
Expired activity
Please go to the PowerPak
homepage and select a course.
Non-tuberculous Mycobacterial Lung Disease (NTM-LD): New Guidelines to Manage a Challenging Respiratory Disease
» Educational Tools
Identifying the Patient With Nontuberculous Mycobacterial Lung Disease: Pathophysiology and Diagnosis
Kevin Winthrop, MD, MPH
Nontuberculous mycobacteria (NTM) are ubiquitous environmental bacteria found in both soil and water, including municipal and natural water systems.1 These bacteria can produce disease in humans of all ages, both in pulmonary and extrapulmonary sites, and are becoming increasingly responsible for human morbidity and mortality worldwide.1-4 More than 180 bacterial species are currently recognized, many of which are nonpathogenic and may be contaminants in patient cultures.5 One retrospective multicenter study in Belgium reviewed patient respiratory samples that were positive for NTM from 2010 through 2017.6 Of the 384 patients, 165 (43%) fulfilled the American Thoracic Society/Infectious Diseases Society of America criteria for NTM-lung disease (LD).6 This represented more than 20 different mycobacterium species (Figure 1).6 Rare isolates (totaling <1% of samples) not associated with NTM-LD included Mycobacterium gilvum, M holsaticum, M wolinsky/jacuzzi, M novocastrense, and M terrae complex.6
| Figure 1. Clinical Relevance of NTM-LD Isolates |
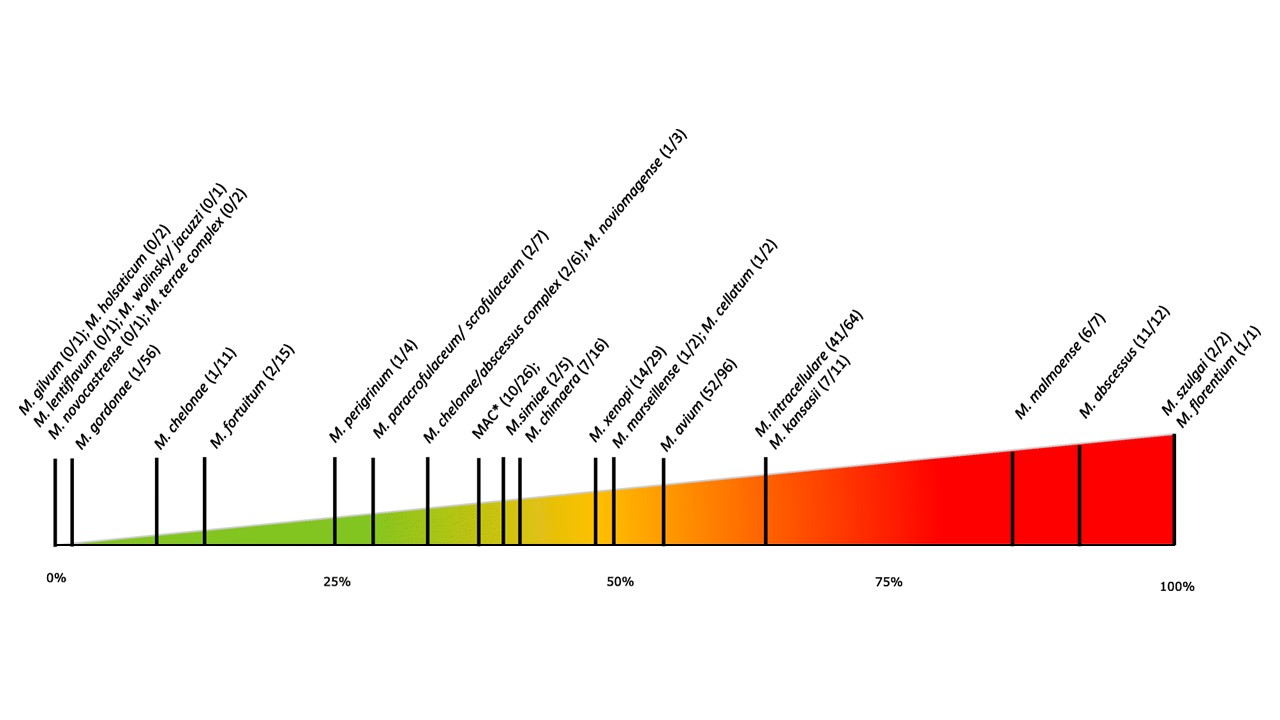 |
Ratio of clinical significance: clinical significance per species; presented as a percentage based on the number of cases meeting American Thoracic Society/Infectious Diseases Society of America criteria for NTM-LD and the number of isolates per species.
*MAC – not further specified; reported as “MAC.”
MAC = Mycobacterium avium complex; NTM-LD = nontuberculous mycobacterial lung disease.
Source: Vande Weygaerde Y, et al.6 Open Access – http://creativecommons.org/licenses/by/4.0/ |
Mycobacterium avium complex (MAC) is reported to account for up to 91% of NTM-LD isolates.3,4 This complex includes several mycobacterial species—M avium (with its 4 subspecies), M intracellulare, and other lesser known or more rare species.7 The majority of the remaining cases of NTM-LD are caused by M abscessus (6%-13%), with M kansasii, M xenopi, and M fortuitum making up the remainder of isolates at <5% each.4
The NTM-Network European Trials Group acquired 2008 NTM species-identification data for 20,182 pulmonary samples provided by 62 laboratories on 6 continents.8 MAC predominated in most samples, present in 47% of the overall samples.8 The lowest MAC presence among NTM pulmonary samples in the study was noted in South America (31%) and Europe (37%), and the highest presence was seen in samples from Australia (71%).8 MAC was identified in more than half (52%) of North American samples.8
Mycobacteria species distribution also varies widely geographically within the United States, as reported in a study of almost 6 million patients from 2009 to 2013 in a US healthcare database.3 Of these patients, 0.13% had at least 1 NTM-positive culture, and 17% had at least 2 positive cultures within the same patient encounter.3 MAC was the most frequent species identified, present in 61% to 91% of isolates, with greater frequencies in the Southern and Northeast regions of the United States.3 Some species were more frequent in Western states, including M abscessus/M chelonae (ranging from 2% to 18% of isolates) and M fortuitum and M kansasii (ranging from 7% to 26% of isolates).3
The Prevalence and Incidence of NTM-LD
The prevalence of NTM-LD is increasing worldwide, including in the United States.4,9 The increased prevalence may be influenced in part by increased awareness and improved diagnostics leading to more accurate detection.2 Conversely, a lack of access to medical care can have a negative impact on prevalence estimates.2
Annual contiguous US population-based prevalence estimates for NTM-LD ranged from 1.4 to 13.9 per 100,000 persons, with up to 44 per 100,000 persons reported for Hawaii—the highest rate seen in the United States.2 The lack of uniformity among locations is most likely related to the interaction of environmental, microbial, and host factors, including inherent structural (eg, chronic obstructive pulmonary disease [COPD]); immunologic; and genetic differences.2 In the US Medicare population of beneficiaries aged ≥65 years, the prevalence of NTM-LD increased 8.2% per year between 1997 and 2007, from 20 to 47 cases per 100,000 persons.2
A statewide population-based incidence estimate in Oregon noted a slight increase from 4.8/100,000 to 5.6/100,000 from 2007 to 2012, with MAC being present in approximately 91% of those infected.10 Females comprised 42% of cases in patients <50 years of age, with incidence rates of 4.8 and 5.4 per 100,000 for females and males, respectively, between the ages of 50 and 59.10 However, in patients between 60 and 69 years of age, the incidence rate in females exceeded that of males (11.2 vs 9.0 per 100,000), and rates reached 30.0 and 28.0 per 100,000 for females and males aged ≥80 years, respectively.10
A large, US managed-care claims database comprising a population of approximately 27 million members annually was accessed to estimate annual incidence and prevalence of NTM-LD between 2008 and 2015 (Figure 2).11 During this interval, the annual incidence increased from 3.13 to 4.73 per 100,000, with a greater increase for women (range, 4.16 to 6.69) compared with men (range, 2.05 to 2.71).11 Both incidence and prevalence increased in most states during that period, with marked increases observed in Florida and adjacent states.11
| Figure 2. NTM-LD: Yearly Health Insurance Plan Incidence |
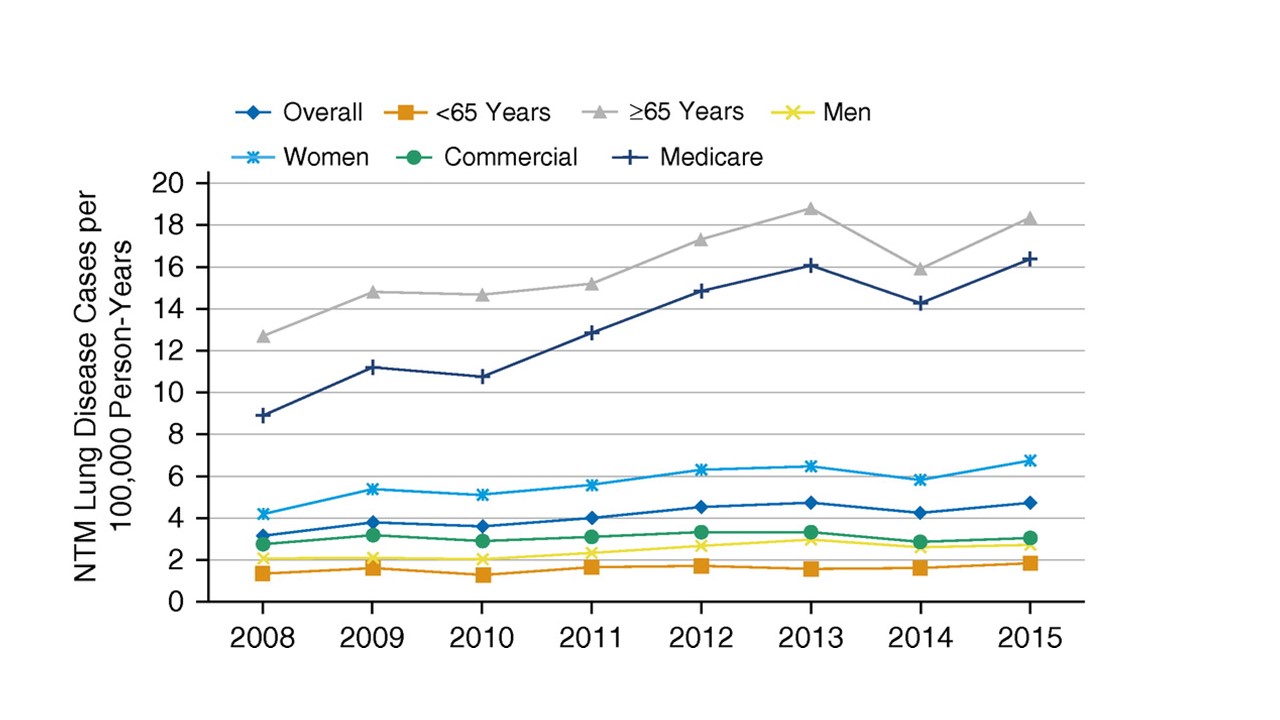 |
NTM-LD = nontuberculous mycobacterial lung disease.
