
Expired activity
Please go to the PowerPak
homepage and select a course.
COVID-19 Quarterly Update: Emergency Declaration Ends While Endemic Persists
INTRODUCTION
From a 2023 high of 44,000 weekly hospitalizations in early January, coronavirus disease 2019 (COVID-19) hospitalizations are at summer nadirs typical of respiratory infections (Figure 1). The federal public health emergency has ended in the United States. Most of the country has returned to a sense of normalcy. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) will remain a likely seasonal respiratory virus with inherent morbidity and mortality based on a number of factors: SARS-CoV-2 variant virulence, the effectiveness of vaccines, overall vaccine uptake, and availability/effectiveness of safe and effective treatments.
| Figure 1. Weekly Trends in COVID-19 New Hospital Admissions and Weekly COVID-19 Death Rate per 100,000 Population (Age-Adjusted) in the United States Reported to U.S. Centers for Disease Control and Prevention |
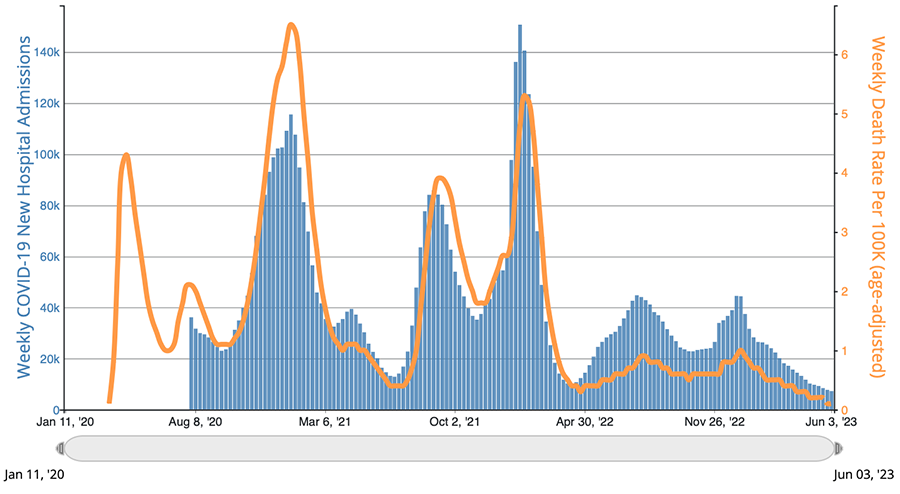 |
| Source: U.S. Centers for Disease Control and Prevention, https://covid.cdc.gov/covid-data-tracker/#trends_weeklyhospitaladmissions_weeklydeathrateaa_00 |
A number of groups are affected by the sunset of the national and public health pandemic emergencies. The federal government will no longer cover COVID-19-related testing, vaccinations, and treatments in these situations:
- Everyone:
- COVID-19 testing coverage has expired, and free tests will not be available as supplies already purchased are depleted.
- Patients with private health coverage:
- Cost sharing will likely increase the costs of testing and treatment related to COVID-19.
- COVID-19 vaccines and boosters will be covered until the government supply purchases through the pandemic are exhausted. At that point, an in-network provider would be needed.
- Patients with Medicare coverage:
- Telehealth coverage has been extended through the end of 2024 using any device in any geographic location, including audio-only telephones.
- No-cost coverage of over-the-counter diagnostic testing and treatments other than oral antiviral agents ended on May 11, 2023. Tests ordered by a provider are generally covered with no cost-sharing under traditional Medicare; people with Medicare Advantage plans have differing coverage and cost-sharing requirements.
- Patients with Medicaid coverage:
- Vaccinations will continue to be 100% covered.
- Testing and treatment with cost-sharing will begin in the third quarter 2024.
- Patients with no health insurance: Will have coverage of certain services through the HHS Bridge Access Program For COVID-19 Vaccines and Treatments Program, which uses a $1.1 billion public–private partnership to help maintain access to COVID-19 care through local chain pharmacies, the existing public health infrastructure (such as health departments), and local health centers.
