
Expired activity
Please go to the PowerPak
homepage and select a course.
CBD, Hemp, and Pharmacist Implications: What’s It All About? “Ask the Experts” (Monograph)
OVERVIEW: CBD AND MEDICAL MARIJUANA
For millennia, the Cannabis sativa plant has been used by numerous cultures throughout the world for a variety of medical, religious, or recreational purposes.1,2 While Cannabis preparations were included in the US Pharmacopeia from 1851 to 1942, only in the 20th century have there been restrictions on the use of Cannabis and its constituents when the Marijuana Tax Act of 1937 effectively banned its legal use in the United States.2,3 Despite that ban, Cannabis has remained a common recreational drug of choice given the psychotropic effects associated with delta-9-tetrahydrocannabinol (THC), a major phytocannabinoid in the plant. After California approved the medical use of marijuana via Proposition 215 in 1996, a wave of marijuana legislation has swept the US, with 36 states and 4 territories passing laws establishing medical marijuana programs that allow the use of marijuana for approved medical purposes. Furthermore, 15 states and 3 territories have established adult marijuana use programs whereby the recreational use of marijuana by adults is permitted.4 The popularity of another Cannabis phytocannabinoid, cannabidiol (CBD), expanded with changes in hemp policy through the Farm Bill of 2018.5
CBD and THC have established medical purposes and several FDA-approved drug products are currently on the market, including Epidiolex (cannabidiol), Marinol (dronabinol capsules), Syndros (dronabinol oral solution), and Cesamet (nabilone).6-9 Of the FDA-approved products, Epidiolex contains plant-based CBD, and the others contain synthetic THC derivatives. This activity will discuss FDA-approved and OTC CBD products, as well as aspects of medical marijuana that are pertinent to pharmacists.
Differences Among Hemp, Marijuana, and Other Cannabis Derivatives
A brief description of hemp, marijuana, and cannabis (or Cannabis) may be helpful in establishing an understanding of the practical differences between the terms. Cannabis is the taxonomical name of the genus of plants within the Cannabaceae family. Species of Cannabis include C sativa, C indica, and C ruderalis. The number of species is not, however, universally accepted. Alternative designations suggest there is a single species (C sativa), or two species (C sativa and C ruderalis), where C indica is lumped into C sativa.10,11 When discussing Cannabis, strains of marijuana, which are different wild and cultivated breeds of the plant, have some importance. Over the years, more than 2500 strains (with colloquial names such as “Mango Kush,” “Purple Haze,” and “Harlequin”) have been created with the goal of imparting particular qualities and properties.12 A further distinction is made between Cannabis and hemp, which is also referred to as industrial hemp. Hemp is defined by US law as Cannabis that contains 0.3% or less of THC.5 For the purposes of this activity, the focus will be on C sativa and C indica and the terms Cannabis or marijuana will be used interchangeably.
Chemical Substances in the CannabisSativa Plant
Of the >550 chemicals produced by the Cannabis plant, there are two major classes of compounds with current medical interest: terpenes and phytocannabinoids. Over 100 chemicals from each class have been identified. The various Cannabis strains are known to produce a wide range of terpenes (including linalool, myrcene, limonene, pinene, and caryophyllene) that are believed to contribute to the sativa–indica spectrum of effects and cannabis odor.13 The abundance of terpenes and other phytochemicals in Cannabis has fostered the expansion of the theoretical “entourage effect” (originally attributed to endogenous fatty acid glycerol esters)14 to explain apparent differences between Cannabis strains, although the biochemical basis for the apparent strain effects remains uncertain.15,16
In the phytocannabinoid class of phytochemicals, the plant produces the carboxylic acid precursors of THC and CBD (THCA and CBDA, respectively) in the greatest amounts.17 While THC and CBD have identical chemical formulas, their slightly different chemical structures (FIGURE 1) result in very different pharmacology profiles.1 The effects of THC, which include psychoactivity, analgesia, sedation, antinausea/antiemetic, and appetite stimulation, among others, are attributed to its action as a partial agonist of cannabinoid-1 (CB1) and cannabinoid-2 (CB2) receptors.17
| FIGURE 1. Chemical Structures of THC, CBD, and d8-THC67-69 |
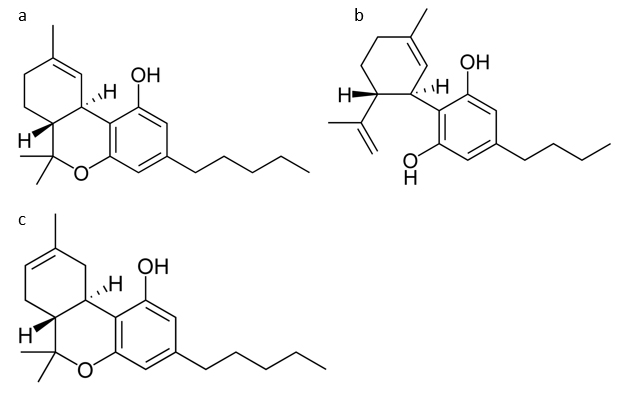 |
Chemical structures of (a) delta-9-tetrahydrocannabinol (THC); (b) cannabidiol (CBD); and
(c) delta-8-tetrahydrocannabinal (d8-THC).