Source: Winthrop KL, et al.11 Open Access. https://creativecommons.org/licenses/by-nc-nd/4.0/ |
Risk Factors for Pulmonary NTM Infection
Major risk factors for NTM-LD include underlying structural lung disease (eg, COPD); prior tuberculosis or other infections; cystic fibrosis (CF); pneumoconiosis; and bronchiectasis.1,12 A case-control study in Denmark of adults with microbiologically confirmed NTM-LD between 1997 and 2008 reported a 16.5-fold increased risk of NTM-LD for persons with chronic respiratory disease, reaching the highest adjusted odds ratio (OR) of 187 for persons with a history of bronchiectasis.13 In addition, a protease inhibitor phenotype with a relative deficiency of alpha-1 antitrypsin phenotype can predispose to NTM-LD as well as bronchiectasis.12,14
Bronchiectasis and MAC often coexist, complicating causality determinations.15,16 Among 1826 patients in the Bronchiectasis Research Registry, 63% had coexistent NTM.16 The CF Foundation reported 20% of persons in their patient registry had a pathogenic NTM species isolated at least once between 2010 and 2014,17 while 14% of patients undergoing a mycobacterial culture during 2019 had at least 1 positive culture.18 Nationwide US Veterans Affairs Hospitals data from 2001 to 2015 revealed that the prevalence of NTM in patients with COPD increased from 93.1 per 100,000 patients in 2001 to 277.6 per 100,000 in 2015.19
Among nonpulmonary risk factors, the adjusted risk for NTM infection was reported as being 6.24-fold higher in patients with rheumatoid arthritis (RA) than in the general population in Taiwan, with 51.9% also having NTM disease.1,20 In Canada, the adjusted NTM-LD risk was increased 1.93-fold in patients with RA compared with the general population.21 Gastroesophageal reflux disease (GERD) has also been associated with NTM-LD, reported in 26% to 44% of NTM-LD patients in 3 studies, and is presumed to be acquired by aspiration of oropharyngeal secretions or gastrointestinal tract contents.1,14 Rapidly growing species, such as M abscessus or M fortuitum, frequently are the most likely cause of NTM-LD in patients with GERD.1
Pathophysiology
The pathophysiology of NTM-LD is complicated and poorly understood. Host susceptibility factors, which include preexisting lung disease and systemic risk factors, overlap with environmental exposures and can result in NTM infection (Figure 3).22-24 A multigenic association with NTM-LD has been proposed, where variants in immune, CF transmembrane conductance regulator, ciliary function, and connective tissue gene sets may make NTM-LD more likely—particularly in a setting where other risk factors, including environmental exposures, are present.23
| Figure 3. NTM Pulmonary Infections—Pathophysiology |
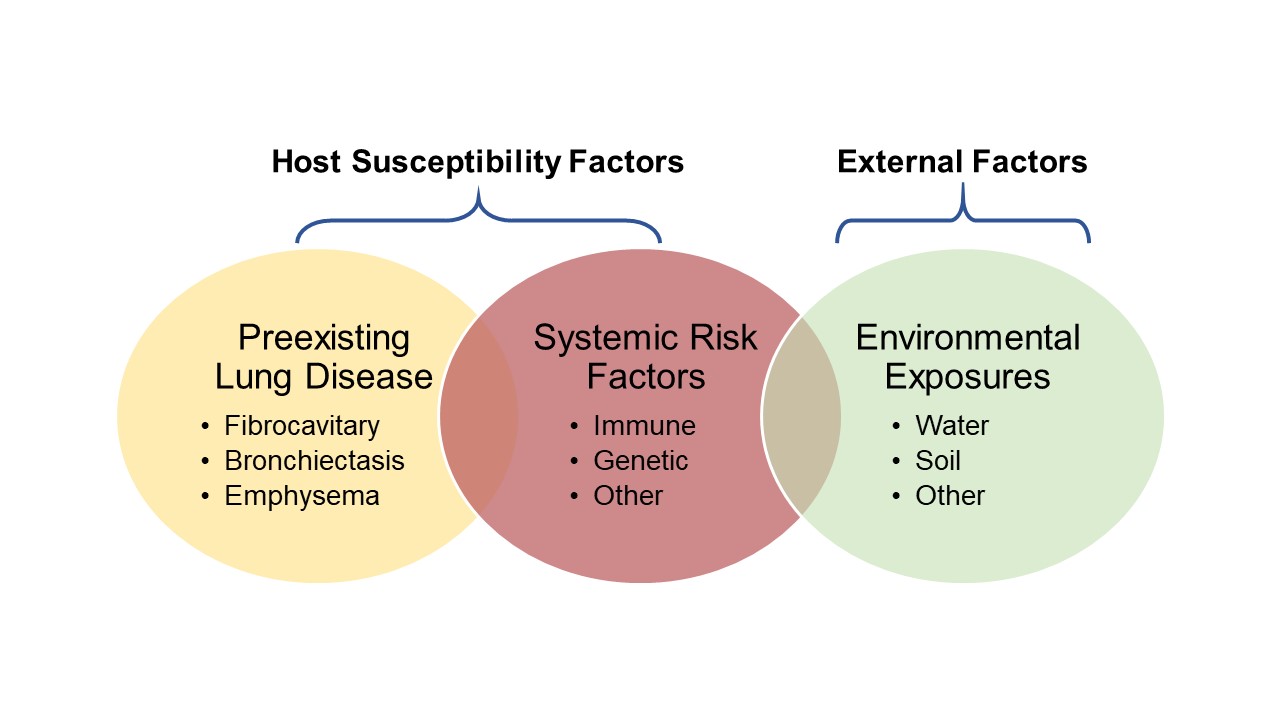 |
NTM = nontuberculous mycobacteria.
Source: Marras TK.22 Szymanski EP, et al.23 Dirac MA, et al.24 |
Immunosuppressants and Pulmonary NTM Infection
The use of immunosuppressants can increase the risk for NTM-LD.1 A case-control study in Oregon and Washington reported that oral prednisone use was associated with an OR of 8.0 for MAC disease.24 Similar findings were reported in a case-control study from Denmark, where the OR of NTM-LD in patients with COPD and no history of inhaled corticosteroid (ICS) use was 7.6 compared with population controls, which increased to an OR of 19.6 for patients who had ever used ICS, and 29.1 for those with current ICS use.13 The odds were increased from 28.1 for patients with a mean daily dose <800 µg/day over 365 days to 47.5 for those with a mean daily dose ≥800 µg/day.13
In a Japanese study of 14 patients with NTM-LD and asthma who were receiving ICS compared with similar controls with asthma but without NTM-LD, the daily fluticasone propionate equivalent was higher in those with NTM-LD than controls (650 ± 257 µg vs 358 ± 273 µg; P<.01), and patients with NTM-LD had been using ICS longer than controls (8.2 ± 4.8 years vs 5.3 ± 4.9 years; P<.01).25 Another 1:10 matched case-control study of patients in northern California included health plan data for subjects with airway disease both with (n=248) and without (n=2480) NTM-LD between 2000 and 2010.26 Researchers examined the use of ICS, other airway disease medications, and health care use within 6 months of NTM-LD identification.26 The odds of NTM infection increased among tertiles of patients with increasing cumulative dose, based on beclomethasone-equivalent doses used.26
Tumor necrosis factor (TNF) inhibitors, which are used to treat a variety of autoimmune diseases, also increase the risk for NTM-LD.27-29 In a US study conducted between 2000 and 2008 that assessed mycobacterial diseases in individuals who were on anti-TNF therapy, rates of NTM disease were elevated, particularly among individuals with RA.27 An Ontario population-based study of persons with RA also demonstrated that anti-TNF therapy was associated with greater risk for developing NTM-LD.28 Additional findings from a study using the FDA MedWatch database found NTM infections were most commonly associated with infliximab use but also noted with use of etanercept and adalimumab.29 Notably, more than half of these patients were on concurrent prednisone or methotrexate.29
NTM-LD: 2 Disease Types
Two NTM-LD phenotypes have been described—fibrocavitary and nodular/bronchiectatic—which have important implications for monitoring and treatment recommendations.1,4,23,30 The cavitary type is characterized by upper lobe fibrocavitary disease and is more commonly seen in older men with a history of smoking and underlying COPD.4 It is more rapidly progressive compared with the second, nodular/bronchiectatic type, which is typically without other significant lung disease (Figure 4).4 This slowly progressive type is more common in women and is often called Lady Windermere syndrome.4 Women with this type often are tall with a low body mass index (BMI), with associated anatomic abnormalities including scoliosis or a pectus deformity and mitral valve prolapse, and exhibiting “tree-in-bud” bronchiolitis on computed tomography (CT), with nodularity and mucoid impaction.1,30 This type typically begins and focuses in either the right middle lobe or lingula.30 There is considerable overlap between the 2 types; for example, a Lady Windermere counterpart was recently described in older males with NTM-LD and a low BMI.1 In addition, patients with nodular/bronchiectatic NTM-LD can also develop cavities (Figure 5).1
| Figure 4. MAC Disease Types |
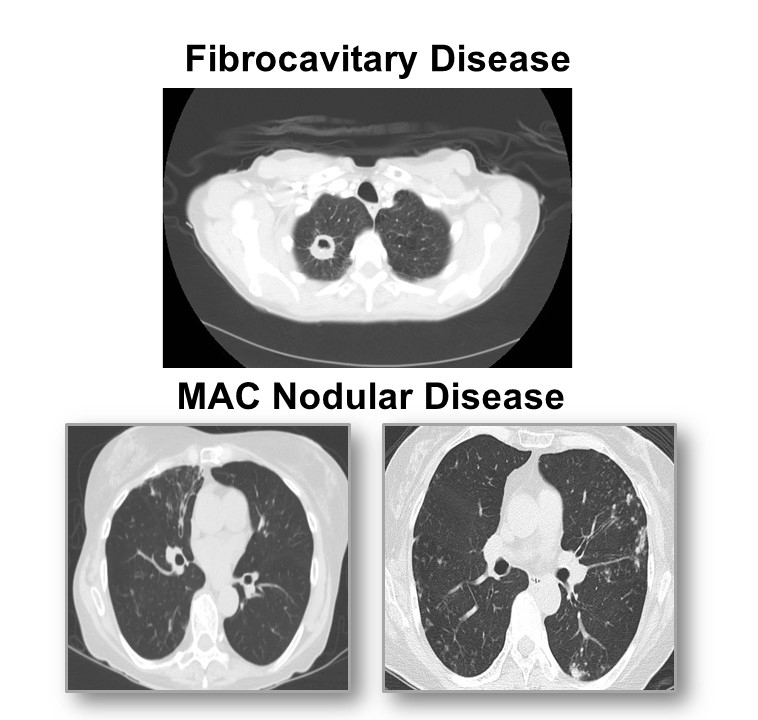 |
MAC = Mycobacterium avium complex.
Images courtesy of Anne O’Donnell, MD. |
| Figure 5: Cavities in the NTM-LD Nodular/Bronchiectatic Form |
 |
NTM-LD = nontuberculous mycobacterial lung disease.