- Health care providers:
- Enhanced Inpatient Prospective Payment System reimbursement rates end
- Health Insurance Portability and Accountability Act (HIPAA) penalty waivers that allowed the use of nonsecure devices such as smartphones will end when the telehealth waivers expire at the end of 2024.
This continuing pharmacy education program provides information and answers for frontline pharmacists and pharmacy technicians to use in answering the questions of patients and professional colleagues and providing state-of-the-art care for preventing and treating COVID-19.
BIVALENT VACCINE DATA IN OLDER ADULTS SHOW PROMISING OUTCOMES
In early 2021 — when the very first COVID-19 vaccines were reaching community pharmacies and healthcare centers across the United States — security teams were needed to protect the vaccines, and crowds of people were willing to wait in line for hours to receive their dose. As detailed in the last quarterly update, uptake of the newer bivalent COVID vaccines was and remains low, with fewer than 20% of the population up to date with current booster recommendations.
There are 3 primary reasons for this overall decreased uptake: limited clinical data, vaccine fatigue, and assumptions about immunity acquired from natural infection. Data from ongoing phase 3 trials of the new bivalent vaccines provide evidence of efficacy and safety, addressing one of these key reasons.
An ongoing phase 3 noninferiority trial of the monovalent omicron-adapted BA.1 vaccine and the bivalent vaccine included 1,846 adults older than 55 years old who had previously received 3 doses of the BNT162b2 vaccine. Participants were randomized to one of the following vaccines and doses1:
- BNT162b2 vaccine (30 or 60 mcg)
- Monovalent omicron BA.1–adapted BNT162b2 vaccine (monovalent BA.1, 30 or 60 mcg)
- Bivalent omicron BA.1–adapted BNT162b2 vaccine (30-mcg bivalent BA.1 [15 mcg of BNT162b2 + 15 mcg of monovalent BA.1])
- Bivalent BA.1 60 mcg (30 mcg of BNT162b2 + 30 mcg of monovalent BA.1)
The components of these vaccines are listed in Table 1. The study results 1 month after vaccination showed the following1:
- Bivalent BA.1 (30 mcg and 60 mcg) and monovalent BA.1 (60 mcg) had superior neutralizing activity against BA.1 compared with BNT162b2 (30 mcg)
- Bivalent BA.1 (30 mcg and 60 mcg) and monovalent BA.1 (60 mcg) were noninferior against BA.1 compared with BNT162b2 (30 mcg)
- Bivalent BA.1 (either dose) was noninferior to BNT162b2 (30 mcg) with respect to neutralizing activity against the ancestral strain.
- Bivalent BA.1 (30 mcg) had numerically higher neutralizing titers against BA.4/BA.5 and BA.2.75 (these more recently emerged strains are antigenically similar to BA.1) than BNT162b2 (30 mcg).
- Monovalent or bivalent BA.1 (30 or 60 mcg) had similar safety profiles as BNT162b2 (30 mcg).
- Monovalent-BA.1 (30 mcg) and bivalent-BA.1 (60 mcg) had more adverse events reported than the other groups (8.5% and 10.4%, respectively, versus 3.6% to 6.6% in other groups).
These results indicate that the virus evades the acquired immunity from previous vaccines and infections as well as many of the current COVID-19 treatments. The bivalent vaccines provide additional benefits in older adults, and the neutralizing titer and seroresponse data show some protection against the omicron subvariants BA.4, BA.5, and BA.2.75. However, the data also indicate the virus is mutating faster than vaccines are being updated. Further studies on patient efficacy and safety outcomes with the bivalent vaccines — such as prevention of disease, hospitalization, and death — are needed to confirm these findings and provide further evidence to patients and providers of efficacy to alleviate vaccine hesitancy.
