
Expired activity
Please go to the PowerPak
homepage and select a course.
COVID-19 Quarterly Update on All Things Viral: Vaccinations and Treatments for the Winter Respiratory Viruses
INTRODUCTION
Testing is down and travel is up as Americans enjoy their first near-normal holiday season since the identification of the severe acute respiratory syndrome 2 coronavirus (SARS-CoV2) in 2020. That means the potential for spreading this and other respiratory viruses is increased, but without testing, we may never know the cause of many of the resulting infections.
Quest Diagnostics, a leading provider of SARS-CoV-2 testing, reported in August 2023 that overall testing for coronavirus disease 2019 (COVID-19) was down nearly 90%. More recent data (early December 2023) from the Centers for Disease Control and Prevention (CDC) COVID Data Tracker indicates little to no change in SARS-CoV-2 test positivity or deaths. Still, emergency department visits and hospitalizations were climbing by about 10% week-over-week. The most common variant was the omicron subvariant HV.1 followed by JN.1 and EG.5.
Influenza overall incidence began to climb in November, according to CDC data. Several Southern states and California reported high or very high activity levels of influenza-like illness in November, and by December, the virus was spreading across the country (Figure 1).
As we transition to endemic management of SARS-CoV-2 as a seasonal illness, we must continue to evaluate optimal ways to both prevent COVID-19 disease through vaccination as well as test for probable cases and treat confirmed cases with safe and effective therapeutic agents for both ambulatory patients with mild-to-moderate COVID-19 and those hospitalized with severe disease. Incorporating COVID-19 vaccination into the successful pharmacy-based programs for influenza vaccination is a focus in this article, and information is provided on the new vaccines for preventing respiratory syncytial virus (RSV).
| Figure 1. U.S. Influenza-Like Illness (ILI) Levels for the Week Ending December 2, 2023 |
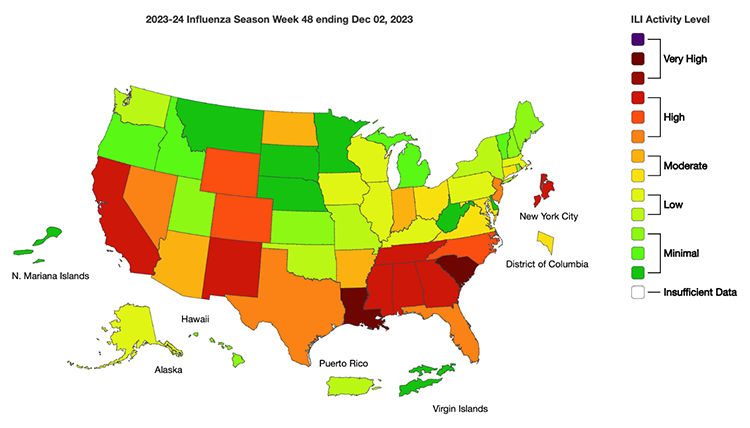 |
| Source: U.S. Centers for Disease Control and Prevention, https://www.cdc.gov/flu/weekly/index.htm |
CDC, FDA, AND ACIP AGREE ON MONOVALENT COVID-19 VACCINE
Despite differences of opinion earlier in the year, the Food and Drug Administration (FDA) and the CDC’s Advisory Committee on Immunization Practices (ACIP) agreed on a monovalent approach for this season’s COVID-19 vaccines. First, the FDA voted to approve and authorize the emergency use of the updated COVID-19 vaccines. The ACIP then voted nearly unanimously (13-1) on this same recommendation, which is to use the updated mRNA monovalent mRNA vaccines (Pfizer/BioNTech and Moderna) containing the XBB.1.5 variant.
These recommendations apply to all patients 6 months and older. Patients 6 months through 4 years of age should receive 2 or 3 doses of the updated vaccine, while patients 5 years of age and older should receive a single dose of the updated mRNA vaccine provided 2 months have passed since any previous COVID-19 vaccination.
By November, overall uptake of these COVID-19 vaccines was minimal compared with previous COVID-19 vaccines. The COVID Data Tracker stopped tracking vaccination production and administration in May 2023 when the federal emergency declaration ended. Indications are that overall uptake of the newest authorized vaccines was low because of vaccine fatigue. Healthcare providers, including pharmacists, will likely face significant challenges in achieving COVID-19 vaccination rates that would approach anywhere near previous pandemic highs. Continued health promotions are needed to establish the importance of vaccinations, especially in older adults and others at the highest risk for complications such as hospitalizations and death.