Image courtesy of Kevin Winthrop, MD. |
Cavitary and nodular/bronchiectatic disease require different treatment approaches; therefore, distinguishing between them is essential for optimum management.1 Cavitary disease should be treated more aggressively, while nodular/bronchiectatic disease is more likely to recur, requiring lifelong follow-up.1
Diagnosis of NTM-LD
Diagnosis of NTM-LD can be complex, with its variable, nonspecific symptoms, and specimen cultures may require several weeks to finalize.12,31 Patients may be unable to produce sputum, in which cases sputum induction should be used.12 Bronchoscopy may be necessary if sputum cannot be obtained, either spontaneously or by induction.12
Pulmonary symptoms associated with NTM-LD include chronic cough in most patients and variability in expression of sputum production, with occasional hemoptysis and chest pain.12 Systemic symptoms include fatigue, malaise, fever, weight loss, and night sweats.12,31 Underlying lung disease can complicate diagnosis.12
The diagnostic triad for NTM-LD includes clinical, radiologic, and microbiologic criteria that must be fulfilled.1,32 In the presence of pulmonary or systemic symptoms, patients should have radiologic findings consistent with nodular/bronchiectatic or cavitary NTM-LD.12 Although a plain chest radiograph may be adequate to demonstrate fibrocavitary disease, high-resolution CT is routinely used to demonstrate multifocal bronchiectasis with multiple nodules and to allow exclusion of other diagnoses.12 Microbiologic standards include positive culture results from ≥2 separate expectorated sputum samples identifying the same species (subspecies for M abscessus), or positive culture results from ≥1 bronchial wash or lavage, or mycobacterial histologic features (granulomatous inflammation or acid-fast bacilli) in transbronchial or other lung biopsy specimens with ≥1 positive NTM cultures.12
Determining the specific species responsible for the infection varies considerably in relation to their pathogenicity, which may differ among geographic areas.1,12 Organisms with low pathogenicity may require multiple repeated positive cultures over months (supported by strong clinical and radiologic evidence or even growth on a biopsy specimen to identify it as the causative organism), whereas a single positive culture of a more pathogenic organism like M kansasii may be sufficient to initiate treatment.33 Accordingly, practitioners should understand the virulence of these organisms in their practice settings and conduct testing accordingly.
Summary
Disease caused by NTM is increasing globally, although the majority of the almost 200 NTM species that have been identified are non-pathogenic.3 Pathogenic species can be responsible for 2 types of lung disease: the typically more rapidly progressing fibrocavitary form and the often slower progressing nodular/bronchiectatic form.4 Clinicians should know when to have a suspicion of NTM-LD and perform the recommended diagnostic investigations to allow timely initiation of optimum management practices when cases are identified.
References
- Daley CL, Winthrop KL. Mycobacterium avium complex: addressing gaps in diagnosis and management. J Infect Dis. 2020;222(Suppl 4):S199-S211.
- Adjemian J, Daniel-Wayman S, Ricotta E, Prevots DR. Epidemiology of nontuberculous mycobacteriosis. Semin Respir Crit Care Med. 2018;39(3):325-335.
- Spaulding AB, Lai YL, Zelazny AM, Olivier KN, Kadri SS, Prevots DR, et al. Geographic distribution of nontuberculous mycobacterial species identified among clinical isolates in the United States, 2009-2013. Ann Am Thorac Soc. 2017;14(11):1655-1661.
- Novosad S, Henkle E, Winthrop KL. The challenge of pulmonary nontuberculous mycobacterial infection. Curr Pulmonol Rep. 2015;4(3):152-161.
- Gupta RS, Lo B, Son J. Phylogenomics and comparative genomic studies robustly support division of the genus Mycobacterium into an emended genus Mycobacterium and four novel genera. Front Microbiol. 2018;9:67.
- Vande Weygaerde Y, Cardinaels N, Bomans P, Chin T, Boelens J, Andre E, et al. Clinical relevance of pulmonary non-tuberculous mycobacterial isolates in three reference centres in Belgium: a multicentre retrospective analysis. BMC Infect Dis. 2019;19(1):1061.
- Diel R, Lipman M, Hoefsloot W. High mortality in patients with Mycobacterium avium complex lung disease: a systematic review. BMC Infect Dis. 2018;18(1):206.
- Hoefsloot W, van Ingen J, Andrejak C, Angeby K, Bauriaud R, Bemer P, et al. The geographic diversity of nontuberculous mycobacteria isolated from pulmonary samples: an NTM-NET collaborative study. Eur Respir J. 2013;42(6):1604-1613.
- Diel R, Jacob J, Lampenius N, Loebinger M, Nienhaus A, Rabe KF, et al. Burden of non-tuberculous mycobacterial pulmonary disease in Germany. Eur Respir J. 2017;49(4):1602109.
- Henkle E, Hedberg K, Schafer S, Novosad S, Winthrop KL. Population-based incidence of pulmonary nontuberculous mycobacterial disease in Oregon 2007 to 2012. Ann Am Thorac Soc. 2015;12(5):642-647.
- Winthrop KL, Marras TK, Adjemian J, Zhang H, Wang P, Zhang Q. Incidence and prevalence of nontuberculous mycobacterial lung disease in a large U.S. managed care health plan, 2008-2015. Ann Am Thorac Soc. 2020;17(2):178-185.
- Griffith DE, Aksamit T, Brown-Elliott BA, Catanzaro A, Daley C, Gordin F, et al. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007;175(4):367-416.
- Andrejak C, Nielsen R, Thomsen VO, Duhaut P, Sorensen HT, Thomsen RW. Chronic respiratory disease, inhaled corticosteroids and risk of non-tuberculous mycobacteriosis. Thorax. 2013;68(3):256-262.
- Moon P, Guillaumin E, Chan ED. Non-tuberculous mycobacterial lung disease due to multiple “minor” risk factors: an illustrative case and a review of these “lesser elements”. J Thorac Dis. 2020;12(9):4960-4972.
- Bonaiti G, Pesci A, Marruchella A, Lapadula G, Gori A, Aliberti S. Nontuberculous mycobacteria in noncystic fibrosis bronchiectasis. Biomed Res Int. 2015;2015:197950.
- Aksamit TR, O'Donnell AE, Barker A, Olivier KN, Winthrop KL, Daniels MLA, et al. Adult patients with bronchiectasis: a first look at the US Bronchiectasis Research Registry. Chest. 2017;151(5):982-992.
- Adjemian J, Olivier KN, Prevots DR. Epidemiology of pulmonary nontuberculous mycobacterial sputum positivity in patients with cystic fibrosis in the United States, 2010-2014. Ann Am Thorac Soc. 2018;15(7):817-826.
- Cystic Fibrosis Foundation. 2019 Patient Registry Annual Data Report. Published September 2020. Accessed March 10, 2021. https://www.cff.org/Research/Researcher-Resources/Patient-Registry/2019-Patient-Registry-Annual-Data-Report.pdf
- Pyarali FF, Schweitzer M, Bagley V, Salamo O, Guerrero A, Sharifi A, et al. Increasing non-tuberculous mycobacteria infections in veterans with COPD and association with increased risk of mortality. Front Med (Lausanne). 2018;5:311.
- Liao TL, Lin CH, Shen GH, Chang CL, Lin CF, Chen DY. Risk for mycobacterial disease among patients with rheumatoid arthritis, Taiwan, 2001-2011. Emerg Infect Dis. 2015;21(8):1387-1395.
- Brode SK, Jamieson FB, Ng R, Campitelli MA, Kwong JC, Paterson JM, et al. Risk of mycobacterial infections associated with rheumatoid arthritis in Ontario, Canada. Chest. 2014;146(3):563-572.
- Marras TK. Host susceptibility or environmental exposure in Mycobacterium avium complex lung disease: it takes two to tango. Am J Respir Crit Care Med. 2012;186(7):585-586.
- Szymanski EP, Leung JM, Fowler CJ, Haney C, Hsu AP, Chen F, et al. Pulmonary nontuberculous mycobacterial infection. a multisystem, multigenic disease. Am J Respir Crit Care Med. 2015;192(5):618-628.
- Dirac MA, Horan KL, Doody DR, Meschke JS, Park DR, Jackson LA, et al. Environment or host? A case-control study of risk factors for Mycobacterium avium complex lung disease. Am J Respir Crit Care Med. 2012;186(7):684-691.
- Hojo M, Iikura M, Hirano S, Sugiyama H, Kobayashi N, Kudo K. Increased risk of nontuberculous mycobacterial infection in asthmatic patients using long-term inhaled corticosteroid therapy. Respirology. 2012;17(1):185-190.
- Liu VX, Winthrop KL, Lu Y, Sharifi H, Nasiri HU, Ruoss SJ. Association between inhaled corticosteroid use and pulmonary nontuberculous mycobacterial infection. Ann Am Thorac Soc. 2018;15(10):1169-1176.
- Winthrop KL, Baxter R, Liu L, Varley CD, Curtis JR, Baddley JW, et al. Mycobacterial diseases and antitumour necrosis factor therapy in USA. Ann Rheum Dis. 2013;72(1):37-42.
- Brode SK, Jamieson FB, Ng R, Campitelli MA, Kwong JC, Paterson JM, et al. Increased risk of mycobacterial infections associated with anti-rheumatic medications. Thorax. 2015;70(7):677-682.
- Winthrop KL, Chang E, Yamashita S, Iademarco MF, LoBue PA. Nontuberculous mycobacteria infections and anti-tumor necrosis factor-alpha therapy. Emerg Infect Dis. 2009;15(10):1556-1561.
- Winthrop KL, McNelley E, Kendall B, Marshall-Olson A, Morris C, Cassidy M, et al. Pulmonary nontuberculous mycobacterial disease prevalence and clinical features: an emerging public health disease. Am J Respir Crit Care Med. 2010;182(7):977-982.
- National Organization for Rare Disorders (NORD). Nontuberculous Mycobacterial Lung Disease. Accessed March 12, 2021. https://rarediseases.org/rare-diseases/nontuberculous-mycobacterial-lung-disease/
- Griffith DE, Aksamit TR. How I do it: managing M avium complex lung disease with a little help from my friend. Chest. 2020;159(4):1372-1381.
- Daley CL, Iaccarino JM, Lange C, Cambau E, Wallace RJ, Andrejak C, et al. Treatment of nontuberculous mycobacterial pulmonary disease: an official ATS/ERS/ESCMID/IDSA Clinical Practice Guideline: Executive Summary. Clin Infect Dis. 2020;71(4):e1-e36.