Given the results with the adapted vaccines against the omicron BA.1 variant, patients should be encouraged to stay on schedule with recommended bivalent COVID-19 vaccines, especially when they are at a higher risk for severe disease.
| Table 1. Pfizer/BioNTech Vaccines and Their Components |
| Vaccines |
Components |
| BNT162b2 |
mRNA encoding the spike protein of the original SARS-CoV-2 strain |
| Monovalent B1.1.529 BA.1 adapted BNT162b2 (Monovalent BA.1) |
Adapted monovalent mRNA vaccine encoding spike proteins of the omicron variant |
| BA.1 adapted BNT162b2 (Bivalent BA.1) |
Bivalent mRNA vaccine containing 50% of each of the above-mentioned vaccines |
FDA, CDC SIMPLIFYING VACCINATION REGIMENS
As discussed previously, a number of factors are responsible for poor overall vaccination rates with the updated bivalent vaccines. Significant confusion about if, how, and when to receive the newer bivalent vaccines may have contributed to less-than-optimal vaccination rates as well. A telephone survey of more than 1,000 patients who had received a bivalent vaccine dose showed that nearly half were currently awaiting further guidelines to determine when/if they would receive an additional bivalent dose.
The Centers for Disease Control and Prevention (CDC) has simplified its recommendations for COVID-19 vaccinations, and the Food and Drug Administration (FDA) is moving toward a monovalent COVID-19 vaccination for this fall. Among the changes made by the CDC as of June 2023 are the following:
- The original monovalent mRNA COVID-19 vaccines are no longer recommended for use in the United States.
- All patients 6 years of age and older should receive an authorized dose of a bivalent mRNA vaccine, regardless of whether they completed a primary series with the parent vaccine.
- Patients 6 years of age and older who have already received a bivalent vaccine do not need to receive an additional dose, unless they are immunocompromised or 65 years of age or older.
- COVID-19 vaccine dosing schedules vary by age, vaccine type, and previous history of vaccine receipt for young children.
- No changes to the monovalent Novavax vaccine are recommended at this time.
While CDC in April recommended updating the bivalent vaccine, FDA voted in June that the 2023-2024 formulation should be a monovalent COVID-19 vaccine with an XBB-lineage of the omicron variant, with a preference for XBB.1.5. The monovalent vaccine would be used beginning in fall 2023. As this program was being finalized in mid-June 2023, the CDC Advisory Committee on Immunization Practices was preparing to discuss COVID-19 vaccines at its meeting on June 23. While no votes were scheduled, the committee may comment on the difference between its recommendations and the FDA action.
POST-PANDEMIC DEPRESCRIBING OPPORTUNITIES: FOCUS ON ANTIDEPRESSANTS
Early in the pandemic, the effects of COVID-19 on physical health were clear. As lockdowns and social distancing ensued, the implications on social and mental well-being emerged. Many people encountered financial and food instability, loss of loved ones, fear of the virus, and isolation due to lockdowns, among many other factors that led to stress and loneliness, all contributing to an increase in depression and anxiety symptoms. Worldwide prevalence of depression increased from 25.25% before February 2020 to 30.51% in March/April 2020, coinciding with the declaration of COVID-19 as a global pandemic.2
An increase in antidepressant use accompanied the increase in the prevalence of depression. An Australian study noted that the largest increase in antidepressant use in the first year of the pandemic was in adolescent girls aged 10 to 17 years.3 This increase likely happened in other countries, as most schools, sports, and other social avenues were shifted to online platforms or cancelled during the lockdown period.
As society shifts to a post-pandemic normalcy, antidepressant use in patients whose depression symptoms developed during the COVID-19 pandemic should be evaluated for deprescribing. Antidepressants are associated with many adverse effects such as headache, insomnia, changes in weight, and sexual dysfunction. Healthcare professionals, particularly pharmacists, should evaluate these patients for a continued indication for antidepressants. Pharmacists are in a prime position to identify potential patients, discuss deprescribing of antidepressants with prescribers, and conduct research on this topic.