Officials are optimistic that the XBB.1.5-containing vaccines will offer some protection against the currently circulating variants, including EG.5. The previously available bivalent vaccines from 2022 targeted the parent and BA.5 strains of SARS-CoV-2.
WHAT ABOUT THE NOVAVAX COVID-19 VACCINE?
The 2 approved mRNA vaccines from Pfizer and Moderna have had the greatest usage for preventing COVID-19 disease. Novavax also offers a COVID-19 vaccine made using a unique protein-based process. Experts had hoped the more traditional approach to vaccine development could overcome the hesitancy expressed by some about the new mRNA technology.
However, acceptance and uptake of the Novavax vaccine have been limited. The low uptake rate led to a company announcement earlier this year that raised concerns that Novavax would be unable to remain in business long-term unless the updated COVID-19 vaccine was authorized for use in the United States.
Some good news came in October as the FDA amended the current emergency use authorization for the Novavax product, to approve use for the adjuvant vaccine for those 12 years and older. Similar to the variant modification for the mRNA vaccines, the modified protein vaccine includes the spike protein from the omicron lineage XBB.1.5. One additional advantage of the protein vaccine over the mRNA vaccine is improved tolerability upon vaccination. A number of patients experience significant side effects from the mRNA vaccines, which may be increasing vaccine hesitancy. Patients wanting the Novavax vaccine can use an online finder tool to identify locations offering that product.
The ACIP did not meet to specifically discuss the updated Novavax injection. According to a company spokesman, “ACIP’s recommendation last month…was inclusive of all FDA-licensed or authorized updated COVID-19 vaccines including those expected to be licensed or authorized in the coming months.” Time will tell if increased uptake of the Novavax vaccine can offset the decreased uptake of mRNA COVID vaccines.
IN WHICH ARM WOULD YOU LIKE YOUR COVID VACCINE?
When patients receive a number of common intramuscular vaccines, the focus by the administrator is typically on the location of the deltoid muscle using proper technique. The choice of which arm to use is nearly always the patient's preference, with some preferring to use the arm they aren’t using throughout the day in case of soreness. Some new research is challenging the assumption that the choice of arm doesn’t matter, at least for COVID-19 vaccines.
A study published in eBioMedicine evaluated humoral and cellular immune responses after contralateral (different arms) and ipsilateral (same arm) administration of 2 doses of a COVID-19 vaccine. Approximately 303 German adult participants who previously had not received a COVID-19 vaccine were randomized to receive either both doses of the Pfizer/BioNtech mRNA vaccine in the same arm or one in each arm. The primary decision for the arm to administer the vaccine was made based on the calendar day of the vaccination, where certain days were ipsilateral while other days were contralateral. Approximately 14 days after the second dose, blood samples were obtained to test for spike-specific immunoglobulin (Ig) G and neutralizing antibodies and immunologic markers. A subgroup of patients was evaluated for spike-specific CD4 and CD8 T-cells.1
Both methods elicited strong immunologic responses. Median IgG levels were not statistically significantly different between the administration groups. Neutralizing antibodies, median spike-specific CD8 T-cell concentrations, and the numbers of individuals with CD8 T-cells were all statistically significantly lower when the 2 doses were given in opposite arms.
Previously completed COVID-19 vaccine studies could provide interesting data about any differences in immunologic markers after contralateral and ipsilateral administration. The authors of the current study theorize that second shots of vaccines are improved when the same lymph nodes are accessed for immune stimulation. These data bring up a lot of questions. The population here is very limited to a few hundred adult workers. But if this effect can be confirmed, could ipsilateral administration increase the immune response in immunosuppressed patients, which has been problematic with COVID-19 vaccines?
Future research should continue to examine the effect of this initial data on hard outcomes, such as hospitalization and death due to COVID-19 if possible. As the authors state, previous studies with other vaccines had mixed results, with some demonstrating better responses using the contralateral arm (Hemophilus influenzae vaccine) or ipsilateral arm (rabies vaccine).1
CAN INFLUENZA AND COVID-19 VACCINES BE COADMINISTERED?
