospitalization for heart failure (30% reduction), urgent visit for heart failure (57% reduction), and CV death or hospitalization for heart failure (25% reduction). Importantly, the significant reduction in the primary composite event observed with dapagliflozin was similar in patients with and without T2DM. This suggests that the benefits of dapagliflozin in HFrEF involve nonglycemic mechanisms.
|
Table 9. DAPA-HF Trial38
Objective: To evaluate the efficacy and safety of dapagliflozin in patients with HFrEF and with or without T2DM
Methods:
- Randomized, double-blind, placebo-controlled, parallel-group, multicenter, phase 3
- Patients (N=4744)
- Adults with NYHA class II, III, or IV symptoms and LVEF £40%
- NT-proBNP ≥600 pg/mL; if hospitalized for heart failure within previous 12 months: NT-proBNP ≥400 pg/mL; if atrial fibrillation or atrial flutter: NT-proBNP ≥900 pg/mL
- Implantable cardioverter-defibrillator and/or cardiac resynchronization therapy
- ACEI, ARB, or sacubitril/valsartan + beta-blocker, if tolerated
- Screening period to confirm inclusion/exclusion criteria
- Randomized to dapagliflozin 10 mg or placebo once daily plus standard care
Primary endpoint(s): composite of worsening heart failure or CV death
Median follow-up: 18.2 months
|
Dapagliflozin was also very well-tolerated in the DAPA-HF study. The frequency of adverse events related to volume depletion, renal dysfunction, and hypoglycemia did not differ between the dapagliflozin and placebo groups.
Cardiovascular-Related Indications for SGLT-2 Inhibitors
The FDA-approved product labeling for canagliflozin, dapagliflozin, and empagliflozin have been expanded based on the results of the CV outcome trials. With respect to heart failure, the indications for canagliflozin and dapagliflozin include reducing the risk of heart failure hospitalization in selected adults with T2DM. In addition, dapagliflozin is indicated to reduce the risk of cardiovascular death and hospitalization for heart failure in adults with NYHA class II, III or IV HFrEF, irrespective of whether or not they have diabetes.
The SGLT-2is are generally well-tolerated. Adverse events can include genitourinary infection, volume depletion, postural hypotension, acute renal dysfunction, and others. SGLT-2is can be initiated in patients with T2DM who have or are at high risk for cardiovascular disease already on metformin, but who remain above their A1C goal. All 4 SGLT-2is significantly reduce the risk of heart failure hospitalization, with the greatest heart failure benefits demonstrated with dapagliflozin, including patients with or without T2DM.
SUMMARY
Several classes of medications including ACE inhibitors, ARBs, beta-blockers, and MRAs, have demonstrated a mortality benefit in patients with HFrEF, but not HFpEF. Ivabradine and sacubitril/valsartan have been recently approved for HFrEF, providing further opportunities to individualize therapy, improve outcomes, and reduce hospitalizations. Emerging evidence indicates that dapagliflozin has a role in treating patients with HFrEF with or without diabetes. Unfortunately, current evidence demonstrates that the use of approved medications is far from optimal, indicating the need for clinicians, including pharmacists, to work more closely with patients to improve adherence and overall self-management.
REFERENCES
- Virani SS, Alonso A, Benjamin EJ, et al. Heart Disease and Stroke Statistics-2020 Update: A Report From the American Heart Association. Circulation. 2020;141(9):e139-e596.
- Heidenreich PA, Albert NM, Allen LA, et al. Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association. Circ Heart Fail. 2013;6(3):606-619.
- Komanduri S, Jadhao Y, Guduru SS, Cheriyath P, Wert Y. Prevalence and risk factors of heart failure in the USA: NHANES 2013 - 2014 epidemiological follow-up study. J Community Hosp Intern Med Perspect. 2017;7(1):15-20.
- Heo S, Doering LV, Widener J, Moser DK. Predictors and effect of physical symptom status on health-related quality of life in patients with heart failure. Am J Crit Care. 2008;17(2):124-132.
- Lesman-Leegte I, Jaarsma T, Coyne JC, Hillege HL, Van Veldhuisen DJ, Sanderman R. Quality of life and depressive symptoms in the elderly: a comparison between patients with heart failure and age- and gender-matched community controls. J Card Fail. 2009;15(1):17-23.
- Inamdar AA, Inamdar AC. Heart failure: Diagnosis, management and utilization. J Clin Med. 2016;5(7).
- Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;62(16):e147-239.
- Yusuf S, Pitt B, Davis CE, Hood WB, Cohn JN. Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. N Engl J Med. 1991;325(5):293-302.
- Young JB, Dunlap ME, Pfeffer MA, et al. Mortality and morbidity reduction with candesartan in patients with chronic heart failure and left ventricular systolic dysfunction: results of the CHARM low-left ventricular ejection fraction trials. Circulation. 2004;110(17):2618-2626.
- CIBIS-II Investigators and Committees. The Cardiac Insufficiency Bisoprolol Study II (CIBIS-II): a randomised trial. Lancet. 1999;353(9146):9-13.
- MERIT-HF Study Group. Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure (MERIT-HF). Lancet. 1999;353(9169):2001-2007.