Most antidepressants should be tapered upon discontinuation to avoid a well-known discontinuation syndrome. Common symptoms with selective serotonin reuptake inhibitors can be remembered through the mnemonic “FINISH”: flu-like symptoms, insomnia, nausea, imbalance, sensory disturbances, and hyperarousal (e.g., agitation).4
The COVID-19 pandemic affected the healthcare system well beyond the illness caused directly by the virus. As we reach the close of the pandemic, it is important for healthcare professionals — including pharmacists — to look for opportunities to help the public return to normalcy. For many patients, that may be accomplished partly by addressing unnecessary polypharmacy safely and effectively.
COVID-19 IN PREGNANCY
While overall risks are low, pregnancy is a risk factor for progression to severe COVID-19 and its adverse outcomes, including the death of the mother, preterm delivery, and stillbirths. For adverse neonatal outcomes, the timing of the mother’s COVID-19 is important. All-cause mortality was increased among infants when maternal COVID-19 occurred 14 or fewer days before delivery (1.0% versus 0.3% for ≤14 days and >14 days before delivery). Other adverse outcomes of recent maternal COVID-19 were less breastmilk feeding and a higher risk of infant infection.5
Women with diabetes mellitus, hypertension, and cardiovascular disease have an increased risk for severe COVID-19–related outcomes when pregnant, including maternal morbidities and adverse birth outcomes. Human immunodeficiency virus infection, prepregnancy underweight, and anemia also place women at increased risk of adverse outcomes. Prepregnancy obesity is a risk factor for severe COVID-19–related outcomes, including admission to an intensive care unit, ventilation, any critical care, and pneumonia.6 A recent study published in JAMA Network Open showed that receipt of a third dose of a monovalent mRNA COVID-19 vaccine was not associated with an increased risk of spontaneous abortion in the following 28 or 42 days.7
Because the COVID-19 vaccines reduce the occurrence and severity of COVID-19, they are recommended for everyone aged 6 months or older, including women who are pregnant, are trying to get pregnant, or might become pregnant in the future. Unvaccinated or partially vaccinated women who become pregnant should receive COVID-19 vaccines as early as possible during pregnancy. The vaccine can be administered late in pregnancy when needed. Data on vaccine safety are reassuring, and monitoring is ongoing to detect any emerging concerns. The CDC and the American College of Obstetricians and Gynecologists recommend the use of a bivalent formulation at this time. For those who completed a monovalent series or received a partial series, a bivalent mRNA vaccine is recommended.
While evidence continues to grow demonstrating that COVID-19 vaccination during pregnancy is safe and effective, vaccine hesitancy remains a problem. Based on research on influenza vaccines during pregnancy, some individuals are willing to receive vaccines whether pregnant or not, and others do not want to be vaccinated either way. Two other groups of women have also been identified: some will accept vaccines when pregnant but not at other times, and others will accept vaccines only when they are not pregnant. Since different motivating factors are at play in these views, clinicians should ask patients about their views and counsel them appropriately. Those accepting vaccines at any time need only reminders and little counseling. Those always opposed can be informed of the need for vaccines but should not be alienated to the point they do not accept other needed interventions. Those in the intermediate groups can be counseled on the safety of the vaccine for the fetus or on the need for vaccines throughout life.8
COVID-19 ADENOVIRUS VACCINE NO LONGER AVAILABLE IN UNITED STATES
The Janssen (Johnson & Johnson) COVID-19 adenovirus vaccine is no longer available in the United States. All remaining U.S. government bought vials of the vaccine expired on May 7, 2023, and should be discarded.
Use of the Janssen vaccine was much lower than the Pfizer/BioNTech and Moderna vaccines, with just over 90 million doses administered compared with more than 600 million mRNA doses of the original vaccines. Use of the Janssen vaccine has been limited by efficacy and safety advantages of the mRNA products, including rare cases of thrombosis with thrombocytopenia syndrome in people who received the Janssen product.9
Adult patients who have received 1 dose of the Janssen COVID-19 vaccine are considered to have received a single-dose primary series. Adult patients who have received either 1 or 2 doses of the Janssen COVID-19 vaccine are recommended at this time to receive a bivalent mRNA dose of either the Pfizer/BioNTech or Moderna vaccine at least 2 months after the previous Janssen COVID-19 dose.