This year’s winter respiratory virus season has the potential to be a “perfect storm” in which people have influenza infections and COVID-19 — a phenomenon termed “Flurona” in the consumer media. During the COVID-19 pandemic, rates of influenza were strikingly low. In addition, uptake of newly updated COVID-19 vaccines has been minimal compared with previous rounds of administration during the pandemic.
For those patients who are seeking vaccination, questions have arisen about administering both vaccines at the same time. A 2022 study demonstrated an approximate 10% increase in systemic symptoms after simultaneous administration of COVID-19 mRNA boosters and influenza vaccine, but symptoms were generally mild.2
A recent study in JAMA Open Network provides initial data on this question. A prospective cohort study among Israeli healthcare workers evaluated the reactogenicity and immunogenicity of influenza and COVID-19 vaccines when administered simultaneously or separately. Participants received the 2022–23 influenza vaccine (Influvac Tetra) with the Pfizer/BioNTech omicron BA.4/BA.5-adapted bivalent vaccine (contralaterally) or the COVID-19 vaccine alone. Those receiving the vaccines could opt for administration 1 day apart. The primary reactogenicity outcome was post-vaccine symptoms, including fatigue, fever, local symptoms, systemic symptoms, or weakness. The duration of each of these was documented as well. The primary immunogenicity outcomes were anti-spike IgG titers after vaccination.3
The risk of systemic symptoms was similar in the coadministered cohort (OR 0.82; 95% CI, 0.43–1.56). The IgG titers were lower but not significantly different from those in the COVID-19 alone group (95% CI, 0.69–1.04).3
While no previous study looked at the effects of the specific vaccines available for the 2023–24 season, the CDC advises that the COVID-19 and influenza vaccines can be coadministered (unless the patient has received a COVID-19 vaccine within the past 8 weeks or is receiving more than 1 dose of either vaccine and the dosing interval is too short). If both injections are administered on the same day, the injections may be given contralaterally or ipsilaterally. If given in the same arm, at least 1 inch should separate the influenza and COVID-19 vaccinations.
HOW DO PATIENTS WITH LONG COVID RESPOND TO SUBSEQUENT COVID-19 VACCINES?
The primary benefit of vaccination is to decrease the incidence of severe manifestations of COVID-19, including hospitalization and death, which occur mostly in high-risk patients. While some data suggest decreases in duration and incidence of long COVID symptoms in vaccinated patients, the effect of subsequent vaccination on patients reporting long COVID symptoms is unknown.
A recent prospective observational cohort study in the International Journal of Infectious Diseases sheds some light on this topic. Canadian participants (n = 83) who reported long COVID symptoms during 2021 were vaccinated with their choice of either mRNA vaccine (Moderna or Pfizer/BioNTech) or the AZD1222 vector-based vaccine by AstraZeneca. During up to 2 years of follow-up, nearly 90% of participants reported fewer long COVID symptoms (an average decrease of nearly 3 symptoms). Organ system involvement decreased significantly (3.19 vs. 1.89). World Health Organization (WHO)-5 Well-Being Index scores improved nearly 15 points from baseline (42.67 vs. 56.15). More than 75% of patients had improved well-being scores, while 7.4% of participants had worsened symptoms and 14.8% were unchanged. Plasma pro-inflammatory cytokines as well as chemokines were decreased after vaccination.4
If confirmed as more findings are reported, patients with long COVID can be reassured that vaccination can be beneficial in decreasing symptoms such as fatigue, concentration difficulties, memory difficulties, headache, and shortness of breath at rest.
FREE COVID-19 VACCINES FOR MANY CHILDREN AND ADULTS
With government funding ending earlier this year with the emergency declaration, concerns have arisen over the affordability of the COVID-19 vaccines. The CDC and FDA have implemented access programs supporting no-cost vaccinations for many children and adults.
For children, the Vaccines for Children program — or VFC — covers all costs if they are uninsured, Medicaid-eligible, American Indian or Alaska Native, or underinsured. For adults, the Bridge Access Program will cover the costs completely for the 25–30 million adults who are not covered completely through federal or private insurance.
NO BENEFIT FROM INVESTIGATIONAL NOVEL COVID-19 THERAPY
Treatments recommended for COVID-19 vary in their effectiveness, with some marginally effective, such as remdesivir, and others with risks of significant immunosuppression, such as baricitinib or tocilizumab. A recent pilot study evaluated a novel phosphoinositide-3-kinase (PI3K) inhibitor for the treatment of critically ill COVID-19–infected patients.
