
Expired activity
Please go to the PowerPak
homepage and select a course.
COVID-19 Monthly Update: 12 Key Questions Addressing Present and Future Use of COVID-19 Vaccines
INTRODUCTION
Nearly 18 months into the coronavirus disease 2019 (COVID-19) pandemic, much has been accomplished that will ultimately lead to a sense of normalcy, even as soon as mid-summer 2021 for most Americans. The U.S. Food and Drug Administration (FDA) has authorized 3 vaccines, including 2 mRNA vaccines manufactured by Pfizer/BioNTech and Moderna and the adenovirus vector vaccine from Janssen/Johnson & Johnson. Tremendous progress has been made in the mass vaccination efforts employed by health care providers, especially pharmacists, across the United States. As of May 2021, more than 321 million doses of vaccine have been manufactured and delivered in the United States, with 250 million vaccine doses administered. At the time this program was prepared, this represented more than 160 million patients receiving at least 1 dose (approximately 48% of population) and more than 125 million patients fully vaccinated, nearly 40% of the U.S. population. Importantly, in one of the most at-risk populations (65 years of age and older) from severe COVID-19 disease and death, 85% had received at least 1 dose while 73% had been fully vaccinated. The breakdown of received vaccinations by manufacturer consists of Pfizer/BioNTech (53%), Moderna (43%), and Janssen/Johnson & Johnson (3.6%).
While significant progress has been made to work toward herd immunity, challenges definitely remain. While the highest number of vaccines administered in the United States peaked at 4.25 million on April 1, 2021, the 7-day average has continually decreased from its peak of ~3.3 million on April 11 to less than 2 million in early May 2021. Addressing vaccine hesitancy is now of utmost importance and many questions still remain about currently authorized COVID-19 vaccines, especially the Janssen/Johnson & Johnson vaccine, as well as future potential vaccines, such as the candidates from AstraZeneca and Novavax.
This article addresses a number of important and timely questions related to COVID-19 vaccines in a question-and-answer format.
Question 1: Influenza vaccines are available in multiple dosage forms. Is there any potential for COVID-19 vaccines to be available in alternative dosage forms?
Answer: Yes. There is significant interest in evaluating alternative dosage forms for COVID-19 vaccination for several reasons. First, storage of the most widely administered vaccines (mRNA vaccines by Moderna and Pfizer/BioNTech) have difficult cold-chain temperature storage requirements and have limited shelf-lives after thawing. Second, these vaccines while extremely effective in people receiving 2 separate doses 3 or 4 weeks apart. Nonadherence with the second injection may result in less overall immunity in the population. Third, with overall vaccination rates decreasing and vaccine hesitancy a constant barrier, alternative dosage forms of vaccines could capture a segment of the population for whom injectables are not optimal due to fear of needles and other factors.
While many companies are working on additional COVID-19 vaccines, 2 companies in particular are likely to produce COVID-19 vaccines using alternative dosage forms. Vaxart Inc., based in California, is developing an oral tablet dosage form that in early studies, demonstrates immune responses with potential activity versus variants. Altimmune, a Maryland firm, is developing a nasal spray similar to FluMist that would avoid the needs for both needles and syringes. Both of these dosage forms would be optimal for children who are typically more hesitant about receiving injectable vaccines.
Question 2: Will COVID-19 vaccines be authorized by the Food and Drug Administration for younger children?
Answer: On May 10, 2021, the FDA expanded the emergency use authorization for the Pfizer/BioNTech COVID-19 vaccine for the prevention of disease in adolescents 12–15 years of age. This product was originally authorized for patients 16 years or older.
This expansion of the approved age range was based safety information obtained from clinical studies on 2,260 participants 12–15 years of age, 1,131 of whom received active vaccine in 2 doses 3 weeks apart, the same regimen approved earlier for older adolescents and adults. Among about half of the vaccinated participants in the younger age group who were followed for 2 months or longer, the most commonly listed side effects were localized injection site reactions, fatigue, headache, chills, fever, and joint and muscle pain. With the exception of injection site pain, side effects were more prevalent after the second vaccine dose. Seven children in the vaccinated group had enlarged or swollen lymph nodes compared with 1 child in the placebo group. Four cases of psychiatric disorders occurred in the vaccine arm, all in patients with previously documented diagnoses of the illness found in the study (depression) or who had been on medications before the study for the disease in question. These symptoms lasted up to 3 days in most patients.
