
Expired activity
Please go to the PowerPak
homepage and select a course.
Conceiving Confidence: Maximizing the Pharmacy Team’s Role in Infertility Treatment
INTRODUCTION
Reproduction is a unique, hormone-regulated process with many checks and balances. The capacity to conceive and produce offspring is not a given for everyone. Infertility—a diminished capacity to bear offspring—affects 1 in 8 couples and has always been a social stigma.1 Clinically, infertility is defined by the inability to conceive (get pregnant) after 1 year or longer of unprotected heterosexual intercourse.2 This issue is unfortunately common, as about 10% of men and 13% of women are afflicted with infertility.3
Being unable to fulfill the biological role of parenthood can be a socially, mentally, and physically damaging experience. Inability to conceive children is stressful and often heartbreaking.4 For many, infertility becomes the focal point of daily conversations and tasks, often to the point of excluding other important aspects of life. Luckily, science has come a long way in helping infertile individuals to conceive and many options exist for those struggling.
Assisted reproduction encompasses a range of technologies used to enhance the probability of becoming pregnant after collection and direct handling of oocytes, sperm, and/or resulting embryos outside the body.5 The first baby born through in vitro fertilization (IVF) was Louise Brown in 1978 thanks to British medical researcher Robert Edwards and gynecologist Patrick Steptoe.6 Edwards later won a share of the 2010 Nobel Prize for his work developing IVF technique. Over the following 3 decades, IVF and other assisted reproductive technologies produced about 5 million babies worldwide.
Pharmacists and pharmacy technicians will likely encounter couples undergoing fertility treatment, given its high prevalence. Understanding the medications and procedures involved in assisted reproduction is important to empathize and provide optimal patient care.
Where Do Babies Come From?
Getting pregnant involves successful completion of complex physiologic events, but at a minimum it requires5
- production of competent sperm
- production and ovulation of a competent oocyte (egg)
- sperm proximity to the oocyte in the reproductive tract
- embryo transport into the uterine cavity
- embryo implantation into the endometrium (uterine wall)
To understand how pregnancy occurs, first consider a woman’s menstrual cycle. The first day of menstruation (bleeding) is cycle day 1, and typical cycle length ranges from 21 to 40 days.7 Contrary to popular perception, a woman’s menstrual cycle is rarely 28 days long. In fact, only about 13% of women experience a 28-day cycle naturally.8 Hormones regulate the menstrual cycle (see Figure 1), and fluctuations split the menstrual cycle in to 3 phases: follicular (before egg release), ovulatory (egg release), and luteal (after egg release). During the follicular phase—day 1 to about day 14 (based on a 28-day cycle)—follicle stimulating hormone (FSH) rises to recruit a small number of follicles for growth and development. Between days 5 and 7, one follicle becomes dominant and secretes estrogen to signal the body to stop menstrual flow. Around day 14, sustained FSH levels cause LH to surge, and 28 to 32 hours later, this surge causes ovulation (release of the mature oocyte).7 The egg then travels down the woman’s fallopian tube towards the uterus.
Figure 1. Hormonal Regulation of the Menstrual Cycle5,7
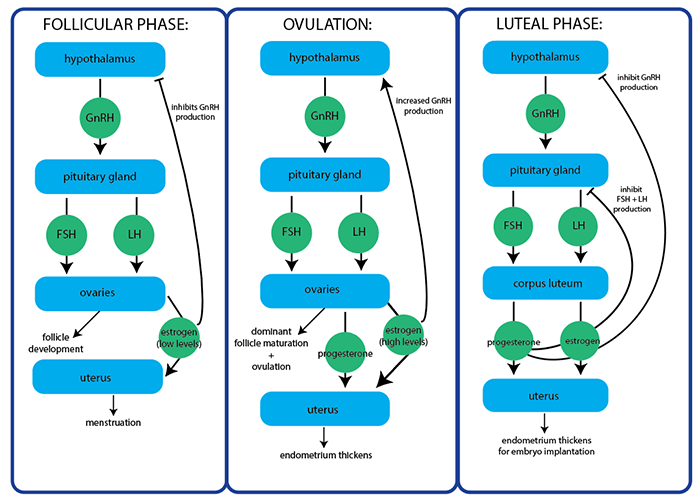
FSH, follicle-stimulating hormone; GnRH, gonadotropin-releasing hormone; LH, luteinizing hormone
It takes an egg about 30 hours to travel the 7 to 12 centimeters from an ovary to the end of the tube.3 For natural conception, a competent sperm must swim up through a woman’s vagina and uterus to join with the oocyte as it travels down one of the fallopian tubes. Additionally, if any sperm were waiting in the reproductive tract before ovulation occurred (they can survive there for about 5 days), those sperm can fertilize the egg.3 Sperm binding to the egg relies on the acrosome reaction.9 The acrosome is a structure at the sperm’s head that contains enzymes that break through the egg’s coating, zona pellucida (ZP). ZP is a mixture of sugars and proteins surrounding the egg’s outer membrane. Sperm binding to the ZP triggers enzymatic reactions that create a “lock and key” recognition, causing the acrosome to release enzymes. Once a sperm has traversed the ZP, it expels different enzymes to harden the ZP, hindering other sperm from penetrating.9 The likelihood of conception when sexual intercourse occurs the day before ovulation is similar to when intercourse occurs on the day of ovulation (about 40%).5
The remainder of the menstrual cycle is the luteal phase. During this phase, the remaining follicles that developed but did not release an egg form a structure called the corpus luteum.7 The corpus luteum produces progesterone to prepare the uterus for embryo implantation. If fertilization fails to occur, the corpus luteum degenerates and progesterone production declines, triggering menstruation to begin. However, if conception occurs, human chorionic gonadotropin (hCG) produced by the fertilized embryo prevents corpus luteum regression so it continues producing hormones to maintain pregnancy.7 Pregnancy tests (serum or urine) detect an hCG increase, indicating presence of a fertilized embryo.
A fertilized egg, however, does not always equal successful conception. Only about 40% of fertilized eggs successfully implant into the uterine lining.3 (This data is hard to come by, so estimates in the literature may vary.) It takes about 6 days for a fertilized embryo to travel into the uterus, where it burrows into the uterine lining. On average, fertilized eggs implant 6 to 10 days after conception in the fallopian tube.3 A study of about 3,000 couples in the U.S. trying to conceive found that about 58% conceived within 6 months and 75% conceived within a year.10 As participants were not instructed how to time intercourse, this is likely representative of what is expected in real-world scenarios. In another study of couples using cycle tracking and timed intercourse, about 38% conceived within 1 month, 68% within 3 months, 81% within 6 months, and 92% within 12 months.11 Patients should typically see a fertility specialist after 1 year of trying to conceive.2 This window decreases to 6 months for women over 35 years old or with a known condition affecting fertility.