Adult participants who displayed hypoxic respiratory failure, cardiovascular shock, and/or new cardiovascular disease who had not improved after 2 days of corticosteroid therapy were randomized to either standard care or the novel PI3K inhibitor duvelisib. The primary endpoint was 28-day all-cause mortality with several secondary endpoints such as hospital and intensive care unit length of stay and 60-day all-cause mortality. Due to its unique mechanism of action, serial cytokine evaluation and analysis were performed.
While the patients tolerated therapy well and cytokine reduction was achieved, 28-day all-cause mortality was not different than for standard-of-care COVID-19 treatment. Since the total number of patients enrolled in both arms of this study was 28, it was not powered to detect a difference in mortality. Further study will be required to further delineate the role of this compound in severe COVID-19.5
ANTIVIRAL EFFECTIVENESS VS. LONG COVID
As the COVID-19 pandemic has shifted to endemic status, most people have either received a full series of COVID-19 vaccinations, have been infected, or both. In addition, compared with previous strains of SARS-CoV-2, the omicron variant appears less likely to cause hospitalization and death. While prevention of death and hospitalization are still primary endpoints for the management of COVID-19, a growing concern is the morbidity associated with long COVID symptoms.
A high number of patients have persistent symptoms for months and even years as outlined above, and this can lead to significant use of resources with little relief along with a decreased quality of life. A critical unanswered question is whether treatment with antiviral therapy decreases the incidence, duration, or both of long COVID symptoms. While the government-sponsored trials evaluating a number of therapies for long COVID are ongoing, 2 recent publications with different populations are of interest.
A retrospective study published in Annals of Internal Medicine evaluated ambulatory veterans with COVID-19. Matching cohorts of those receiving nirmatrelvir/ritonavir vs. no treatment were measured for the start of post-COVID-19 complications. The cumulative incidence from days 31 to 180 after treatment or a matched index date evaluated a number of organ-specific symptoms including cardiac, endocrine, gastrointestinal, mental health, musculoskeletal, neurologic, and thromboembolic.
Participants were well-matched demographically and with comorbid conditions, including vaccination rates (approximately 20% were unvaccinated). Patients were excluded if they were hospitalized on the index date of the positive test or if they died. The nirmatrelvir/ritonavir cohort included nearly 10,000 patients. There were no statistically significant differences favoring the treatment group with the exception of venous thromboembolic disease (0.65; 95% CI 0.47–0.97). One major strength of this study was that 93.2% of participants in the active treatment arm received nirmatrelvir/ritonavir within 24 hours of the positive SARS-CoV-2 test.6
There are several limitations to these findings. First, the trial was retrospective in nature, evaluating the electronic health record for results. Second, most participants, as expected, were men (86%) with a median age of 66. Some studies have demonstrated a higher incidence of long COVID symptoms in women (including the study discussed below) and therefore this metric could be underestimated in this study.
The second study evaluated nirmatrelvir/ritonavir and molnupiravir within an older (Medicare) population. Participants were enrolled if diagnosed with COVID-19 between January and September 2022 using International Classification of Diseases (ICD) codes. In addition, prescriptions for either antiviral therapy were used as inclusion criteria for evaluation. Unlike the previously detailed study, only 11 long COVID symptoms were evaluated and included only if they occurred within 4 to 12 weeks after SARS-CoV-2 infection. The symptoms included fatigue/malaise/weakness, dyspnea, cognitive impairment, cough, chest pain, palpitations, headache, muscle/joint pain, memory issues, loss of taste/smell, and sleep disturbances. Cox regression was performed using a number of demographic variables as well as chronic comorbidities.
After applying exclusion criteria, 57% of participants (all ambulatory) remained among the initial nearly 4 million screened people. Most participants who received antiviral therapy received nirmatrelvir/ritonavir (19.5%); only 2.6% received molnupiravir, which is consistent with current guideline recommendations. The incidence of long COVID symptoms was 11.8%, 13.7%, and 14.5% for the nirmatrelvir/ritonavir, molnupiravir, and no treatment groups, respectively. The absolute risk reduction was 2.7% for nirmatrelvir/ritonavir and 0.8% for molnupiravir compared with no treatment; the respective hazard ratios were significant at 0.87 (95% CI, 0.86–0.88; P <0.001) and 0.92 (95% CI, 0.90–0.94; P <0.001). Several demographic factors were associated with increased risk of long COVID symptoms, including female sex; Black, Asian, and Hispanic ethnicity; and low socioeconomic status. The 3 most common long COVID symptoms detected were fatigue (29.9%), dyspnea (22.4%), and cough (21%).7
This trial had several limitations. Vaccination status data were incomplete, use of prescription COVID-19 agents was the indicator of COVID-19, and participants were 65 years and older. Future long-term studies sponsored by the National Institutes of Health should provide further data to help inform this very important question.