Regarding efficacy, immune response in these participants were compared to those age 16–25 years of age in the previous study. A noninferior immune response was demonstrated in the 12–15 age group, with 0 cases of COVID-19 occurring in the active treatment arm versus 16 cases detected among the placebo participants at least 7 days after the second dose. Based on these data, the Advisory Committee on Immunization Practice (ACIP), a federal advisory panel to the CDC, recommended 2 days later that 12–15 year-olds be eligible to receive the Pfizer/BioNTech COVID-19 vaccine. The vote was 14–0, with one member recusing.
Vaccination of adolescents and children represents a potentially important step toward herd immunity, as adolescent COVID-19 cases had been increasing and making up a growing proportion of overall cases. Hospitalizations due to COVID-19 among 12–17-year-olds have exceeded historical rates for influenza, sometimes with a rare complication of multisystem inflammatory syndrome (MIS-C). Approximately 1.3% of all deaths in this age group during 2020 and the first 4 months of 2021 were attributed to COVID-19, which would make it a top 10 cause of death based on 2019 data.
Pfizer has announced plans to pursue COVID-19 vaccination authorization in patients younger than 12 years of age. If studies demonstrate efficacy and safety, authorization for children aged 2–11 years will be sought in September 2021, with data on children 6 months to 2 years of age expected to follow in the fourth quarter 2021.
Despite these data, vaccine hesitancy is an obstacle not only among adults, but also in the adolescent population and also some parents. A recent survey of 1,258 parents by the polling company Invisibly reported that 53% planned to have their children vaccinated “eventually,” but only 26% stated they would do as soon as possible once a vaccine product is authorized. One-third of respondents stated they do not plan on vaccinating their children regardless. Intensive, detailed, long-term follow-up within this population will be critical to reassure parents of tolerability and side effect considerations before vaccine rates within this population will increase. As of May 18, 2021, Dr. Rochelle Walensky, CDC director, stated that more than 4.1 million adolescents aged 12–17 years had been vaccinated in the few days following FDA approval and CDC recommendation of the Pfizer/BioNTech product.
Question 3: What are the potential risks of the Janssen/Johnson & Johnson vaccine that temporarily necessitated pausing vaccinations?
Answer: The adenovirus-vector COVID-19 vaccine by Janssen/Johnson & Johnson was recommended to be suspended by both the FDA and CDC on April 13, 2021, due to concerns over rare cases of cerebral venous sinus thrombosis (CVST) which was accompanied by thrombocytopenia. ACIP one day later recommended to continue the pause in order to further evaluate the cases and provide a longer-term recommendation. As of early April 2021, no cases of CVST with thrombocytopenia had been reported to the Vaccine Adverse Event Reporting System (VAERS) in approximately 100 million doses of the Pfizer/BioNTech vaccine. Three thrombotic cases have been reported with the Moderna vaccine in approximately 90 million vaccinations administered, but these patients had no thrombocytopenia. CVST is a rare event, occurring in 0.22-1.57 per 100,000 patients, making up only about 1% of all strokes. Females are typically more affected (3:1 ratio) with most cases occurring earlier in life with a median age of 37 years. Known risk factors include genetic or acquired prothrombotic conditions, oral contraceptive therapy, pregnancy with post-partum period, cancer, infection, and mechanical manipulation.
Most patients with CVST present with isolated intracranial hypertension syndrome (headache with or without vomiting, papilledema, and visual disturbances), focal syndromes such as seizures, or encephalopathy. Rare presentations include cavernous sinus syndrome, subarachnoid hemorrhage, or cranial nerve palsies. While all strokes can be disabling or cause death, CVST often necessitates intensive care unit admission and can cause permanent disability from neurologic sequalae or death from consumptive coagulopathy.
The initial 6 cases of CVST associated with the Janssen/Johnson & Johnson vaccine all occurred in women ages 18–48 years with symptoms beginning approximately 1–2 weeks after vaccine administration. Most patients initially presented with headache initially, and several developed severe headaches late. Of the 6 patients, 3 had extracranial thromboses, 4 developed intraparynchemal brain hemorrhage, and 1 died of complications. Notable comorbid conditions included obesity, hypertension, hypothyroidism, and asthma. One patient was receiving combination estrogen/progesterone at the time of the event.
The incidence of CVST with thrombocytopenia in these patients, as well as those patients experiencing CVST with the Oxford/AstraZeneca adenovirus-vector vaccine, has elevated serum concentrations of platelet factor 4 antibody complexes, similar to those seen with heparin-induced thrombocytopenia. Therefore, unless patients have been ruled out for these complexes via enzyme-linked immunosorbent assay (ELISA) testing, treatment with heparin or low molecular weight heparin should not be initiated when treating CVST. Alternatively, a non-heparin anticoagulant, such as argatroban, could be considered along with high-dose intravenous immune globulin.