Miscarriage
Clinical miscarriage—defined as a pregnancy loss after positive hCG and ultrasound confirmation—is a common, distressing early pregnancy complication.12 It generally represents a failure of normal embryos to progress to viability.
Overall, researchers state that up to two-thirds of all fertilized oocytes do not produce a live birth.12 About 30% of preclinical losses (pregnancy loss before ultrasound confirmation) occur pre-implantation and 30% occur post-implantation. Another 10% of pregnancies end in clinical miscarriage and only 30% end in a live birth.12 Age is a significant factor to consider when discussing miscarriage rates. About 10% of pregnancies in women aged 20 to 24 years end in early clinical miscarriage, compared with 51% in women aged 40 to 44 years and 53% of those 45 years and older.12,13
It is an accepted assumption that sporadic pregnancy loss occurring before an embryo has developed represents a “physiological phenomenon.” In other words, the body prevents conceptions affected by structural abnormalities or serious chromosomal aberrations incompatible with life from progressing to viability.12 Pharmacy teams who encounter people who have experienced a miscarriage should direct them to their obstetrician/gynecologist for support.
CAUSES OF INFERTILITY
Infertility can result from abnormalities in the male or female reproductive system. Infertility evaluation focuses on irregularities in 5 major processes5:
- Competent oocyte production (e.g., anovulation, depletion of oocyte pool, poor oocyte function or quality)
- Reproductive tract transport of sperm, oocyte, and/or embryo (e.g., tubal, uterine, cervical, or peritoneal factors)
- Embryo implantation (e.g., early embryo development or embryo-endometrial interactions)
- Sperm production
- Other conditions (e.g., immunological factors that can affect many components of the reproductive process)
The most common causes of infertility are abnormal semen parameters, ovulation problems, endometriosis, pelvic adhesions, and tubal disease.5 Many couples, however, are infertile with no identifiable cause, referred to as unexplained infertility. Known risk factors for male and female infertility are the same: alcohol and/or tobacco use, being over- or underweight, older age, and over-exercising.
Female Causes
Oocyte production disorders commonly cause infertility. Polycystic ovary syndrome (PCOS) is the leading cause of anovulatory (lack of ovulation) infertility, as 75% to 85% of women with PCOS have some degree of ovulation dysfunction.5 Understanding of this condition has evolved over decades and will likely be defined further in years to come. PCOS currently refers to a multisystem reproductive-metabolic disorder. The cardinal signs and symptoms of PCOS are5
- evidence of excess androgen (e.g., acne, elevated testosterone levels, excess hair growth)
- irregular menstrual bleeding (e.g., infrequent, irregular, or prolonged menstrual cycles)
- polycystic ovaries (i.e., numerous small collections of fluid [follicles] on imaging)
- weight gain (sometimes)
Women with PCOS who have regular menstrual cycles can also be anovulatory. In normal-weight patients with PCOS, endocrine events cause the ovulatory dysfunction. However, obesity often accompanies this condition, adding metabolic factors (e.g., abnormal glucose-insulin homeostasis) that pose additional risks for anovulation.5 Weight loss can restore ovulation and fertility in many obese patients with PCOS but not in normal-weight women with PCOS.
Other causes of ovarian dysfunction include5,13,14
- Diminished ovarian reserve: A woman is born with all the oocytes she will ever have already present in the ovaries. Over her lifetime, the number of available oocytes for ovulation declines. If a woman’s FSH is elevated, she likely has diminished ovarian reserve.
- Functional hypothalamic amenorrhea: Psychological stress, intense exercise, and/or disordered eating results in gonadotropin releasing hormone (GnRH) suppression, which decreases the amount of FSH and LH released from the anterior pituitary. This impaired feedback mechanism causes ovarian cells to cease estrogen production, resulting in anovulation and infertility.
- Improper hypothalamus or pituitary gland function: The hypothalamus is responsible for GnRH release, which then stimulates the pituitary gland to secrete FSH and LH. If either of these is functioning improperly, it disrupts this feedback loop and ultimately ovulation.
- Premature ovarian insufficiency: Menopause occurring before the age of 40 (i.e., the ovaries stop working and menstruation ends) affects about 10% of amenorrheic women. While research has identified many causes (e.g., chemotherapy/radiation, genetics), it is often idiopathic (no identified cause).
Fallopian tube inflammation—referred to as salpingitis—can result from infections in the pelvic area (e.g., vaginal or cervical) including sexually transmitted infections like gonorrhea or chlamydia.15 Ruptured appendicitis can also cause salpingitis. Previous salpingitis can cause hydrosalpinx, a fallopian tube blocked with watery fluid. Hydrosalpinx blocks the transport of eggs, sperm, or embryos through the fallopian tube(s), leading to infertility.
A reproductive endocrinologist (RE) will often complete a radiologic procedure called hysterosalpingography (HSG) to determine if a patient’s fallopian tubes are obstructed.15 The RE administers a contrast medium through the cervix into the reproductive tract. They then use an ultrasound to detect the contour and morphology of the uterine cavity, cervical canal, and fallopian tubes. Although this procedure is diagnostic, the flushing effect of the contrast media may also be therapeutic for clearing tubes and allowing conception to occur.15 This procedure typically occurs between days 7 and 10 of the menstrual cycle, after bleeding ends (endometrium is thin) but before ovulation occurs (ensures the patient is not pregnant). Patients may require antibiotics 1 day before through a few days after an HSG to prevent infection, and an RE may prescribe steroid premedication in asthmatics due to the use of contrast dye.15
Some REs use a saline infusion sonohysterogram as a less invasive diagnostic option for patients with abnormal uterine bleeding, infertility, or recurrent miscarriage.16 For this procedure, the RE places a transvaginal ultrasound probe in the vagina, then uses a catheter to fill the uterus with saline. This inflates the uterus so that the provider can see any structural abnormalities in the uterine walls and cavity, including fibroids, polyps, or scar tissue.16
An HSG or saline infusion sonohysterogram can detect abnormal tissue growth or uterine contour affecting fertility. Endometriosis is an estrogen-dependent, chronic inflammatory disease that causes endometrial tissue growth outside the uterine cavity. The incidence of endometriosis is 10-fold higher in women with infertility (20% to 50%) than those without (0.5% to 5%).17 Aside from infertility, endometriosis can also cause debilitating symptoms, including dysmenorrhea (menstrual pain), non-menstrual pelvic pain, and dyspareunia (painful intercourse). HSG can also help an RE find uterine fibroids, which are the most common benign tumors in women of reproductive age.18 Uterine fibroids can cause abnormal uterine bleeding, bowel dysfunction, dyspareunia, low back pain, pelvic pressive, and urinary frequency, urgency, and/or retention. Presence of these abnormal growths can impair a woman’s ability to conceive and carry a child to full term.
