ADVERTISEMENT

Team-Based Approaches to Help Older Adults With Type 2 Diabetes Achieve Individualized Glycemic Goals
Introduction
The prevalence of type 2 diabetes mellitus (T2DM) has reached an epidemic level and continues to rise. The American Diabetes Association (ADA) estimates that 29.1 million people, approximately 9.3% of the US population, have diabetes.1 In the older adult population, the prevalence of diabetes is even higher. Approximately 26% of adults over age 65 in the United States (11.2 million people) have diabetes.1
A variety of factors associated with aging contribute to an increased risk of T2DM for older adults. Pathophysiologic changes, age-related decreased insulin secretion, age-related decreases in beta cell function, insulin resistance, and genetics all play a role. This population is generally more prone to hypoglycemia and other adverse events related to drug therapy and, due to numerous barriers, older adults with T2DM often do not achieve recommended goals for glycemic control.2 Many of these individuals, therefore, are experiencing negative health consequences from T2DM that could be prevented or improved with optimal evidence-based care.
Part I: Special Considerations for Older Adults
The ADA recommendations point out that depression is highly prevalent among older adult patients and should always be assessed. An undiagnosed or untreated depression can have a negative impact on self-care behaviors for these patients.3,4 The geriatric syndromes listed below should also be considered.5
Geriatric syndromes to consider when treating diabetes in older adults:
- Polypharmacy
- Cognitive impairment
- Urinary incontinence
- Injurious fall and fractures
- Pain
- Vision and hearing impairments
Physiology must be considered when treating T2DM in older individuals, because they often exhibit postprandial hyperglycemia due to impaired prandial insulin secretion. Postprandial spikes should never be ignored. If fasting blood glucose or A1c are the only screening criteria, it is possible to miss up to a third of individuals who have T2DM.3 The increased risk of hypoglycemia in older adults must also be considered. This is brought about, in part, by age-related pharmacokinetic and pharmacodynamic changes. Renal function can affect dosing of medications and adverse event management; patients with severe hypoglycemia are also at increased risk of dementia.6
To engage the patient as a member of the health care team, clinicians need to have some idea of the patient’s self-management skills and any competing priorities. Clinicians also need to include family members and other caregivers to determine what the patient’s priorities are. This means achieving stringent blood glucose control throughout the day might not be as high a priority for an older adult as maintaining flexible meal times. It is important to know what is important to the patient. Engaging colleagues such as dietitians can be particularly beneficial. A patient’s overall level of care can often be improved through meal planning and improved nutrition.
Hyperglycemia and hypoglycemia can both affect cognition.4,7 Cross-sectional studies have shown an increased prevalence of cognitive impairment and dementia, with up to a 2-fold increase versus age-matched controls without diabetes.5 Diabetes places people at increased risk for cognitive impairment and T2DM is certainly a risk factor for cerebrovascular disease and vascular-related dementia.5
In a sub-study of the ACCORD trial, called the ACCORD-MIND trial, investigators studied the relationship between A1c at baseline and performance on several cognitive tests. There were almost 3,000 individuals in the study. Investigators found that a 1% higher A1c was significantly associated with worse performance on a variety of cognitive function tests.8
| Table 1: Hypoglycemia and Risk of Incident Dementia4 |
| Hypoglycemia Episodes |
Hazard Ratio |
95% CI |
| None |
1.00 |
|
| 1 |
1.26 |
1.10 – 1.49 |
| 2 |
1.80 |
1.37 – 2.36 |
| 3 or more |
1.94 |
1.42 – 2.64 |
Hypoglycemia can also have negative effects on cognition. This was the focus of a study in more
than 16,000 individuals who were followed from 1980 to about 2002, looking at severe
hypoglycemic events requiring emergency services or hospitalization.6 Individuals who did not
have a hypoglycemic episode composed the reference cohort in this Cox proportional hazard
analysis. As seen in the table above, the more severe hypoglycemic events these individuals had,
the more their hazard ratio increased, up to an almost 2-fold risk of any form of dementia.
As shown in Figure 1 below, a one-size-fits-all approach is not appropriate for many individuals when assessing treatment targets, and that includes people who are less motivated, potentially non-adherent, or who may have poor self-care capacities.
Figure 1. Glycemic Targets: One Size Does Not Fit All
 |
Team-based medical care in T2DM is absolutely important. Engaging our health care team as a whole to help achieve individualized goals means engaging dietitian colleagues, case manager colleagues, and other members of the health care team to meet patient-centered treatment goals. Patient-centered medical homes have been studied as a means to coordinate patient care, with demonstration projects involving patients with T2DM showing benefits such as cost savings, improved achievement of self-management goals, reduced hospitalization rates, and improved monitoring for T2DM-related complications. Of course, in this model, patients play an important part in their own care as well. Pioneer accountable care organizations, likewise, have shown improvement in outcomes, including reduced readmission rates and increased rates of achieving blood pressure goals, as well as cholesterol targets.9 Not all of the pioneer accountable care organization projects resulted in cost savings, but the majority have.
