
Expired activity
Please go to the PowerPak
homepage and select a course.
The Evolving Management of Irritable Bowel Syndrome with Constipation: Pharmacists’ Key Role in Improving Outcomes
Epidemiology
Irritable bowel syndrome (IBS) is a chronic symptom-based disorder of the gut-brain axis (GBA) characterized by abdominal pain and altered bowel habits.1-3 It is the most common functional gastrointestinal (GI) disorder, with a global prevalence rate of 11.2% and a prevalence rate of 5% to 9.9% in the United States.2 Additional prevalence rates have been reported due to variations in the Rome diagnostic criteria used in studies. For example, prevalence rates in similar regions varied from 4.1% with the Rome IV criteria to 10.1% with the Rome III criteria.3
IBS is more common in women, and studies have found rates of IBS may be up to 3 times higher in women than in men.4 This potentially debilitating disorder primarily affects younger adults (<50 years) at a critical phase in their life when they are focused on advancing their education, establishing their career path, or raising a family.5 IBS is not associated with mortality but is often associated with a reduced quality of life (QoL).4
Pathophysiology
Although the pathophysiology of IBS is complex and not fully understood, dysregulation of the GBA, visceral hypersensitivity, and alterations in GI motility are the main proposed underlying mechanisms. Interactions between these 3 mechanisms are believed to increase the susceptibility of bowel habits to environmental factors such as stress, infection, antibiotics, diet, and food intolerances.6,7
The GBA is a complex bilateral communication pathway involving neuro-immuno-endocrine mediators that connects the central nervous system and enteric nervous system (ENS). The ENS extends from the esophagus to the rectum and regulates digestion and GI motility. Disruption in either direction of the GBA can contribute to symptoms of IBS (Figure 1).8 Visceral hypersensitivity, a neuroenteric phenomenon, contributes to abdominal discomfort and pain in patients with IBS. This heightened sensitivity causes discomfort that is more significant than usual when the intestines stretch from gas or stool and can lead to a sensation of swelling and bloating.9,10
| Figure 1. Gut-Brain Access Bidirectional Communication8 |
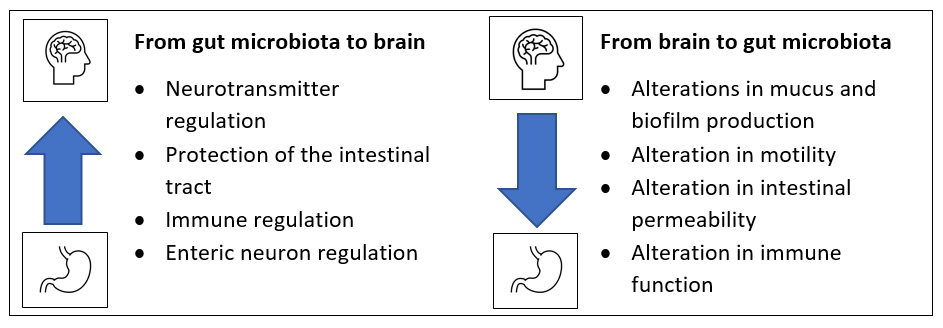 |
| Adapted from Carabotti et al.8 |
The gut synthesizes approximately 90% of serotonin (5-HT) in the body.11 5-HT secretion plays an important role in IBS, and alterations in 5-HT levels may explain the changes in GI motility observed in the different IBS subtypes.12,13 Additionally, studies have found alterations in the gut microbiota in patients with IBS. Data suggest these alterations may lead to altered bowel habits and visceral hypersensitivity commonly reported by patients with IBS.8 Moreover, hormone fluctuations affect bowel function in women. During the luteal phase of the menstrual cycle, when estrogen and progesterone levels are at their highest, GI transit time is delayed, leading to firmer stools. In addition, estrogen may be a contributing factor to visceral hypersensitivity.14 Lastly, genetic factors such as mutations in SCN5A, a sodium channel gene, may have clinical consequences for patients with IBS.15
Etiology
The exact etiology of IBS remains unknown. However, chronic stress (>6 months), infections, and alterations in the gut microbiota may lead to IBS symptoms. Prospective studies suggest that 7% to 33% of patients with acute bacteria enteric infections develop postinfectious IBS (IBS-PI),4 and long-term follow-up studies indicate that IBS-PI symptoms can persist for over 10 years.16
Additionally, diet and food intolerances can trigger IBS symptoms. Fermentable carbohydrates, including mono-, di-, and oligosaccharides, and polyols (FODMAPs), increase GI water secretion and fermentation in the colon, which leads to colonic distension and abdominal symptoms such as bloating. Diets high in FODMAPs can trigger meal-related IBS symptoms. Other foods commonly associated with worsening IBS symptoms include coffee, alcohol, and spicy and fatty foods.17 Compared with the general population, food intolerances are more common in patients with IBS, with prevalence rates as high as 50%. However, patients with IBS are not more likely to develop true food allergies, and the American College of Gastroenterology (ACG) does not recommend routine food allergy testing in patients with IBS. Fiber intake is also an important consideration. There are 2 primary sources of fiber: soluble and insoluble. Soluble fiber is found in psyllium, oat, bran, barley, and beans. It increases the stool water content and resists fermentation in the colon, resulting in laxative effects. In contrast, insoluble fiber, which is in wheat bran, whole grains, and some vegetables, ferments in the colon and results in gas formation, bloating, and flatulence.5
Diagnosis
The ACG IBS guidelines recommend a positive diagnostic strategy that incorporates a physical examination, a thorough clinical history focused on characteristic IBS symptoms (abdominal pain and altered bowel habits), and symptom duration, plus rules out a family history of inflammatory bowel disease and colorectal cancer and alarm symptoms. Alarm symptoms include blood in stools, unintentional weight loss, and symptom onset after age 50 years.5
The Rome criteria are used to diagnose IBS in both clinical and research settings.18 Per the Rome IV criteria, individuals with IBS have experienced recurrent abdominal pain on average at least 1 day/week in the past 3 months that is associated with 2 or more of the following: related to defecation, associated with alteration in stool frequency, or associated with alteration in stool form. Additionally, symptom onset must occur more than 6 months prior to diagnosis.5
Characteristics of IBS Subtypes
There are 4 IBS subtypes: constipation-predominant (IBS-C), diarrhea-predominant (IBS-D), mixed bowel habits (IBS-M), and unclassified (IBS-U). Patients with IBS-M have both diarrhea and constipation on the same day, and patients with IBS-U meet the diagnostic criteria for IBS, but stool form is inconsistent and does not correlate with any of the other subtypes. The ACG IBS guidelines recommend using the Bristol Stool Form Scale to evaluate stool appearance, with lower numbers representing hard and dry stools and higher numbers representing loose and watery stools (Table 1).5,19
| Table 1. 7 Types of Stool Forms on the BSFS5 |
| BSFS Type |
Stool Description |
IBS Subtype According to the Rome IV Criteria |
| IBS-C |
IBS-D |
IBS-M |
IBS-U |
| 1 |
Separate hard lumps that resemble nuts |
>25% of associated bowel movements OR |
<25% of associated bowel movements OR |
>25% of associated bowel movements AND |
Cannot be determined |
| 2 |
Sausage-shaped but lumpy |
| 3 |
Like a sausage but with cracks on its surface |
N/A |
N/A |
N/A |
| 4 |
Like a sausage, smooth and soft |
N/A |
NA |
N/A |
| 5 |
Soft blobs with clear-cut edges |
N/A |
N/A |
N/A |
| 6 |
Mushy with fluffy pieces and ragged edges |
<25% of associated bowel movements |
>25% of associated bowel movements |
>25% of associated bowel movements |
| 7 |
Watery with no solid pieces |
| BSFS=Bristol Stool Form Scale; IBS=irritable bowel syndrome; IBS-C=IBS with constipation; IBS-D=IBS with diarrhea; IBS-M=IBS with mixed or alternating bowel habits; IBS-U=IBS without a significant pattern of abnormal stool; N/A=not applicable as not included in the Rome IV criteria. |
IBS symptoms may fluctuate—disappearing and re-emerging—and more than 50% of patients change predominant IBS subtypes over a 1-year period. Most medications treat a specific IBS subtype. Determining the patient's subtype when they are not taking treatment that could affect their bowel movements is a critical first step in caring for patients with IBS. US Food and Drug Administration (FDA)-approved treatment options are available for IBS-D and IBS-C; however, there are no FDA-approved treatment options for subtypes IBS-M or IBS-U in the United States.5 The focus of this learning activity is IBS-C.