Male Causes
Under normal conditions, the male reproductive system makes, stores, and transports sperm, and hormones regulate this process.19 The testicles, found in the scrotum, produce sperm and testosterone. Sperm then leave the testicles to enter the epididymis (a tube behind each testicle). Just before ejaculation, sperm leave the epididymis to enter another set of tubes called the vas deferens, which joins the ejaculatory duct from the seminal vesicle. When ejaculation occurs, sperm mix with fluid from the prostate and seminal vesicles to form semen, which then travels through the urethra to exit the body.19
Sometimes, testicular or ejaculatory function is impaired, leading to male factor infertility. Varicoceles—swollen veins in the scrotum, which houses the testicles—are present in about 16% of men, but they are more common in infertile men (40%).19 These harm sperm growth because they block proper blood drainage, which can cause blood to flow back into the scrotum from the stomach. This creates an environment too warm for making sperm, leading to low sperm numbers.19 Repeated infections, surgery (e.g., vasectomy), swelling, or developmental defects can cause obstruction of sperm transport. Any part of the male reproductive tract can be blocked, causing sperm to become trapped and unable to leave the body during ejaculation.19
REs complete a sperm analysis to gather information about sperm quantity and quality.19 Upon obtaining an ejaculate sample, they will evaluate sperm volume, number of sperm present, concentration, motility (i.e., movement), and morphology (i.e., structure). REs will perform this test at least twice if sperm numbers are abnormal.19
Genetics can affect sperm production in men, most commonly those with azoospermia (i.e., no sperm in the ejaculate fluid). One of these genetic conditions is Klinefelter’s syndrome, a chromosomal variation causing an extra X chromosome in males (sometimes referred to as XXY).20 This genetic disease is not inherited, rather a nondisjunction error that randomly occurs during sex chromosome division in the egg or sperm. The extra X chromosome usually results in primary testicular failure, leading to androgen deficiency and infertility. Many environmental factors can also impair sperm production, function, and delivery, including19
- anabolic steroid use
- cigarette smoking
- diabetes
- heavy alcohol use
- heavy metal, pesticide, or radiation exposure
- history of mumps infection
- marijuana and other recreational drugs
MEDICATIONS TO TREAT INFERTILITY
Ovulation-Inducing Drugs
About 25% of infertile women have problems with ovulation, including those who ovulate less often or not at all.21 For anovulatory women, the goal is to develop and ovulate one follicle.22 Follicle development requires FSH and LH, so REs can utilize oral agents, including clomiphene or letrozole, to stimulate the pituitary gland to release FSH and LH. They can also utilize gonadotropin (FSH and/or LH) injections, but they often reserve these for women who are unresponsive to oral therapies and those requiring assisted reproductive procedures. Final follicular maturation and ovulation requires an LH surge, which some patients achieve through hCG injection.22 For medication examples from each class discussed, see Table 1.
| Table 1. Common Medications Used for In Vitro Fertilization5,21,23,24 |
| Ovarian Stimulation |
| Follicle stimulating hormone (FSH) |
· urofollitropin (urinary-derived)
· follitropin alpha (recombinant)
· follitropin beta (recombinant) |
| Luteinizing hormone (LH)* |
· lutropin alpha (recombinant) |
| Human chorionic gonadotropin (hCG) |
· chorionic gonadotropin (urinary-derived)
· choriogonadotropin alfa (recombinant) |
| Human menopausal gonadotropin (hMG) |
· menotropins for injection (multiple products, all urinary-derived) |
| Oral alternatives |
· clomiphene citrate (nonsteroidal estrogen agonist-antagonist)
· letrozole (aromatase inhibitor)** |
| Preventing Premature Ovulation |
| Gonadotropin-releasing hormone (GnRH) agonists |
· goserelin acetate
· leuprolide acetate**
· nafarelin acetate |
| GnRH antagonists |
· ganirelix acetate
· cetrorelix acetate |
| Luteal Phase Support |
| Progesterone supplementation |
· progesterone in oil injection
· vaginal progesterone |
| Other supplements (less evidence for use) |
· estrogen
· low-dose aspirin
· doxycycline
· methylprednisolone |
| *used in conjunction with FSH, not alone; **not approved for this indication |
Clomiphene Citrate
Clomiphene citrate is a nonsteroidal estrogen agonist-antagonist used first line for infertile women with infrequent or absent ovulation.22 The U.S. Food and Drug Administration (FDA) approved clomiphene for this indication in 1967, and it has a proven track record as a safe fertility medication.25,26 In the hypothalamus, clomiphene blocks estrogen production to trigger the hypothalamus to release GnRH, which stimulates pituitary gland release of FSH and LH. This catalyzes egg follicle maturation, increasing the chance of ovulation.26 About 80% of anovulatory women taking clomiphene will ovulate, but only 10% to 13% will get pregnant per cycle, so multiple cycles are often required for success.25
Patients take 50 mg of clomiphene orally at bedtime for 5 days starting between days 2 and 5 of the menstrual cycle.26 Most patients will ovulate after the first cycle, but if they don’t, providers can increase the second cycle to 100 mg daily for 5 days. If ovulation does not occur after 3 courses of treatment, further clomiphene is not recommended. Additionally, if 3 ovulatory responses occur but the patient does not conceive, further treatment is not recommended. Patients should not use clomiphene long-term (i.e., beyond a total of 6 cycles).26 The drug’s manufacturer does not recommend doses over 100 mg daily.26 However, the American Society for Reproductive Medicine (ASRM) indicates a maximum dose of 200 mg daily, and doses over 200 mg are not helpful.21 Providers should consider other options for women who do not ovulate using 200 mg.
Clomiphene’s adverse effects include abnormal uterine bleeding, breast discomfort, gastrointestinal disturbances, headaches, hot flashes, mood swings, and visual changes.22,26 Rarely, women experience ovarian hyperstimulation syndrome (OHSS; see Stimulation Sidebar), and ovarian cancer risk is higher for patients who use clomiphene for 12 or more cycles. No drug interactions with clomiphene have been documented.26 Women should understand that clomiphene will not increase the chance of pregnancy if infertility factors are unrelated to ovulation, such as blocked fallopian tubes, ovarian failure, or male factor infertility.25 Additionally, clomiphene’s tendency to cause more than one egg to ovulate increases the chance for multiple births (e.g., twins, triplets). Clinical trials showed the incidence of multiple pregnancies was 7.98% (6.9% twin, 0.5% triplet, 0.3% quadruplet, and 0.1% quintuplet), and this risk is dose dependent.25,26
Stimulation Sidebar: Recognizing Ovarian Hyperstimulation Syndrome22,27
Ovarian hyperstimulation syndrome (OHSS) is a serious adverse effect of fertility medications that should not be ignored. It results from excessive response to medications used to make eggs grow, especially injectable gonadotropins but potentially clomiphene or GnRH analogs. OHSS occurs due to a large number of growing follicles along with high estrogen levels in the body, and symptoms typically appear a few days after ovulation. The ovaries swell and leak fluid into the abdomen causing abdominal distention, nausea, pelvic discomfort, and vomiting. OHSS can be mild, moderate, or severe, and providers determine the degree of OHSS by ultrasound measurement of ovary size. In the most severe cases, OHSS causes vascular permeability and ascites, potentially leading to blood clots, decreased renal perfusion, hypovolemia (decreased blood volume), hyperkalemia (high potassium levels), and respiratory difficulty. Rarely, it can be fatal.