In summary, consensus recommendations3 include the following:
- Screen older adults periodically for cognitive function, functional status, and fall risk.
- Assess patients regularly for hyperglycemia.
- Assess the burden of treatment on patients and caregivers.
- Keep recommendations in line with patient priorities.
- Choose antihyperglycemic therapies carefully.
- Individualize goals and reassess goals frequently.
Part II. Treatment Choices and Goals
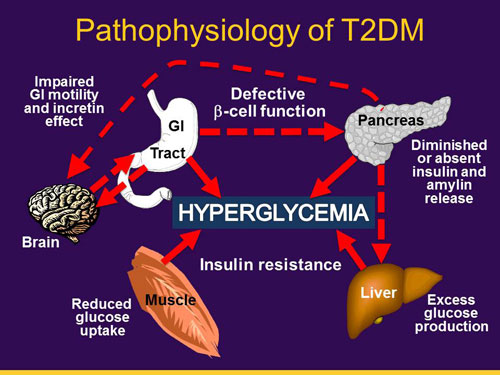
T2DM is a complex disorder whose pathophysiology involves pancreatic beta cell dysfunction along with insulin resistance. In addition to the pancreas, there is a connection between several pathophysiologic disturbances at the level of the gut, the brain, the liver, and the muscles in terms of regulating the secretion of insulin and glucagon as well as glucose uptake. Current therapies are directed at several of these pathophysiologic disturbances. (See Figure 2)
Figure 2. Pathophysiology of T2DMl
 |
Of course nonpharmacological approaches are critically important too, especially appropriate intake of carbohydrates as well as regular physical activity to stimulate muscle uptake of glucose. However, older adults may have more difficulty engaging in these behaviors due to loss of access to good food. Poor dietary habits may be firmly established and hard to change at an older age. Physical activity may be more difficult due to comorbidities and an established, sedentary lifestyle. In addition to lifestyle changes, pharmacological agents must also be considered.
In the late 1980s, only 2 general classes of agents were approved in the United States: insulin and sulfonylureas. During the past 20 years we have seen an explosion in the number of drugs, as well as entirely new classes of drugs.
Metformin, introduced in the mid-1990s, continues to be our workhorse. Others include alpha-glucosidase inhibitors and insulin analogs. Meglitanides were introduced in the late 1990s and have largely fallen out of favor. Sulfonylureas, introduced in the 1950s, are also falling out of favor. The thiazolidinediones (TZDs) were introduced in 1999 and became very widely used but are now declining in frequency of use for many reasons.
Agents introduced since 2000 are listed below. The last 3 classes of agents listed have been “game-changers” in the past 5 to 6 years. These all seem to be growing in popularity as clinicians learn more about their therapeutic applications.
Pharmacologic agents available after 2000:
- Amylin analogs (pramlintide)
- Bile acid sequestrants (colesevalem)
- Dopamine antagonists (bromocriptine)
- DPP-4 inhibitors
- GLP-1 receptor agonists
- SGLT-2 inhibitors
Treatment selection is becoming more challenging with the proliferation of treatment options. Metformin continues to be favored due to its proven track record. It’s well tolerated, relatively low cost, and can be combined with a wide variety of other agents. Most patients will eventually require a second agent, however. Factors to consider when deciding which agents to add to a patient’s regimen include, first and foremost, the patient’s glycemic control. This includes consideration of A1c levels, fasting blood glucose and postprandial blood glucose, and the patient’s risk for hypoglycemia. An A1c level above 10% will rule out certain possibilities. Also, some agents are better at lowering fasting blood glucose while others are far better at lowering postprandial blood glucose.
Other factors to consider include:
- Body mass index/obesity
- Renal function
- Cardiovascular disease and risk of heart failure
- Blood pressure
- Serum lipids
Figure 3. Action of Antidiabetic Agents
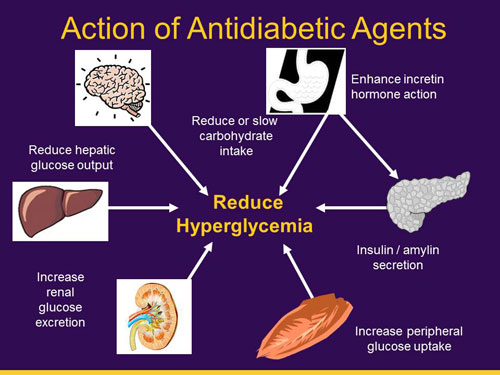 |
Agents that address postprandial blood glucose exert effects on the gut and the brain. They reduce appetite and stimulate release of incretin hormones, or reduce absorption of carbohydrates from the gut. This is what it means to have postprandial glucose as a primary target. By contrast, fasting blood glucose relates to basal insulin release, glucose production in the liver, muscle uptake of glucose, and glucose excretion from the kidneys. Most agents that address those issues have a greater effect on fasting blood glucose. None of these agents limit their effects entirely to one target or the other. They all have an effect on both. The biggest bang for the buck comes by combining one drug that targets postprandial with one that targets fasting, in terms of lowering blood glucose and overall A1c levels.