Complications
Reduced QoL
IBS negatively impacts patients' ability to work and socialize and is associated with significantly reduced QoL. A survey of nearly 2000 adults with IBS found that, on average, patients had to restrict their usual activities 20% of the calendar year. When asked about the risk they would tolerate to receive a new and effective treatment for their IBS that would make them symptom-free, patients were generally willing to give up 15 years of their life, equivalent to approximately 25% of their remaining years.20
Economic Impact
Although not indicated or recommended to diagnose IBS, colonoscopy is one of the most frequent and expensive tests used to evaluate patients with IBS symptoms.5 Nearly 25% of colonoscopies in the United States are performed on patients aged younger than 50 years to investigate IBS symptoms despite the lack of evidence to support this practice in the absence of a family history of colorectal cancer or alarm symptoms.5,21
There are an estimated 3.6 million physician visits for IBS care annually in the United States and compared with matched controls without IBS, patients with IBS consumed 50% more healthcare resources.22 In the United States, the estimated annual cost per patient with IBS ranges from $742 to $7,547, with annual direct and indirect associated care costs exceeding $20 billion.21,22
Patient Scenario
KL is a 40-year-old woman at the gastroenterology clinic today to discuss her IBS symptoms and treatment options. Over the past 7 months, she has been having very few bowel movements—usually only 2 to 3 days of the week, often with significant straining. On the days she does have a bowel movement, her stool is hard, lumpy, and hard to evacuate. In addition, her abdominal pain improves after having a bowel movement. She has noticed significant bloating, which worsens when she eats a lot of fiber.
KL has no past medical history, and she denies having a GI-related family history. Her physical examination, including her rectal examination and recent laboratory tests, are all normal. She is not currently on any medications except over-the-counter (OTC) vitamins. Her gastroenterologist diagnoses KL with IBS-C. KL is referred to you, the pharmacist, for disease management. She tells you she is hesitant to start taking medications because she is concerned about having diarrhea and she first wants to try to change her diet to manage her IBS-C symptoms. She asks you what dietary interventions she can try for her IBS-C.
IBS Treatment Guidelines
The ACG IBS guidelines provide recommendations for nonpharmacologic and pharmacologic treatment options based on their ability to improve global IBS symptoms or IBS-C–specific symptoms (Figure 2),5 and the American Gastroenterology Association (AGA) IBS guidelines focus on the pharmacologic management of IBS-C (Figure 3).3
| Figure 2. American College of Gastroenterology Recommended Nonpharmacologic and Pharmacologic Treatment Options for the Management of IBS-C Symptoms5 |
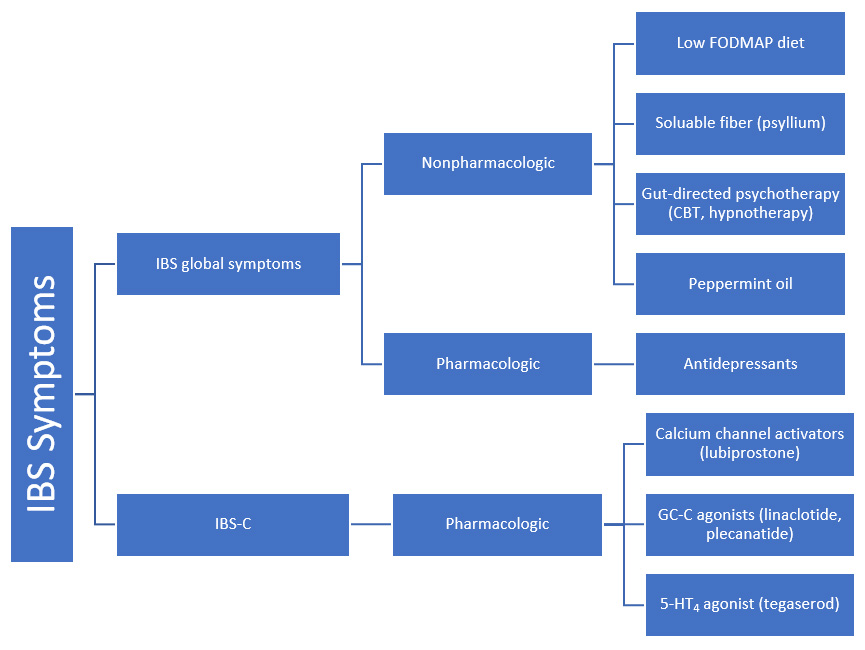 |
| 5-HT=serotonin; CBT=cognitive behavioral therapy; FODMAP=fermentable oligosaccharides, disaccharides, monosaccharides, and polyols; GC-C=guanylate cyclase-C; IBS=irritable bowel syndrome; IBS-C=IBS with constipation. |
| Figure 3. American Gastroenterological Association Guidelines for IBS-C Treatment3 |
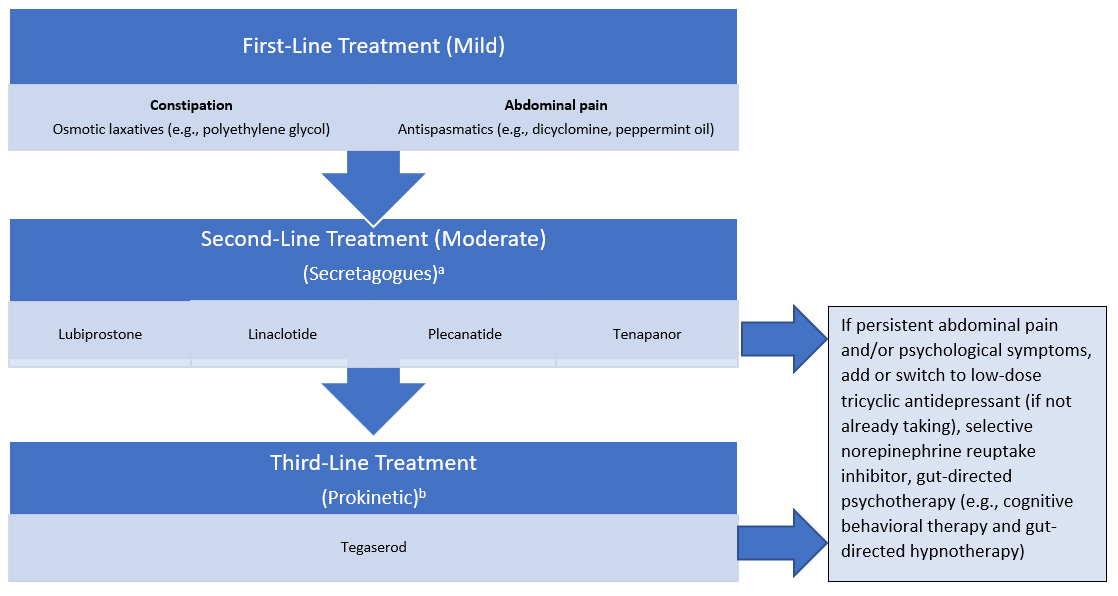 |
aMedication selection should be based on the patient’s individual clinical features and needs.