Advise women to seek medical attention if they experience the following symptoms after ovarian stimulation:
- abdominal swelling
- continued nausea and/or vomiting
- decreased urination
- difficulty breathing
- difficulty tolerating fluids
- facial numbness
- lower extremity swelling
- sudden abdominal pain onset
- weight gain more than 3 pounds in 2 days
- weakness
Superstitious Sidebar
Pharmacists and technicians should not be surprised if they encounter a clomiphene prescription for a male patient. Men require FSH to support sperm maturation during spermatogenesis (sperm synthesis) and LH to increase testosterone levels.28 Male patients whose low sperm count stems from low testosterone production can take clomiphene off label to support this process. The typical starting dose for this use is 25 mg daily.28
Aromatase Inhibitors
Letrozole is a nonsteroidal inhibitor of aromatase, the enzyme that converts androgens (e.g., testosterone) to estrogen.22,29 REs use this drug off-label for ovulation induction.29 Similar to clomiphene, letrozole suppresses estrogen production. In response, the pituitary gland releases FSH and LH, triggering ovarian follicle development. The most common dose of letrozole is 2.5mg once daily on days 5 through 9 of the menstrual cycle, but some patients take 5 mg or 7.5 mg daily.22,29 As REs use letrozole off-label for ovulation induction, the manufacturer makes no recommendation about a maximum number of cycles. Providers are left to use professional judgement to determine a cycle limit. Patients with breast cancer take letrozole daily, so some providers may be comfortable with longer-term letrozole use.
About 65% to 80% of anovulatory women taking letrozole will ovulate.22 Some women who cannot tolerate clomiphene’s adverse effects find letrozole more tolerable.29 In 2005, fertility doctors in Canada raised concerns about letrozole-related birth defects.29 However, letrozole has a short half-life in the bloodstream and is cleared from the system long before a fertilized embryo is present, making related fetal abnormalities unlikely.29 In fact, the ASRM indicates that providers can confidently advise patients that ovulation-inducing medications are not associated with increased risk of birth defects.21 Rarely, REs use other aromatase inhibitors (e.g., anastrozole) to induce ovulation, but no aromatase inhibitor is FDA approved for this indication.22
Injectable Gonadotropins
Women of advanced fertility age (35 years or older) or those who have not become pregnant after oral treatment may use injectable gonadotropins for ovulation induction.21,30 These injectable preparations contain FSH alone or in combination with LH. Combination FSH and LH products are referred to as menotropins or human menopausal gonadotropin (hMG). Rather than working with the brain to simulate the ovaries, gonadotropins work directly on the ovaries to develop multiple follicles.30 Patients—especially those of advanced fertility age or those with diminished ovarian reserve—may be concerned that gonadotropins may “use up” more eggs than a nonmedicated menstrual cycle. Rather than “wasting” eggs, gonadotropins actually rescue the eggs that would normally die off, allowing them to mature and become available for retrieval (discussed later) or conception.21
OHSS is the most serious adverse effect of FSH and LH supplementation, requiring hospitalization in up to 2% of gonadotropin cycles.21,30 Patients can also experience abdominal pain, breast tenderness, headache, injection-site reactions, mood swings, and nausea.21,30 Mood swings with gonadotropin injections are generally milder than those seen with clomiphene use. It is difficult, however, to separate the emotional changes caused by hormone fluctuations from the stress associated with infertility treatment.21 Also, the risk of multiple births is 30% when patients use injectable gonadotropins alone or with intrauterine insemination compared with 1% to 2% in naturally-occurring pregnancies.30
Most patients undergoing fertility treatment also inject hCG, which is structurally similar to LH, to induce final follicular maturation and ovulation.22 Injecting hCG subcutaneously or intramuscularly also stimulates the ovaries to produce progesterone, which is important for the uterus to prepare for embryo implantation.23 If too many follicles develop or estrogen levels are too high, an RE may withhold hCG injection to reduce the risk of OHSS or a high-order (i.e., more than twins) multiple pregnancy.21
Bromocriptine and Cabergoline
Some women do not ovulate regularly because they have hyperprolactinemia, meaning their pituitary gland secretes too much of the hormone prolactin.21 The presence of too much prolactin inhibits FSH and LH release, thus disrupting development of a dominant follicle and subsequent ovulation. Hyperprolactinemia has many causes, including21
- an adenoma (benign tumor composed of prolactin-secreting cells)
- use of certain drugs (e.g., alcohol, hallucinogens, oral contraceptives, painkillers, tranquilizers)
- kidney or thyroid disease
Patients can take bromocriptine or cabergoline to reduce the amount of prolactin secreted by the pituitary gland.21 Prolactin levels in the blood return to normal in about 90% of patients who take these drugs, and about 85% will ovulate and can become pregnant if no other infertility causes are present.21 Patients take bromocriptine once daily or cabergoline twice daily, and they discontinue treatment upon conceiving. Women whose prolactin levels return to normal but fail to ovulate may concurrently use clomiphene citrate or gonadotropins to trigger ovulation.21
Adverse effects of bromocriptine and cabergoline include dizziness, drowsiness, fainting, fatigue, headaches, hypotension, nasal congestion, nausea, and vomiting.21 These are dose-dependent, so providers should start patients at a low dose and titrate it up slowly to prevent them. Providers can adjust doses to minimize or eliminate adverse effects should they occur. Unlike other ovulation-inducing medications discussed, bromocriptine and cabergoline do not increase the risk of multiple-order pregnancies when taken without other fertility medications.21
GnRH Analogs
The hypothalamus naturally releases small amounts of GnRH about every 90 minutes.21 This pulsatile release stimulates the pituitary gland to release FSH and LH. GnRH analogs (including agonists and antagonists) are synthetic hormones similar to naturally-occurring GnRH that are chemically modified to make them last longer in the body. REs use these to prevent spontaneous natural ovulation in women undergoing reproductive procedures.