Treatment Optimization: New Guidelines for NTM-LD Management
Charles Daley, MD
The American Thoracic Society (ATS), European Respiratory Society (ERS), European Society of Clinical Microbiology and Infectious Diseases (ESCMID), and Infectious Diseases Society of America (IDSA) jointly sponsored development of a new Clinical Practice Guideline for Treatment of Nontuberculous Mycobacterial Pulmonary Disease, which was published in 2020.1 The guideline focuses on nontuberculous mycobacterial (NTM) lung disease (LD) in adults without cystic fibrosis or human immunodeficiency virus infection and that is caused by the most common NTM pathogens, comprising slow-growing Mycobacterium avium complex (MAC), M kansasii, and M xenopi; and the rapidly growing M abscessus.1 The 2020 guideline encompasses 22 PICO (Population, Intervention, Comparators, Outcomes) questions and associated recommendations that were developed from evidence appraised using GRADE (Grading of Recommendations Assessment, Development, and Evaluation) methodology.1
Initiating Treatment for MAC-LD
The expert panel suggested that practitioners begin treating patients who meet the diagnostic criteria for NTM-LD rather than following a watchful waiting approach that monitors for evidence of progression.1 This conditional recommendation was especially pertinent for patients with positive acid-fast bacilli sputum smears or cavitary lung disease.1 Relevant to this, one Korean study reported on a cohort of 488 patients diagnosed with treatment-naïve MAC-LD between 1998 and 2011.2 It included 305 (62.5%) patients with progression that resulted in treatment initiation within 3 years of diagnosis and 115 (23.6%) patients with stable untreated disease for at least 3 years, with a median 5.6-year follow-up.2 Of 93 untreated patients, 51.6% spontaneously converted to culture-negative status.2 Bacterial load and a greater extent of disease on radiologic findings (including fibrocavitary disease) were more common in patients with progressive disease compared with those with stable disease.2 Other studies show that older age; male gender; lower body mass index; and presence of comorbidities, anemia, low albumin, and elevated inflammatory markers are also factors associated with a poorer prognosis.1,3
The joint ATS/ERS/ESCMID/IDSA guidelines suggest that patients with MAC-LD be given susceptibility-based macrolide treatment.1 In cohort studies, macrolide susceptibility has been a strong predictor of treatment success, and macrolide resistance is associated with a markedly reduced rate of sputum culture conversion, decreasing from approximately 80% to only 5% to 36%.1 Azithromycin and clarithromycin have demonstrated similar culture conversion in cohort studies; however, azithromycin has less potential for drug–drug interactions, once-daily dosing, and a lower pill burden.1 Accordingly, azithromycin-based treatment regimens are suggested for treating patients with macrolide-susceptible MAC-LD.1
Parenteral aminoglycoside therapy is suggested to be included in the initial treatment regimen for patients with cavitary or advanced/severe bronchiectatic or macrolide-resistant MAC-LD.1 A single, randomized controlled trial reported a significantly higher sputum culture conversion rate for patients who received parenteral streptomycin compared with those who received oral therapy only (71.2% vs 50.7%).4 In addition, adding aminoglycoside treatment to the regimen increases rates of culture conversion in patients with macrolide-resistant disease.1
A treatment regimen with at least 3 drugs (eg, macrolide, ethambutol, rifamycin) is suggested for patients with macrolide-susceptible MAC-LD.1 In an open-label study in Japan, treatment-naïve patients were randomly assigned to a daily 3-drug regimen (clarithromycin, ethambutol, rifamycin) or 2-drug regimen (clarithromycin, ethambutol) for 12 months.1 Although culture conversion on the 2-drug regimen (82.5%) was noninferior to the 3-drug regimen (75%) in the intention-to-treat analysis, the study was underpowered due to the small sample size and considerable drop-out during the study, and some of the drug doses were lower than ATS/IDSA recommended dosing.1 Even at similar conversion rates, inclusion of a third drug in the regimen may help prevent development of macrolide resistance.1
In MAC-LD, susceptibility data have been correlated with clinical outcomes for clarithromycin and amikacin.1,5 An in vitro macrolide minimum inhibitory concentration (MIC) of ≤8 mg/mL in MAC isolates is considered susceptible, and ≥32 mg/mL is considered resistant.5 For parenteral amikacin, the separation between “susceptible” and “resistant” is at 64 mg/mL; that is, resistance is predicted by MIC values >64 mg/mL.5 For inhaled liposomal amikacin, the resistance cut-point is ≥128 µg/mL.1 Importantly, rifampicin, ethambutol, clofazimine, fluoroquinolone, and streptomycin MICs have not been shown to be associated with clinical response; therefore, in vitro susceptibility test results for these drugs are not clinically applicable.5 Ethambutol is the most important drug for protecting against emergence of macrolide resistance, despite an MIC that is typically above the established level for ethambutol-susceptible M tuberculosis isolates.5 Therefore, the mechanism for this protective effect is not mediated by its MIC for MAC, and discontinuation of ethambutol in response to in vitro susceptibility results not only increases the risk of treatment failure but also the emergence of macrolide resistance.5
The guidelines suggest daily treatment administration for cavitary disease and intermittent, 3-times weekly administration for noncavitary disease.1 Cohort studies and case series have reported similar conversion rates following both intermittent and daily therapy, including 2 studies in patients with nodular/bronchiectatic MAC-LD on either daily or intermittent regimens for a minimum of 12 months.1 In addition to similar culture conversion rates in patients on intermittent compared with daily regimens, medication intolerance requiring a switch to intermittent treatment or regimen modification was significantly greater in patients taking daily medication.1 Acquired macrolide resistance was not reported in either study.1 However, very low culture conversion rates have been reported following intermittent therapy in cavitary MAC.1 In a prospective open-label, multicenter trial, culture conversions occurred in only 4% of patients with cavitary disease on a 3-times-weekly treatment regimen. Accordingly, intermittent therapy is not recommended for cavitary disease.1
It is suggested that treatment should be continued for at least 12 months after culture conversion, but there have been no randomized studies to examine this aspect of patient management.1 However, a single-center retrospective, observational cohort study evaluated treatment outcomes in patients with nodular/bronchiectatic MAC-LD, where a clarithromycin- or azithromycin-based combination was given either daily or 3 times a week to 27 patients for <12 months, and to 180 patients for ≥12 months.1 Culture conversion was significantly greater for patients who completed at least 12 months of therapy compared with those who were treated for <12 months (86% vs 22%; P<.001).1 However, neither this study nor studies included in a subsequent systematic review that reported similar outcomes evaluated treatment outcomes by duration of treatment after culture conversion.1 A study in Japan reported bacteriologic relapse in 5% of patients when treatment was continued for <15 months after sputum culture conversion compared with zero patients who continued treatment for >15 months.1 Therefore, with a lack of randomized controlled trial data on the optimal duration of therapy, the guidelines continue to recommend the treatment duration that was included in the 2007 guidelines.1
These observations reinforce the importance of monitoring the mycobacterial culture response to therapy, as the time of sputum culture conversion defines the total duration of therapy.1 In addition, per the guidelines, lack of sputum culture conversion 6 months after guideline-based therapy defines a patient as treatment-refractory.1
Guideline Summary: Treating Macrolide-Susceptible MAC-LD
Management of patients with macrolide-susceptible MAC-LD is based on whether they have nodular/bronchiectatic or cavitary disease (Table).1 The 3-drug regimen of azithromycin, rifampicin, and ethambutol can be expanded for patients with cavitary disease, extensive nodular/bronchiectatic disease, or macrolide-resistant MAC to include parenteral amikacin or streptomycin 3 times a week.1 The standard dosing frequency is 3 times weekly for nodular/bronchiectatic disease and daily for cavitary disease.1 Alternative drugs for patients who are intolerant of—or whose isolates are resistant to—first-line drugs include clofazimine, moxifloxacin, linezolid (tedizolid), and bedaquiline.1
| Table. Recommended Treatment Regimens for MAC Lung Disease |
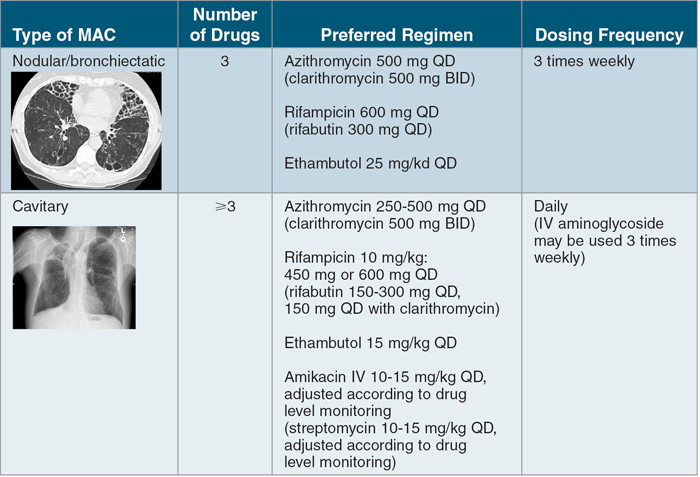 |
BID = twice daily; IV = intravenous; MAC = Mycobacterium avium complex; QD = daily.
Source: Adapted from Daley CL, et al.1 Images courtesy of CL Daley, MD. |
Patient Management
Testing for culture conversion should initially be done every 1 to 2 months, with “culture negative” defined as 3 consecutive negative sputum cultures.1,5 Subsequent testing every 2 to 3 months can be done while therapy continues to the target of 12 months after sputum culture conversion, designated as the date of the first negative culture.5 If the patient is failing therapy, follow-up should include repeat drug susceptibility testing to check for possible acquisition of macrolide resistance.6,7 One small retrospective study reported that recurrences due to relapse, compared with reinfection, occurred in fewer days after treatment completion (210 vs 671 days, respectively; P=.004), and recurrences were more likely to have increased macrolide MICs compared with the reinfection group (P=.002).8
Treating Refractory NTM-LD
Amikacin, in either the parenteral or the amikacin liposome inhalation suspension (ALIS) formulation, is not recommended for patients with newly diagnosed MAC-LD.1 However, 2 randomized controlled trials have demonstrated the safety and efficacy of ALIS in treatment-refractive pulmonary disease.9,10 Significantly more patients who received ALIS (590 mg/day) plus guideline-based therapy (GBT) achieved culture conversion by month 6 compared with those receiving GBT only.9 At the primary endpoint, conversion to negative cultures was achieved by 29% and 9% of patients receiving ALIS + GBT and GBT only, respectively (odds ratio, 4.22; 95% CI, 2.08-8.57; P <.001). Patients receiving ALIS were almost 4 times more likely to convert to negative cultures (Figure 1). Accordingly, for patients with therapy failure after ≥6 months following treatment guidelines, the 2020 guidelines now recommend the addition of ALIS (590 mg/day) to a guideline-based treatment regimen for patients with refractory disease.1 The ALIS formulation received FDA-accelerated approval in 2018 for treating adults who have limited or no alternative treatment options for treating MAC-LD,11 as part of a combination antibacterial drug regimen in patients who do not achieve negative sputum cultures after ≥6 consecutive months of multidrug background therapy.12 Practitioners should remain alert for respiratory adverse reactions in patients treated with ALIS. Dysphonia was the most commonly reported adverse event in clinical trials, typically peaking within the first month of therapy with declining rates thereafter.9 For cavitary disease, parenteral amikacin may be more effective than ALIS, as inhaled treatment is less likely to have adequate deposition into cavitary areas, although no studies have compared the 2 approaches.13
| Figure 1. Addition of ALIS to Patients With Refractory MAC-LD Improves Sputum Conversion |
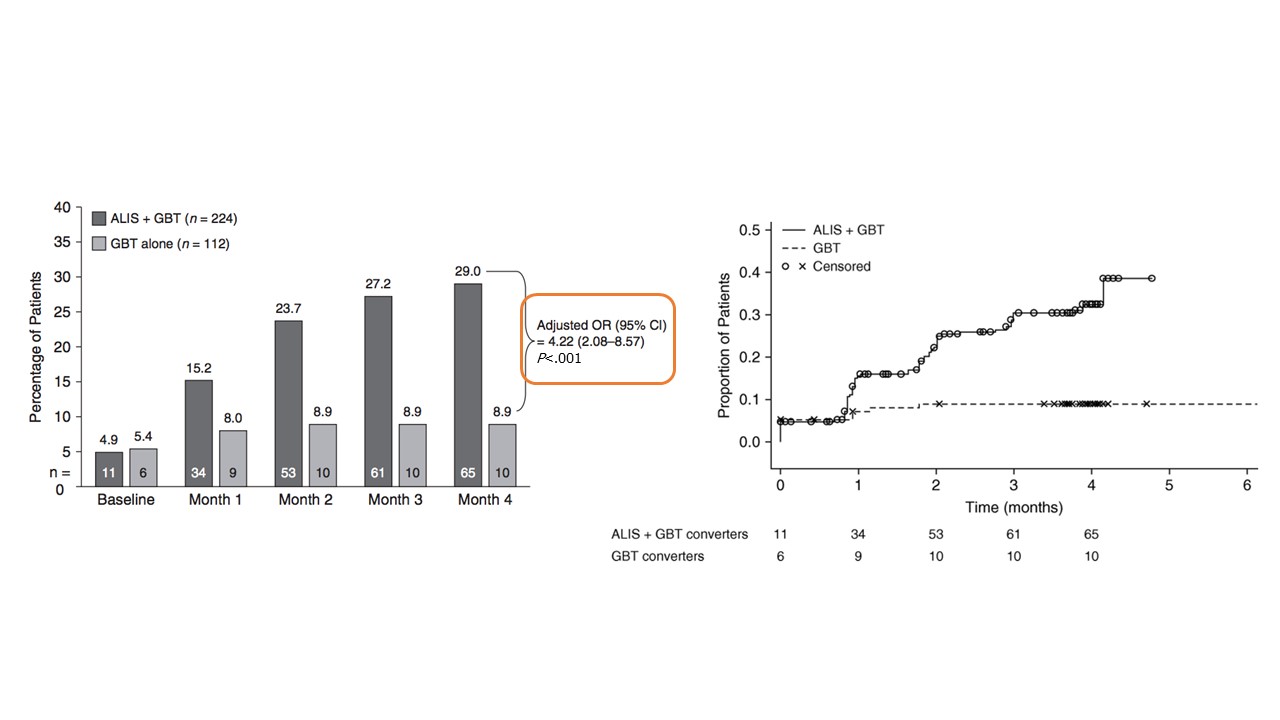 |
ALIS = amikacin liposome inhalation suspension; GBT = guideline-based therapy; MAC = Mycobacterium avium complex;
OR = odds ratio.