bWithdrawn from the US marketplace in June 2022.
IBS-C=irritable bowel syndrome with constipation. |
Nonpharmacologic Global IBS Treatments
Low FODMAP Diet
A systematic review and meta-analysis of 9 randomized controlled trials (N=397) found that a low FODMAP diet was more effective at improving IBS symptoms compared with various control diets.23 The ACG IBS guidelines include a conditional recommendation, based on very low-quality evidence, for a limited trial of a low FODMAP diet to improve global IBS symptoms.5
A 3- to 6-week trial is generally considered sufficient for most patients with IBS.17 Examples of high FODMAP foods and low FODMAP alternatives are shown in Table 2.24 Low FODMAP diets are generally considered safe; however, long-term avoidance of FODMAPs may lead to alterations in the gut microbiota and nutritional deficiencies.17
| Table 2. Food Categories and Examples of High and Low FODMAPs24 |
| Food Category |
High FODMAP |
Low FODMAP Alternatives |
| Cereals (bread and pasta) |
Rye and wheat cereals when eaten in large quantities (e.g., bread, pasta, crackers) |
Gluten-free cereals, spelt (type of grain) bread/cereals, quinoa |
| Fruits |
Apples, pears, watermelon, mango, apricots, cherries, plums, prunes |
Banana, blueberry, cantaloupe, grapes, grapefruit, oranges, strawberries, raspberries, honeydew melon |
| Vegetables |
Artichoke, asparagus, beetroot, broccoli, brussel sprout, cauliflower, cabbage, garlic, leek, okra, mushrooms, onion, pea, shallot |
Bamboo shoot, bok choy, carrot, celery, chives, corn, eggplant, green bean, lettuce, parsnip, pumpkin, silverbeet, scallion (green part only) |
| Protein |
Legumes: baked beans, chickpeas, lentils, red kidney beans |
Nuts and seeds: almonds, hazelnuts, peanuts, pumpkin seeds; tofu |
| Milk and diary |
Regular and low-fat cow, goat, and sheep milk; ice cream; yogurt; cheese: soft and fresh cheeses |
Lactose-free milk and yogurt, rice milk, almond milk, gelato, sorbet, hard cheese |
FODMAPs, fermentable oligosaccharides, disaccharides, monosaccharides, and polyols.
Adapted from Magge and Lembo.24 |
Fiber
Soluble fiber in doses up to 35 g/d is recommended in the ACG IBS guidelines to treat global IBS symptoms. However, soluble fiber may worsen IBS symptoms of bloating and flatulence in some patients and should be gradually introduced into the diet.5,12
Probiotics
In the United States, probiotics are considered dietary supplements and are not intended to diagnose, treat, or cure a disease. The ACG IBS guidelines recommend against probiotics for the treatment of global IBS symptoms due to very poorly designed studies and heterogeneity in probiotic strains.5,25
Gut-Directed Psychotherapy
Gut-directed psychotherapies (GDPs), such as cognitive behavioral therapy and gut-directed hypnotherapy, have reduced IBS symptoms in some patients. Current ACG IBS guidelines suggest using GDPs combined with other IBS treatments for patients who are mentally stable. However, patients with underlying mental health disorders should be referred to non-GI mental health professionals because GDPs are less effective in these patients. Attractive features of GDPs include a favorable safety profile and long-term benefits even after treatment discontinuation.5
Peppermint Oil
Peppermint oil is antispasmodic, and studies of total daily doses ranging from 450 mg to 900 mg have shown positive results in relieving global IBS symptoms.12,25 Based on low-quality evidence, the ACG IBS guidelines recommend peppermint oil for global IBS symptoms.5 Enteric-coated formulations are available to minimize the risk of GI reflux that commonly occurs with peppermint oil.25
Nonpharmacologic Next Steps for KL
To address KL's question about the role of diet in IBS, as a pharmacist, you can discuss a 3- to 6-week trial of the FODMAP diet, explaining that there is very low evidence to support this diet in patients with IBS and that there are concerns about prolonged use of this diet given the risk of micronutrient deficiencies. Gradually introducing soluble fiber, such as psyllium, is another option, but you should advise KL to avoid insoluble fiber because it can worsen bloating and abdominal pain.
Pharmacotherapy for Global IBS
Antispasmodics
Antispasmodics, such as hyoscine and dicyclomine, are used to treat global IBS symptoms, particularly abdominal pain, due to their ability to relax intestinal smooth muscle and reduce GI motility. There are no FDA-approved antispasmodics for the treatment of IBS-related symptoms. The ACG IBS guidelines recommend against their use due to the lack of data to support their efficacy and poor tolerability.5 Conversely, the AGA IBS guidelines recommend using antispasmodics in IBS-C as a conditional recommendation with low certainty, given the potential for constipation effects due to anticholinergic activity.3
Antidepressants
Tricyclic antidepressants.