At the ACIP meeting on April 23, 2021, the number of thromboses cases associated with the Janssen/Johnson & Johnson vaccine had been updated to 15 in approximately 8 million patients vaccinated with wide variation in location and severity of thrombotic events not only in the cerebral sinuses, but also in other locations such as the portal vein, hepatic vein, pulmonary artery, and iliac artery. In these cases, at the time of the meeting, 5 of these patients had been discharged home, 4 were in the intensive care unit, 7 remained hospitalized, and 3 had died. ACIP members voted 10–4 to recommend resumption of use of this vaccine in all patients, and the CDC and FDA concurred while adding a warning about thrombosis with thrombocytopenia syndrome (TTS).
The most common reason cited by ACIP members who voted against continuing the vaccine was the belief that stronger labeling should be against using this vaccine in younger women, the predominant population affected by CVST. For women 18–49 years of age, the estimated rate of TTS is 1 in 140,000 doses. As some have argued, with the current significant supply of mRNA vaccines available, the overall falling case numbers, and continued vaccine hesitancy not draining supply, a case for not administering the Janssen/Johnson & Johnson vaccine to most young women can be made in favor of mRNA vaccines that have a plentiful supply.
Question 4: Are any changes upcoming regarding storage or administration for the mRNA vaccines?
Answer: There are several notable updates with the Moderna vaccine. First, the FDA has authorized an increase from 10 doses per vial up to 15 doses per vial. The FDA also is allowing an 11th dose to be drawn up from 10-dose vials that remain. Moderna vaccine vials may also now be stored in a standard refrigerator for 30 days before vials are punctured, and can be kept at room temperature for 24 hours, an extension from the prior 12-hour allowance. Once the vial has been punctured for use, the provider administering the vaccine has 12 hours to administer the dose, an increase from the previous guidance of 6 hours.
For the Pfizer/BioNTech vaccine, the FDA announced that undiluted, thawed vaccine can be safely stored in a standard refrigerator for up to 1 month. This is a significant extension from the previously recommended 5 days.
To alleviate cold-storage requirements and increase vaccination rates in rural and developing countries, Pfizer/BioNTech is evaluating a lyophilized (freeze-dried) version of its mRNA vaccine. In April 2021, Pfizer initiated a study of a lyophilized formulation in approximately 1,100 U.S. adults aged 18–55 years. Study participants are being followed for 2 months to ensure safety and efficacy similar to the currently available dosage form. While the FDA in February allowed the Pfizer/BioNTech vaccine to be stored at –20° C (–4° F) for up to 2 weeks, the lyophilized dosage form would allow for storage at standard refrigeration temperatures.
Question 5: How effective are the current vaccines against the circulating variants of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)?
Answer: A number of variants that have been described over the past few months as COVID-19 has infected hundreds of millions of people worldwide. Variants appear and proliferate; other times they appear and then disappear. The most common ones discussed worldwide currently are B.1.1.7 (discovered in the United Kingdom), B.1.351 (discovered in South Africa), P.1. (discovered in Brazil), B.1.526 (discovered in New York), and B.1.429 (discovered in California). All of these variants have been found in the United States, the predominant variant is in April 2021 was B.1.1.7, with substantial numbers of other variants also present.
To date, the authorized mRNA vaccines appear to be providing significant protection but with some decrease in efficacy against these variants compared with parent strains of SARS-CoV-2. This has been demonstrated versus most of the variants listed in lab studies, randomized clinical trials, real-world evidence, or a combination of these.
A recent publication out of Qatar evaluated Pfizer/BioNTech mRNA vaccine effectiveness versus the B.1.1.7 and B.1.351 variants. Vaccine effectiveness was estimated to be 87% against the B.1.1.7 variant and 72.1% against the B.1.351 variant. Of utmost importance, vaccine effectiveness against severe, critical, or fatal disease due to either variant was 97.4%, which was confirmed with sensitivity analyses.1 The Janssen/Johnson & Johnson vaccine in particular likely had a higher number of participants with B.1.351 variants in its seminal studies, explaining some of its overall lower efficacy rates compared with earlier studies of mRNA vaccines.