Many adults also have cardiovascular comorbidities, so we may wish to consider compounds
that reduce cardiovascular risk. Unfortunately, data are limited in this regard. Most drugs used
for T2DM have not been adequately studied to determine their long-term impact on
cardiovascular disease (CVD). Renal function is another factor to consider, since many
compounds are eliminated via the kidneys. Dose reductions may be necessary in patients who
have compromised renal function.
Older adults are an at-risk population for hypoglycemia for a number of reasons.10 For example,
older adults are sometimes overtreated in an effort to achieve tight glycemic control. As people
age, eating habits change and they may lose weight. With aggressive treatment the A1c may fall
as low as 5.5%, but this should be avoided. The risk for severe hypoglycemia is greatly increased.
They are also at great risk of hypoglycemia unawareness due to repeatedly low and very low
levels of blood glucose. They become accustomed to this state, physiologically, so they miss all
warning signs until suddenly they become comatose. Autonomic neuropathy is another risk
factor for developing hypoglycemia and hypoglycemic unawareness. This diabetes-related
complication is far more common in older adults.10
Figure 4. Hypoglycemic Risk of Antihyperglycemic Agents Added to Metformin
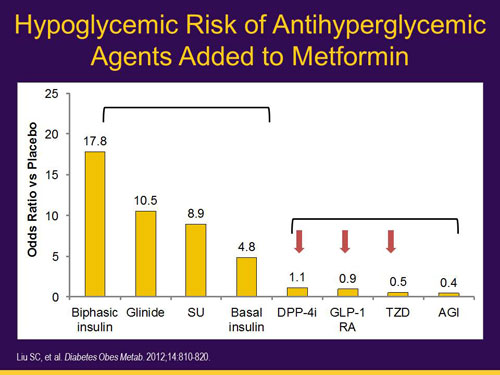 |
Hypoglycemic risk can be mitigated by drug choices. Metformin is often used at baseline and carries a negligible risk for hypoglycemia. Risk increases with various metformin combinations. Greatest risk derives from insulin, especially prandial insulin combined with basal insulin, sometimes called basal-bolus insulin treatment. The meglitinides and sulfonylureas also carry a fairly high risk for hypoglycemia; however, often the hypoglycemia associated with meglitinides is transient and mild. The risk of hypoglycemia associated with some sulfonylureas can be substantial. Sulfonylureas with prolonged half-lives and that are renally eliminated—such as glyburide or chlorpropamide—should be avoided in older adults.
Newer agents, including DPP-4 inhibitors, GLP1 receptor agonists, TZDs, and alpha-glucosidase inhibitors, are all associated with far less risk of developing hypoglycemia.9 For this reason they would be favored in older adults for achieving glycemic goals.
Figure 5. Hypoglycemia With Glyburide
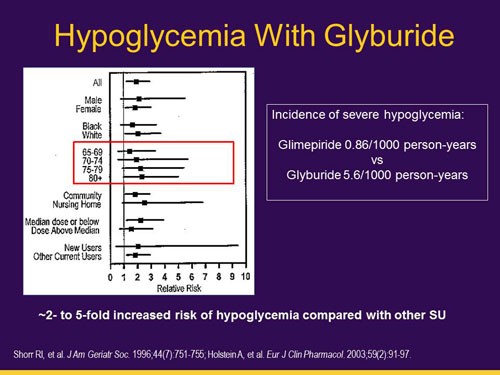 |
Glyburide should not be used in older adults. As can be seen in Figure 6, glyburide has a 5-fold
increase in risk for hypoglycemia compared to glimepiride.