No antidepressants are FDA approved to treat IBS symptoms. Tricyclic antidepressants (TCA) are used based on their ability to alter GI motility, secretions, and sensation, and their beneficial effects are thought to be independent of their antidepressant effects. TCAs are associated with greater improvements in abdominal pain relief compared with placebo. In patients with IBS-C, secondary amine TCAs such as desipramine and nortriptyline are preferred due to their lower anticholinergic effects.3 Based on moderate-quality evidence, the ACG IBS guidelines strongly recommend using antidepressants to treat global IBS symptoms.5 The AGA guidelines provide a conditional recommendation for the use of TCAs with low certainty of evidence.3
Selective serotonin reuptake inhibitors.
The efficacy of centrally acting selective serotonin reuptake inhibitors (SSRIs) to treat IBS symptoms has been studied based on their ability to alter intestinal motility and use in clinical practice to treat chronic pain. However, in most patients with IBS, SSRIs do not appear to significantly impact visceral hypersensitivity. Additionally, studies have failed to find significant improvements in global IBS symptoms or abdominal pain with SSRIs. The AGA IBS guidelines recommend against SSRI use in patients with IBS (conditional recommendation based on low certainty evidence).3
Serotonin-norepinephrine reuptake inhibitors.
No serotonin-norepinephrine reuptake inhibitors (SNRIs) are FDA approved to treat IBS-C, and clinical trials in patients with IBS-C are lacking. However, it has been proposed that there is greater effectiveness among members of this class of medication compared with SSRIs due to SNRIs’ effects on both serotonin and norepinephrine and their efficacy in treating other pain conditions.3
3-Month Follow-up Visit
KL presents to the gastroenterology clinic for a follow-up after trying a low FODMAP diet and gradually increasing her soluble fiber intake over the past 3 months. She tells you she could not follow the low FODMAP diet due to the cost and feels that some of her bloating has improved since starting psyllium. Despite some improvement, she is still experiencing IBS-C symptoms. She also mentions that in the past, she has tried and failed several treatments, including OTC stool softeners, which did not work; magnesium citrate, which failed to improve her abdominal pain and caused diarrhea; and polyethylene glycol (PEG), which did not help her abdominal pain or ease her bloating. Today she is interested in FDA-approved pharmacologic treatment options.
Pharmacotherapy for IBS-C
OTC IBS-C Treatment Options
OTC osmotic laxatives such as PEG increase water in the intestinal lumen and reduce intestinal transit time.1 Studies have found doses of PEG ranging from 17 to 35 g/d to be effective for relieving constipation associated with IBS-C. However, placebo-controlled trials failed to show improvements in overall symptoms or pain.3,12 Based on low-quality evidence, ACG IBS guidelines conditionally recommend against using PEG-containing products to relieve global IBS symptoms in patients with IBS-C.5 However, the AGA guidelines conditionally recommend using PEG laxatives based on low certainty of evidence, given its low cost and availability.3
FDA-Approved IBS-C Treatment Options
Five medications have received FDA approval for the treatment of IBS-C symptoms in the United States: 4 secretagogues (lubiprostone, linaclotide, plecanatide, and tenapanor) and 1 prokinetic (tegaserod) (Table 3).5,26-33 On June 30, 2022, the sponsor of tegaserod issued a press release stating its intention to voluntarily withdraw their product from the United States market for commercial reasons.27
| Table 3. Summary of 5 US Food and Drug Administration-Approved Pharmacotherapies for IBS-C |
| Medication Name (S or P) |
Drug Target |
Mechanism of Action |
Lubiprostone (S)28 |
Chloride channel activator that selectively activates type 2 channels on the intestines |
• Increases intestinal fluid secretion
• Increases motility in the intestine
• May stimulate recovery of mucosal barrier function and reduce intestinal permeability |
Linaclotide (S)29 |
Guanylate cyclase-C agonist that acts locally on the luminal surface of the intestinal epithelium |
• Stimulates secretion of chloride and bicarbonate into intestinal lumen
• Increases intestinal fluid and accelerates transit time
• Mediates visceral hypersensitivity (in animal model) |
Plecanatide (S)30 |
Tenapanor (S)31 |
Locally acting sodium-hydrogen ion exchange isoform-3 receptor inhibitor |
• Reduces absorption of sodium from the small intestine and colon
• Increases water secretion into the intestinal lumen
• Accelerates intestinal transit time
• Reduces abdominal pain by decreasing visceral hypersensitivity |
Tegaserod (P)32,a |
Serotonin (5-HT4) receptor agonist |
• Initiates the peristaltic reflex
• Accelerates gastrointestinal transit
• May reduce visceral hypersensitivity |
aWithdrawn from the US marketplace in June 2022.27
IBS-C=irritable bowel syndrome with constipation; P=prokinetic; S=secretagogue. |
The most recent FDA guidance on regulatory IBS efficacy endpoints recommends a composite primary endpoint that assesses improvements in abdominal pain and abnormal bowel movements. The FDA recommends asking patients to evaluate abdominal pain by rating their worst abdominal pain daily over the past 24 hours and to evaluate abnormal bowel habits by rating weekly changes in the number of complete spontaneous bowel movements (CSBMs). Patients are categorized as overall responders if they achieve prespecified improvements in daily or weekly responses for both measures at least 50% of the time.34
Lubiprostone.
Lubiprostone is a locally acting prostaglandin derivative that selectively activates chloride type-2 channels on the apical membranes of the intestinal epithelial cell to increase intestinal secretion of calcium and water. In addition, lubiprostone reduces GI transit time and may stimulate recovery of mucosal barrier function and reduce intestinal permeability, improving visceral hyperalgesia.28,35 Based on moderate-quality evidence, the ACG IBS guidelines strongly recommend the use of lubiprostone to treat global IBS-C symptoms.5 Likewise, the AGA IBS guidelines include a conditional recommendation based on moderate certainty of evidence recommending the use of lubiprostone in patients with IBS-C.3 Lubiprostone is the only FDA-approved IBS-C treatment available as both brand and generic.
The approved adult IBS-C dose of lubiprostone is 8 µg orally twice daily. In patients with severe hepatic impairment (Child-Pugh Class C), a reduced starting dose of 8 µg daily is recommended with dose escalation based on tolerability and treatment response.28 Efficacy was primarily established based on findings in the intent-to-treat population (N=1154) of 2 similarly designed placebo-controlled, phase 3, 12-week trials (NCT00380250, NCT00399542).28,29
These trials were conducted before the release of the most recent FDA guidance document and used a more rigorous primary efficacy endpoint. The primary efficacy endpoint used in these trials was a weekly assessment of patient responses to a global symptom relief question. Patients were asked to rate their relief of IBS symptoms (abdominal discomfort/pain, bowel habits, and other IBS symptoms) over the past week compared with when they entered the study. Patients who reported moderate relief in IBS symptoms 100% of the time or significant relief 50% of the time per month during at least 2 of the 3 months of the study were considered responders.28,29 Patients who reported more than mild worsening of IBS symptoms, required an increase in rescue medications use, or discontinued treatment due to lack of efficacy during each monthly evaluation period were considered nonresponders.1,28 The percentage of lubiprostone-treated responders in the pooled analysis of the two trials was 17.9%, compared with 10.1%% in placebo patients (P=0.001), respectively.29 A post hoc analysis (N=515) conducted using the revised FDA guidance definition of overall treatment responder found significantly higher responder rates with lubiprostone (23.8%) compared with placebo (12.6%) (P = .012).36 The most common adverse events (AEs) reported during clinical trials occurring at an incidence of at least 5% of patients treated with lubiprostone were nausea (8%), diarrhea (7%), and abdominal pain (5%).28
Pharmacists should counsel patients to take lubiprostone with food to reduce the potential for nausea. Lubiprostone’s indication is limited to women aged 18 years and older because more than 90% of adults in the pivotal trials were female. Patients with known or suspected mechanical GI obstruction should not take lubiprostone. Pharmacists should counsel patients on the importance of holding dosing and rehydration if they experience severe diarrhea.28
Linaclotide and plecanatide.