Source: Griffith et al.9 Reprinted with permission of the American Thoracic Society. Copyright © 2021 American Thoracic Society. All rights reserved. The American Journal of Respiratory and Critical Care Medicine is an official journal of the American Thoracic Society. |
Patients who have treatment failure on intermittent therapy can be switched to daily therapy.14 A study in South Korea reported 30% conversion to negative cultures in a small group of patients who started daily therapy after failing an intermittent regimen.1
Drug substitutions or additions to the regimen may be successful.1 The potential benefits of clofazimine, moxifloxacin, and bedaquiline have been examined in retrospective studies of patients with refractory MAC-LD, and culture conversion rates of approximately 30% have been reported.1,3
Surgery may be indicated for patients with MAC-LD whose disease is unresponsive to medication.5 Selected patients with acquire drug resistance or those who develop large cavities, uncontrolled symptoms, hemoptysis, or destroyed lung tissue may benefit from surgical resection.1
New Investigational Treatments for MAC-LD
Research priorities for NTM-LD focus on specific treatments and clinical outcome improvements.3 Treatment goals include having more effective drugs with a shorter treatment duration and identifying predictors of treatment response.3 Clinical outcome goals include developing a composite measure of disease activity or severity and identifying and validating biomarkers associated with disease risk, prognosis, and treatment response.3
Potential new treatments are focused on 4 main approaches (Figure 2).3 Repurposed antimicrobials include bedaquiline, clofazimine, and tedizolid, which are currently being used off-label.3 These require additional investigation, including alternate administration routes.3 New antimicrobials or novel formulations of existing drugs include gyrase inhibitors, new aminoglycosides, oral amikacin, and inhaled clofazimine.3 Nitric oxide, granulocyte-macrophage colony-stimulating factor, and gallium are nonmicrobial drugs that are being investigated for their safety and efficacy as inhaled formulations.3 Other treatment approaches beyond conventional therapeutics, such as bacteriophages, are also being investigated.3,15
| Figure 2. Potential New Treatment Approaches for MAC-LD |
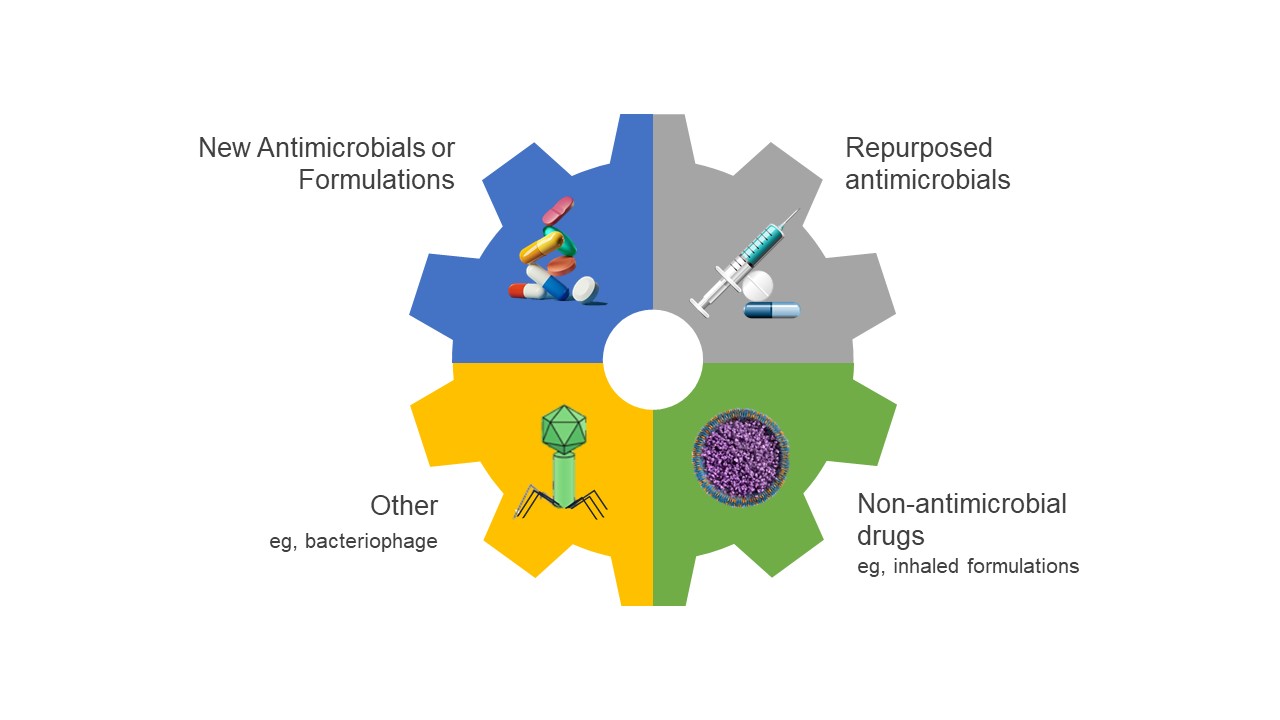 |
MAC-LD = Mycobacterium avium lung disease.
Source: Daley CL, et al.3 |
Summary
Treatment of NTM-LD is recommended over watchful waiting, especially for patients with risk factors for progression.1 Initial treatment of MAC-LD should include a 3-drug, macrolide-containing regimen administered for 12 months beyond culture conversion, using intermittent therapy for noncavitary disease and daily therapy for cavitary disease.1 Parenteral amikacin (or streptomycin) should be considered for cavitary, extensive bronchiectatic, and macrolide-resistant disease.1 Clinical, radiographic, and microbiologic data (cultures every 1 to 2 months) should be monitored to assess response to therapy.1 In treatment-refractory disease, ALIS should be added to guideline-based therapy.1
References
- Daley CL, Iaccarino JM, Lange C, Cambau E, Wallace RJ, Andrejak C, et al. Treatment of nontuberculous mycobacterial pulmonary disease: an official ATS/ERS/ESCMID/IDSA Clinical Practice Guideline: Executive Summary. Clin Infect Dis. 2020;71(4):e1-e36.
- Hwang JA, Kim S, Jo KW, Shim TS. Natural history of Mycobacterium avium complex lung disease in untreated patients with stable course. Eur Respir J. 2017;49(3):1600537.
- Daley CL, Winthrop KL. Mycobacterium avium complex: addressing gaps in diagnosis and management. J Infect Dis. 2020;222(Suppl 4):S199-S211.
- Kobashi Y, Matsushima T, Oka M. A double-blind randomized study of aminoglycoside infusion with combined therapy for pulmonary Mycobacterium avium complex disease. Respir Med. 2007;101(1):130-138.
- Griffith DE, Aksamit TR. How I do it: managing M avium complex lung disease with a little help from my friend. Chest. 2020;159(4):1372-1381.
- Haworth CS, Banks J, Capstick T, Fisher AJ, Gorsuch T, Laurenson IF, et al. British Thoracic Society guidelines for the management of non-tuberculous mycobacterial pulmonary disease (NTM-PD). Thorax. 2017;72(Suppl 2):ii1-ii64.
- Woods G, Brown-Elliott B, Conville P, Desmond EP, Hall GS, Lin G, et al. Susceptibility Testing of Mycobacteria, Nocardiae, and Other Aerobic Actinomycetes; Approved Standard. 2nd ed. Wayne, PA: Clinical and Laboratory Standards Institute (CLSI); 2011.
- Boyle DP, Zembower TR, Qi C. Relapse versus reinfection of Mycobacterium avium complex pulmonary disease. Patient characteristics and macrolide susceptibility. Ann Am Thorac Soc. 2016;13(11):1956-1961.
- Griffith DE, Eagle G, Thomson R, Aksamit TR, Hasegawa N, Morimoto K, et al. Amikacin liposome inhalation suspension for treatment-refractory lung disease caused by Mycobacterium avium complex (CONVERT). A prospective, open-label, randomized study. Am J Respir Crit Care Med. 2018;198(12):1559-1569.
- Olivier KN, Griffith DE, Eagle G, McGinnis JP, 2nd, Micioni L, Liu K, et al. Randomized trial of liposomal amikacin for inhalation in nontuberculous mycobacterial lung disease. Am J Respir Crit Care Med. 2017;195(6):814-823.
- US Food and Drug Administration. FDA approves a new antibacterial drug to treat a serious lung disease using a novel pathway to spur innovation. Published September 28, 2018. Accessed April 11, 2021. https://www.fda.gov/news-events/press-announcements/fda-approves-new-antibacterial-drug-treat-serious-lung-disease-using-novel-pathway-spur-innovation
- Amikacin liposome inhalation suspension. Package insert. Insmed; 2020.
- Shirley M. Amikacin liposome inhalation suspension: a review in Mycobacterium avium complex lung disease. Drugs. 2019;79(5):555-562.
- Griffith DE, Aksamit TR. Therapy of refractory nontuberculous mycobacterial lung disease. Curr Opin Infect Dis. 2012;25(2):218-227.
- Pereira AC, Ramos B, Reis AC, Cunha MV. Non-tuberculous mycobacteria: molecular and physiological bases of virulence and adaptation to ecological niches. Microorganisms. 2020;8(9):2000535.