Credit: Chemical structures are reproduced without alteration and published under the GNU Free Documentation License, Version 1.2, and the Creative Commons Attribution-ShareAlike 3.0 Unported license.66-68 > |
While the specific biochemical activity of CBD is not fully understood, CBD appears to act as a noncompetitive antagonist of CB1 and an inverse agonist of CB2 receptors.2,17,18 CBD’s actions at a wide range of receptors, channels, and enzymes outside of the endocannabinoid system contribute to its pharmacological effects, including inhibiting fatty acid amide hydrolase, resulting in increases in levels of anandamide.19,20 Although CBD does not possess psychotoxicity, CBD has neuroactivity that is beneficial for a variety of central nervous system (CNS) conditions, including epilepsy and related conditions.21 Other effects of CBD include anxiolytic and antipsychotic properties, and there is evidence that CBD curbs the psychoactivity of THC.17,20,22
Pharmacology
Research on the molecular pharmacology of psychoactivity of marijuana and THC in particular have led to the discoveries of cannabinoid receptors and endogenous cannabinoids of the endocannabinoid system. To date, two G protein-coupled cannabinoid receptors, CB1 and CB2, have been identified, while other associated receptors also appear to be involved in the endocannabinoid system.18 CB1 receptors are expressed primarily in the CNS while also being expressed in various peripheral sites such as the liver, skeletal muscle, cardiovascular system, reproductive system, and gastrointestinal tract.21,23 CB2 receptors, however, are primarily expressed in peripheral tissues and immune cells with some expression in the brain.2,18,21
The distribution of the CB1 and CB2 receptors influence the pharmacological effects of their ligands, agonists, and antagonists (FIGURE 2). Stimulation of CB1 receptors in the CNS contribute to observed effects such as cognition, short-term memory, sedation, altered motor function, and analgesia.2,18 Activation of CB2 receptors appears to produce anti-inflammatory effects via the immune system.24 The endogenous cannabinoids include N-arachidonylethanolamine (anandamide), 2-arachidonoylglycerol (2-AG), noladin ether, virodhamine, N-arachidonyldopamine (NADA), and oleamide.18,25 The multiple functions of endocannabinoids reflect the wide distribution of CB1 and CB2 receptors as well as other receptors of the endocannabinoid system. Such functions involve locomotion, cognition, mood, nociception, pain, and inflammation pathways.25
| FIGURE 2. Mechanism of Action of CBD19 |
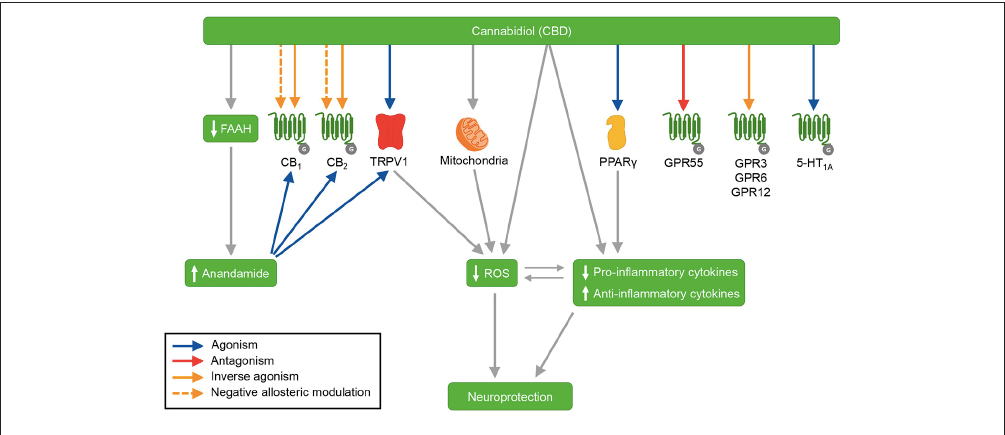 |
Depiction of the various mechanisms of action of CBD. Agonist activity: TRPV1, PPARG, and 5-HT1A. Antagonist activity: GPR55. Inverse agonist activity: GPR3, GPR6, and GPR12. CBD may act as an inverse agonist and negative allosteric modulator of the CB1 and CB2 receptors, leading to antagonism of agonists of those receptors. In addition, CBD inhibits the enzyme FAAH, leading to increased anandamide levels. CBD also exhibits antioxidant and anti-inflammatory effects via actions on TRPV1, mitochondria, and PPARG.
Abbreviations: 5-HT1A, serotonin receptor 1A; CB1, cannabinoid receptor type 1; CB2, cannabinoid receptor type 2; CBD, cannabidiol; FAAH, fatty acid amide hydrolase; GPR3, G-protein-coupled receptor 3; GPR6, G-protein-coupled receptor 6; GPR12, G-protein-coupled receptor 12; GPR55, G-protein-coupled receptor 55; PPARG, peroxisome proliferator-activated receptor gamma; ROS, reactive oxygen species; TRPV1, transient receptor potential vanilloid type 1.