Two recent studies published in the New England Journal of Medicine documented limited efficacy of the AstraZeneca/University of Oxford and Novavax vaccines against the B.1.351 variant. The vaccine efficacy versus this variant was 10.4% and 51.0% for the ChAdOx1 nCoV-19 and NVX-CoV2373 nanoparticle vaccines, respectively, in patients in South Africa who were not infected by the human immunodeficiency virus. These products have yet to be authorized for use in the United States.2,3
At the time this program was prepared, more than 200,000 new cases of COVID-19 were occurring daily in India, peaking above 400,000 on some days. Much of this rapid progression of disease is due to the specific B.1617/B.1.617.2 variant first found in India, sometimes called the “double mutant.” While limited data are available on efficacy of currently available vaccines versus this particular variant, some laboratory studies have shown benefit with the mRNA vaccines.
Overall, the data suggest reduced but significantly retained neutralizing ability of currently authorized vaccines in the United States versus the circulating variants. This is another reason to continue to push for increased vaccination rates, as more vaccinated individuals means less opportunity for viruses to mutate as well as decreased transmission. A first-step immunization study has been published in Nature working toward a pan-coronavirus mRNA nanoparticle vaccine that would have neutralizing activity against major circulating variants.4
Question 6: Do any of the COVID-19 vaccines cause infertility?
Answer: Unfortunately, this is one of the most rampant “truths” being spread on the internet in many different platforms, especially social media outlets, regarding COVID-19 vaccines. What is believed to be the genesis of these theories was a possible proposed link by a skeptical German epidemiologist named Wolfgang Wodarg. He partnered with a former Pfizer employee to petition the European Medicines Agency to delay approval of the Pfizer/BioNTech vaccine (the BioNTech main headquarters are in Mainz, Germany), primarily over a protein named syncytin-1. This protein shares similar genetic instructions with the COVID-19 spike protein and is an important component of some mammal placentas. In theory, antibodies versus the COVID-19 spike protein could result in rejection of a human placenta, causing infertility in women. This petition spread over social media including Facebook, causing the company to remove posts regarding it from antivaccination advocates from its site.
While small pieces of the same genetic code are shared by synctin-1 and COVID-19 spike protein, it is not enough to give a full match. Dr. Wodarg readily admits in his petition that “there is no indication whether antibodies against spike proteins of SARS viruses would also act like anti-syncytin-1 antibodies.” Because mRNA vaccines contain no live virus, do not contain syncytin-1, and do not encode for syncytin-1, they are very unlikely to create antibodies against syncytin-1 once administered to a patient. While pregnancy was initially an exclusion criterion within the registry trials for the Pfizer/BioNTech studies, 23 women did become pregnant during the course of the trial, 12 of these receiving the vaccine without any reported adverse effect. Similarly, in the Moderna studies, 13 pregnancies were reported to date with 6 participants receiving the vaccine while 7 received placebo. One elective and one spontaneous abortion occurred, both in the placebo arm of the study.
In a reproductive study of rabbits, 1 mL of the Janssen/Johnson & Johnson vaccine (adult dose is 0.5 mL) did not affect female fertility. Other adenovirus vaccine studies also have not demonstrated a link to infertility. The American College of Obstetricians and Gynecologists (ACOG) recommends vaccination of all eligible people, stating that “unfounded claims linking COVID-19 vaccines to infertility have been scientifically disproven.” Adenovirus vector vaccines cannot replicate following administration. Because these adenovector viruses cannot replicate intracellularly, the vaccine cannot alter DNA of the recipient and therefore cannot cause infertility.
The CDC clearly states that women trying to become pregnant now or in the future can receive a COVID-19 vaccine. In addition, routine pregnancy screening tests are not needed before COVID-10 vaccination; there is no evidence that any COVID-19 vaccine has been associated with male or female infertility.
Question 7: Have regulatory bodies made any new recommendations about vaccination during pregnancy and lactation?
Answer: This is likely one of the most common questions asked of health care providers — including pharmacists — about the currently available COVID-19 vaccines. Pregnant women with symptoms during COVID-19 infection have higher risks of ICU admission, mechanical ventilation, and mortality, compared with nonpregnant women of similar age, especially for Asian and Native Hawaiian/Pacific Islander women.5
Official recommendations from the CDC have not changed since initial recommendations were provided several months ago. Pregnant patients are eligible for vaccination under the emergency use authorization and are encouraged (but not mandated) to have a discussion with their health care provider to determine benefit/risk ratio for each individual case.