Figure 6. DPP-4 Inhibitors
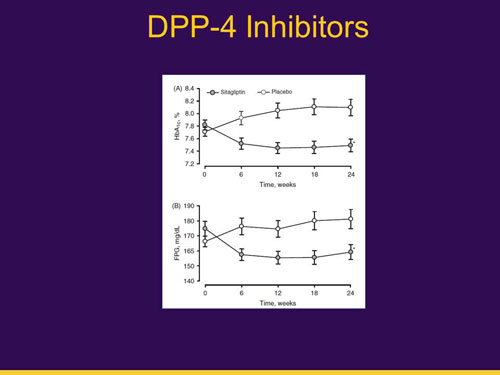 |
DPP-4 inhibitors are an option and their use has seen a remarkable increase in the past 5 years, due to their low risk of hypoglycemia and their simplicity of administration. They can be used in people with various levels of renal function, including patients with end-stage renal disease (ESRD). Figure 6 shows their effectiveness versus placebo, at both reducing A1c levels and fasting plasma glucose. As a class, these agents have a favorable adverse event (AE) profile. Overall, AEs and serious AEs were similar in both arms of the study.12 Long-term effects, including an increased risk of heart failure, are under investigation. In the short term, these agents are very well tolerated.
Figure 7. GLP-1 Receptor Agonists
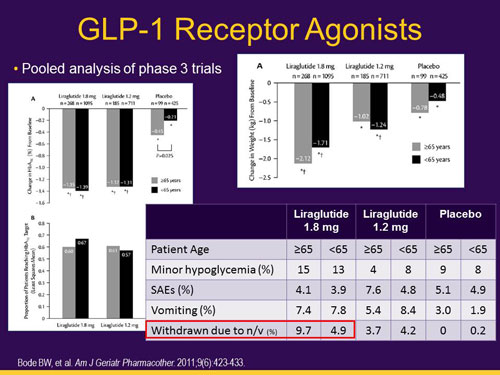 |
The glucagon-like peptide-1 (GLP-1) receptor agonists are a second form of incretin-based
therapy. These agents are injectable and they bind to the GLP-1 receptor, also known as the
incretin receptor, in the pancreas. They are more powerful than the DPP-4 inhibitors, so their
capacity to lower blood glucose levels is twice as great. However, they carry no more risk of
hypoglycemia. They can induce significant weight loss, which is a major benefit. Some patients
cannot tolerate the nausea and vomiting these agents can cause.13
The newest agents are the SGLT-2 inhibitors. This class of agents causes glucose wasting
through the kidneys. Their effectiveness in older adults seems to be somewhat less than in
younger adults. For older adults, the glucose lowering is in the 0.4% to 0.5% range, as compared
to 1.0 to 1.5% for GLP-1 receptor agonists. SGLT-2 inhibitors are very similar to DPP-4 inhibitors
in terms of their ability to lower A1c. Significant weight loss, in the range of 1 to 2 kilograms,
has also been observed. Hypoglycemia risk is negligible; however, they do carry an increased
risk of genitourinary tract infections in both men and women. SGLT-2 inhibitors also cause an
osmotic diuresis, and this can cause some older adults to become hypotensive and dizzy.14
| Table 2. Glycemic Goals for Older Adults |
| Organization/Guideline |
A1c Target |
| American Geriatrics Society |
7.5%-8.0% 7.0%-7.5% 8.0%-9.0% |
General
Healthy/few comorbidities
Comorbidities/poor health |
| American Diabetes Association |
<7.5% <8.0% <8.5% |
Healthy
Complex/intermediate
Very complex/poor health |
| International Diabetes Federation |
7.0%-7.5% 7.5%-8.0% |
Functionally independent
Functionally dependent |
When it comes to setting glycemic targets for older adults, standards vary from one organization to the next. As shown in the table above, the American Geriatrics Society (AGS) has the most liberal goals, compared to other organizations. The AGS guidelines state that an older adult with poor health and significant comorbidities should have an A1c goal of between 8% and 9%.15 Such lenient glycemic goals would have been heresy 10 years ago, but recent data indicate that older adults with multiple comorbidities are unlikely to benefit from aggressive treatment and may be harmed.
Figure 8. Framework to Assist in Determining Glycemic Targets
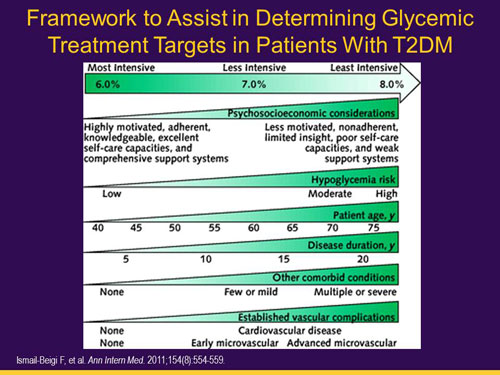 |
Treatment goals can be more intense for some patients than for others. Intense treatment is
most appropriate for patients who are highly motivated; have good adherence to medications,
blood glucose monitoring, and medical appointments; excellent capacity for self-care; low risk
of hypoglycemia; age in the 40s or 50s; have only recently been diagnosed; and have few
comorbidities. They might have high blood pressure with dyslipidemia, but they have no end
organ damage and no established cardiovascular disease. These are the kinds of patients with
whom we should be trying to achieve normal or near-normal targets. At the other end of the
spectrum are patients with poor self-care behaviors or those who are much older, who have
had diabetes for decades, and who have many comorbidities. In these patients, an A1c target of
8% to 9% is perfectly acceptable.16
In summary:
- Diabetes is very common in older adults but this patient population is very heterogeneous.