The RECOVER-VITAL (viral persistence and reactivation, and immune dysregulation) trial is evaluating an extended treatment of nirmatrelvir/ritonavir of 15 or 25 days. Of note, the 15-day duration group will then receive 10 days of ritonavir alone, which is not expected to have any antiviral effect.
EPIC-SR TRIAL HALTED
Most data evaluating oral antivirals or monoclonal antibodies for the treatment of mild-to-moderate COVID-19 demonstrated decreased hospitalizations when treating the initial SARS-CoV-2 strain in an unvaccinated population. However, a study of nirmatrelvir/ritonavir in a younger population (age 18–50) that was primarily vaccinated showed no benefit using this metric.
The EPIC-SR (Evaluation of Protease Inhibition for COVID-19 in Standard-Risk Patients) trial was designed to answer the question of whether oral nirmatrelvir/ritonavir provided benefit in a standard-risk population. A previous interim analysis showed that treatment had no statistically significant benefit on hospitalization or death, with a low number of overall events (13). In addition, an outcome of sustained cessation of all symptoms was not met. Therefore, Pfizer has unsurprisingly elected to cease enrollment in this study because no benefit is likely to be demonstrated.
HIGH COST OF NIRMATRELVIR/RITONAVIR
In the current COVID-19 practice guidelines, monoclonal antibodies are not recommended. Remdesivir is recommended as an option for ambulatory patients but requires intravenous infusion. This leaves nirmatrelvir/ritonavir as the only “preferred” option for treating outpatient disease.
Previously, the U.S. government had contracted a price of just over $500 for nirmatrelvir/ritonavir. According to a letter obtained by the Wall Street Journal, the 5-day course of therapy will be $1390 when the product becomes available without government support. Pfizer is expected to offer significant discounts and provide patient assistance with out-of-pocket costs, which should leave small copayments for most patients. Medicare patients may receive therapy for no cost through the end of next year. Most commercial health plans are likely to have much lower contracted prices as well through manufacturer subsidies through 2028.
Regardless of the ultimate copayment for the patient, significant questions regarding the cost-effectiveness of nirmatrelvir/ritonavir are unaddressed, considering most of the data documenting effectiveness is in a population that no longer exists (unvaccinated) and a SARS-CoV-2 strain (original parent strain) that has now mutated several times into what appears to be a less virulent omicron subvariant. Based on current studies demonstrating minimal benefit in the vaccinated younger population, conflicting effects with at best minimal impact on long COVID symptoms, and the cessation of the EPIC-HR study, most use is likely to be in the highest-risk population (e.g., people with immunocompromising conditions or obesity) to provide the most cost-effective strategy to decrease morbidity and mortality. In addition, a significant drug interaction risk is present that could result in adverse reactions due to the accumulation of other medications. If current federal studies demonstrate decreased incidence or length of long COVID symptoms, such as shortness of breath or brain fog, then more widespread use could be justified.