The CDC is asking women in the periconception period (within 30 days before last menstrual period) or during pregnancy to participate in the v-safe COVID-19 Vaccine Pregnancy Registry. As of May 10, 2021, more than 110,000 patients have indicated that they were pregnant at the time of receiving COVID-19 vaccination through v-safe, with nearly 5,000 of these patients officially enrolled in the v-safe COVID-19 Vaccine Pregnancy Registry. V-safe is a smartphone-based program using text messages and web surveys to provide personalized health updates and check-ins after COVID-19 vaccination. The difference in number is due to a number of factors such as delay in rollout and launch of the registry and time required for staff to contact those who identified as pregnant in v-safe.
A recent publication in JAMA has provided further evidence of immunogenicity of COVID-19 mRNA vaccines in both pregnant and lactating women.6 This exploratory, descriptive cohort study enrolled 103 women aged 18–45 years who received a Pfizer/BioNTech or Moderna COVID-19 vaccine (nonpregnant and nonlactating, pregnant, and lactating groups) and 28 women who had confirmed COVID-19 infection (22 pregnant and 6 nonpregnant). A number of humoral and cellular immune responses were elicited in the pregnant and lactating patients as well as the nonpregnant patient, including antibodies as well as CD4 and CD8 T-cells. Binding and neutralizing antibodies were detected in infant cord blood, demonstrating transfer of maternal antibodies. Of note, some strains evaluated were variants, B.1.1.7 and B.1.351 specifically, demonstrating a reduced binding and neutralizing capacity but preserving T-cell responses.
A second recent publication sheds further light on preliminary safety findings of mRNA vaccines in pregnant women.7 More than 35,000 women who received the COVID-19 vaccine before or during pregnancy were evaluated via the v-safe surveillance system, v-safe pregnancy registry, and Vaccine Adverse Effect Reporting System (VAERS). In the 3,958 women enrolled in the registry, 827 had completed pregnancy with 86.1% resulting in live births (most of whom were vaccinated during the third trimester) and 13.9% in pregnancy loss. Adverse neonatal outcomes reported included preterm birth (9.4%) and small size for gestational age (3.2%) with no neonatal deaths reported. While not a randomized trial, calculated proportions of adverse pregnancy and neonatal outcomes among vaccinated pregnant women were similar to previous studies carried out before the pandemic. Further longer-term, longitudinal studies of patients within these databases will provide better information regarding overall safety, but at this time, there is no evidence of a safety signal associated with mRNA vaccines within the pregnant population.
No specific publication efficacy or safety data to date is available for the Janssen/Johnson & Johnson vaccine within the pregnant population. While any authorized vaccine is an option for pregnant patients, concerns over increased risk of blood clots and thrombocytopenia with the Janssen/Johnson & Johnson COVID-19 vaccine, which have occurred most often in women of childbearing age, will likely lead to low utilization of this particular vaccine in this population.
Question 8: How long does immunity from COVID-19 vaccination last?
Answer: This of course is the million-dollar question, literally and figuratively as many companies who have invested in COVID-19 vaccines are preparing for the next phase of potential vaccination needs. We are still very early in the postvaccination phase, so much research is ongoing to determine ultimate need for something akin to a yearly vaccine such as influenza, or potentially a vaccine needed every few years, such as pneumococcal vaccine.
At this point there are some things we do know. We do know that the mRNA vaccines from both Pfizer/BioNTech and Moderna have vaccine effectiveness data out to 6 months that is discussed in depth in a later question. There was little antibody decline over time in those patients who received either vaccine. It is important to note that while some countries outside of the United States have adopted more of a “give 1 dose” approach to maximize initial vaccination rates, 2-dose mRNA regimens are likely the best approach to long-term immunity. The first doses provide excellent initial immunity and some long-term immunity, but the second doses tend to increase antibodies further and provide more T-cell immunity as well as memory B cell responses that will help long-term even if antibodies wane.
A lot is not known at this time about the need for booster COVID-19 vaccine. First, it is possible that some level of protection could last for years or decades. This has been documented with patients who were infected with severe acute respiratory syndrome (SARS), a different coronavirus that caused significant respiratory illness in 2003 that emerged initially in China. A recent study published in Nature demonstrated that T-cell immunity was present in these patients 17 years after infection.8 As quickly as 7 weeks after vaccination, the Pfizer/BioNTech vaccine induces memory B cells that can potentially stimulate additional antibody levels. Survivors of the Spanish flu in 1918 were able to produce antibodies from B cells nearly 100 years after that pandemic.