Copyright © 2018 Peres, Lima, Hallak, Crippa, Silva, and Abílio. This figure is reproduced under the Creative Commons Attribution License (CC BY). |
Broad Uptake of CBD (and Medical Marijuana) Products by Consumers
While California paved the way for medical cannabis in 1996, decriminalization efforts, which typically reduced marijuana possession penalties to misdemeanors, began in the 1970s.26 Many states followed California’s lead in creating medical marijuana programs of one form or another, and those changes continue to evolve. Marijuana supporters subsequently advocated for the legalizing marijuana at the state level, and these efforts bore fruit with Colorado and Washington passing legislation in 2012 to legalize recreational marijuana. Similar to the timeline of medical marijuana programs, multiple states subsequently legalized recreational marijuana in adult-use programs. To date, 36 states and 4 territories have passed legislation for medical marijuana programs, while 15 states and 3 territories have passed laws to establish adult-use marijuana programs.4
As states adopt medical marijuana and adult-use marijuana programs, consumer demand for marijuana has exploded. Sales of medical marijuana were estimated at $4 to $4.9 billion in 2019, $5.8 to $7.1 billion in 2020, and projected to be in the range of $9.5 to $11.7 billion in 2024.27 The adult-use marijuana market takes a larger portion of sales with $6.6 to $8.1 billion in 2019, $9.7 to $11.8 billion in 2020, and an estimated $20.7 to $25.3 billion in 2024.27 Potential changes to the federal classification may be forthcoming from the new Biden-Harris Administration that would likely impact both the adult-use and medical marijuana markets.28
The popularity of CBD lagged behind medical marijuana but has subsequently increased as products containing or purporting to contain the cannabinoid have flooded the OTC and retail markets after the passage of the Farm Bill of 2018. The economics of CBD clearly affect the number of marketed OTC CBD products, where the size of the US CBD market has been estimated at $1 billion and expected to grow to $16 billion.29
Purity and Potency
While state level regulation of marijuana products has produced markets where products are tested regularly, the CBD market suffers from lax regulation. The lack of clarity and/or enforcement of FDA regulations may have led to the marketing of OTC CBD products that do not contain labeled amounts of CBD, make unsupported claims on efficacy, and/or contain potentially harmful contaminants.30 In one example, a study of 84 products from 31 companies found that approximately 69% of the products did not contain the labeled amount of CBD, with 36 products (43%) having >10% of the labeled content and 22 products (26%) having <10% of the labeled content.31 Over the past several years, the FDA has also sent warning letters to multiple companies regarding the marketing of unapproved CBD-containing products.32 Other studies and review articles highlight the potential public health issue of OTC CBD products based on the presence of contaminants and the lack of clinical evidence for effectiveness.21,33-36 Given such concerns, before recommending and/or selling CBD products to patients, pharmacists should ensure that such products are of sufficient quality and purity.
Currently, OTC CBD products are not subject to the stricter regulations of drugs, which has led to a flood of CBD and purported CBD products that are sold in establishments ranging from the local gas station to chain pharmacy stores. The FDA specifically states that such products are not approved by the agency.37 The somewhat gray legal area of OTC CBD products, the Farm Bill of 2018, and the apparent lax enforcement of current regulations has opened the market to a wide range of CBD-containing products.30 Furthermore, other interpretations of the Farm Bill of 2018 have contributed to recent attention on another naturally occurring cannabinoid, delta-8-tetrahydrocannabinol (d8-THC), which differs from THC by the location of a single double bond while retaining euphoric properties, although to a lesser extent than THC.38 Some retailers believe that the wording of the Farm Bill of 2018 allows for the sale and distribution of products containing d8-THC beyond registered marijuana dispensaries.39 The legality of d8-THC sales outside registered dispensaries, however, is not clear.