Linaclotide and plecanatide are structural peptide analogs that act as guanylate cyclase-C (GC-C) receptor agonists. Stimulation of GC-C receptors in the intestines results in increased chloride and bicarbonate secretion, intestinal fluid secretion, and accelerated transit time. In addition, animal models suggest that these 2 medications relieve abdominal pain by reducing abdominal muscle contractions and activating visceral neurons.30,31,34
The ACG IBS guidelines include a strong recommendation based on high-quality evidence for using GC-C agonists to treat global IBS-C symptoms.5 AGA guidelines also have a strong recommendation based on high-quality evidence for the use of linaclotide and a conditional recommendation based on moderate-quality evidence for the use of plecanatide to treat patients with IBS-C.3
The approval of linaclotide 290 µg orally once daily for IBS-C was based primarily on findings from 2 placebo-controlled, phase 3 trials (linaclotide, n=806; placebo, n=798) (NCT00948818, NCT00938717).37,38 These trials used the updated FDA overall responder primary endpoint with a prespecified combined reduction of at least 30% from baseline in worst abdominal pain and an increase of at least 1 CSBM per week from baseline during the same week for at least 50% of the 12-week trial duration. In both trials, 34% of linaclotide-treated patients met the definition of overall responder compared with 21% and 14% of placebo patients for NCT00948818 and NCT00938717, respectively.37,38 A significant difference between the 2 treatment groups was observed in the first week, with maximum effects seen at weeks 6 to 9 and maintained until the end of the studies. During the IBS-C clinical trials, the most frequently reported AE was diarrhea, which occurred in 20% of linaclotide-treated patients, followed by abdominal pain (7%), flatulence (4%), and abdominal distension (2%).30
Linaclotide should be taken on an empty stomach at least 30 minutes before the first meal of the day. Linaclotide is contraindicated in pediatric patients aged younger than 2 years due to the risk of serious dehydration (boxed warning) and in patients with known or suspected mechanical GI obstruction. Of note, linaclotide was previously contraindicated in children aged younger than 6 years, but the package insert has since been modified to claim that although no longer a contraindication, the safety and effectiveness of linaclotide in patients aged younger than 18 years still have not been established. Pharmacists should counsel their patients on the importance of holding dosing and rehydration if they experience severe diarrhea.30
The efficacy of plecanatide 3 mg orally daily for managing symptoms of IBS-C was established in two 12-week, double-blind, placebo-controlled trials (plecanatide, n=724; placebo, n=729) (NCT02387359, NCT02493452).39 The primary efficacy endpoint used in these trials was the FDA overall responder endpoint used in the linaclotide trials. Significantly more plecanatide-treated patients than placebo-treated patients achieved this primary endpoint in both studies (plecanatide 30% vs placebo 18% and plecanatide 21.5% vs placebo 14%).39 As with linaclotide, the most common AE reported in 4.3% of plecanatide-treated patients was diarrhea.39 It can be taken with or without food in all adults. Plecanatide also carries a boxed warning about the risk of serious dehydration in pediatric patients, specifically being contraindicated in patients aged younger than 6 years. Pharmacists should discuss the importance of holding dosing and rehydration if individuals experience severe diarrhea while on plecanatide.31
Tenapanor.
Tenapanor is the most recent secretagogue approved by the FDA in September 2019.32 Tenapanor is a first-in-class, minimally absorbed, small-molecule inhibitor of GI sodium-hydrogen ion exchange isoform-3 (NHE3) receptor. NHE3 is expressed on the apical surface of the small intestines and colon and is primarily responsible for the absorption of dietary sodium. By inhibiting NHE3, tenapanor reduces sodium absorption from the small intestine and colon, increasing water secretion into the intestinal lumen and accelerating intestinal transit time. In addition, in animal models, tenapanor has been shown to reduce abdominal pain by reducing visceral hypersensitivity.32,34 The ACG IBS guidelines were developed before tenapanor was approved, thus it is not included. Tenapanor is conditionally recommended for treating IBS-C based on moderate-quality evidence in the more recent AGA guidelines.3
The efficacy of oral tenapanor 50 mg twice daily for the treatment of adults with IBS-C was established in 2 double-blind, placebo-controlled, phase 3 trials: T3MPO-1 (NCT02621892), a 12-week study (tenapanor, n=307; placebo, n=299)32,40; and T3MPO-2 (NCT02686138), a 26-week study (tenapanor, n=293; placebo, n=300).32,41 Both studies used the same FDA overall responder primary endpoint evaluated in the linaclotide and plecanatide placebo-controlled studies. Overall responders were prespecified as patients with a reduction of at least 30% in average weekly worst abdominal pain and an increase of at least 1 weekly CSBM from baseline, both in the same week, for at least 50% of the first 12 treatment weeks. Responder rates in T3MPO-1 were 27% in the tenapanor group compared with 19% in the placebo group (P = .02)40; in T3MPO-2, 37% of tenapanor-treated patients versus 24% of placebo-treated patients (P < 0.001) met this primary responder endpoint.41 In both trials, improvements from baseline in average weekly CSBMs and abdominal pain were observed starting at week 1 and maintained throughout the study.32,40,41 Diarrhea was the most common AE in both studies, reported by 15% to 16% of tenapanor-treated patients. Diarrhea was generally rated as mild to moderate in severity and typically lasted 1 week or less.40,41
Selecting a Treatment for KL
Because KL is a 40-year-old woman with no history of cardiovascular (CV) disease and no CV risk factors, any of the 5 FDA-approved medications would be indicated for treatment of her IBS-C. However, the ACG IBS guidelines suggest reserving tegaserod for patients with 1 or fewer CV risk factors who have not adequately responded to secretagogues, including lubiprostone, linaclotide, and plecanatide. The updated AGA guidelines include a similar recommendation and now include tenapanor as a recommended secretagogue.
Her gastroenterologist secures approval for tenapanor. What counseling points should you provide to KL on the use of this treatment when she visits the pharmacy?