- Glycemic targets need to consider several factors including age, health status, life expectancy, cognition, and risk of hypoglycemia.
- Available choices to treat diabetes have doubled in the past 10 years making therapeutic decision making more challenging.
- Newer agents offer some advantages, but at a higher cost; and long-term benefits and adverse effects are not yet fully understood.
- Hypoglycemia, weight gain, and cardiovascular complications are all issues we must consider when developing the therapeutic plan.
Part III. Case Studies
Clinical Case #1
Mrs. T is an 84-year-old retired waitress. She presents to a pharmacotherapy clinic for follow-up of T2DM of 21 years’ duration. She is upset that her A1c is not <7.0%. Mrs. T lives alone in an assisted living facility; she self-manages her diabetes, but can request help from staff if needed.
She tests her blood glucose (BG) once daily in the morning before breakfast. She reports several hypoglycemic events recently, but does not report hypoglycemic symptoms until her BG is <60 mg/dL. The patient denies shortness of breath or chest pain with exertion. Pedal pulses are intact. A foot exam shows absence of sensation to 10-g monofilament.
PMH: T2DM, osteoporosis, dyslipidemia, HTN, depression, hospitalization following severe hypoglycemic event 4 months ago
Current Medications:
- Glyburide/metformin 2.5/500 mg BID
- Simvastatin 20 mg QHS
- Lisinopril 20 mg QAM
- HCTZ 12.5mg QAM
- Ibuprofen 200 mg PRN
- ASA 81 mg QD
Allergies: No known drug allergies
Vital Signs:
- BP: 124/68 mmHg (seated)
- Pulse: 72; Resp: 14
- Height: 5'5"
- Weight: 184 lbs
- BMI: 30.6
Recent Labs:
| Na |
138 mg/dL |
K |
4.7 mg/dL |
Total Chol |
153 mg/dL |
| Cl |
98 mg/dL |
CO2 |
37 mg/dL |
HDL |
34 mg/dL |
| SCr |
1.5 mg/dL |
TSH |
0.96 mIU/L |
LDL |
86 mg/dL |
| BUN |
20 mg/dL |
ALT |
28 U/L |
TG |
140 mg/dL |
| eGFR |
35 mL/ min/1.73 m2 |
AST |
26 U/L |
A1c |
7.5% |
| eCrCl* |
36 mL/min |
|
|
Gluc |
97 mg/dL |
| *eCrCl calculated using Cockcroft-Gault formula and lean body weight |
Laboratory Reference Ranges:
| Electrolytes |
Blood Gases |
| Calcium |
8.8-10.3 mg/dL |
CO2 |
35-45 mg/dL (arterial), 38-52 (venous) |
| Chloride |
95-107 mEq/L |
BUN |
7-20 mg/dL |
| Potassium |
3.5-5.2 mEq/L |
Lipoproteins and Triglycerides |
| Sodium |
135-147 mEq/L |
Total cholesterol |
<200 mg/dL |
| |
|
HDL cholesterol |
30-70 mg/dL |
| Creatinine |
0.5-1.4 mg/dL |
LDL cholesterol |
65-180 mg/dL |
| eGFR |
>90 mL/min/1.73 m2 |
Triglycerides |
45-155 mg/dL (<160) |
| |
|
|
|
| Glucose, fasting |
60-110 mg/dL |
SGOT (AST) |
<35 IU/L (20-48) |
| Glucose, 2 hours postprandial |
≤140 mg/dL |
SGPT (ALT) |
<35 IU/L |
| Hemoglobin A1c |
<5.9% |
Thyroid Function |
| |
|
TSH |
0.25-4.30 microunits/mL |
Recent Blood Glucose Log:
Date |
Glucose (mg/dL) |
Time |
10-16 |
83 |
6:15 AM |
10-17 |
111 |
7:00 AM |
10-18 |
68 |
8:32 AM |
10-19 |
92 |
7:11 AM |
10-20 |
63 |
9:15 AM |
10-21 |
88 |
7:05 AM |
10-22 |
103 |
6:10 AM |
10-23 |
72 |
7:55 AM |
10-24 |
69 |
8:40 AM |
10-25 |
95 |
7:20 AM |
Discussion Questions
- What changes, if any, would you recommend for Mrs. T’s current antihyperglycemic therapy?