CBD IN NEUROLOGIC AND PSYCHIATRIC DISORDERS
Scientifically Proven Medical Benefits of CBD in Seizure Disorders
Through a series of preclinical studies, anecdotal case studies, and eventually clinical trials, the evidence for the use of CBD in treating epilepsy was established.40 A few of the anecdotal cases were broadcast through popular media, which, along with descheduling hemp, contributed to the current robust interest in CBD seen today.40,41 Inspired by such cases, robust clinical investigations of purified, plant-derived, liquid CBD for epilepsy was conducted with a focus on Dravet syndrome, Lennox-Gastaut syndrome, and tuberous sclerosis complex.40 Dravet syndrome and Lennox-Gastaut syndrome are rare epileptic encephalopathies characterized by multiple seizure types. Dravet syndrome often manifests early in life, and many patients with the condition have a mutation in a sodium channel gene. Persons with Lennox-Gastaut syndome have a very high seizure burden and often experience drop (atonic) seizures. Tuberous sclerosis complex is a genetic disorder characterized by an abundance of benign tumors and multiple types of seizures.40
Studies in Dravet syndrome used doses of CBD at 10 mg/kg/day and 20 mg/kg/day. In the first randomly controlled, double-blind study (NCT02091375), 120 patients were enrolled in the study ranging in age from 2.3 to 18.4 years.42 In the CBD treatment group, median monthly convulsive seizures decreased from 12.4 to 5.9, while in the placebo group median monthly convulsive seizures decreased from 14.9 to 14.2 (P = .01).42 Patients in the treatment arm experienced more adverse events, which included “diarrhea, vomiting, fatigue, pyrexia, somnolence, and abnormal results on liver-function tests.”42
The second study (NCT02224703) investigated the effects of liquid CBD formulation at 2 doses (10 or 20 mg/kg/day) as an add-on treatment to current antiepileptic drug therapy in 199 patients (2.2 to 18.9 years of age).43 The frequency of convulsive seizure decreased by 48.7% in the 10 mg/kg/day group and 45.7% in the 20 mg/kg/day group compared to 26.9% in the placebo group (P = .01 and P = 0.03, for 10 and 20 mg/kg/day, respectively).43 There appeared to be a dose-dependent increase in adverse events where 13 patients who received the higher CBD dose experienced elevated liver transaminase levels compared to 3 patients in the lower CBD dose group and none in the placebo group.43
Similar studies were conducted in patients with Lennox-Gastaut syndrome with a primary outcome of drop seizures.44,45 The first study (NCT02224560) investigated CBD alone at a dose of 10 mg/kg/day or 20 mg/kg/day compared to placebo with a total of 225 patients (2 to 55 years of age).44 Reductions in median percent drop-seizure frequency from baseline were greater in the CBD treatment groups compared to the placebo group. The placebo group exhibited a reduction of 17.2% while the seizure reduction in the 10 mg/kg/day group was 37.2% (P = .002 compared to placebo) and 41.9% in the 20 mg/kg/day (P = .005 compared to placebo).44 Dose-dependent adverse events were observed including diarrhea, decreased appetite, and somnolence, and adverse events led to the withdrawal of 1 patient in the lower dose CBD group and 6 patients in the higher dose CBD group.44 In the adjunctive CBD treatment study, 171 patients (2 to 55 years of age) received either placebo or CBD at 20 mg/kg/day in addition to concurrent antiepileptic therapy.45 A greater decrease in monthly drop seizure frequency from baseline was observed in the CBD treatment group (43.9%) compared to the placebo group (21.8%, P = .0135). Adverse events that were mild to moderate in nature occurred more frequently in the CBD group (86%) compared to the placebo group (69%).45
The studies established the efficacy of the liquid CBD formulation leading to the approval of Epidiolex for the treatment of Dravet syndrome, Lennox-Gastaut syndrome, and seizures associated with tuberous sclerosis complex in patients ≥1 year of age.6,46 Pharmacists should be familiar with Epidiolex dosing guidelines for Dravet syndrome and Lennox-Gastaut syndrome that recommend a gradual increase in dose starting at 5 mg/kg/day (in 2 divided doses) and increasing to 10 mg/kg/day (in 2 divided doses) after 1 week with a maximum dose of 20 mg/kg/day.6,46 For tuberous sclerosis complex patients, the recommended starting dose for the first week of treatment remains the same (5 mg/kg/day in 2 divided doses). Subsequently, the dose can be increased weekly by 5 mg/kg/day to the maximum recommended maintenance dose of 25 mg/kg/day (in 2 divided doses).6 Potential drug-drug interactions that may warrant dose adjustments include a decrease in CBD plasma concentration when coadministered with CYP3A4 and/or CYP2C19 inducers and an increase in the active metabolite of clobazam when coadministered with CBD.6,46
Other Neurologic and Psychiatric Conditions
Knowledge of the endocannabinoid system and the distribution of CB1 and CB2 receptors has led to considering CBD for a range of neurologic and psychiatric conditions. Such conditions include Huntington’s disease, Parkinson’s disease, psychosis, social phobia, generalized anxiety, and schizophrenia.21 Investigations of CBD with these conditions has been primarily limited to small pilot studies with fewer than 100 patients and with a variety of CBD formulations.21
Pharmacists should be aware of ongoing research into the potential applications of CBD. With the wide availability of OTC CBD products of varying quality, pharmacists should advise patients and caregivers on the proper use of such products, particularly for patients using Epidiolex. While possible adverse effects of CBD (based on the prescribing information for the FDA-approved CBD product) include hepatic injury, sedation/somnolence, and diarrhea,6 high doses of CBD (1500 mg/day) are reported to be well tolerated.47 A likely greater concern than combining OTC and prescription CBD products is the potential for OTC CBD products to be mislabeled in that they do not contain the labeled amount/concentration of CBD. As indicated above, the lack of regulation of OTC CBD products unsurprisingly created markets, both in the US and abroad, in which many products are mislabeled or contaminated.21,31,32,34,48
LEGAL IMPLICATIONS
The Farm Bill of 2018: What Does It Mean for Pharmacists?