GnRH agonists—including nafarelin acetate and goserelin acetate—do not mimic the body’s natural rhythmic GnRH release, rather they provide constant exposure. Leuprolide acetate is a GnRH agonist not FDA-approved for infertility treatment, but REs use it off label for this indication.23 Ongoing exposure produces an initial FSH and LH increase followed by a decline in further release, therefore preventing spontaneous ovulation.21 Advantages to using GnRH agonists during assisted reproduction include23
- suppressing a patient’s natural hormone production to make ovarian stimulation easier to regulate
- increasing the number of available mature oocytes
- decreasing risk of a premature LH surge that would cause procedure cancellation
- creating flexibility in procedure scheduling due to the ability to suspend ovarian function temporarily
GnRH antagonists—including ganirelix acetate and cetrorelix acetate—suppress FSH and LH production without the initial rise seen with GnRH agonists.21 Of note, while the oral GnRH antagonists relugolix and elagolix are available in the U.S., these are FDA approved for prostate cancer and endometriosis pain, respectively.31,32 REs do not use them as fertility treatments.
GnRH agonists and antagonists have similar adverse effect profiles which vary with time.21 Temporary adverse effects include hot flashes, mood swings, and vaginal dryness. Long-term use of GnRH analogs may cause bone loss, decreased breast size, headaches, insomnia, and painful intercourse. All of these adverse effects resolve with medication discontinuation as the effects on the pituitary gland are reversed.21
Insulin-Sensitizing Agents
About 70% of women with PCOS experience insulin resistance and hyperinsulinemia (high insulin levels in the blood) due to increased weight.33 Hyperinsulinemia may contribute to excess testosterone production and can lead to ovulatory issues. Some will benefit from insulin-sensitizing agents, such as metformin. While it is not FDA approved for this indication, metformin taken alone for 4 to 6 months can cause regular menstrual period and ovulation in some women with PCOS.21 Additionally, some women with PCOS who are clomiphene resistant may respond to clomiphene in combination with metformin.
Metformin’s most common adverse effect is gastrointestinal irritation (e.g., diarrhea, nausea), which usually improves after a few weeks of use.33 A rare but serious adverse effect is lactic acidosis, a buildup of acid in the blood stream due to inefficient metabolism. Patients taking metformin should monitor for abdominal pain, deep and rapid breathing, heart-rhythm disturbances, lethargy, and vomiting, which can be signs of lactic acidosis.33 Other insulin-sensitizing agents (e.g., pioglitazone, rosiglitazone) have also been used off label in women with PCOS.
LIFESTYLE CHANGES AND COMPLEMENTARY AND ALTERNATIVE MEDICINE
Infertility treatment is expensive and can be cumbersome. This leads patients to seek lifestyle changes that may help them avoid formal treatment or increase their chances of conceiving through assisted reproduction. Diet is often the first place that patients make changes, especially those who are overweight or obese. Antioxidant-rich foods (e.g., fruits, grains, nuts, vegetables) are good for men and women. Antioxidants like beta carotene, folate, lutein, vitamins C and E, and zinc deactivate free radicals in the body that could damage sperm and egg cells. Insulin resistance can affect ovulation (especially in patients with PCOS), so eating a bigger breakfast while reducing the size of dinner could also help. Cutting down on carbohydrates, especially refined ones, can also help with insulin resistance issues.34
A ketogenic diet—high in fat, moderate in protein, low in carbohydrates—is all the rage for weight loss, but it may also help with hormone balance.35 Dramatically reducing carbohydrate intake forces the body to become more efficient at burning fat for energy instead. Initially, this shift can enhance weight loss and reduce systemic inflammation that could hinder fertility. Over time, a properly followed ketogenic diet can reduce insulin levels and possibly regulate reproductive hormone levels, including FSH, LH, and testosterone.35 Patients on a ketogenic diet should never use metformin, as this greatly increases the risk of lactic acidosis.33
Exercise is a healthy lifestyle choice; that’s no secret. For people who are trying-to-conceive (TTC), however, this can be complicated. Moderately physically active men (i.e., those who exercise for about 1 hour 3 times a week) tend to have higher sperm counts and better sperm morphology than those who do not.36 Physical activity has a protective effect on women’s fertility when coupled with weight loss if they are overweight or obese. However, excessive exercise can negatively affect the reproductive system. When energy demand due to over-exercising exceeds dietary intake, it can cause hypothalamic dysfunction and alterations in natural pulsatile GnRH release.36 This can lead to menstrual abnormalities and decreased fertility.
Some patients may also to turn to complementary and alternative medicine (CAM) to improve outcomes and/or decrease stress and anxiety levels during fertility treatment.37 Patients also use CAM to incorporate cultural traditions of health and fertility and increase feelings of hope and control during assisted reproduction. CAM’s definition is far-reaching, but includes acupuncture, body work (e.g., massage), energy healing (e.g., reiki), herbal medicine, mind-body techniques (e.g., meditation, yoga), and more.37
Quality evidence for CAM interventions is lacking, and the ASRM only recognizes acupuncture as a viable option.37,38 Acupuncture, originating thousands of years ago in China, involves placing very thin needles at different points on the body. Traditional Chinese acupuncture is the most common type practiced in the U.S.38 The ASRM states that some medical studies have shown acupuncture to be helpful for patients with fertility issues, including those with PCOS, fibroids, endometriosis, or issues with ovarian reserve or sperm quality. They state that acupuncture 1 to 3 times a week, especially when started 3 months prior to other fertility treatments, may be beneficial.38 It may also relieve some adverse effects associated with fertility drugs (e.g., bloating, nausea).
The infertility or TTC community has also developed its own ideas about what can help with assisted reproduction success (see Superstitious Sidebar). While they certainly are not harmful, these theories and remedies have not been formally tested in the scientific community.
Superstitious Sidebar39-42
Many superstitions and wives’ tales circulate through the TTC community about ways to optimize natural fertility or boost the chances of assisted reproductive success. They don’t pose any harm, only potential benefits, so some patients choose to follow them. These are just the tip of the iceberg when it comes to fertility superstitions.
Pineapple core: Bromelain—an enzyme found in abundance in pineapple, especially the core—is thought to promote embryo implantation. This enzyme has anti-inflammatory properties, so some people believe it helps with infertility conditions associated with inflammation (e.g., endometriosis). Bromelain also has anticoagulant (blood thinning) properties, so some think that these effects may improve the uterine lining and blood flow to the uterus. Women who are TTC eat pineapple core around the time of implantation or immediately following an assisted embryo transfer. However, timing is everything here, as some people believe eating too much pineapple before ovulation could make the vaginal and cervical pH too acidic for sperm to survive. While the data on this intervention is unclear, pineapple is full of healthy nutrients, so it’s a good snack regardless. Bromelain can be dangerous in high amounts, but patients are unlikely to reach these amounts through pineapple ingestion alone.