- Which of the following would/would not be a good treatment option for Mrs. T? Explain why.
- SGLT-2 inhibitor
- TZD
- DPP-4 inhibitor
- GLP-1 receptor agonist
- Basal insulin
Interactive Case Discussion (Excerpts Edited for Clarity)
Neumiller: What do you think about her current treatment regimen for diabetes?
Speaker: She’s taking glyburide, which caused that hypoglycemia, so you have to eliminate the glyburide.
Neumiller: I think most all of us would agree that glyburide is not a good agent for this particular individual, especially given her kidney function and the fact that glyburide has active metabolites.
Now let’s talk about other possible changes to therapy. What about the metformin? Here’s a slide to guide our discussion.
Figure 9. Metformin and Renal Impairment
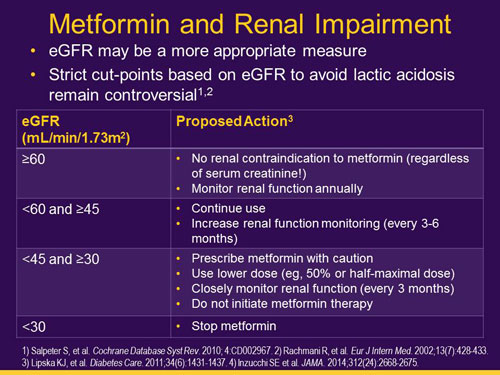 |
Speaker: I believe there’s something in the literature that talks about age and metformin, specifically that it should be used with extreme caution with those over the age of 80. So between the fact that the patient’s over 80 and the patient has a GFR of about, was it 34-36? We would be very, very cautious about continuing metformin for this patient.
Haines: Thank you. This raises the question: What’s the right dose? And should we discontinue it? This is an area of evolving science. Some practitioners will strictly avoid it because in the FDA approved labeling it’s contraindicated in men when the serum creatinine is above 1.5 mg/dL and above 1.4 mg/dL in women. That’s a potential legal liability if the patient develops lactic acidosis. Others would feel more confident about using metformin if the estimated creatinine clearance or glomerular filtration rate (GFR) is above 30 ml/min. As long as the family and the patient are aware of what the potential risks are and we’re monitoring renal function every 2 to 3 months, I would continue metformin in this case. But I’d recommend a dose no higher than 1000 mg per day.
Speaker: Can I just make a point?
Neumiller: Yes, please.
Speaker: Mrs. T is on hydrochlorothiazide and her blood pressure is nice and low. Maybe if you just took away the hydrochlorothiazide, the renal function would improve and she could stay on the metformin because we know it’s a good drug. That would be one thing I’d look at.
Neumiller: Thank you, that is definitely something to consider when evaluating the regimen in its entirety.
Speaker: And the ibuprofen. Don’t use it.
Neumiller: Yes, ibuprofen is not a good choice for her, most certainly. That would definitely be something to counsel her about and discuss alternatives for pain relief, if needed.
Haines: That point is really well taken because we want to look at things comprehensively. We want to look at the entire regimen and examine things that could be impacting her renal function. We want to keep her on metformin, so let’s look at other ways that we can address this. That’s an excellent point.
Neumiller: Let’s go to Question 2. Which of the choices listed would or would not be a good treatment option? Any reasons you would or would not use SGLT-2 inhibitors in this patient?
Speaker: I’m concerned about her kidneys.
Neumiller: Absolutely, adequate renal function is required for efficacy with these agents. Also, Dr. Haines talked about some safety considerations related to SGLT-2 inhibitors, so I wouldn’t start with an SGLT-2 inhibitor in this individual. What about TZDs? Would anybody start a TZD for her? She has osteoporosis, so it may be best to avoid a TZD in this case as to not contribute to fracture risk. She also has decreased kidney function, and the addition of a TZD to her regimen could contribute to some fluid retention as well. What about a DPP-4 inhibitor? One thing we might want to look at is additional detail as related to her blood glucose profile and trends. We only have information about her fasting blood sugars. We talked about discontinuing the glyburide, so it may also be worth taking a step back after we discontinue the sulfonylurea and see what her needs are from there. What about a GLP-1 receptor agonist? Okay, I see a raised hand. Why would you go with that?
Speaker: She’s a little heavy for her height and it probably wouldn’t hurt her, and I think it’s a safe product.
Neumiller: Okay. It is an option, but as Dr. Haines mentioned, you have to be cautious. There have been some postmarketing reports of acute renal failure with the use of these medications. Older adults with impaired kidney function tend to have more tolerability issues related to GLP-1 receptor agonist therapies, but they can be used with appropriate monitoring. It would be important to be in close communication with Mrs. T during the initiation phase to monitor her for tolerability. Is there anybody who would go with basal insulin? No takers? Okay. I think the group agrees that Mrs. T is not the best candidate for starting insulin given her hypoglycemia risk.