The Agriculture Improvement Act of 2018 (ie, the “Farm Bill” of 2018)5 ushered in the gold rush of the CBD market by effectively descheduling hemp (cannabis plant that has ≤0.3% of THC by dry weight) as a controlled substance.41 Under the Controlled Substances Act (CSA), marijuana and compounds found within the plant are categorized as Schedule I substances, ie, chemicals that do not have a currently accepted medical use. By removing hemp from the CSA, the Farm Bill of 2018 opened the door for CBD products since the compound can be isolated from marijuana or hemp.41,49 While OTC CBD is readily available, the FDA has specified that food or dietary supplements cannot contain CBD no matter the source (eg, hemp or marijuana) even though hemp-derived CBD is no longer a controlled substance.41 The presence of CBD-containing products and the FDA stance on such products seems to contribute to consumer confusion regarding CBD. Pharmacists should be prepared to discuss the intricacies of the regulations and advise patients on the risks and benefits of OTC CBD products.
State-By-State Variance in Medical Marijuana Laws
As of publication time, 36 states and 4 territories have established some form of a medical marijuana program. Some of those states and another territory have also established adult marijuana use (or recreational marijuana) programs.4 In part due to lack of federal oversight, the state/territory programs will differ in many aspects (eg, available products, quantity/possession limits, allowable THC content). Two of the pertinent differences will be briefly discussed here¾THC content and the role of pharmacists. One such difference is the allowable THC content of products. While many state programs do not define limits on THC concentration of products, several state programs only allow products with low THC and high CBD concentrations (eg, Limited Access Marijuana Product Laws). In those limited access states, the allowable amount/concentration of THC varies from 0% to 5%.4
State laws on the roles of pharmacists in medical marijuana programs vary widely. The majority of state programs do not specify a defined role for pharmacists, and, thus, dispensaries in those states typically do not employ pharmacists even though medicines, in the form of marijuana products, are sold and dispensed to patients based on approved medical conditions. Common outlets where OTC CBD is sold (eg, grocery stores, gas stations) do not typically offer the opportunity for interaction with a pharmacist or health care provider. A handful of states specify roles for pharmacists in dispensing medical marijuana. For example, in Connecticut, only pharmacists can obtain a medical marijuana dispensary permit and the state rescheduled marijuana as a Schedule II controlled substance,50 while Louisiana’s medical marijuana program established specialty marijuana pharmacy licenses with the Louisiana Board of Pharmacy providing oversight.51 Other states require a pharmacist to be involved with a dispensary in one form or another. These states include Minnesota, New York, and Pennsylvania, which require a pharmacist on site, and Arkansas, which requires a pharmacist consultant for each dispensary, but not necessarily on site.52 Note that Pennsylvania requires a pharmacist or physician on site at the dispensary while also allowing a nurse practitioner or physician assistant when a dispensary has multiple locations.53
Implications of FDA Approval of Purified CBD
With the various OTC and prescription CBD products, as well as other products that claim to contain CBD or hemp oil, consumer/patient confusion can be expected. To help patients address the potential confusion, pharmacists can identify the differences between prescription cannabis-based products and OTC cannabis-based products. Prescription products undergo rigorous regulatory processes that include multiple clinical trials. Such trials provide the evidence needed to establish efficacy for FDA-approved therapeutic indications. Manufacturing of prescription formulations are subject to extensive FDA regulation, resulting in products with known and consistent ingredients. As a result of the testing and regulatory processes, prescription drug products have standardized doses and formulations.
On the other hand, OTC cannabis-based products are not subject to clinical trials. Health claims and therapeutic indications cannot be listed on labels. The OTC formulations and ingredients may be known and may be consistent, but not necessarily so. In addition, the lack of rigorous oversight can lead to variability in dosing and formulations. As a means to establish consumer confidence in the safety and quality of OTC cannabis-based products, manufacturers may submit their products to third-party testing, which would detail the concentration/potency of ingredients, contaminant analysis, and other pertinent information.54 Manufacturers are also beginning to use QR codes on labels so that consumers can access certificates of analysis via mobile devices.55
PHARMACIST CONSIDERATIONS
Patient Counseling Strategies