- Zannad F, McMurray JJ, Krum H, et al. Eplerenone in patients with systolic heart failure and mild symptoms. N Engl J Med. 2011;364(1):11-21.
- Pitt B, Zannad F, Remme WJ, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. Randomized Aldactone Evaluation Study Investigators. N Engl J Med. 1999;341(10):709-717.
- Packer M, Fowler MB, Roecker EB, et al. Effect of carvedilol on the morbidity of patients with severe chronic heart failure: results of the carvedilol prospective randomized cumulative survival (COPERNICUS) study. Circulation. 2002;106(17):2194-2199.
- McMurray JJ, Packer M, Desai AS, et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014;371(11):993-1004.
- Greene SJ, Butler J, Albert NM, et al. Medical therapy for heart failure with reduced ejection fraction: The CHAMP-HF registry. J Am Coll Cardiol. 2018;72(4):351-366.
- Yancy CW, Januzzi JL, Jr., Allen LA, et al. 2017 ACC Expert Consensus Decision Pathway for Optimization of Heart Failure Treatment: Answers to 10 Pivotal Issues About Heart Failure With Reduced Ejection Fraction: A Report of the American College of Cardiology Task Force on Expert Consensus Decision Pathways. J Am Coll Cardiol. 2018;71(2):201-230.
- Goodlin SJ. Palliative care in congestive heart failure. J Am Coll Cardiol. 2009;54(5):386-396.
- Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation. 2017;136(6):e137-e161.
- Swedberg K, Komajda M, Bohm M, et al. Ivabradine and outcomes in chronic heart failure (SHIFT): a randomised placebo-controlled study. Lancet. 2010;376(9744):875-885.
- Böhm M, Swedberg K, Komajda M, et al. Heart rate as a risk factor in chronic heart failure (SHIFT): the association between heart rate and outcomes in a randomised placebo-controlled trial. Lancet. 2010;376(9744):886-894.
- Thollon C, Cambarrat C, Vian J, Prost JF, Peglion JL, Vilaine JP. Electrophysiological effects of S 16257, a novel sino-atrial node modulator, on rabbit and guinea-pig cardiac preparations: comparison with UL-FS 49. Br J Pharmacol. 1994;112(1):37-42.
- Packer M, McMurray JJ, Desai AS, et al. Angiotensin receptor neprilysin inhibition compared with enalapril on the risk of clinical progression in surviving patients with heart failure. Circulation. 2015;131(1):54-61.
- Velazquez EJ, Morrow DA, DeVore AD, et al. Angiotensin-neprilysin inhibition in acute decompensated heart failure. N Engl J Med. 2019;380(6):539-548.
- He J, Ogden LG, Bazzano LA, Vupputuri S, Loria C, Whelton PK. Risk factors for congestive heart failure in US men and women: NHANES I epidemiologic follow-up study. Arch Intern Med. 2001;161(7):996-1002.
- Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2018;71(19):e127-e248.
- Kannel WB, Hjortland M, Castelli WP. Role of diabetes in congestive heart failure: the Framingham study. Am J Cardiol. 1974;34(1):29-34.
- Dei Cas A, Khan SS, Butler J, et al. Impact of diabetes on epidemiology, treatment, and outcomes of patients with heart failure. JACC Heart Fail. 2015;3(2):136-145.
- American Diabetes Association. 10. Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes-2020. Diabetes Care. 2020;43(Suppl 1):S111-S134.
- American Diabetes Association. 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes-2020. Diabetes Care. 2020;43(Suppl 1):S98-S110.
- Neal B, Perkovic V, Mahaffey KW, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med. 2017;377(7):644-657.
- Wiviott SD, Raz I, Bonaca MP, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2019;380(4):347-357.
- Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373(22):2117-2128.
- Caffrey M. VERTIS CV: Ertugliflozin falls short of SGLT2s on CV outcomes, despite promise in heart failure. Published June 16, 2020. https://www.ajmc.com/conferences/ada-2020/vertis-cv-ertugliflozin-falls-short-of-sglt2s-on-cv-outcomes-despite-promise-in-heart-failure. Accessed July 24, 2020.
- Figtree GA, Radholm K, Barrett TD, et al. Effects of canagliflozin on heart failure outcomes associated with preserved and reduced ejection fraction in type 2 diabetes mellitus. Circulation. 2019;139(22):2591-2593.
- Fitchett D, Inzucchi SE, Cannon CP, et al. Empagliflozin reduced mortality and hospitalization for heart failure across the spectrum of cardiovascular risk in the EMPA-REG OUTCOME trial. Circulation. 2019;139(11):1384-1395.
- Wanner C, Lachin JM, Inzucchi SE, et al. Empagliflozin and clinical outcomes in patients with type 2 diabetes mellitus, established cardiovascular disease, and chronic kidney disease. Circulation. 2018;137(2):119-129.
- McMurray JJV, Solomon SD, Inzucchi SE, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019;381(21):1995-2008.
- Cannon CP, McGuire DK, Pratley R, et al. Design and baseline characteristics of the eValuation of ERTugliflozin effIcacy and Safety CardioVascular outcomes trial (VERTIS-CV). Am Heart J. 2018;206:11-23.
Back to Top