Haines: Yes, especially with an A1c at 7.5 and a history of severe hypoglycemia, I wouldn’t be considering insulin in this patient.
Speaker: I have a comment. I’m not a pharmacist but I am a registered dietitian, and I have participated in lots of team rounds on patients. Mrs. T has early morning hypoglycemic episodes. Get the dietitian in there and figure out what she’s eating for supper and then add a snack with at least 2 ounces of protein and some fat and things like that. All the comments up to now have been about throwing in another medicine or taking one away. Let’s look a bit more closely at lifestyle changes.
Haines: Your comment is spot on. That’s one of the reasons we call this a team approach, because we pharmacists focus on the meds. That’s our bailiwick and what we bring to the team. But we all recognize our knowledge and skills are limited, and that’s why we have to work with team members to bring a different skill set and different expertise. Thank you very much for your comment.
Clinical Case #2
Mr. K is a 74-year-old retired postal worker. He presents for routine follow-up of T2DM of 10 years’ duration. Mr. K lives independently with his wife, who assists with medication taking and blood glucose monitoring. He appears healthy, in no acute distress. He tests his blood glucose (BG) 1 to 3 times a week. His log book is shown below. He denies hypoglycemia symptoms. He also denies shortness of breath or chest pain with exertion. On examination he shows diminished pedal pulses; a foot exam shows loss of sensation to 10-g monofilament.
PMH: T2DM, history of left coronary artery stent placed 3 years ago, dyslipidemia, HTN, osteoarthritis (hands and hips)
Current Medications:
- Sitagliptin 100 mg QAM
- Atorvastatin 40 mg QHS
- Irbesartan 300 mg QHS
- Chlorthalidone 12.5mg QAM
- ASA 81 mg QD
- Acetaminophen 650 mg TID
Allergies: No known drug allergies
Vital signs:
- BP: 138/76 mmHg (seated)
- Pulse: 68; Resp: 12
- Height: 5'10"
- Weight: 242 lbs
- BMI: 34.7
Recent Labs:
| Na |
140 mg/dL |
K |
4.9 mg/dL |
Total Chol |
166 mg/dL |
| Cl |
100 mg/dL |
CO2 |
39 mg/dL |
HDL |
44 mg/dL |
| SCr |
1.7 mg/dL |
TSH |
1.92 mIU/L |
LDL |
64 mg/dL |
| BUN |
17 mg/dL |
ALT |
24 U/L |
TG |
188 mg/dL |
| eGFR |
56 mL/ min/1.73 m2 |
AST |
19 U/L |
A1c |
8.6% |
| eCrCl* |
36 mL/min |
|
|
Gluc |
139 mg/dL |
| *eCrCl calculated using Cockcroft-Gault formula and lean body weight |
Recent Blood Glucose Log:
Date |
Glucose (mg/dL) |
Time |
9-24 |
131 |
7:21 AM |
9-27 |
107 |
7:32 AM |
9-30 |
124 |
7:48 AM |
10-6 |
166 |
8:12 AM |
10-7 |
109 |
7:24 AM |
10-10 |
152 |
8:24 AM |
10-13 |
179 |
6:58 AM |
10-15 |
129 |
7:15 AM |
10-21 |
160 |
8:22 AM |
10-25 |
151 |
8:10 AM |
Discussion Questions
- How frequently should this patient measure his blood glucose?
- What changes would you recommend for antihyperglycemic therapy?
- What action, if any, would you take with sitagliptin?
Interactive Case Discussion (Excerpts Edited for Clarity)
Haines: How frequently should the patient test his blood glucose? I’m going to burst all your bubbles. With the medication he’s on, this patient does not need to routinely monitor his blood glucose. There’s no evidence that self-monitored blood glucose when you’re on an oral agent at low risk for hypoglycemia has any benefit.
Speaker: So for this patient I’d like to do it 2 to 3 times a day because his A1c is above goal, to try and figure out where the discrepancies are, to help with selecting future treatments. So do you think it’s not even appropriate in that type of setting?
Haines: You make an excellent point. If you’re doing it for a short period of time, meaning for 1 week, to measure postprandial blood glucose, that’s an excellent thing to do. But in that case you’re doing it for diagnostic purposes, not routine monitoring.
Haines: Next question. Which changes would you recommend and why? I see no one recommended just lifestyle changes—this gentleman’s A1c is quite high at 8.6 and his fasting blood glucose readings are frequently above 120 mg/dL. How about adding a long-acting insulin—such as NPH insulin, insulin glargine, or insulin detemir—at bedtime? This would be a very common choice in practice, and it is a recommended option in the ADA guidelines for a patient like this. What about the sitagliptin? How many people would get rid of it? And why?