Second, SARS-CoV-2 variants that currently exist or could be generated through continued infection due to lack of herd immunity may be more apt to evade immunity provided by currently available vaccines. Historically, the immune system would still provide some protection, often decreasing the risk of a severe and/or fatal COVID-19 infection. Many pharmaceutical companies are working feverishly to determine/provide “boosters” to attenuate the potential effects of variants. David Topham, professor of microbiology and immunology at the University of Rochester Medical Center, has stated that boosters likely will be required for some years “out of an abundance of caution, knowing that immunity does wane in some individuals more than others.” Fortunately, with mRNA vaccine technology, rapid adaptation of vaccine is easier compared to traditional vaccines, allowing for a newer vaccine that would better protect against circulating variants.
A number of patients incorrectly believe that if they have had confirmed COVID-19 infection, vaccination is not required due to presence of immunity. While immunity is obtained after naturally occurring infection, the CDC still recommended vaccination due to variable responses after infection. This was confirmed in a recent study that found some patients demonstrating substantial antibody levels 8 months after COVID-19 infection while others had lost antibodies in as little as 3 months after infection.
The current CDC recommendation regarding vaccination is to wait until symptoms have resolved from initial COVID-19 infection. In addition, patients with confirmed COVID-19 infection who were treated with monoclonal antibodies or convalescent plasma should wait 90 days before receiving vaccination. It is important to counsel patients that the 2-shot mRNA vaccine series can produce side effects in any patient, especially with the second injection, vaccine-related adverse effects can be more pronounced in individuals who were previously infected with COVID-19. More research is needed to understand the frequency and nature of responses after infection.
Question 9: If I have been fully vaccinated, do I need to continue to physically distance or wear a mask in either indoor or outdoor settings?
Answer: The CDC made an important announcement on May 13, 2021, with regard to progressing toward postpandemic normalcy. The agency said that most people who have been fully vaccinated can resume prepandemic activities, inside and outside, without wearing a mask or physically distancing, except where required by federal, state, local, tribal, or territorial laws, rules, and regulations, including local business and workplace guidance. The definition per the CDC of fully vaccinated includes all people who are at least 2 weeks out from their second dose of an mRNA vaccine or 2 weeks out from a single dose of Janssen/Johnson & Johnson vaccine.
Two factors supported by evidence drove this decision: (1) COVID-19 vaccines are incredibly effective at preventing COVID-19 disease, especially morbidity such as hospitalization and ultimately death and (2) these vaccines protect the person vaccinated and also reduce their risk of spreading SARS-CoV-2 once vaccinated. Anthony Fauci, MD, director of National Institute of Allergy and Infectious Diseases, stated in addition that “it is very unlikely that a vaccinated person, even if there’s a breakthrough infection, would transmit it to someone else.”
There are some notable exceptions to these recommendations. First, immunocompromised patients may not be fully protected even after receiving a full-dose COVID-19 vaccination series. Therefore, discussion with their health care provider would be optimal, as these individuals may need to continue to follow pandemic restrictions with regard to physical distancing and masking. Second, crowded areas involved in transportation, — such as buses, airplanes, trains, as well as transportation hubs — would still require a mask for travel.
While breakthrough COVID-19 infections may occur, these would likely be infrequent. With vaccine hesitancy common across the country, the hope is that relaxing of restrictions for those who are fully vaccinated will encourage others to get vaccinated, bringing the country ever closer to herd immunity.
Question 10: How effective are the mRNA vaccines at protecting health care providers from COVID-19 disease?
Answer: A MMWR publication published on May 14, 2021, addresses this important question. This was a multisite, test-negative vaccine effectiveness study of health care providers across 33 U.S. sites in 25 states. As of mid-March 2021, 623 case patients and 1,220 controls had been enrolled with median ages of 38 and 37 years, respectively. Most health care providers participating in the active arm had substantial patient contact (~75%), were women (84%), and were White (64%). Vaccine efficacy was 82% versus symptomatic COVID-19 after 1 mRNA dose and 94% effective at 14 days or more after the second mRNA dose. Of note, approximately three-quarters of those patients who had been vaccinated received the Pfizer/BioNTech product, while the rest received the Moderna product.9
These data are reassuring for pharmacists who practice in the community or institutional setting where contact with vaccinated and unvaccinated individuals occurs often.
Question 11: Does the COVID-19 vaccine have to be given 14 days separately from other normally scheduled vaccines?