LONG COVID CAN PERSIST FOR MANY MONTHS
While the COVID-19 pandemic was declared nearly 4 years ago, quality data regarding the incidence and persistence of long COVID symptoms are only now emerging. Complicating matters is the ebb and flow of a number of circulating variants. Studies have shown a high variation in persistent COVID-19 symptoms. A recently published study provided some much-needed information on the natural history of long COVID and some indication of the overall prognosis.8
Participants in a hospital-based post-COVID clinic in Denmark were evaluated for the long-term prognosis (18 months after index infection) of COVID-19 symptoms, using a post-COVID symptom questionnaire (PCQ) score as the primary outcome. Surveys were administered and repeated 4 times until the 18-month timeframe had been met. Patients were referred to the clinic by their general practitioners after infection with the parent strain or a SARS-CoV-2 variant (alpha, delta, or omicron). The long COVID diagnosis was based on confirmed or probable SARS-CoV-2 infection with symptoms lasting at least 12 weeks and not explainable by an alternative diagnosis as defined by the World Health Organization and referenced in the Danish guidelines.8
A total of 806 participants were enrolled, with most patients previously infected with the parent strain of SARS-CoV-2, followed by omicron, alpha, and delta strains, respectively. Patients in the delta period presented with more significant severe long COVID symptoms per PCQ score (PCQ of 43 for delta vs. 38 for the wild-type strain; P = 0.003). Organ-specific scores did not differ among the variant groups compared with the parent strain. Patients in the omicron group were hospitalized less often but sought long COVID referrals more quickly than the pre-omicron patients. The decreased hospitalization rates correlate well with other studies and known CDC metrics. Increased awareness of and knowledge about long COVID likely led to earlier referrals later in the pandemic period.8
There was no clinically significant decrease in median severity up to 18 months after infection. More concerning, long COVID symptoms failed to improve in 50% of participants or more based on all available scoring measures. Pharmacists should continue to encourage preventive health measures, including recommended COVID-19 vaccines, to prevent infection.8
RSV VACCINES BECOME AVAILABLE
In addition to influenza and COVID-19, people are now learning more about RSV. This common seasonal respiratory virus in most cases causes a mild, self-limiting illness similar to the common cold.
Similar to influenza, 2 common types of RSV (A and B) tend to predominate. While most patients who experience RSV recover within a typical viral time course, several populations are at higher risk of severe disease and hospitalization: infants and older adults. For infants, 2 prophylactic monoclonal antibodies are marketed (but not always available) for administration. Palivizumab (Synagis) is approved for high-risk children 2 years of age or younger. Nirsevimab (Beyfortus) is FDA-approved as a single dose for all infants during their first RSV season.
Until this year, no FDA-approved vaccines were available to prevent RSV in adults. Previous vaccine candidates had poor immunogenicity, and studies lacked an accurate protection endpoint.9 Two vaccines have been recently approved to prevent lower respiratory tract disease in adults 60 years of age and older.
The first product, Arexvy, is a recombinant vaccine in the prefusion form of the F glycoprotein, which enables attachment of the virus to the host cell and after transformation to the postfusion form, entrance of the virus into the host cell (Figure 2). The prefusion form encourages the development of neutralizing antibodies and works well for the RSV A and B subtypes. Most of the evidence supporting approval for this vaccine comes from a large international phase 3 trial published earlier this year in the New England Journal of Medicine; the trial is ongoing.10
| Figure 2. Prefusion and Postfusion States of the RSV F Protein |
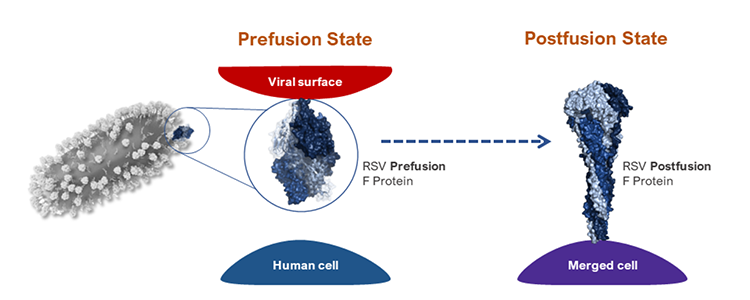 |
In its prefusion state, the respiratory syncytial virus (RSV) F protein is attached to the viral surface and helps the virus attach to host cells. After the virus recognizes a human cell, the F protein irreversibly transitions from its prefusion to its postfusion state, and the virus merges with the human cell. This allows the virus to infect the host.