Tenapanor should be taken immediately before breakfast or the first meal of the day and immediately before the evening meal. As with most other secretagogues, tenapanor carries a boxed warning about the risk of serious dehydration in pediatric patients and is contraindicated in children aged younger than 6 years and patients with known or suspected mechanical GI obstruction. Pharmacists should counsel patients on the importance of contacting their healthcare provider (HCP) if they experience severe diarrhea because treatment may need to be suspended. In addition to diarrhea, other common AEs reported during the clinical trials included abdominal distension (3%), flatulence (3%), and dizziness (2%). Pharmacists should be aware that tenapanor may reduce the exposure of OATP2B1 substrates, such as enalapril.32
Tips for Counseling KL
When KL comes to pick up her prescription, you provide the following counseling points on the use of tenapanor:
- The recommended adult dose is 50 mg orally twice a day immediately before breakfast or the first meal of the day and immediately before dinner.
- Tenapanor works by softening stool and accelerating bowel movements to improve constipation. It also lessens pain-sensing nerve activity to reduce abdominal pain, including bloating and discomfort.
- Diarrhea was the most common AE in the clinical trials and was generally considered mild-to-moderate and resolved in less than 1 week with continued treatment. However, if diarrhea is severe, KL should stop treatment and contact her HCP.
- Other potential AEs include abdominal swelling, gas, and dizziness. IBS is a chronic disease and taking tenapanor daily as prescribed is important. If there are any barriers to treatment, such as insurance coverage, KL should contact her gastroenterologist's office immediately.
Tegaserod.
Tegaserod, a 5-HT4 receptor partial agonist, is the only prokinetic agent that has received FDA approval to treat IBS-C.33 Stimulation of 5-HT4 receptors initiates the peristaltic reflex, accelerates GI transit, increases fluid in the GI tract, and may reduce visceral hypersensitivity.3,34 Based on low-quality evidence, the ACG IBS guidelines conditionally recommend reserving tegaserod for treating IBS-C symptoms in women aged younger than 65 years without a history of ischemic CV disease (ie, myocardial infarction, stroke, transient ischemic attack, or angina) with 1 or fewer CV disease risk factors (ie, active smoker, high blood pressure, high cholesterol, history of diabetes, aged >55 years, or obese) who have not adequately responded to secretagogues.1,5,33 The AGA guidelines also recommend reserving tegaserod as a third-line treatment option for patients who have failed other secretagogues.3,42
Tegaserod was initially approved in 2002 for treatment of women with IBS-C. It was later voluntarily removed from the market in 2007 due to concerns of a small but statistically significant increased rate of CV events.27 However, subsequent studies have not been able to replicate this finding, leading to FDA reapproval of tegaserod in 2019 with a narrower indication limiting its use to women aged younger than 65 years with no history of CV disease and 1 or fewer CV disease risk factors.1,33 As previously mentioned, tegaserod was recently voluntarily removed from the United States market again, this time for commercial reasons.27
The efficacy of tegaserod 6 mg orally twice daily was established during 3 multicenter, double-blind, placebo-controlled, 12-week trials (tegaserod, n=1244; placebo, n=1226).33 The primary efficacy endpoint used in these trials was the Subject’s Global Assessment (SGA) of symptom relief. Patients were classified as responders if they reported their symptoms as “completely relieved” or “considerably relieved” for at least 50% or “somewhat relieved” 100% of the time during the last 4 available weeks.33,43 Across the 3 trials a greater proportion of tegaserod-treated (39%, 44%,43%) compared to placebo-treated patients (28%, 39%, 38%) met the primary responder endpoint. The most common AEs reported during these trials were headache (14%), abdominal pain (11%), nausea (8%), and diarrhea (8%). Among the patients who experienced diarrhea, 84% had a single episode, typically within the first week of therapy.33
Because tegaserod is being removed from the market, pharmacists should refer patients on tegaserod to their prescriber to discuss alternative IBS-C treatment options. Patients can continue to take their medication until supplies are depleted as the product was not withdrawn due to any concerns about efficacy, safety, or an imposed recall.
Emerging Therapies
A few emerging therapies and future targets are under investigation for treating IBS-C. Mizagliflozin is a sodium-glucose co-transporter 1 inhibitor that reduces small intestinal fluid absorption by preventing glucose absorption, thereby increasing colonic fluid secretion. Another option is elobixibat, which is an ileal bile acid transporter inhibitor that accelerates colonic transit and softens the stool.7 The endocannabinoid system (ECS) has been identified as another potential treatment target. This complex network of endogenous cannabinoids, cannabinoid receptors, and regulatory enzymes is widely distributed throughout the body and may play an important role in tissue homeostasis, motor and sensory functions, and epithelial barrier integrity. The most abundant cannabinoid receptor is the CB1 receptor.44 Previously, CB1 receptor inverse agonists have been associated with diarrhea and are being considered for IBS-C treatment.7
Pharmacists Role
Patient Advocates
Unfortunately, many patients with IBS-C have significant misconceptions about the nature and prognosis of their condition. For example, they often believe anxiety, dietary factors, and depression cause their disorder.45 Patients with IBS-C are frequently reluctant to seek specialized care and follow-up for diagnosis due to the embarrassment of discussing their bowel habits with their HCP.14 Pharmacists can ease their patient's misconceptions and shame by reassuring them that their symptoms are a sign of a diagnosable disorder and that HCPs are trained to listen to their concerns, including bowel habits and associated symptoms.
Pharmacists are widely accessible, and studies have found that patients visit their community pharmacies twice as often as other HCPs.46 More frequent patient interactions give pharmacists additional opportunities to build trust, especially among patients suffering from chronic conditions such as IBS-C. Patients with IBS-C frequently report feeling frustrated.14 Using good communication skills and empathy, pharmacists can learn about patients' preferences toward their care. Pharmacists can build patient trust by explaining how IBS-C medications work, notifying them when generic versions become available, discussing both the advantages and disadvantages of the various treatment options, and setting realistic treatment expectations.
Prescribers report that cost is the primary consideration when selecting treatments for chronic conditions such as IBS. From the patient's perspective, up to 60% discontinue their medication primarily due to a lack of drug coverage and costs.47 Pharmacists can reduce these economic barriers by working with prescribers to identify formulary IBS-C treatments and facilitate the prior authorization process and by helping patients find manufacturer rebate coupons or other discount programs to reduce out-of-pocket costs.