Brazil nuts: Selenium—a mineral found in brazil nuts—could help with fertility in a few ways, leading many women to consume brazil nuts while TTC. First, selenium is thought to thicken the uterine wall to aid in healthy implantation. Similar to bromelain, selenium also has anticoagulant properties that could help prevent clots that could hinder implantation. Last, selenium has antioxidant properties that can assist in creating a healthy environment for a developing egg by decreasing damaging free radicals in the body. Online TTC forums suggest eating 2 to 3 raw brazil nuts (not roasted or cooked) daily from ovulation until 10 days post-ovulation for those selenium benefits. Like pineapple, brazil nuts are a healthy snack, fertility benefits aside.
Crystals: There is an ancient belief over 6,000 years old that the right stone or crystal can heal almost any health problem, including infertility. The premise is that health issues can stem from problems in chakras (energy centers) or the body’s energy flow, which can be corrected with crystals’ electromagnetic properties. Fertility crystals specifically revolve around the heart chakra, root chakra (spine and pelvic floor), and sacral chakra (above the belly button). Crystal healers and vendors most often suggest aquamarine, moonstone, and rose quartz for reproductive health and fertility. The scientific community has not proven these stones’ benefit, but many women still place crystals around the home or wear them around their wrist for added fertility support.
Warm feet: Chinese medicine has said for thousands of years that warm feet equate to a warm uterus and that a woman needs a lush warm uterus for an embryo to implant and thrive. The feet are connected to the uterus because the channels that start in your feet connect up to the reproductive organs, so if cold enters these channels, it will run into the uterus. Chinese medicine practitioners, including some acupuncturists, believe that a “cold uterus” indicates a lack of proper blood circulation. Also, Chinese medicine refers to progesterone as the “warming hormone,” so it is believed that women with low progesterone levels should take special care to remove cold and increase warmth however possible. For these reasons, many women who are TTC elect to wear socks all day and all night to increase the chances of a warm uterus and successful embryo implantation.
PROCEDURES
Intrauterine Insemination
Intrauterine insemination (IUI) involves washing an ejaculated semen specimen to remove prostaglandins and other factors and then concentrating the sperm in a small volume of culture media.5 Culture media used in IUI has a high protein concentration to enhance capacitation (physiologic changes to sperm that activate them) and the acrosome reaction. Just prior to ovulation, an RE runs a small catheter through the cervix to deliver the sperm directly to the upper uterine cavity. IUI is ideal for couples with male factor infertility or cervical factor infertility (i.e., sperm cannot swim through cervical mucus or anti-sperm antibodies are present).22 Women utilizing donor sperm also undergo IUI to conceive. IUI more than doubles the pregnancy rate for couples with male factor infertility.5 Sometimes, IUI is also effective for couples with unexplained infertility.5
IUI is less invasive, less expensive, and is more acceptable to patients than other procedures.43 Some REs also prefer to attempt 3 IUI cycles before embarking on more invasive treatments, like IVF. Women may also use medications to induce ovulation before IUI, especially those with documented ovarian failure or unexplained infertility.5 A 2018 retrospective cohort study found that among 765 infertile women with PCOS, clomiphene, letrozole, and injectable gonadotropins were equally efficacious and safe for stimulating ovulation before IUI.44
In Vitro Fertilization
IVF is an assisted reproduction method that combines a man’s sperm and a woman’s oocyte outside the body in a laboratory to create fertilized embryos.24 Providers historically used IVF to help women with blocked, damaged, or absent fallopian tubes to conceive.24 Now, they use IVF to treat many infertility causes, including endometriosis, male factor infertility, or unexplained fertility.
The basic steps of IVF are ovarian stimulation, egg retrieval, fertilization, embryo culture, and embryo transfer.24 Ovarian stimulation, also referred to as “ovarian induction,” is where the majority of medications are involved. Women use medications to stimulate multiple eggs to grow and mature in the ovaries, rather than the usual 1 egg per cycle. The goal is to stimulate multiple eggs because some eggs will not fertilize or develop normally after fertilization in the laboratory. An RE will order transvaginal ultrasounds and blood samples every few days to monitor the ovaries’ response to stimulation. They expect estrogen levels to increase as follicles develop and progesterone levels to remain low until after ovulation.24
Egg retrieval is a minor surgical procedure where an RE uses an ultrasound-guided needle connected to a suction device to enter through the vagina and retrieve multiple eggs.24 After laboratory fertilization, the RE will then transfer 1 or more embryos back into a woman’s uterus through a catheter to, hopefully, implant and develop. They can also cryopreserve (freeze) unused embryos for future use.
Every fertility clinic is not identical, and each RE employs different IVF protocols on a patient-by-patient basis. Ovarian stimulation protocols in the U.S. generally involve at least 3 drugs (refer to Table 1)45:
- FSH product to stimulate multiple eggs to develop
- GnRH agonist or antagonist to suppress premature LH surge and natural ovulation
- hCG to cause final egg maturation
An “antagonist protocol” (also known as a “short protocol”; see Figure 2) is the most common IVF protocol, as it involves the fewest injections and is effective for most patients.5,46
Figure 2. Antagonist IVF Stimulation Protocol5,46
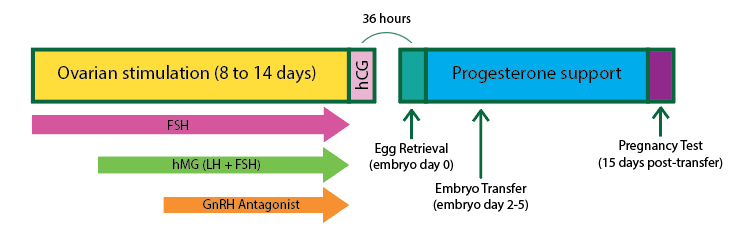
FSH, follicle-stimulating hormone; GnRH, gonadotropin-releasing hormone; hCG, human chorionic gonadotropin; hMG, human menopausal gonadotropin; IVF, in vitro fertilization; LH, luteinizing hormone
It is important to note that patients undergoing IVF self-administer all of these medications, which can be overwhelming. Proper injection technique is crucial to ensure patients receive full medication doses, avoid infections, and are adequately stimulated for egg retrieval. For subcutaneous injection, patients or their partner should47
- wash their hands
- choose a spot to inject into the abdomen (at least 2 inches away from the belly button), top of the thigh, or back of the arm (alternate injection sites daily)
- clean the injection area with an alcohol swab and allow to air dry
- gently grasp a small fold of skin between the thumb and index finger of the nondominant hand
- insert the entire length of the needle at a 45- to 90-degree angle into the fold of skin
- release the pinched skin and inject the medication in a slow, steady motion
- when all medication has been administered, pull the needle straight out and apply gentle pressure with a sterile gauze pad
- dispose of needles in a Sharps container
For intramuscular injection, patients or their partner should48
- wash their hands
- choose a spot to inject into the hip (upper, outer quadrant of the buttocks), outer area of the mid-thigh, or deltoid muscle in the arm (alternate injection sites daily)
- clean the injection area with an alcohol swab and allow to air dry
- use the thumb and index finger of the nondominant hand to gently spread the skin taut at the injection site
- insert the entire length of the needle in a quick, dart-like motion at a 90-degree angle straight in
- inject the medication in a slow, steady motion until the full dose is injected
- when all medication has been administered, pull the needle straight out and apply gentle pressure with a sterile gauze pad
- dispose of needles in a Sharps container
Many medications for IVF are in devices with special storage and administration instructions. Pharmacy technicians should always refer patients using them for the first time to the pharmacist. Additionally, pharmacists should always check the package insert before counseling a patient on unfamiliar devices.