RISK OF CARDIAC DEATH IN YOUNG PATIENTS RECEIVING COVID-19 VACCINATION
A number of studies have documented associations between COVID-19 vaccinations, specifically those evaluating mRNA vaccines, and cardiac morbidity, typically manifested by myocarditis and pericarditis. These adverse effects typically occur within 1 week of vaccination (most often after the second dose) and respond well to rest and medications. Patients can return to normal activities soon after their symptoms improve.
Myocarditis and pericarditis are also known complications of COVID-19 infection, making it difficult to establish that these are adverse effects of the vaccines. Cardiac and all-cause mortality data to date have remained sparse. A recent self-controlled case series study using national electronic health data in England evaluated the risk of COVID-19 vaccines and SARS-CoV-2 infection on cardiac and all-cause mortality in young people 12–29 years of age. Comparing the 12 weeks after COVID-19 vaccination with later periods, no significant increases in the incidence of any of 3 mortality endpoints (all-cause registered death, cardiac registered death, and all-cause hospital death) were identified. A significantly increased risk of all-cause and cardiac death was demonstrated in females receiving non-mRNA vaccines and a nonsignificant increase in cardiac death was seen in males (second dose). The risk of all-cause and cardiac mortality was increased after a positive SARS-CoV-2 test among both unvaccinated and to a lesser extent, vaccinated individuals.10
Pharmacists can use studies such as this to discuss risks and benefits of mRNA vaccination in this age group as part of informed and shared decision-making for patients seeking information on COVID-19 vaccines.
ENSITRELVIR EFFICACY AND SAFETY FOR MILD-TO-MODERATE COVID-19
As COVID-19 becomes yet another respiratory virus in general circulation, treatments will continue to be important in its management, especially oral antiviral agents. Ritonavir-boosted nirmatrelvir and molnupiravir are available but have drawbacks. Ritonavir is associated with significant drug interactions because of its strong cytochrome 3A4–inhibiting properties. Because of limited efficacy, molnupiravir is recommended in a limited number of clinical situations — essentially when ritonavir-boosted nirmatrelvir or intravenous antiviral agents, such as remdesivir, are not appropriate or logistically feasible. In addition, ritonavir-boosted nirmatrelvir and molnupiravir are both dosed twice daily.
Ensitrelvir fumaric acid (S-217622) is a novel oral SARS-CoV-2 3C-like protease inhibitor expected to have minimal drug interactions and is dosed once daily. These properties would make ensitrelvir a welcome addition to the COVID-19 armamentarium.
In a phase 2b trial conducted in Japan, 5 days of ensitrelvir therapy was well tolerated overall, with 2 patients discontinuing therapy due to mild eczema or nausea/headache. Transient decreases in high-density lipoprotein (HDL) concentrations were seen as a dose-related adverse effect of ensitrelvir.11 Phase 3 data evaluating clinical outcomes should better ascertain ensitrelvir’s role in the treatment of COVID-19.
ORAL ANTIVIRAL AGENTS AND THE RISK OF LONG COVID
As the pandemic shifts to endemic status, the goals of therapy have begun to shift in comparison to the early stages of the pandemic, when no safe or effective vaccine was available. Most of the U.S. population has acquired immunity through SARS-CoV-2 infections and/or vaccinations (generally with monovalent mRNA products). Recently emerging strains of SARS-CoV-2, such as omicron, have had less severe disease manifestations.