Pharmacists are uniquely trained to counsel patients, caregivers, and health care professionals on all aspects of pharmacotherapy, and counseling for medical marijuana and CBD products should be no exception.55,56 Counseling on FDA-approved THC, CBD, and cannabis-derived drugs should be standard procedure for pharmacists.56,57 Pharmacies are often points of sale for CBD products, although pharmacists may not feel entirely comfortable with recommending or counseling of CBD products.57 Aspects of pharmacist-driven counseling of medical marijuana and CBD products would include similar points as done for counseling conducted for standard prescription and OTC medications. Topics of medical uses, pharmacokinetics, administration, drug-drug interactions, adverse events, and precautions could all be tailored to particular products and routes of administration.55,56,59 Pharmacists, as drug expert resources, should also be forthcoming about the potential negative aspects of medical cannabis use, which can include cannabis use disorder.60
Pharmacists and other health care professionals may find resources from the Canadian Pharmacists Association and the Australian Centre for Cannabinoid Clinical and Research Excellence helpful for determining if medical marijuana is an appropriate therapy choice and for making dosing recommendations.61,62 Pharmacists and pharmacy students may recognize that they have not received sufficient education on the medical uses of marijuana.63,64 In response to changes in public acceptance, medical marijuana laws, and the need for more educations, colleges and schools of pharmacy are increasingly adding topics on medical marijuana and related products to their curricula.65,66
| TABLE 1. Summary of Differences Between Prescription and OTC Cannabis-Based Products |
| Prescription Cannabis-Based Products |
OTC Cannabis-Based Products |
- Rigorous regulatory process
- Rigorous clinical trials
- Evidence they work for therapeutic indications
- Ingredients are known and consistent
- Standardized dose and formulation
|
- No clinical trials
- No specific indications for any health claims should be included on the label
- Ingredients may be known and may be consistent (or may not be)
- Variable dosing and many different formulations
|
SUMMARY
The landscape of marijuana legalization in the US is rapidly changing both for medical and adult use purposes. As medical uses of marijuana and CBD products are investigated and accepted, pharmacists should be prepared to assert their established roles as medication experts. In particular, pharmacists can help patients navigate the difference between prescription cannabis-based products, OTC cannabis-based products, and medical marijuana products (TABLE 1). Different regulatory requirements (or lack thereof) apply to each type of product and pharmacists should be equipped to advise patients on those differences. A major difference is that prescription cannabis-based products have established medical indications (ie, seizure disorders, anorexia associated with AIDS, nausea/vomiting associated with chemotherapy) as a result of the FDA regulatory approval process. Changes in hemp regulation from the Farm Bill of 2018 have created actual or perceived relaxation in regulation of OTC cannabis-based products. With marijuana classified as a Schedule I drug on the federal level, variability in state regulations for medical and adult use marijuana produces a wide range of legal requirements. Continued changes in marijuana regulations at the state and federal levels will continue to evolve and pharmacists should keep up to date with those changes.
REFERENCES
- Atakan Z. Cannabis, a complex plant: different compounds and different effects on individuals. Ther Adv Psychopharmacol. 2012;2(6):241-254.
- Borgelt LM, Franson KL, Nussbaum AM, Wang GS. The pharmacologic and clinical effects of medical cannabis. Pharmacotherapy. 2013;33(2):195-209.
- Malone T, Gomez K. Hemp in the United States: a case study of regulatory path dependence. Appl Econ Perspect Policy. 2019;41(2):199-214.
- State medical marijuana laws. National Conference on State Legislatures. https://www.ncsl.org/research/health/state-medical-marijuana-laws.aspx. Accessed February 11, 2021.
- The Agriculture Improvement Act of 2018, Pub L No. 115-334 amending 21 USC §§802(16), 812(c).
- Epidiolex (cannabidiol) [package insert]. Carlsbad, CA: Greenwich Biosciences, Inc; 2020.
- Marinol (dronabinol capsules) [package insert]. North Chicago, IL: AbbVie, Inc; 2017.
- Syndros (dronabinol oral solution) [package insert]. Chandler, AZ: Insys Therapeutics, Inc; 2018.
- Cesamet (nabilone) [package insert]. Costa Mesa, CA: Meda Pharmaceuticals, Inc; 2015.
- Pollio A. The name of cannabis: a short guide for nonbotanists. Cannabis Cannabinoid Res. 2016;1(1):234-238.
- Schilling S, Melzer R, McCabe PF. Cannabis sativa. Curr Biol. 2020;30(1):R8-R9.
- Radhakrishnan R, Ranganathan M, D’Souza DC. Medical marijuana: what physicians need to know. J Clin Psychiatry. 2019;80(5):18ac13537.
- Hazekamp A, Fischedick JT. Cannabis - from cultivar to chemovar. Drug Test Anal. 2012;4(7-8):660-667.
- Ben-Shabat S, Fride E, Sheskin T, et al. An entourage effect: inactive endogenous fatty acid glycerol esters enhance 2-arachidonoyl-glycerol cannabinoid activity. Eur J Pharmacol. 1998;353(1):23-31.
- Santiago M, Sachdev S, Arnold JC, et al. Absence of entourage: terpenoids commonly found in cannabis sativa do not modulate the functional activity of Δ9-THC at human CB1 and CB2 receptors. Cannabis Cannabinoid Res. 2019;4(3):165-176.
- Cogan PS. The ‘entourage effect’ or ‘hodge-podge hashish’: the questionable rebranding, marketing, and expectations of cannabis polypharmacy. Expert Rev Clin Pharmacol. 2020;13(8):835-845.
- Rock EM, Parker LA. Constituents of cannabis sativa. Adv Exp Med Biol. 2021;1264:1-13.
- Pertwee RG, Howlett AC, Abood ME, et al. International Union of Basic and Clinical Pharmacology. LXXIX. Cannabinoid receptors and their ligands: beyond CB1 and CB2. Pharmacol Rev. 2010;62(4):588-631.