Progesterone Support
Medications used during IVF can hinder the body’s ability to make progesterone, so supplementation is important. In fact, successful conception rates are much higher in patients who use progesterone support during and after IVF.49 REs typically initiate progesterone supplementation the day of egg retrieval and continue it through most of the first trimester. Patients can deliver progesterone vaginally or inject it intramuscularly. Often, patients who go through IVF find progesterone-in-oil injection to be the least pleasant injection of all. Warming the oil before drawing out the dose for injection thins it to reduce discomfort. Using a heating pad and gently massaging the area after injection can also be helpful.
CONCLUSION & RESOURCES
Infertility is a stressful, complicated condition. Patients are often overwhelmed by the cumbersome treatments and their high costs. Pharmacists and pharmacy technicians should recognize this and empathize with patients seeking fertility treatments to grow their families. See Table 2 for additional resources for pharmacy teams and patients. Adequate counseling and patient care can help individuals undergoing assisted reproduction maximize outcomes and reduce stress.
| Table 2. Resources for Pharmacy Teams and Patients Undergoing Fertility Treatments |
| American Society for Reproductive Medicine Patient-friendly factsheets and booklets about reproductive medicine |
https://www.reproductivefacts.org/news-and-publications/patient-fact-sheets-and-booklets/documents/new-factsheets-and-booklets/ |
| American Society for Reproductive Medicine Information for health care providers about reproductive medicine |
https://www.asrm.org/?vs=1 |
| Freedom Fertility Pharmacy MedTEACH Preparation and administration videos for commonly used medications during fertility treatment |
http://www.freedommedteach.com/eng/ |
| “It Starts with the Egg” by Rebecca Fett Book about how to improve egg quality, increase assisted reproduction success rates, and prevent miscarriage |
https://itstartswiththeegg.com/ |
REFERENCES
- Sharma RS, Saxena R, Singh R. Infertility & assisted reproduction: A historical & modern scientific perspective. Indian J Med Res. 2018;148(Suppl):S10-S14. doi:10.4103/ijmr.IJMR_636_18
- Centers for Disease Control and Prevention. Infertility FAQs. Updated April 13, 2021. Accessed April 29, 2021. https://www.cdc.gov/reproductivehealth/infertility/index.htm
- Shirazi T. How your chances of conception are affected by your cycle, age, birth control, health conditions (and more). Modern Fertility Blog. February 28, 2021. Accessed April 10, 2021. https://modernfertility.com/blog/chances-of-conception/
- Cousineau TM, Domar AD. Psychological impact of infertility. Best Pract Res Clin Obstet Gynaecol. 2007;21(2):293-308. doi:10.1016/j.bpobgyn.2006.12.003
- Strauss J, Barbieri R.. Yen & Jaffe’s Reproductive Endocrinology. 8th ed. Elsevier; 2017.
- Manganaro CL. "Louise Brown". Encyclopedia Britannica. July 21, 2020. Accessed April 27, 2021. https://www.britannica.com/biography/Louise-Brown
- Shrader SP, Ragucci KR. Contraception. In: DiPiro JT, Talbert RL, Yee GC, eds. Pharmacotherapy: A Pathophysiologic Approach. 10th ed. New York, NY: McGraw-Hill; 2017:1247-1262.
- Bull JR, Rowland SP, Scherwitzl EB, et al. Real-world menstrual cycle characteristics of more than 600,000 menstrual cycles. NPJ Digit Med. 2019;2:83. doi:10.1038/s41746-019-0152-7
- Male Contraceptive Initiative. Fertilization. Accessed April 10, 2021. https://www.malecontraceptive.org/fertilization.html
- Wesselink AK, Rothman KJ, Hatch EE, et al. Age and fecundability in a North American preconception cohort study. Am J Obstet Gynecol. 2017;217(6):667.e1-667.e8. doi:10.1016/j.ajog.2017.09.002
- Gnoth C, Godehardt D, Godehardt E, et al. Time to pregnancy: results of the German prospective study and impact on the management of infertility. Hum Reprod. 2003;18(9):1959-1966. doi:10.1093/humrep/deg366
- Larsen EC, Christiansen OB, Kolte AM, Macklon N. New insights into mechanisms behind miscarriage. BMC Med. 2013;11:154. doi:10.1186/1741-7015-11-154
- American Society for Reproductive Medicine. Infertility: an overview. Revised 2017. Accessed April 20, 2021. https://www.reproductivefacts.org/globalassets/rf/news-and-publications/bookletsfact-sheets/english-fact-sheets-and-info-booklets/infertility-an_overview_booklet2.pdf
- Shufelt CL, Torbati T, Dutra E. Hypothalamic amenorrhea and the long-term health consequences. Semin Reprod Med. 2017;35(3):256-262. doi:10.1055/s-0037-1603581
- Chalazonitis A, Tzovara I, Laspas F, et al. Hysterosalpingography: technique and applications. Curr Probl Diagn Radiol. 2009;38(5):199-205. doi:10.1067/j.cpradiol.2008.02.003
- American Society for Reproductive Medicine. Saline infusion sonohysterogram (SHG). Revised 2015. Accessed April 26, 2021. https://www.reproductivefacts.org/news-and-publications/patient-fact-sheets-and-booklets/documents/fact-sheets-and-info-booklets/saline-infusion-sonohysterogram-shg/
- Sturpe DA, Pincus KJ. Endometriosis. In: DiPiro JT, Talbert RL, Yee GC, eds. Pharmacotherapy: A Pathophysiologic Approach. 10th ed. New York, NY: McGraw-Hill; 2017:1279-1286.
- De La Cruz MS, Buchanan EM. Uterine Fibroids: Diagnosis and Treatment. Am Fam Physician. 2017;95(2):100-107.