While antiviral therapy continues to focus on decreasing days of symptoms, clinicians and researchers are equally focused on preventing long-term manifestations of the COVID-19 illness, known as “long COVID.” An estimated 65 million people worldwide have long COVID, which can lead to significant clinical and economic manifestations.12
Recent studies conducted in U.S. Veterans Affairs facilities included mostly male veterans with positive SARS-CoV-2 tests; about half had diabetes and/or cardiovascular disease. Those treated with oral antiviral agents had a decreased risk of developing postacute sequelae such as acute kidney injury, cough, deep vein thrombosis, diabetes, dysautonomia, dysrhythmia, fatigue/malaise, incident ischemic heart disease, liver disease, muscle pain, neurocognitive impairment, pulmonary embolism, and shortness of breath. The use of molnupiravir was associated with a 14% decreased risk of later problems.13 Receipt of ritonavir-boosted nirmatrelvir within 5 days of a SARS-CoV-2 positive test was associated with a 26% decreased risk of a post-COVID condition.14 Importantly, patients with an eGFR of 30 mL/min or less were excluded from these studies; this important population that should also be evaluated in future trials.
IMMUNE DETERMINANTS OF COVID-19 DISEASE PRESENTATION AND SEVERITY
COVID-19 is typically mild to moderate in severity in the majority of immunocompetent patients. However, in a significant number of cases, severe disease and death can occur, especially with increasing age. The questions remain as to what factors predict disease severity.
Advanced age, obesity, diabetes mellitus, and chronic kidney disease are conclusively associated with higher risk of disease severity. However, a number of unanswered questions remain about severity as well as long-term symptoms. Some data suggest men are more likely to experience acute illness, yet women are more likely to develop long COVID. In addition, younger children appear to be less likely to contract severe disease. What immune determinants of disease explain these variations in disease prevalence, severity, and long-term effects?
SARS-CoV-2 virus inhibits and delays induction of type I interferon, which influences the development of innate and adaptive immune responses in healthy individuals. When the SARS-CoV-2 virus inhibits type I interferon, the virus can spread and cause greater tissue damage and necrosis. One explanation for a higher disease severity in men is that women elicit a stronger type I interferon response. In addition, toll-like receptor 7 (TLR7), a common virus detector, is expressed on the X chromosome and not Y chromosome, which may further delineate rationale for women developing stronger vaccine responses and better survival rates for acute infections than men. These differences are also seen in boys and girls before puberty, further advancing the possibility of a genetic chromosomal etiology rather than a strictly hormonal variation.15
Type I interferon responses may help explain why men seem to have worse outcomes than women in acute illness, but it does not explain why young children have a lower risk of more severe COVID-19. Other factors may protect young children, including their immune systems being better at with novel challenges (with aging, immune systems rely more on memory).15
Another aspect that correlates with worsening disease severity is the neutrophil-to-lymphocyte ratio (NLR). NLR reflects immune cell composition and serves as an intermediate marker of systemic inflammation. NLR positively correlates with increasing age and obesity, especially in patients with diabetes, indicating worse disease severity in older adults and those who are obese. The NLR ratio is linked to low-grade, chronic inflammation, which is a negative prognostic predictor within COVID-19.15
Further characterization and research into immune determinants of COVID-19 disease can help guide clinicians, including pharmacists, to identify patients at higher risks for poor outcomes.
COVID-19 AND CONJUNCTIVITIS
Over the course of the pandemic, unique symptoms of COVID-19 have emerged. Early in the pandemic, anosmia (lack of smell) was a common finding with the parent SARS-CoV-2 strain. The most recent omicron strain, XBB.1.16 (Arcturus), is causing conjunctivitis in approximately 1 in 10 patients with COVID-19.
Conjunctivitis, or “pink eye,” can be caused by bacteria, allergies, and other factors. However, one of the most common causes is viral infection, such as SARS-CoV-2. In some circumstances, red, swollen, itchy eyes may be the only sign of COVID-19 infection.
Symptoms resolve in most patients but in some cases may be prolonged. Important counseling for any patient with conjunctivitis includes washing hands with soap and water frequently, avoid touching the eye/area surrounding the eye, and not to share personal items such as eyeliner. Patients with suspected COVID-19 with conjunctivitis should be referred primarily based on the risk of severe disease.