Patient Communication, Treatment Tolerability, and Management of Adverse Events
David Griffith, MD
The 2020 clinical practice guidelines for the treatment of nontuberculous mycobacterial (NTM) pulmonary disease were prepared by an expert panel selected by the American Thoracic Society, European Respiratory Society, European Society of Clinical Microbiology and Infectious Diseases, and Infectious Diseases Society of America.1 The multidisciplinary committee included a patient representative who was a full participant in each step of the guideline-development process.1 A comprehensive review of the literature through June 2018 assured that the resulting recommendations were based on the best available evidence regarding the identification and treatment of NTM lung disease (LD), including data on the efficacy and safety of treatment options.1 These recommendations can provide the basis for developing an optimum treatment plan in partnership with the patient.1
Practice Pearls: Nurturing Patient Adherence Before Developing the Treatment Plan
The long-term therapy burden of NTM-LD, hampered with frequent adverse events (AEs), can be a challenge to patient treatment adherence.2 Adherence with Mycobacterium avium complex (MAC) therapy can be facilitated when patients acquire understanding of:
- The disease process,
- Their personal prognosis,
- The risks and benefits of therapy (or no therapy),
- The potential AEs of therapeutic agents, and
- The dedication of the treating clinician to shepherd them through the ups and downs of therapy.3,4
Most patients are highly motivated to improve clinically, and they usually comply with frequent clinic visits, toxicity monitoring, and submission of samples for acid fast bacilli (AFB) analysis.5 Practitioners can more effectively partner with their patients to develop a treatment plan by providing adequate information and education that can help motivate treatment adherence. Practitioners should explain MAC-LD and bronchiectasis using appropriate language for each patient, and they should define the extent of the patient’s disease, including a review of the patient’s radiologic images. By explaining the patient’s prognosis, a clinician can correct any misinformation the patient received elsewhere, while summarizing the quality-of-life improvements the patient can expect with good adherence to therapeutic regimens.
Next, practitioners should explain the indications for and goals of therapy and relate these to the individual patient’s diagnostic criteria. Initially, the goal should be to eradicate MAC.6 However, for patients whose disease is refractory to treatment, the goals can shift to symptom control and suppression of MAC.7 Once a patient understands the disease, treatment options and expected outcomes can then be discussed—including consequences of no treatment—relating this discussion to the patient’s prognosis. Patients with slowly progressing disease should understand that they may enjoy a period of initial stability without treatment.
Some patients can clear the organism from their sputum by optimizing airway clearance alone.8 Accordingly, the importance of bronchiectasis management should be explained, and the role of optimizing airway clearance for both bronchiectasis and MAC management should be emphasized, including the significant symptom improvement experienced by some patients.8,9
However, the practitioner should be prepared to encounter some patients who have been told that the treatment is worse than the disease. In these situations, it is important to explain that this is not the experience of most patients.10 The practitioner should clarify that cure rates are not 100%; rather, there is an approximate 80% chance for most patients with nodular/bronchiectatic disease to have MAC eradication.1,11 Patients should also be informed that that MAC-LD is rarely fatal.10 In addition, patients should be informed that once therapy is completed, there is an approximate 25% to 50% risk that MAC will recur.12
Practice Pearls: Assuring Patient Understanding of the Comprehensive Management Plan
A multidisciplinary team is important for successful NTM-LD treatment, including a pulmonologist, respiratory therapist, infectious disease specialist, and—as warranted—a nutritionist. Team members cooperate to support the patient through the NTM-LD–management process.
After the physician presents the guideline-based recommendations, the expectations of the patient and physician should be discussed frankly. Differences in objectives and expectations should be reconciled based on the available evidence. Guideline-recommended antibiotics should be discussed with the patient, carefully describing the potential AEs and rates of occurence.1,8 This is especially important for the ocular-toxicity risk associated with ethambutol, which is greater for patients being treated for MAC-LD compared with tuberculosis treatment and most likely related to the longer duration of ethambutol exposure when treating MAC-LD.1,13 In addition, the risk may be greater when ethambutol is administered daily compared with an intermittent regimen.14 Patients should be counseled to report any new ocular symptoms that develop while on ethambutol therapy.
The basis for the 3-drug standard treatment should be explained, emphasizing that there are a limited number of effective antibiotics available for treating MAC-LD.1 Therefore, there are few options for replacement if one of the treatment drugs must be discontinued.1
The critical importance of adherence with the prescribed regimen should be persuasively presented to the patient. A patient should understand the risk of drug-resistant MAC emergence, which greatly diminishes the chance for treatment success.15
The plans for monitoring and mitigating AEs in those who develop them should be discussed with the patient.1 A retrospective study of adult patients treated for NTM-LD at 5 French hospitals between 2010 and 2015 included 71 patients with NTM-LD, of whom 45 had MAC.16 In the entire cohort, 20% stopped treatment prematurely, and 31% had regimen changes due to poor treatment tolerance.16 Rapid identification of an adverse drug reaction may possibly improve treatment completion.16 Although the optimum frequency of AE monitoring has not been identified, follow-up should be performed at 1- to 2-month intervals, with additional visits in response to patient inquiries and other needs.1 Many symptoms can occur between visits, and patients should be told to not wait until their next appointment to report them, particularly with new ocular symptoms.17 Patients should know that dosage and regimen adjustments can be made, as warranted, to help resolve symptoms.
Assessing the patient’s clinical response is also based on the 3 pillars of diagnosis: symptoms, microbiology, and radiology.18 In addition to the status of their symptoms, their sputum will be tested for conversion to AFB culture negativity, and their chest computed tomography (CT) scans will be examined for improvement.1 The guideline-based duration of therapy should be discussed with the patient, assuring they accept that treatment will continue for 12 months after achieving sputum culture negativity.1
Antibiotic Intolerance and Managing AEs
The currently available therapies for NTM-LD are associated with significant AEs.12,19 Despite concerns that many patients are unable to complete their treatment due to AEs, several studies support that most patients are able to finish treatment.11 A recent online survey acquired responses from 347 patients with bronchiectasis and/or NTM-LD regarding various aspects of their disease.20 Concerns about drug-related AEs was a factor related to not accepting treatment for 36% of the untreated patients, while AEs were reported as a cause for treatment discontinuation by only 8%.20
Azithromycin and Clarithromycin
Macrolides are the most important class of agents in the MAC-treatment regimen.1 There is no alternative class that has equal clinical efficacy.1 Common AEs with macrolides include gastrointestinal symptoms, such as abdominal pain, nausea, flatulence, vomiting, dyspepsia, and anorexia. Further, ototoxicity can occur, including tinnitus and hearing loss.1,21,22 Baseline audiometry is warranted and should be continued intermittently during treatment.21
Hypersensitivity has occasionally been observed with macrolides; however, some studies indicate that cross-reactivity between the 2 macrolides does not always occur.23 Therefore, a patient who develops a rash with clarithromycin may tolerate azithromycin.23 Hepatitis is an uncommon but potentially serious AE of macrolide therapy.1,21 Liver function tests should be performed at 1- to 3-month intervals during treatment.21 Finally, macrolide treatment also may be associated with potentially serious QTc prolongation.21 Accordingly, electrocardiogram (ECG) monitoring should be performed at baseline and 2 weeks after starting therapy.21
Ethambutol
The main safety concern with ethambutol treatment is ocular toxicity.14 In some studies, ocular toxicity incidence ranged from 3% to 8% for patients taking daily ethambutol, and in 1 study, no patients on intermittent therapy were diagnosed with ocular toxicity.14,22 However, ocular toxicity risk grows with increasing drug exposure and typically becomes evident 3 to 6 months after starting therapy.24 Blurred vision and color vision disturbance are the most common manifestations, warranting baseline and ongoing visual acuity and color discrimination tests.25 Fundoscopic examination should be done at baseline and every 3 months during treatment.14 Patients should report any visual disturbances when they occur and be referred to an ophthalmologist for further investigation.14
Peripheral neuropathy has also been reported during ethambutol treatment.1,5 Accordingly, clinical monitoring, which can include neurologic examination, blood tests, imaging, and nerve function tests, is recommended.1,26
Ethambutol is the most important drug for protecting against the emergence of macrolide resistance and is not easily replaced.8 Patients who have a hypersensitivity reaction to ethambutol may not need to discontinue treatment, as successful desensitization protocols are available.27
Rifamycins
Two rifamycins, rifabutin and rifampin, have been used to treat NTM-LD.1 Rifabutin has better efficacy compared with rifampin; however, it is less well tolerated, and there is overlap in some AEs associated with both treatments.1,8 Both drugs cause orange discoloration of secretions, which is not a toxicity.25 However, patients should be informed to expect orange urine and—possibly—tears, sweat, and sputum.21,25 Cytopenias can occur with both drugs, warranting baseline complete blood count and comprehensive metabolic panel with follow-up every 1 to 3 months.1 Hypersensitivity has also been observed with both drugs.1,8 Retrospective studies showed that switching from rifampin to rifabutin can be successfully achieved in many patients without hypersensitivity recurrence.28,29 Uveitis reports have been limited to rifabutin,1,25 and rifabutin has been more frequently associated with arthralgia syndrome and fever.13,28
Hepatotoxicity is uncommon during treatment with the rifamycins and is primarily observed in patients with underlying hepatic disease.1,25 A recent expert panel survey of drug toxicity found that ongoing surveillance was adequate for mild rifampicin-associated alanine aminotransferase (ALT) and/or aspartate transaminase (AST) elevations, while treatment interruption or a switch to a rifamycin-free regimen was warranted in response to severe hepatotoxicity (ALT and/or AST concentrations >5 times the upper limit of normal).22 In 1 study, >90% of patients with MAC-LD did not have a recurrence of hepatotoxicity after rifampicin reintroduction.30
Rifampin is a strong inducer of the hepatic and intestinal cytochrome P-450 enzymes and the P-glycoprotein transport system.31 Accordingly, it is associated with a considerable number of clinically significant drug interactions.31 Rifabutin is also associated with drug interactions that are typically less severe than those observed with rifampin.32 Rifabutin may replace rifampin in the 3-drug regimen if rifampin is precluded by drug interactions.8,12 Because both drugs have considerable drug–drug interaction potential, a review of all co-administered medications is necessary throughout patient management.21,25
Rifampin has also been associated with drug-induced hypersensitivity.32 Retrospective studies have shown that substituting rifabutin for rifampin can be successful for many patients without recurrence of the events.28,29 Clofazimine is also an acceptable substitute for rifampin, and it has efficacy that may be equal to that of rifampin.8
Parenteral Amikacin
Adverse drug reactions associated with parenteral amikacin and other aminoglycoside drugs include vestibular toxicity, ototoxicity, nephrotoxicity, and electrolyte disturbances.1,33 Monitoring for these reactions is necessary, with regular follow-up while the patient is on treatment.33 A baseline audiogram should be repeated as indicated, and similarly, vestibular testing with follow-up as clinically indicated is warranted for patients taking parenteral amikacin.34
Routine peak amikacin level analysis should be performed, and the dose adjusted according to the targeted drug monitoring level.1,25,33 Although the optimal level is not known,25 daily dosing should target a peak of 35 to 45 µg/mL, and intermittent dosing should target a peak of 65 to 80 µg/mL, with a trough level <5 µg/mL.1
Amikacin Liposome Inhalation Suspension
Amikacin liposome inhalation suspension (ALIS) is approved for treating refractory MAC-LD after ≥6 months of unsuccessful multidrug therapy.34 In the CONVERT randomized trial that provided data contributing to its FDA approval, respiratory AEs were more common in the group with ALIS added to the background regimen compared with those receiving only the background regimen.35 Dysphonia (46% vs 1%), cough (37% vs 15%), and dyspnea (22% vs 9%) usually occurred in the first month after starting treatment, with declining incidence of new-onset AEs thereafter.12 In addition, audiologic treatment-emergent AEs were more common with ALIS, warranting baseline and routine audiogram monitoring.1,12 Using strategies to reduce the risk of dysphonia and cough can be beneficial.1 For example, one could predose with a bronchodilator or take a break in therapy and restart treatment on a 3-times-a-week regimen and then increase to the indicated daily dose, when possible.1,12,35 Spirometry should be measured at baseline and repeated as necessary (eg, for cough or shortness of breath).12,35 In cases of persistent or severe shortness of breath, in-depth evaluation including CT scan may be necessary to rule out hypersensitivity pneumonitis, which occurred in 3.1% of patients treated with ALIS in clinical trials.34
Clofazimine
Clofazimine has been associated with gastrointestinal AEs in as many as 50% of patients, including abdominal pain, nausea, vomiting, diarrhea, and weight loss.21 A skin discoloration resembling suntanning occurs within 1 to 4 weeks in 75% to 100% of patients. Patients should be advised of this AE before starting treatment and should be reassured that it usually disappears within 6 to 12 months after stopping treatment. Hepatotoxicity has been observed, and patients should receive routine clinical monitoring and liver enzyme tests.1 Similarly, ECG at baseline and during follow-up is recommended, due to possible QTc elongation.