- Peres FF, Lima AC, Hallak JEC, et al. Cannabidiol as a promising strategy to treat and prevent movement disorders? Front Pharmacol. 2018;9:482.
- dos Santos RG, Hallak JEC, Crippa JAS. Neuropharmacological effects of the main phytocannabinoids: a narrative review. Adv Exp Med Biol. 2021;1264:29-45.
- Britch SC, Babalonis S, Walsh SL. Cannabidiol: pharmacology and therapeutic targets. Psychopharmacology (Berl). 2021;238(1):9-28.
- Crippa JA, Guimarães FS, Campos AC, Zuardi AW. Translational investigation of the therapeutic potential of cannabidiol (CBD): toward a new age. Front Immunol. 2018;9:2009.
- Zou S, Kumar U. Cannabinoid receptors and the endocannabinoid system: signaling and function in the central nervous system. Int J Mol Sci. 2018;19(3):813.
- Turcotte C, Blanchet MR, Laviolette M, Flamand N. The CB2 receptor and its role as a regulator of inflammation. Cell Mol Life Sci. 2016;73(23):4449-4470.
- Kilaru A, Chapma KD. The endocannabinoid system. Essays Biochem. 2020;64(3):485-499.
- Patton D V. A history of United States cannabis law. J Law Heal. 2020;34(1):1-29.
- McVey E. Exclusive: US retail marijuana sales on pace to rise 40% in 2020, near $37 billion by 2024. Marijuana Business Daily. https://mjbizdaily.com/exclusive-us-retail-marijuana-sales-on-pace-to-rise-40-in-2020-near-37-billion-by-2023/. Published June 30, 2020. Accessed February 15, 2021.
- GlobalData Healthcare. Biden baking plans for federal marijuana legalisation, boost for CMOs. Pharmaceutical Technology. https://www.pharmaceutical-technology.com/comment/biden-marijuana-legalisation-plans/. Published February 1, 2021. Accessed February 15, 2021.
- Brodwin E, Berke J. Wall Street thinks the $1 billion market for CBD could explode to $16 billion by 2025. Business Insider. https://www.businessinsider.com/cbd-marijuana-hemp-billions-health-industry-wall-street-analysts-2019-2. Published February 27, 2019. Accessed February 14, 2021.
- Hazekamp A. The trouble with CBD oil. Med Cannabis Cannabinoids. 2018;1(1):65-72.
- Bonn-Miller MO, Loflin MJE, Thomas BF, et al. Labeling accuracy of cannabidiol extracts sold online. JAMA. 2017;318(17):1708-1709.
- Warning letters and test results for cannabidiol-related products. FDA. https://www.fda.gov/news-events/public-health-focus/warning-letters-and-test-results-cannabidiol-related-products. Updated March 22, 2021. Accessed March 24, 2021.
- Chesney E, McGuire P, Freeman TP, et al. Lack of evidence for the effectiveness or safety of over-the-counter cannabidiol products. Ther Adv Psychopharmacol. 2020;10:2045125320954992.
- Dubrow GA, Pawar RS, Srigley C, et al. A survey of cannabinoids and toxic elements in hemp-derived products from the United States marketplace. J Food Compos Anal. 2021;97:103800.
- Liebling JP, Clarkson NJ, Gibbs BW, et al. An analysis of over-the-counter cannabidiol products in the United Kingdom. Cannabis Cannabinoid Res. https://doi.org/10.1089/can.2019.0078. Published April 1, 2020. Accessed April 5, 2021.
- Corroon J, MacKay D, Dolphin W. Labeling of cannabidiol products: a public health perspective. Cannabis Cannabinoid Res. 2020;5(4):274-278.
- FDA and cannabis: research and drug approval process. FDA. https://www.fda.gov/news-events/public-health-focus/fda-and-cannabis-research-and-drug-approval-process. Updated October 1, 2020. Accessed February 15, 2021.
- Razdan R. Structure-activity relationships in cannabinoids. Pharmacol Rev. 1986;38(2):75-149.
- Richtel M. What Is delta-8-THC?: the hemp derivative that’s a hot seller. New York Times. https://www.nytimes.com/2021/02/27/health/marijuana-hemp-delta-8-thc.html. Published February 27, 2021. Accessed March 11, 2021.
- von Wrede R, Helmstaedter C, Surges R. Cannabidiol in the treatment of epilepsy. Clin Drug Investig. 2021;44:211-220.
- Mead A. Legal and regulatory issues governing cannabis and cannabis-derived products in the United States. Front Plant Sci. 2019;10:697.
- Devinsky O, Cross JH, Laux L, et al. Trial of cannabidiol for drug-resistant seizures in the Dravet syndrome. N Engl J Med. 2017;376(21):2011-2020.
- Miller I, Scheffer IE, Gunning B, et al. Dose-ranging effect of adjunctive oral cannabidiol vs placebo on convulsive seizure frequency in Dravet syndrome: a randomized clinical trial. JAMA Neurology. 2020:77(5):613-621.