Source: National Institute of Allergy and Infectious Diseases |
Before the onset of typical RSV season in their geographic location, adult participants aged 60 years and older worldwide were randomized to receive Arexvy or placebo. The primary endpoint was confirmed development of RSV lower respiratory tract disease as indicated by a positive reverse-transcriptase polymerase chain reaction test during RSV season. Further analyses by RSV subtype, types A and B respectively, were completed. Safety outcomes were also assessed as a secondary endpoint.10
Vaccine efficacy with Arexvy was 83% over approximately 7 months, with 7 total cases in the vaccine group and 40 cases in the placebo group. Efficacy for severe RSV disease was higher at 94.1% (95% CI; 62.4–99.9). Efficacy was similar against both RSV A and B subtypes (80%–85%). The vaccine was well tolerated, with most adverse events reported as transient and mild-to-moderate in severity. Pain at the injection site was the most frequently reported local reaction (61%); fatigue was the most often reported systemic adverse event in the vaccine group (34%). The incidence of associated immune-associated diseases within 6 months of vaccine was similar between groups.10
The second recombinant vaccine, Abrysvo, is a bivalent protein-based vaccine with similar quantities of prefusion F antigens from RSV-A and RSV-B. It is currently FDA-approved for the prevention of lower respiratory tract disease caused by RSV in individuals 60 years and older. In addition, Abrysvo is indicated for individuals with pregnancy at 32–36 weeks of gestational age to prevent lower respiratory tract disease and severe lower respiratory tract disease caused by RSV in infants from birth through 6 months of age. The CDC and ACIP also recommend it for these populations. This approval was supported by 2 studies published in the New England Journal of Medicine.
The RSV Vaccine Efficacy Study in Older Adults Immunized against RSV Diseases (RENOIR) Phase 3 double-blind, multicenter, international, placebo-controlled trial that evaluated this bivalent vaccine in adults 60 years of age and older. Patients with stable chronic hepatitis B or C as well as HIV were included with all other immunocompromised patients excluded. Participants could receive COVID-19 and/or influenza vaccination as long as occurring 2 weeks or more before receiving Abrysvo. Participants were randomized 1:1 to receive a single intramuscular dose of 120mcg (60mcg each of RSV subgroup A and B). The two primary endpoints evaluated were RSV-associated lower respiratory tract illness with at least two or at least three signs or symptoms. Adverse reactions were also evaluated.11
RSV-associated lower respiratory tract illness with at least 2 signs or symptoms occurred in 11 vaccine participants and 33 placebo participants (vaccine efficacy, 66.7%; 96.66% CI 28.8–85.8). RSV-associated lower respiratory tract illness with at least 3 signs or symptoms occurred in 2 vaccine participants and 14 placebo participants (vaccine efficacy, 85.7%; 96.66% CI 32–98.7). Approximately 1% of adverse events reported in each group were deemed by investigators to be injection-related at 30 days after injection. Injection site pain (10.5%), erythema (2.7%), swelling (2.4%), fatigue (15.5%), headache (12.8%), and myalgias (10.1%) were the most common adverse effects occurring in the vaccine group. The most common patient-reported side effect was cough (0.6% in both groups). Serious or life-threatening events were reported in 0.5% and 0.4% of vaccine and placebo patients, respectively. These included a delayed allergic reaction (7 hours after injection) with same-day recovery, Miller-Fisher syndrome (a subset of Guillain-Barre syndrome) with subsequent recovery, and Guillain-Barre syndrome with continued recovery at the time of publication.11
A second study evaluated the efficacy of Abrysvo in patients with pregnancy to decrease the risk of RSV in infants. Women between 24- and 36-weeks’ gestation were administered either placebo or a single intramuscular 120-mcg dose of the bivalent vaccine, similar to the dose used in the older adult study. The primary endpoints were medically attended severe RSV-associated lower respiratory tract illness and medically attended RSV-associated lower respiratory tract illness in infants within 90, 120, 150, and 180 days after birth. Adverse effects were also evaluated within the study.12
In more than 7,000 total participants (trial ongoing at the time the interim analysis was published), infants of women who received Abrysvo experienced 6 cases of medically attended severe lower respiratory tract illness within 90 days after birth, compared with 33 infants in the placebo group (vaccine efficacy, 81.8%; 99.5% CI 40.6–96.3). Medically attended RSV-associated lower respiratory tract illness occurred within 90 days in 24 and 56 infants of the vaccinated and placebo groups, respectively, which was not statistically significant. Injection site pain (40.6%), erythema (7.2%), swelling (6.2%), headache (31%), and myalgias (26.5%) were the most common adverse effects that occurred more commonly in the vaccine group. No specific safety signals were seen in either the pregnant women or infants/toddlers up to 2 years of age. Higher rates of jaundice and low birth weight were seen in the vaccine group; these need to be confirmed as the study continues or in other trials. Preterm births were more common in the vaccine group (5.7% vs. 4.7%), but a causal relationship was not confirmed.12
With the approvals of these vaccines, there is the potential for 3 separate respiratory tract preventive vaccines to be administered seasonally with influenza, COVID-19, and now RSV. Data are limited with regard to coadministration efficacy and safety. In one study with a quadrivalent influenza vaccine, both RSV and influenza antibody titers were somewhat lower when coadministered compared to being administered 1 month apart.13 The clinical significance of this observation is unknown at this time. The CDC currently states that all seasonal vaccines may be administered in the same visit with the caveat that enhanced local side effects may increase with “stacking” of vaccines. Logistically, once reconstituted, both of the RSV vaccines must be administered within 4 hours; prudent planning is key in the 2023–24 season for pharmacists who are likely will be administering most of these vaccines.