Patient Education and Adherence
Adherence is poor among patients with IBS-C, with less than 50% of patients taking their recommended prescription medications.48 Pharmacists are uniquely positioned and trained to identify adherence issues. They should follow up with patients to ensure they are not experiencing problems related to tolerability, lack of effect, product availability, cost, or other factors that could negatively impact treatment. One online survey found that 67% of patients (n=1311) who took an IBS prescription medication stopped taking it at least once without their HCP’s advice, primarily (46%) because they forgot to take it.49 Patient education is a core pharmacist function that, when done effectively, improves patient adherence rates. Pharmacists should educate their patients on how and when to take their medication, most common AEs and what to do if these occur, contraindications, warnings, and drug interactions (Table 4).28,30-33 In addition, pharmacists should educate patients about alarm symptoms and the importance of seeking help if these occur during treatment as they may be a sign of a more serious condition.
| Table 4. Considerations for Pharmacist Dispensing US Food and Drug Administration-Approved Treatments for IBS-C |
| Medication Name (Dose) |
IBS-C Approved Population |
Generic Available?a |
Patient Administration Instructions |
Contraindications |
Adverse Events (≥5%) in IBS-C |
Drug Interactions |
Lubiprostone
(8 µg twice daily)28,b |
Women aged ≥18 years |
Yes |
• Swallow capsules whole
• Take with food and water
• Periodically assess the need for continued therapy |
Known or suspected mechanical GI obstruction |
Nausea (8%)
Diarrhea (7%)
Abdominal pain (5%) |
None |
Linaclotide29
(290 µg daily) |
Adults |
No |
• Take on empty stomach ≥30 minutes prior to first meal of the day
• Capsules can be opened and administered orally in either applesauce or water |
• <2 years of age due to risk of serious dehydration
• Known or suspected mechanical GI obstruction |
Diarrhea (20%)
Abdominal pain (7%) |
None |
Plecanatide30
(3 mg daily) |
Adults |
No |
• Take with or without food
• Tablets can be crushed and administered in applesauce or with water |
• <6 years of age due to the risk of serious dehydration
• Known or suspected mechanical GI obstruction |
None ≥5% |
None |
Tenapanor31
(50 mg twice daily) |
Adults |
No |
• Take immediately before breakfast or the first meal of the day and immediately before dinner
• Do not double up on doses if a dose is missed |
• <6 years of age due to the risk of severe dehydration
• Known or suspected mechanical GI obstruction |
Diarrhea (16%) |
May reduce exposures of OATP2B1 substrates (e.g., enalapril) |
Tegaserod32
(6 mg twice daily) |
Women aged <65 years |
N/A
Withdrawn from the US marketplace in June 2022 |
• Take ≥30 minutes before meals
• Discontinue after 4-6 weeks if patient does not have adequate control of symptoms |
• History of myocardial infarction, stroke, transient ischemic attack, or angina
• History of ischemic colitis or other forms of intestinal ischemia
• Renal or hepatic disease
• A history of bowel obstruction, symptomatic gallbladder disease, suspected sphincter of Oddi dysfunction, or abdominal adhesions
• Hypersensitivity to tegaserod |
Headache (14%)
Abdominal pain (11%)
Nausea (8%)
Diarrhea (8%)
Flatulence (6%) |
No clinically relevant interactions |
aPrior authorization requirements vary based on plan and formulary. bIn patients with severe hepatic impairment (Child-Pugh Class C), a reduced starting dose of 8 µg daily is recommended with dose escalation based on tolerability and treatment response.
GI=gastrointestinal; IBS-C=irritable bowel syndrome with constipation; N/A=not applicable. |
Case Conclusion
To help KL obtain her medicine through her insurance provider, you can facilitate the prior authorization process by empathically explaining and initiating the authorization process. You can also help KL find manufacturer rebate coupons or other discount programs to reduce her out-of-pocket costs.
Conclusions
Pharmacists caring for patients with IBS-C need to understand that this is a common chronic symptom-based and often debilitating GI disorder with no established objective diagnostic tests or biomarkers. Unfortunately, this frustrating disorder primarily affects younger adults during a critical and productive phase of their life. Although there is currently no cure for IBS-C, there are safe and effective FDA-approved treatment options to control IBS-C symptoms. By attending continuing education programs and learning about the most recent advances in IBS-C guidelines and treatments, pharmacists can stay up to date and positively impact the care of patients with IBS-C.
References
- Liu JJ, Brenner DM. Review article: current and future treatment approaches for IBS with constipation. Aliment Pharmacol Ther. 2021;54(suppl 1):S53-S62.
- Lovell RM, Ford AC. Global prevalence of and risk factors for irritable bowel syndrome: a meta-analysis. Clin Gastroenterol Hepatol. 2012;10(7):712-721.e4.
- Chang L, Sultan S, Lembo A, et al. AGA clinical practice guideline on the pharmacological management of irritable bowel syndrome with constipation. Gastroenterology. 2022;163(1):118-136.
- Yadav YS, Eslick GD, Talley NJ. Review article: irritable bowel syndrome: natural history, bowel habit stability and overlap with other gastrointestinal disorders. Aliment Pharmacol Ther. 2021;54(suppl 1):S24-S32.
- Lacy BE, Pimentel M, Brenner DM, et al. ACG clinical guideline: management of irritable bowel syndrome. Am J Gastroenterol. 2021;116(1):17-44.
- Karantanos, T, Markoutsaki T, Gazouli M, et al.Current insights in to the pathophysiology of irritable bowel syndrome. Gut Pathog. 2010;2(1):3.
- Elwing JE, Atassi H, Rogers BD, Sayuk GS. Emerging therapies in the management of irritable bowel syndrome (IBS). Expert Opin Emerg Drugs. 2022;27(1):55-73.
- Carabotti M, Scirocco A, Maselli MA, Severi C. The gut-brain axis: interactions between enteric microbiota, central and enteric nervous systems. Ann Gastroenterol. 2015;28(2):203-209.
- Mertz H, Naliboff B, Munakata J, et al. Altered rectal perception is a biological marker of patients with irritable bowel syndrome. Gastroenterology. 1995;109(1):40-52.
- Mayer EA, Gebhart GF. Basic and clinical aspects of visceral hyperalgesia. Gastroenterology. 1994;107(1):271-293.
- Chojnacki C, Błońska A, Kaczka A, et al. Evaluation of serotonin and dopamine secretion and metabolism in patients with irritable bowel syndrome. Pol Arch Intern Med. 2018;128(11):711-713.
- Bonetto S, Fagoonee S, Battaglia E, et al. Recent advances in the treatment of irritable bowel syndrome. Pol Arch Intern Med. 2021;131(7-8):709-715.
- Saha L. Irritable bowel syndrome: pathogenesis, diagnosis, treatment, and evidence-based medicine. World J Gastroenterol. 2014;20(22):6759-6773.
- Harris LA, Chang CH. Burden of constipation: looking beyond bowel movements. Am J Gastroenterol. 2022;117(4S):S2-S5.
- Holtmann GJ, Ford AC, Talley NJ. Pathophysiology of irritable bowel syndrome. Lancet Gastroenterol Hepatol. 2016;1(2):133-146.
- Klem F, Wadhwa A, Prokop LJ, et al. Prevalence, risk factors, and outcomes of irritable bowel syndrome after infectious enteritis: a systematic review and meta-analysis. Gastroenterology. 2017;152(5):1042-1054.e1.