Pearls for Antibiotic AE Management
Most experts recommend gradual introduction of MAC medications, such as adding additional medications at 1- to 2-week intervals.13 Intermittent 3-times-a-week therapy using the standard macrolide-based regimen is better tolerated, in general, compared to daily therapy.1 There are no persuasive data indicating that daily therapy is more effective than intermittent therapy for nodular/bronchiectatic MAC-LD.8,36 However, there also is no evidence to support using intermittent therapy for cavitary MAC-LD, for which once-daily therapy is recommended.8
Brief interruptions in therapy do not jeopardize the chance of clinical success, and some experts advocate this as a means of responding to tolerance issues for some drugs.22 There have been anecdotal reports of splitting doses or taking medication at night to achieve improved tolerance for some patients. Although taking medications with food may not be optimal, it may allow a patient to better tolerate the medication and may be an acceptable alternative.
Evaluating Clinical Response to Therapy
The duration of therapy is based on the time of culture conversion; that is, treatment should continue for 12 months after serum conversion.1,8 Therefore, sputum AFB cultures should be obtained frequently during treatment follow-up.1,8 The guidelines recommend obtaining specimens for culture at 1- to 2-month intervals.1 Although chest CT can be used to monitor radiographic response to therapy, the frequent association with underlying lung disease can result in variable and nonspecific findings.37 Accordingly, CT investigations should be assigned to the start and end of therapy, with other investigations as needed to answer a specific question. A chest X-ray may be performed every 3 to 6 months.8
A tool for evaluating NTM symptoms, the NTM Module, has been developed and it recently underwent preliminary validation in patients with MAC-LD.38 In this study, the NTM Module was administered at patient enrollment and after 12 months of treatment. It comprises 4 domain scores, based on 1-week recall of 1) NTM nonrespiratory symptoms, 2) body image, 3) digestive symptoms, and 4) eating problems.38 Each domain has a total possible score of 100, with a higher score indicating better functioning.38 The 7 items in the NTM symptoms domain include feverishness, sensitivity to smell, sensitivity to taste, memory problems, bad taste in the mouth, being bothered by cold weather, and problems sleeping.38 Patients in the validation cohort that started treatment had statistically significant increases in all domains, including NTM symptoms, with an average 5-point increase overall (P=.04), and there was an increase of 15 points (P=.002) in 16 patients whose baseline scores were ≤80.38
Summary
As it is a complicated disease to manage, MAC-LD requires good communication and a multidisciplinary team effort, with the patient at the center. The clinical practice guidelines for the treatment of NTM-LD are based on a comprehensive review and interpretation of the existing literature.1 Each recommendation is supported by a summary of the evidence and implementation details.1 Using these guidelines, clinicians and their patients can develop a management plan together that includes awareness of and strategies for responding to the side effects that are associated with each drug. Proper implementation of the guidelines can contribute to better tolerability and improved outcomes.
References
- Daley CL, Iaccarino JM, Lange C, Cambau E, Wallace RJ, Andrejak C, et al. Treatment of nontuberculous mycobacterial pulmonary disease: an official ATS/ERS/ESCMID/IDSA Clinical Practice Guideline: Executive Summary. Clin Infect Dis. 2020;71(4):e1-e36.
- Chalmers JD, Balavoine C, Castellotti PF, Hugel C, Payet A, Wat D, et al. European Respiratory Society International Congress, Madrid, 2019: nontuberculous mycobacterial pulmonary disease highlights. ERJ Open Res. 2020;6(4):00317-02020.
- Lipman M, Cleverley J, Fardon T, Musaddaq B, Peckham D, van der Laan R, et al. Current and future management of non-tuberculous mycobacterial pulmonary disease (NTM-PD) in the UK. BMJ Open Respir Res. 2020;7(1):e000591.
- Center for Drug Evaluation and Research, US Food and Drug Administration. The Voice of the Patient: A series of reports from the US Food and Drug Administration’s (FDA’s) Patient-Focused Drug Development Initiative—Non-Tuberculous Mycobacterial (NTM) Lung Infection Published April 2016. Accessed April 11, 2021. https://www.fda.gov/media/96932/download
- Wallace RJ, Jr., Brown-Elliott BA, McNulty S, Philley JV, Killingley J, Wilson RW, et al. Macrolide/azalide therapy for nodular/bronchiectatic Mycobacterium avium complex lung disease. Chest. 2014;146(2):276-282.
- Kasperbauer SH. National Jewish Health. NTM: Treatment. Published July 1, 2017. Accessed April 11, 2021. https://www.nationaljewish.org/conditions/ntm-nontuberculous-mycobacteria/ntm-nontuberculous-mycobacteria-overview/treatment
- Philley JV, DeGroote MA, Honda JR, Chan MM, Kasperbauer S, Walter ND, et al. Treatment of non-tuberculous mycobacterial lung disease. Curr Treat Options Infect Dis. 2016;8(4):275-296.
- Griffith DE, Aksamit TR. How I do it: managing M avium complex lung disease with a little help from my friend. Chest. 2020;159(4):1372-1381.
- Swenson C, Lapinel NC, Ali J. Clinical management of respiratory adverse events associated with amikacin liposome inhalation suspension: results from a patient survey. Open Forum Infect Dis. 2020;7(4):ofaa079.
- Mirsaeidi M, Machado RF, Garcia JG, Schraufnagel DE. Nontuberculous mycobacterial disease mortality in the United States, 1999-2010: a population-based comparative study. PLoS One. 2014;9(3):e91879.
- Novosad S, Henkle E, Winthrop KL. The challenge of pulmonary nontuberculous mycobacterial infection. Curr Pulmonol Rep. 2015;4(3):152-161.
- Daley CL, Winthrop KL. Mycobacterium avium complex: addressing gaps in diagnosis and management. J Infect Dis. 2020;222(Suppl 4):S199-S211.
- Griffith DE, Aksamit T, Brown-Elliott BA, Catanzaro A, Daley C, Gordin F, et al. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007;175(4):367-416.
- Griffith DE, Brown-Elliott BA, Shepherd S, McLarty J, Griffith L, Wallace RJ, Jr. Ethambutol ocular toxicity in treatment regimens for Mycobacterium avium complex lung disease. Am J Respir Crit Care Med. 2005;172(2):250-253.
- Pan SW, Shu CC, Feng JY, Su WJ. Treatment for Mycobacterium avium complex lung disease. J Formos Med Assoc. 2020;119 Suppl 1:S67-S75.
- Balavoine C, Blanc F-X, Lanotte P, Meurice JC, Andrejak C, Marchand-Adam S. Adverse events during treatment of nontuberculous mycobacterial lung disease: do they really matter? Eur Respir J. 2018;52(suppl 62):PA2664.
- Ryu YJ, Koh WJ, Daley CL. Diagnosis and treatment of nontuberculous mycobacterial lung disease: clinicians' perspectives. Tuberc Respir Dis (Seoul). 2016;79(2):74-84.
- Mirsaeidi M, Farshidpour M, Allen MB, Ebrahimi G, Falkinham JO. Highlight on advances in nontuberculous mycobacterial disease in North America. Biomed Res Int. 2014;2014:919474.
- Adjemian J, Daniel-Wayman S, Ricotta E, Prevots DR. Epidemiology of nontuberculous mycobacteriosis. Semin Respir Crit Care Med. 2018;39(3):325-335.
- Shteinberg M, Boyd J, Aliberti S, Polverino E, Harris B, Berg T, et al. What is important for people with nontuberculous mycobacterial disease? An EMBARC-ELF patient survey. ERJ Open Res. 2021;7(1):00807-02020.
- Haworth CS, Banks J, Capstick T, Fisher AJ, Gorsuch T, Laurenson IF, et al. British Thoracic Society guidelines for the management of non-tuberculous mycobacterial pulmonary disease (NTM-PD). Thorax. 2017;72(Suppl 2):ii1-ii64.
- van Ingen J, Aliberti S, Andrejak C, Chalmers JD, Codecasa LR, Daley CL, et al. Management of drug toxicity in M. avium complex pulmonary disease – an expert panel survey. Clin Infect Dis. Published online September 10, 2020. doi:10.1093/cid/ciaa1361
- Shaeer KM, Chahine EB, Varghese Gupta S, Cho JC. Macrolide allergic reactions. Pharmacy (Basel). 2019;7(3):135.
- Graham SM, Daley HM, Banerjee A, Salaniponi FM, Harries AD. Ethambutol in tuberculosis: time to reconsider? Arch Dis Child. 1998;79(3):274-278.
- Shulha JA, Escalante P, Wilson JW. Pharmacotherapy approaches in nontuberculous mycobacteria infections. Mayo Clin Proc. 2019;94(8):1567-1581.
- Mayo Clinic. Peripheral neuropathy. Accessed April 12, 2021. https://www.mayoclinic.org/diseases-conditions/peripheral-neuropathy/diagnosis-treatment/drc-20352067
- Siripassorn K, Ruxrungtham K, Manosuthi W. Successful drug desensitization in patients with delayed-type allergic reactions to anti-tuberculosis drugs. Int J Infect Dis. 2018;68:61-68.
- Chien JY, Chien ST, Huang SY, Yu CJ. Safety of rifabutin replacing rifampicin in the treatment of tuberculosis: a single-centre retrospective cohort study. J Antimicrob Chemother. 2014;69(3):790-796.
- Lehloenya RJ, Dlamini S, Muloiwa R, Kakande B, Ngwanya MR, Todd G, et al. Therapeutic trial of rifabutin after rifampicin-associated DRESS syndrome in tuberculosis-human immunodeficiency virus coinfected patients. Open Forum Infect Dis. 2016;3(3):ofw130.
- Kamii Y, Nagai H, Kawashima M, Matsuki M, Nagoshi S, Sato A, et al. Adverse reactions associated with long-term drug administration in Mycobacterium avium complex lung disease. Int J Tuberc Lung Dis. 2018;22(12):1505-1510.
- Baciewicz AM, Chrisman CR, Finch CK, Self TH. Update on rifampin, rifabutin, and rifapentine drug interactions. Curr Med Res Opin. 2013;29(1):1-12.
- Horne DJ, Spitters C, Narita M. Experience with rifabutin replacing rifampin in the treatment of tuberculosis. Int J Tuberc Lung Dis. 2011;15(11):1485-1489.
- Amikacin Sulfate. Package insert. Sagent Pharmaceuticals; 2018.
- Amikacin liposome inhalation suspension. Package insert. Insmed; 2020.
- Griffith DE, Eagle G, Thomson R, Aksamit TR, Hasegawa N, Morimoto K, et al. Amikacin liposome inhalation suspension for treatment-refractory lung disease caused by Mycobacterium avium complex (CONVERT). A prospective, open-label, randomized study. Am J Respir Crit Care Med. 2018;198(12):1559-1569.