CONCLUSION
With newly formulated COVID-19 vaccines, newly approved RSV vaccines, and a full spectrum of influenza vaccines, pharmacists will be busy providing important preventive care for patients. With serious concerns about pharmacists’ workload and the number of medication errors in the consumer news, it is critical for pharmacies to be staffed appropriately and safely in order for pharmacists and pharmacy technicians to be able to provide safe and effective dispensing of prescriptions as well as potentially lifesaving vaccines.
REFERENCES
- Ziegler L, Elemis V, Schmidt T et al. Differences in SARS-CoV-2 specific humoral and cellular immune responses after contralateral and ipsilateral COVID-19 vaccination. eBioMedicine. 2023;95:104743.
- Hause AM, Zhang B, Yue X. Reactogenicity of simultaneous COVID-19 mRNA booster and influenza vaccination in the US. JAMA Netw Open. 2022;5(7): e2222241. doi: 10.1001/jamanetworkopen.2022.22241
- Gonen T. Barda N, Asraf K et al. Immunogenicity and reactogenicity of coadministration of COVID-19 and influenza vaccines. JAMA Netw Open. 2023;6:e2332813.
- Nayyerabadi M, Fourcade L, Joshi SA, et al. Vaccination after developing long COVID: impact on clinical presentation, viral persistence, and immune responses. Intl J Infect Dis. Published September 15, 2023. doi: 10.1016/j.ijid.2023.09.006
- Goldsmith SR, Covut F, Fiala M et al. Duvelisib for critically ill patients with coronavirus disease 2019: an investigator-initiated, randomized, placebo-controlled, double-blind pilot trial. Open Forum Infect Dis. 2023;10(11):ofad518.
- Ioannou GN, Berry K, Rajeevan N et al. Effectiveness of nirmatrelvir-ritonavir against the development of post-COVID-19 conditions among U.S. veterans. Ann Intern Med. Published online October 31, 2023. doi.org/10.7326/M23-1394.
- Fung KW, Baye F, Baik SH, McDonald CJ. Nirmatrelvir and molnupiravir and post-COVID-19 condition in older patients. JAMA Internal Med. Published online October 23, 2023. doi: 10.1001/jamainternmed.2023.5099.
- Agergaard J, Gunst JD, Schiottz-Christensen B et al. Long-term prognosis at 1.5 years after infection with wild-type strain of SARS-CoV-2 and alpha, delta, as well as omicron variants. Int J Infect Dis. Published online October 29, 2023. doi: https://doi.org/10.1016/j.ijid.2023.10.022.
- Boyoglu-Barnum S, Chirkova T, Anderson LJ. Biology of infection and disease pathogenesis to guide RSV vaccine development. Front Immunol. 2019;10:1675.
- Papi A, Ison MG, Langley JM et al. Respiratory syncytial virus prefusion F protein vaccine in older adults. N Engl J Med. 2023;388:595-608. doi: 10.1056/NEJMoa2209604
- Walsh EE, Marc GP, Zareba AM et al. Efficacy and safety of a bivalent RSV prefusion F vaccine in older adults. N Engl J Med 2023;388:1465-1477. doi: 10.1056/NEJMoa2213836
- Kampmann B, Madhi SA, Munjal I et al. Bivalent prefusion F vaccine in pregnancy to prevent RSV illness in infants. N Engl J Med. 2023;388:1451-1464. doi: 10.1056/NEJMoa2216480
- Melgar M, Britton A, Roper LE et al. Use of respiratory syncytial virus vaccines in older adults: recommendations of the Advisory Committee on Immunization Practices- United States, 2023. MMWR Morb Mortal Wkly Rep. 2023;72:793-801. doi: http://dx.doi.org/10.15585/mmwr.mm7229a4
Back to Top