Answer: Until recently, the coadministration of COVID-19 vaccines with any other approved vaccine was not recommended “out of an abundance of caution,” per the CDC. Significant data have accumulated through hundreds of millions of vaccinations under the FDA authorization, leading to reconsideration of this advice.
The CDC has updated its policy, now recommending that coadministration of COVID-19 vaccines with any other approved vaccine without regard to timing. Significant experience with a number of other vaccines suggests that both from a safety and efficacy standpoint (specifically immunogenicity), no data suggest that giving vaccines separately increases the benefit with each of these outcomes.
Based on this guidance, COVID-19 vaccines may be given without regard to timing of other vaccines — including on the same day. This is particularly important in the pediatric population, as missed vaccine doses have been common during the pandemic and catch-up vaccines can now be administered in those who present for COVID-19 vaccine. Vaccines that are more likely to provide local reactions (e.g., tetanus) should be given in different limbs. If multiple injections are given in the same area, at least a 1-inch separation of sites should be provided.
Question 12: When will the currently authorized vaccines receive full FDA approval?
Answer: The mRNA vaccines by Pfizer/BioNTech and Moderna were authorized for emergency use in December 2020 by the FDA to allow for vaccinations to begin during the pandemic. Full FDA approval of these and other COVID-19 vaccines occurs after efficacy and safety data are collected and presented to the agency for its normal review.
In May 2021, Pfizer officially asked the FDA for full approval of its COVID-19 vaccine, BNT162b2. Full approval would allow for fewer restrictions on distribution and advertising, and it is likely to become the first COVID-19 vaccine fully approved for use in the United States. The FDA typically has a 60-day timeframe to deny or accept the application, followed by a nearly 1-year timeframe to conduct a standard review. Pfizer/BioNTech has formally requested a priority review considering the circumstances, which would decrease this deadline from 10 months to 6 months. Some new information compiled after the initial emergency use authorization includes data going out to 6 months after 2 doses, demonstrating a 91.3% vaccine effectiveness rate in nearly 50,000 volunteers.
Moderna’s mRNA vaccine has also demonstrated 6-month efficacy and safety data with a 6 month vaccine effectiveness rate of >90%.Moderna plans to file formally with the FDA for full approval in late May 2021, as stated during their latest quarterly earnings call.