- Urology Care Foundation. What is male infertility? Accessed April 16, 2021. https://www.urologyhealth.org/urology-a-z/m/male-infertility
- National Organization for Rare Disorders. Rare disease database: 47,XXY (Klinefelter Syndrome). Accessed April 16, 2021. https://rarediseases.org/rare-diseases/47-xxy-klinefelter-syndrome/
- American Society for Reproductive Medicine. Medications for inducing ovulation. Revised 2016. Accessed April 21, 2021. https://www.reproductivefacts.org/news-and-publications/patient-fact-sheets-and-booklets/documents/fact-sheets-and-info-booklets/medications-for-inducing-ovulation-booklet/
- [No author]. Drugs for ovulation induction. Med Lett Drugs Ther. 2011;53(1376):86-88.
- Society for Assisted Reproductive Technology. ART medications. Accessed April 23, 2021. https://www.sart.org/patients/a-patients-guide-to-assisted-reproductive-technology/general-information/art-medications/
- American Society for Reproductive Medicine. Assisted reproductive technology. Revised 2018. Accessed April 26, 2021. https://www.reproductivefacts.org/news-and-publications/patient-fact-sheets-and-booklets/documents/fact-sheets-and-info-booklets/assisted-reproductive-technologies-booklet/
- Freedom Fertility Pharmacy. 9 things you should know about Clomid. January 16, 2019. Accessed April 21, 2021. https://www.freedomfertility.com/blog/9-things-you-should-know-about-clomid/
- Clomid [prescribing information]. Sanofi-Aventis U.S. LLC; 2012.
- American Society for Reproductive Medicine. Ovarian hyperstimulation syndrome (OHSS). Revised 2014. Accessed April 27, 2021. https://www.reproductivefacts.org/news-and-publications/patient-fact-sheets-and-booklets/documents/fact-sheets-and-info-booklets/ovarian-hyperstimulation-syndrome-ohss/
- Male Fertility & Sexual Medicine Specialists. Clomid for Men: Can it Cure Low Sperm Count? January 7, 2013. Accessed April 21, 2021. https://www.malefertility.com/blog/clomid-for-men-can-it-cure-low-sperm-count
- Advanced Fertility Center of Chicago. Femara (letrozole) for infertility, ovulation problems and PCOS treatment. Accessed April 21, 2021. https://advancedfertility.com/fertility-medications/femara-letrozole-treatment/
- American Society for Reproductive Medicine. Side effects of injectable fertility drugs (gonadotropins). Revised 2012. Accessed April 21, 2021. https://www.reproductivefacts.org/news-and-publications/patient-fact-sheets-and-booklets/documents/fact-sheets-and-info-booklets/side-effects-of-injectable-fertility-drugs-gonadotropins/
- Orgovyx [prescribing information]. Myovant Sciences, Inc; 2020.
- Orilissa [prescribing information]. AbbVie Inc.; 2021.
- American Society for Reproductive Medicine. Insulin-sensitizing agents and polycystic ovary syndrome. Revised 2012. Accessed April 23, 2021. https://www.reproductivefacts.org/news-and-publications/patient-fact-sheets-and-booklets/documents/fact-sheets-and-info-booklets/insulin-sensitizing-agents-and-polycystic-ovary-syndrome/
- Brown MJ, Seitz A. 16 natural ways to boost fertility. Healthline Parenthood. Updated August 13, 2020. Accessed April 26, 2021. https://www.healthline.com/nutrition/16-fertility-tips-to-get-pregnant
- Colini S. Can the keto diet help boost fertility? January 8, 2019. CCRM Fertility. Accessed April 26, 2021. https://www.ccrmivf.com/news-events/keto-diet/
- Sharma R, Biedenharn KR, Fedor JM, Agarwal A. Lifestyle factors and reproductive health: taking control of your fertility. Reprod Biol Endocrinol. 2013;11:66. doi:10.1186/1477-7827-11-66
- Miner SA, Robins S, Zhu YJ, et al. Evidence for the use of complementary and alternative medicines during fertility treatment: a scoping review. BMC Complement Altern Med. 2018;18(1):158. doi:10.1186/s12906-018-2224-7
- American Society for Reproductive Medicine. Acupuncture and infertility treatment. 2015. Accessed April 26, 2021. https://www.reproductivefacts.org/news-and-publications/patient-fact-sheets-and-booklets/documents/fact-sheets-and-info-booklets/acupuncture-and-infertility-treatment/
- Shirazi T. Pineapple core, bromelain, and embryo implantation: what the science really says. Modern Fertility Blog. March 26, 2021. Accessed April 26, 2021. https://modernfertility.com/blog/pineapple-core-bromelain-implantation/
- Mendes C. Pineapple for conception & brazil nuts for implantation. Oh Baby Blog. Accessed April 26, 2021. https://www.ohbabynutrition.com/blog/pineapple-for-conception-brazil-nuts-for-implantation
- Shirazi T. Can crystals for fertility help you get pregnant? Modern Fertility Blog. February 9, 2021. Accessed April 26, 2021. https://modernfertility.com/blog/crystals-for-fertility/
- Mahanian M. How keeping feet warm boosts fertility. Chinese Medicine Clinic. Accessed April 26, 2021. https://chinesemedicineclinic.com/feet-warm-boost-fertility/
- Nandi A, El-Toukhy T. Stimulated intrauterine insemination for unexplained subfertility. Lancet. 2018;391(10119):404-405. doi:10.1016/S0140-6736(17)33038-6
- Huang S, Du X, Wang R, et al. Ovulation induction and intrauterine insemination in infertile women with polycystic ovary syndrome: A comparison of drugs. Eur J Obstet Gynecol Reprod Biol. 2018;231:117-121. doi:10.1016/j.ejogrb.2018.08.002
- Advanced Fertility Center of Chicago. Ovarian stimulation IVF protocols medications and drugs for in vitro fertilization. Accessed April 26, 2021. https://advancedfertility.com/ivf-in-detail/ovarian-stimulation/
- Copperman A. Which IVF protocol is right for you? Progyny. Accessed April 26, 2021. https://progyny.com/education/ivf-facts/which-ivf-protocol/
- Freedom Fertility Pharmacy. Freedom MedTEACH: general subcutaneous injection. Accessed April 26, 2021. http://www.freedommedteach.com/eng/videos.html?play=general_sq
- Freedom Fertility Pharmacy. Freedom MedTEACH: general intramuscular injection. Accessed April 26, 2021. http://www.freedommedteach.com/eng/videos.html?play=general_im
- American Society for Reproductive Medicine. Progesterone supplementation during IVF. Revised 2016. Accessed April 26, 2021. https://www.reproductivefacts.org/news-and-publications/patient-fact-sheets-and-booklets/documents/fact-sheets-and-info-booklets/progesterone-supplementation-during-in-vitro-fertilization-ivf-cycles/
Back to Top