CONCLUSION
Fall 2023 will be the first influenza season when people will need to decide whether to accept the recommended COVID-19 vaccine. Pharmacists and pharmacy technicians involved in the immunization process should be ready to engage patients in this discussion. To do so effectively, they must keep up with COVID-19 and the rapid pace of research into SARS-CoV-2 infections.
Treatment of COVID-19 is another area where results of studies are released daily. Keeping track of the virus and its variants, the available pharmacotherapeutic interventions, and the current recommendations of the National Institutes of Health COVID-19 Treatment Guidelines is necessary to be ready to care for patients who test positive or become symptomatic.
REFERENCES
- Winokur P, Gayed J, Fitz-Patrick D et al. Bivalent omicron BA.1–adapted BNT162b2 booster in adults older than 55 years. N Engl J Med. 2023;388:214-227.
- Mahmud S, Mohsin Md, Dewan MN et al. The global prevalence of depression, anxiety, stress, and insomnia among general population during COVID-19 pandemic: a systematic review and meta-analysis. Trends Psychol. 2023;31:143-170.
- de Oliveira Costa, J, Gillies MB, Schaffer AL et al. Changes in antidepressant use in Australia: a nationwide analysis (2015–2021). Aust N Z J Psychiatry. 2023;57:49-57.
- Gabriel M, Sharma V. Antidepressant discontinuation syndrome. CMAJ.2017;189:E747.
- Gosdin L, Wallace B, Lanzieri TM, et al. Six-month outcomes of infants born to people with SARS-CoV-2 in pregnancy. Pediatrics. 2022;150:e2022059009.
- Smith ER, Oakley E, Grandner GW, et al. Clinical risk factors of adverse outcomes among women with COVID-19 in the pregnancy and postpartum period: a sequential, prospective meta-analysis. Am J Obstet Gynecol. 2023;228:161–177. doi: 10.1016/j.ajog.2022.08.038.
- Kharbanda EO, Haapala J, Lipkind HS, et al. COVID-19 Booster vaccination in early pregnancy and surveillance for spontaneous abortion. JAMA Netw Open. 2023;6(5):e2314350. doi:10.1001/jamanetworkopen.2023.14350
- Mitchell SL, Schulkin J, Power ML. Vaccine hesitancy in pregnant women: a narrative review. 2023;41(29):4220–4227. doi: 10.1016/j.vaccine.2023.05.047
- Banerjee S, Sandhu M, Tonzi E, Tambe A, Gambhir HS. Immune-mediated thrombocytopenia associated with Ad26.COV2.S (Janssen; Johnson & Johnson) vaccine. Am J Ther. 2021;28(5):e604-e606. doi: 10.1097/MJT.0000000000001431. PMID: 34469919; PMCID: PMC8415511.
- Nafilyan V, Bermingham CR, Ward IL et al. Risk of death following COVID-19 vaccination or positive SARS-CoV-2 test in young people in England. Nat Commun. 2023;14:1541.
- Mukae H, Yotsuyanagi H, Ohmagari N, et al. Efficacy and safety of ensitrelvir in patients with mild-moderate coronavirus disease 2019: the phase 2b part of a randomized, placebo-controlled, phase 2/3 study. Clin Infect Dis. 2023;76:1403-1411.
- Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol. 2023;21:133-146.
- Xie Y, Choi T, Al-Aly, Z. Molnupiravir and risk of post-acute sequelae of covid-19: cohort study. 2023;381:e074572.
- Xie Y, Choi T, Al-Aly, Z. Association of treatment with nirmatrelvir and the risk of post-COVID-19 condition. JAMA Intern Med. 2023;183(6):554–564. doi: 10.1001/jamainternmed.2023.0743
- Brodin P. Immune determinants of COVID-19 disease presentation and severity. Nat Med. 2021;27:28-33.
Back to Top