Speaker: It’s cleared renally, and it’s already not reducing A1c to the target you want. The only reason to adjust the dose of this medicine is because of renal issues. The dose is at 100 mg now, renal function is suboptimal, so it’s just a poor choice. Reducing the dose isn’t going to help him.
Haines: Yes, reducing the sitagliptin dose is not going to help the A1c. So discontinuing it is certainly an option. I’d make the assumption that sitagliptin is having some effect; otherwise, his A1c might be 9% or 9.5%. So, I probably would continue it but at a lower dose; but switching to something else is certainly appropriate, too.
Conclusion
Many older adults with T2DM are experiencing negative health consequences from T2DM that could be prevented or improved with optimal evidence-based care. Senior care pharmacists have the opportunity to improve T2DM outcomes in older adults by participating in team-based care and following a chronic care model for older adults with T2DM, promoting appropriate individualized glycemic goals for older adults with T2DM, and helping older adults with T2DM achieve blood glucose targets while balancing the benefits and risks of therapies.
References
- National Diabetes Education Program Website. The facts about diabetes: a leading cause of death in the U.S. http://www.cdc.gov/diabetes/pubs/statsreport14/national-diabetes-report-web.pdf. Accessed April 14, 2015.
- Ali MK, Bullard KM, Saaddine JB, Cowie CC, Imperatore G, Gregg EW. Achievement of goals in U.S. diabetes care, 1999-2010. N Engl J Med. 2013;368(17):1613-1624.
- American Diabetes Association. Diabetes Care. 2015;38:S1-S93.
- Travis SS, Buchanan RJ, Wang S, Kim M. Analyses of nursing home residents with diabetes at admission. J Am Med Dir Assoc. 2004;5(5):320-327.
- Kirkman MS, Briscoe VJ, Clark N, et al. Diabetes in older adults. Diabetes Care. 2012;35(12):2650-2664.
- Whitmer RA, Karter AJ, Yaffe K, Quesenberry CP, Selby JV. Hypoglycemic episodes and risk of dementia in older patients with type 2 diabetes mellitus. JAMA. 2009;301(15):1565-1572.
- Cukierman T, Gerstein HC, Williamson JD. Cognitive decline and dementia in diabetes—systematic overview of prospective observational studies. Diabetologia. 2005;48(12):2460-2469.
- Cukierman-Yaffe T, Gerstein HC, Williamson JD, et al. Relationship between baseline glycemic control and cognitive function in individuals with type 2 diabetes and other cardiovascular risk factors: the action to control cardiovascular risk in diabetes-memory in diabetes (ACCORD-MIND) trial. Diabetes Care. 2009;32(2):221-226.
- Tuttle KR, Bakris GL, Bilous RW, et al. Diabetic kidney disease: a report from an ADA Consensus Conference. Diabetes Care. 2014;37(10):2864-2883.
- Neumiller JJ, Setter SM. Pharmacologic management of the older patient with type 2 diabetes mellitus. Am J Geriatr Pharmacother. 2009;7(6):324-342.
- Liu SC, Tu YK, Chien MN, Chien KL. Effect of antidiabetic agents added to metformin on glycaemic control, hypoglycaemia and weight change in patients with type 2 diabetes: a network meta-analysis. Diabetes Obes Metab. 2012;14(9):810-820.
- Barzilai N, Guo H, Mahoney EM, et al. Efficacy and tolerability of sitagliptin monotherapy in elderly patients with type 2 diabetes: a randomized, double-blind, placebo-controlled trial. Curr Med Res Opin. 2011;27(5):1049-1058.
- Bode BW, Brett J, Falahati A, Pratley RE. Comparison of the efficacy and tolerability profile of liraglutide, a once-daily human GLP-1 analog, in patients with type 2 diabetes ≥65 and <65 years of age: a pooled analysis from phase III studies. Am J Geriatr Pharmacother. 2011;9(6):423-433.
- Mikhail N. Use of sodium-glucose cotransporter type 2 inhibitors in older adults with type 2 diabetes mellitus. South Med J. 2015;108(2):91-96.
- American Geriatrics Society. Guidelines abstracted from the American Geriatrics Society Guidelines for Improving Care for Older Adults with Diabetes Mellitus: 2013 Update. JAGS. 2013;61:2020-2026.
- Ismail-beigi F, Moghissi E, Tiktin M, Hirsch IB, Inzucchi SE, Genuth S. Individualizing glycemic targets in type 2 diabetes mellitus: implications of recent clinical trials. Ann Intern Med. 2011;154(8):554-559.
Back to Top