- Nakagawa T, Hashimoto H, Yagi M, Kogure Y, Sekimizu M, Saito AM, et al. Multicentre, open label, randomised controlled trial comparing intermittent versus daily treatment for non-cavitary nodular/bronchiectatic Mycobacterium avium complex lung disease with rifampicin, ethambutol and clarithromycin (iREC): study protocol. BMJ Open Respir Res. 2019;6(1):e000434.
- Agrawal A. Medscape. Imaging in Nontuberculous Mycobacterial Lung Infections. Updated October 13, 2016. Accessed April 12, 2021. https://emedicine.medscape.com/article/358828-overview#a3
- Henkle E, Winthrop KL, Ranches GP, Plinke W, Litvin HK, Quittner AL. Preliminary validation of the NTM Module: a patient-reported outcome measure for patients with pulmonary nontuberculous mycobacterial disease. Eur Respir J. 2020;55(1):1901300.
Cases Discussion
David Griffith, MD
Case 1
A 55-year-old man presented with a 40-pack history of cigarette smoking. He was diagnosed with Mycobacterium avium complex (MAC) lung disease (LD) in early 2019. He had bacterial pneumonia in August 2018 with partial recovery. However, he had residual fatigue, cough, sputum production, hemoptysis, and night sweats. Acid-fast bacilli (AFB) cultures obtained from a bronchoscopy in January 2019 were positive for MAC, which were susceptible to macrolide and amikacin. In April 2019, he was started on daily rifampin, ethambutol, and azithromycin.
Although he had some symptomatic improvement, his cough, sputum production, fatigue, and intermittent hemoptysis continued. There was also some radiographic improvement, primarily seen as diminished inflammation. However, he had persistent cavitary changes in his right upper lobe with irreversible lung destruction (Figure).
| Figure. Case 1: Radiologic Follow-up During Treatment |
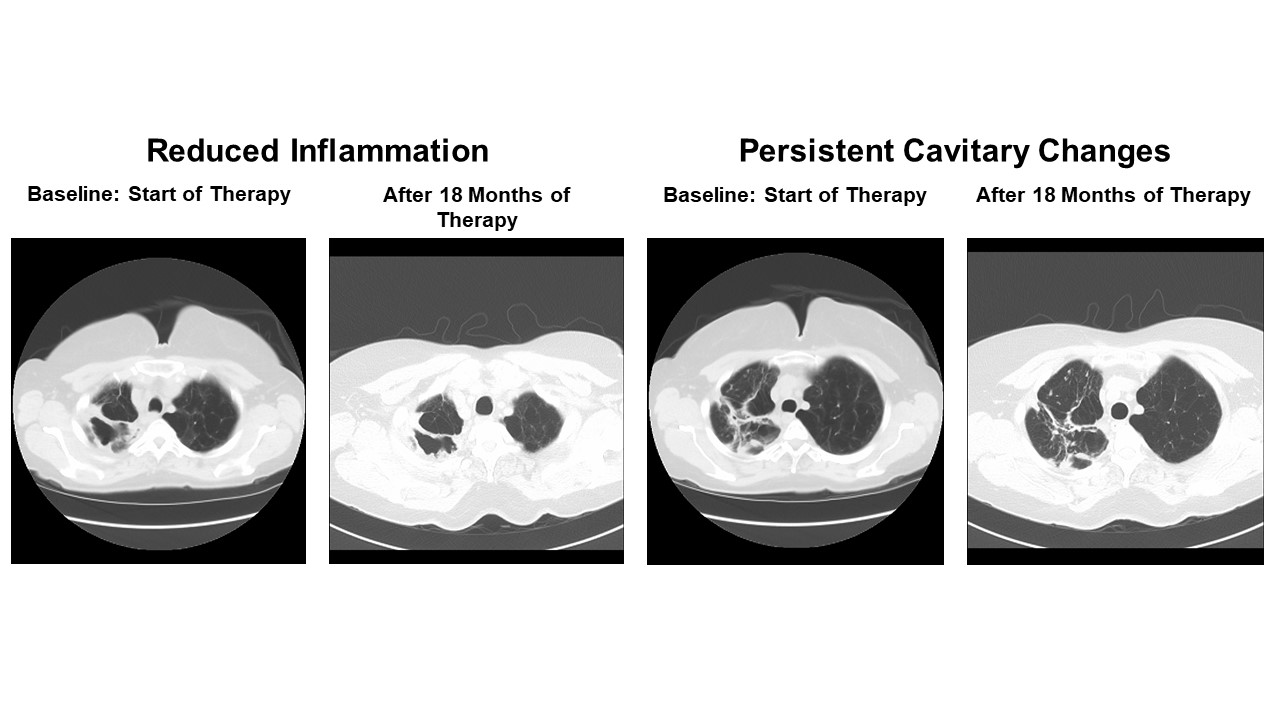 |
| Source: Images courtesy of David Griffith, MD. |
His sputum remained AFB culture positive for MAC after approximately 17 months of therapy, which remained both macrolide and amikacin susceptible. His forced expiratory volume in 1 second (FEV1) was 1.2 L, or 45% of predicted.
Options to treat refractory MAC-LD were considered. He had been following guideline-based therapy, was considered to be only a marginal surgical candidate, and was already following a daily treatment regimen. Although amikacin liposome inhalation suspension (ALIS) is considered a therapeutic option for refractory disease,1,2 the cavitation shown in this patient made parenteral amikacin a more appropriate approach.3 Continued macrolide sensitivity monitoring is warranted for this patient. If the patient is able to tolerate parenteral amikacin, he could be transitioned to inhaled formulations after a few months if he remained culture positive. Alternatively, he could be referred to a surgical physician with expertise managing marginal cases such as this.
Case 2
A 78-year-old woman with MAC-LD was referred for treatment. She was originally treated with rifampin/azithromycin/fluoroquinolone (FQ) based on findings from susceptibility testing that suggested ethambutol resistance and FQ susceptibility. However, this regimen was not in line with guideline-based therapy recommendations and unfortunately, her disease became macrolide-resistant.
Typically, following the guidelines for macrolide/azalide-based regimens for nodular/bronchiectatic MAC-LD results in favorable microbiologic outcomes for most patients, while not promoting development of macrolide resistance.4 Unfortunately, adherence with guideline-based therapy has been poor. Two large surveys examined poor adherence to management guidelines in patients with mycobacterial LD.5,6 One study surveyed a nationally representative sample of US physicians who were treating patients with pulmonary nontuberculous mycobacterial LD from December 2011 through January 2012 regarding treatment patterns for the last 4 patients they treated.6 Responses were compared with the 2007 American Thoracic Society/Infectious Diseases Society of America (ATS/IDSA) guideline recommendations.7 A total of 349 physicians provided questionnaire data on 915 patients (a 60% response).6 Survey data revealed that only 55% of the 747 patients with MAC were treated, and only 13% of the treatment regimens were consistent with guideline recommendations.6 Treatment for 56% of patients did not include a macrolide, and 16% were given macrolide monotherapy.6 An additional 14% of patients received other treatments that have been associated with an increased risk of developing macrolide resistance, including macrolide and rifampin only and/or macrolide plus FQ.6
Another survey study in 5 European countries and Japan reported that 42% of patients in Japan and 9% in the EU5 received >6 months of a rifamycin/ethambutol/macrolide regimen.5 The authors suggested that the difference could be due to more cases in Japan under pulmonologist care compared with Europe (54% vs 29%).5 Findings from a retrospective database review of 159 patient records in Germany between 2014 and 2019 also showed that guideline-based therapy was higher under specialist care, as it was provided to 45% of patients managed by 31 office-based pulmonologists and only 27% of patients managed by 125 general practitioners.8
The authors of these studies noted that poor guideline adherence could be due to the level of acquaintance with, or availability of, guidelines.5 In addition to lack of experience, low treatment persistence may have been associated with poor tolerability of the drug combinations or interactions from comorbidity-related polypharmacy.8 The authors concluded that significant educational efforts by professional societies are warranted to improve physician familiarity with and implementation of the ATS/IDSA guidelines,5,6 which provide succinct direction regarding treatment options in the setting of poor tolerability.9 These guidelines also help clarify the interpretation of susceptibility and emphasize the importance of patient adherence to the recommended regimens.9 In addition, referral pathways and collaboration between expert pulmonary treatment centers as well as primary or secondary care physicians can and should be improved.8
For this patient, misunderstanding and misinterpretation of MAC in vitro susceptibility reports resulted in the transition of macrolide-susceptible MAC lung disease to macrolide-resistant MAC lung disease. It cannot be over emphasized that the only 2 antimicrobial agents where in vitro susceptibility predicts treatment response are macrolides and amikacin. Clinicians cannot base MAC treatment decisions on in vitro susceptibility results for any other agents. That is especially true for ethambutol, where MAC minimum inhibitory concentrations are invariably high, but ethambutol remains the most important element in the macrolide-based therapy for preventing the emergence of macrolide resistance. Unfortunately for this patient, the emergence of macrolide resistance required that she receive parenteral amikacin in addition to ethambutol, clofazimine, and rifabutin. Treatment success for macrolide-resistant MAC usually requires both parenteral antibiotics and surgical resection of the involved lung tissue. This patient’s disease was primarily in the right upper lobe, so in addition to parenteral amikacin-based therapy, she had a right upper lobectomy. With this combined approach, she was able to achieve sputum culture negativity, and she ultimately completed a course of therapy including 12 months with negative cultures.
References
- Griffith DE, Eagle G, Thomson R, Aksamit TR, Hasegawa N, Morimoto K, et al. Amikacin liposome inhalation suspension for treatment-refractory lung disease caused by Mycobacterium avium complex (CONVERT). A prospective, open-label, randomized study. Am J Respir Crit Care Med. 2018;198(12):1559-1569.
- Olivier KN, Griffith DE, Eagle G, McGinnis JP, 2nd, Micioni L, Liu K, et al. Randomized trial of liposomal amikacin for inhalation in nontuberculous mycobacterial lung disease. Am J Respir Crit Care Med. 2017;195(6):814-823.
- Amikacin Sulfate. Package insert. Sagent Pharmaceuticals; 2018.
- Daley CL, Iaccarino JM, Lange C, Cambau E, Wallace RJ, Andrejak C, et al. Treatment of nontuberculous mycobacterial pulmonary disease: an official ATS/ERS/ESCMID/IDSA Clinical Practice Guideline: Executive Summary. Clin Infect Dis. 2020;71(4):e1-e36.
- van Ingen J, Wagner D, Gallagher J, Morimoto K, Lange C, Haworth CS, et al. Poor adherence to management guidelines in nontuberculous mycobacterial pulmonary diseases. Eur Respir J. 2017;49(2):1601855.
- Adjemian J, Prevots DR, Gallagher J, Heap K, Gupta R, Griffith D. Lack of adherence to evidence-based treatment guidelines for nontuberculous mycobacterial lung disease. Ann Am Thorac Soc. 2014;11(1):9-16.
- Griffith DE, Aksamit T, Brown-Elliott BA, Catanzaro A, Daley C, Gordin F, et al. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007;175(4):367-416.
- Diel R, Obradovic M, Tyler S, Engelhard J, Kostev K. Real-world treatment patterns in patients with nontuberculous mycobacterial lung disease in general and pneumologist practices in Germany. J Clin Tuberc Other Mycobact Dis. 2020;20:100178.
- Daley CL, Winthrop KL. Mycobacterium avium complex: addressing gaps in diagnosis and management. J Infect Dis. 2020;222(Suppl 4):S199-S211.