- Galica AN, Galica R, Dumitrașcu DL. Diet, fibers, and probiotics for irritable bowel syndrome. J Med Life. 2022;15(2):174-179.
- Lacy BE, Patel NK. Rome criteria and a diagnostic approach to irritable bowel syndrome. J Clin Med. 2017;6(11):99.
- Chumpitazi BP, Self MM, Czyzewski DI, et al. Bristol Stool Form Scale reliability and agreement decreases when determining Rome III stool form designations. Neurogastroenterol Motil. 2016;28(3):443-448.
- Drossman DA, Morris CB, Schneck S, et al. International survey of patients with IBS: symptom features and their severity, health status, treatments, and risk taking to achieve clinical benefit. J Clin Gastroenterol. 2009;43(6):541-550.
- Canavan C, West J, Card T. Review article: the economic impact of the irritable bowel syndrome. Aliment Pharmacol Ther. 2014;40(9):1023-1034.
- Raskov H, Burcharth J, Pommergaard HC, Rosenberg J. Irritable bowel syndrome, the microbiota and the gut-brain axis. Gut Microbes. 2016;7(5):365-383.
- Dionne J, Ford AC, Yuan Y, et al. A systematic review and meta-analysis evaluating the efficacy of a gluten-free diet and a low FODMAPs diet in treating symptoms of irritable bowel syndrome. Am J Gastroenterol. 2018;113(9):1290-1300.
- Magge S, Lembo A. Low-FODMAP diet for treatment of irritable bowel syndrome. Gastroenterol Hepatol (N Y). 2012;8(11):739-745.
- Wall GC, Bryant GA, Bottenberg MM, et al. Irritable bowel syndrome: a concise review of current treatment concepts. World J Gastroenterol. 2014;20(27):8796-8806.
- Ford AC, Moayyedi P, Chey WD, et al. American College of Gastroenterology monograph on management of irritable bowel syndrome. Am J Gastroenterol. 2018;113(suppl 2):1-18.
- Focht M. Irritable bowel syndrome therapy removed from market (again). Medscape. June 30, 2022. Accessed July 15, 2022. https://www.medscape.com/viewarticle/976460
- Amitiza capsules [product information]. Bedminster, NJ: Sucampo Pharma Americas LLC; 2020.
- Drossman DA, Chey WD, Johanson JF, et al. Clinical trial: lubiprostone in patients with constipation-associated irritable bowel syndrome--results of two randomized, placebo-controlled studies. Aliment Pharmacol Ther. 2009;29(3):329-341.
- Linzess® capsules [product information]. Madison, NJ: Allergan USA, Inc.;
- Trulance® tablets [product information]. Bridgewater, NJ: Salix Pharmaceuticals; 2021.
- Ibsrela® tablets [product information]. Waltham, MA: Ardelyx, Inc.; 2022.
- Zelnorm™ tablets [product information]. Covington, LA: Alfasigma; 2019.
- Wechsler EV, Shah ED. Diarrhea-predominant and constipation-predominant irritable bowel syndrome: current prescription drug treatment options. Drugs. 2021;81(17):1953-1968.
- Liu JJ, Brenner DM. Focus on pharmacotherapy for irritable bowel syndrome with constipation. Gastroenterol Clin North Am. 2021;50(3):639-653.
- Chang L, Chey WD, Drossman D, et al. Effects of baseline abdominal pain and bloating on response to lubiprostone in patients with irritable bowel syndrome with constipation. Aliment Pharmacol Ther. 2016;44(10):1114-1122.
- Rao S, Lembo AJ, Shiff SJ, et al. A 12-week, randomized, controlled trial with a 4-week randomized withdrawal period to evaluate the efficacy and safety of linaclotide in irritable bowel syndrome with constipation. Am J Gastroenterol. 2012;107(11):1714-1724.
- Chey WD, Lembo AJ, Lavins BJ, et al. Linaclotide for irritable bowel syndrome with constipation: a 26-week, randomized, double-blind, placebo-controlled trial to evaluate efficacy and safety. Am J Gastroenterol. 2012;107(11):1702-1712.
- Brenner DM, Fogel R, Dorn SD, et al. Efficacy, safety, and tolerability of plecanatide in patients with irritable bowel syndrome with constipation: results of two phase 3 randomized clinical trials. Am J Gastroenterol. 2018;113(5):735-745.
- Chey WD, Lembo AJ, Rosenbaum DP. Efficacy of tenapanor in treating patients with irritable bowel syndrome with constipation: a 12-week, placebo-controlled phase 3 trial (T3MPO-1). Am J Gastroenterol. 2020;115(2):281-293.
- Chey WD, Lembo AJ, Yang Y, Rosenbaum DP. Efficacy of tenapanor in treating patients with irritable bowel syndrome with constipation: a 26-week, placebo-controlled phase 3 trial (T3MPO-2). Am J Gastroenterol. 2021;116(6):1294-1303.
- The American Gastroenterological Association. AGA issues clinical guidelines outlining drug treatment plans for patients with irritable bowel syndrome (IBS) [press release]. June 21, 2022. Accessed June 29, 2022. https://gastro.org/press-releases/aga-issues-clinical-guidelines-outlining-drug-treatment-plans-for-patients-with-irritable-bowel-syndrome-ibs/
- New 43 Novick J, Miner, P, Krause R, et al. A randomized, double-blind, placebo-controlled trial of tegaserod in female patients suffering from irritable bowel syndrome with constipation. Aliment Pharmacol Ther. 2002;16(11):1877-1888.
- New 44 Lu HC, Mackie K. An Introduction to the endogenous cannabinoid system. Biol Psychiatry. 2016;79(7):516-525. doi:10.1016/j.biopsych.2015.07.028.
- Lacy BE, Weiser K, Noddin L, et al. Irritable bowel syndrome: patients' attitudes, concerns and level of knowledge. Aliment Pharmacol Ther. 2007;25(11):1329-1341.
- Valliant SN, Burbage SC, Pathak S, Urick BY. Pharmacists as accessible health care providers: quantifying the opportunity. J Manag Care Spec Pharm. 2022;28(1):85-90.
- Shah ED, Chang L, Lembo A, et al. Price is right: exploring prescription drug coverage barriers for irritable bowel syndrome using threshold pricing analysis. Dig Dis Sci. 2021;66(12):4140-4148.
- Barberio B, Savarino EV, Black CJ, et al. Adverse events in trials of licensed drugs for irritable bowel syndrome with constipation or diarrhea: systematic review and meta-analysis. Neurogastroenterol Motil. 2022;34(6):e14279.
- Quigley EMM, Horn J, Kissous-Hunt M, et al. Better understanding and recognition of the disconnects, experiences, and needs of patients with irritable bowel syndrome with constipation (BURDEN IBS-C) study: results of an online questionnaire. Adv Ther. 2018;35(7):967-980.
Back to Top