Full approval would be an important message to vaccine-hesitant people who question the rapidity of development and emergency use authorizations for these products. Since the United States appears unlikely to achieve full herd immunity based on current vaccination rates, particularly in some parts of the country (Figure 1), SARS-CoV-2 could well become an endemic virus for which boosters will be needed for the foreseeable future. The more people who are vaccinated, the less likely that will be, and the odds will be reduced that more infectious or pathogenic mutants will emerge. That would good news.
Figure 1. Total Doses of COVID-19 Vaccine Administered by State/Territory per 100,000 of Total Population
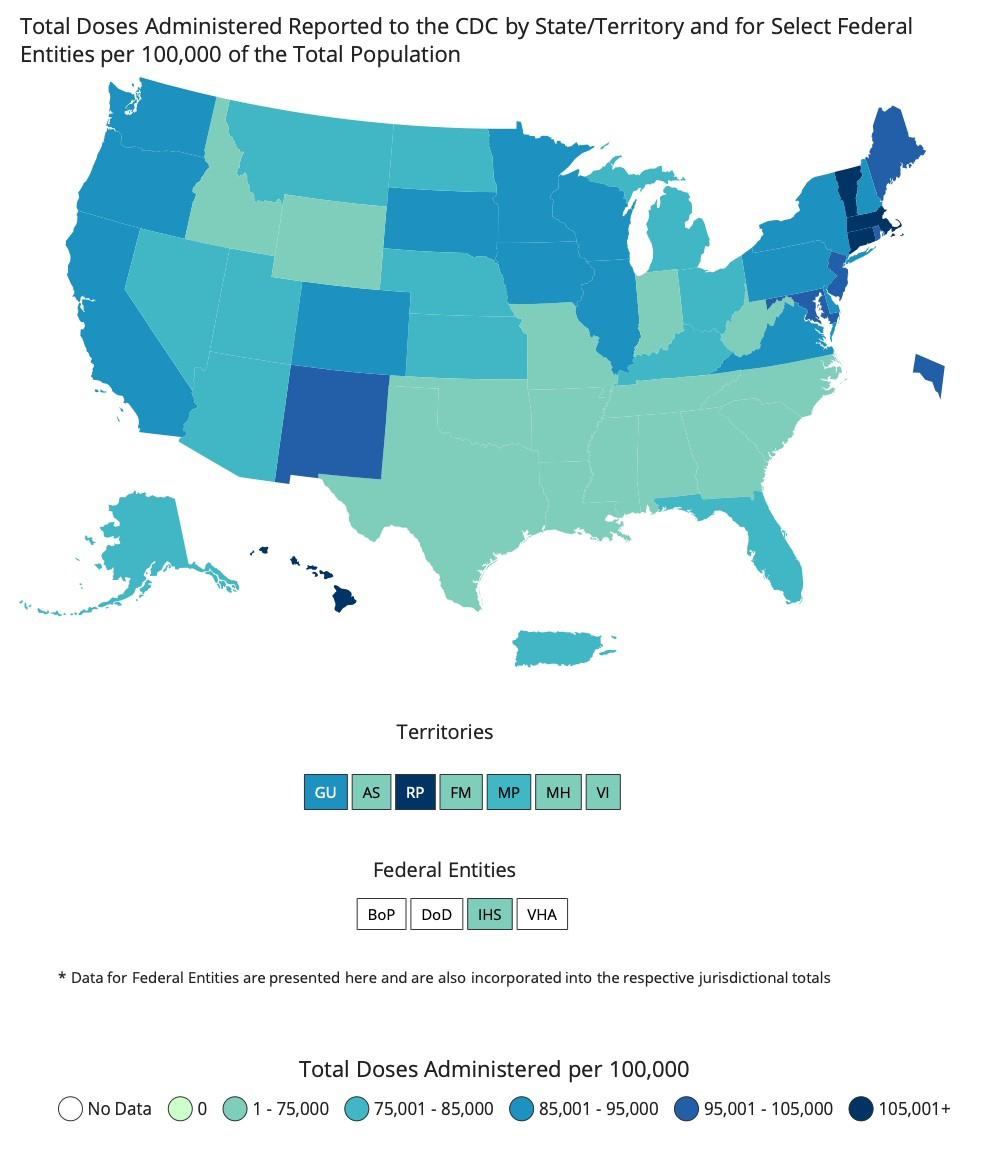
Note: The 2 most commonly used COVID-19 vaccines require 2 doses for full vaccination. This figure tracks doses, not fully vaccinated individuals.
Source: Centers for Disease Control and Prevention.
REFERENCES
- Abu-Raddad LJ, Chemaitelly H, Butt AA; National Study Group for COVID-19 Vaccination. Effectiveness of BNT162b2 Covid-19 vaccine against the B.1.1.7 and B.1.351 variants. N Engl J Med. 2021 May 5; 10.1056/NEJMc2104974
- Madhi SA, Baillie V, Cutland CL, et al. Efficacy of the ChAdOx1 nCoV-19 Covid-19 vaccine against the B.1.351 variant. N Engl J Med. 2021;384:1885–1898.
- Shinde V, Bhikha S, Hoosain Z, et al. Efficacy of NVX-CoV2373 Covid-19 vaccine against the B.1.351 variant. N Engl J Med. 2021;384:1899–1900.
- Saunders KO, Lee E, Parks R, et al. Neutralizing antibody vaccine for pandemic and pre-emergent coronaviruses. 2021 May 10; 10.1038/s41586-021-03594-0
- Zambrano LD, Ellington S, Strid P, et al. Update: characteristics of symptomatic women of reproductive age with laboratory-confirmed SARS-CoV-2 infection by pregnancy status—United States, January 22–October 3, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(44):1641–1647.
- Collier AY, McMahan K, Yu J, et al. Immunogenicity of COVID-19 mRNA Vaccines in Pregnant and Lactating Women. JAMA. 2021 May 13, 2021; 10.1001/jama.2021.7563.
- Shimabukuro TT, Kim SY, Myers TR, et al. Preliminary findings of mRNA Covid-19 vaccine safety in pregnant persons. N Engl J Med. Published online April 21, 2021. Doi: 10.1056/NEJMoa2104983.
- Le Bert N, Tan AT, Kunasegaran K, et al. SARS-CoV-2-specific T cell immunity in cases of COVID-19 and SARS, and uninfected controls. Nature. 2020;584:457-62.
- Pilishvili T, Fleming-Dutra KE, Farrar JL, et al. Interim estimates of vaccine effectiveness of Pfizer-BioNTech and Moderna COVID-19 vaccines among health care personnel—33 U.S. sites, January–March 2021. MMWR Morb Mortal Wkly Rep. ePub: 14 May 2021.
Back to Top