- Devinsky O, Patel AD, Cross JH, et al. Effect of cannabidiol on drop seizures in the Lennox-Gastaut syndrome. N Engl J Med. 2018;378(20):1888-1897.
- Thiele EA, Marsh ED, French JA, et al. Cannabidiol in patients with seizures associated with Lennox-Gastaut syndrome (GWPCARE4): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet. 2018;391(10125):1085-1096.
- Chen JW, Borgelt LM, Blackmer AB. Cannabidiol: a new hope for patients with Dravet or Lennox-Gastaut syndromes. Ann Pharmacother. 2019;53(6):603-611.
- Leehey MA, Liu Y, Hart F, et al. Safety and tolerability of cannabidiol in Parkinson disease: an open label, dose-escalation study. Cannabis Cannabinoid Res. 2020;5(4):326-336.
- Poklis JL, Mulder HA, Peace MR. The unexpected identification of the cannabimimetic, 5F-ADB, and dextromethorphan in commercially available cannabidiol e-liquids. Forensic Sci Int. 2019;294:e25-e27.
- Corroon J, Kight R. Regulatory status of cannabidiol in the United States: a perspective. Cannabis Cannabinoid Res. 2018;3(1):190-194.
- Vivian JC. Dispensing cannabis. US Pharmacist. https://www.uspharmacist.com/article/dispensing-cannabis. Published April 14, 2016. Accessed February 11, 2021.
- Marijuana pharmacies: the beginning of the licensure process. Louisiana Board of Pharmacy. http://www.pharmacy.la.gov/index.cfm?md=pagebuilder&tmp=home&pid=401. Accessed March 21, 2021.
- State of Arkansas. Arkansas Medical Marijuana Amendment of 2016. HB2190. https://www.arkleg.state.ar.us/Acts/Document?type=pdf&act=1024&ddBienniumSession=2017%2F2017R. Published March 6, 2017. Accessed March 24, 2021.
- Gubb SE,. Pharmacists role under Pennsylvannia’s medical marijuana law. https://cdn.ymaws.com/www.papharmacists.com/resource/resmgr/Legislative/Pharmacists%27_Role_Under_Penn.pdf. Accessed April 1, 2021.
- How to read a certificate of analysis (COA)? Kazmira LLC. https://www.kazmira-llc.com/blog/how-to-read-certificate-of-analysis-of-industrial-hemp-derived-products/. Accessed March 24, 2021.
- Bridgeman MB, Abazia DT. Medicinal cannabis: history, pharmacology, and implications for the acute care setting. P T. 2017;42(3):180-188.
- Parmar JR, Forrest BD, Freeman RA. Medical marijuana patient counseling points for health care professionals based on trends in the medical uses, efficacy, and adverse effects of cannabis-based pharmaceutical drugs. Res Social Adm Pharm. 2016;12(4):638-654.
- Kocis PT, Vrana KE. Delta-9-tetrahydrocannabinol and cannabidiol drug-drug interactions. Med Cannabis Cannabinoids. 2020;3(1):61-73.
- Nichols MA, Arnett SJ, Fa B, et al. National survey identifying community pharmacist preceptors’ experience, knowledge, attitudes, and behaviors influencing intent to recommend cannabidiol products. J Am Pharm Assoc (2003). 2021 Feb 6:S1544-3191(21)00018-2.
- Seamon MJ, Fass JA, Maniscalco-Feichtl M, Abu-Shraie NA. Medical marijuana and the developing role of the pharmacist. Am J Health Sys Pharm. 2007;64(10):1037-1044.
- Volkow ND, Baler RD, Compton WM, Weiss SRB. Adverse health effects of marijuana use. N Engl J Med. 2014;370(23):2219-2227.
- Medical cannabis. Canadian Pharmacists Association. https://www.pharmacists.ca/advocacy/medical-cannabis/. Published 2021. Accessed February 11, 2021.
- NSW cannabis medicines prescribing guidance. Australian Centre for Cannabinoid Clinical and Research Excellence. https://www.australiancannabinoidresearch.com.au/resources. Accessed March 24, 2021.
- Szyliowicz D, Hilsenrath P. Medical marijuana knowledge and attitudes: a survey of the California Pharmacists Association. J Prim Care Community Health. 2019;10:2150132719831871.
- Berlekamp D, Rao PSS, Patton T, Berner J. Surveys of pharmacy students and pharmacy educators regarding medical marijuana. Curr Pharm Teach Learn. 2019;11(7):669-677.
- Smithburger PL, Zemaitis MA, Meyer SM. Evaluation of medical marijuana topics in the PharmD curriculum: a national survey of schools and colleges of pharmacy. Curr Pharm Teach Learn. 2019;11(1):1-9.
- Abazia DT, Bridgeman MB. Reefer madness or real medicine? A plea for incorporating medicinal cannabis in pharmacy curricula. Curr Pharm Teach Learn. 2018;10(9):1165-1167.
- Structure of delta-9-tetrahydrocannabinol. Wikimedia Commons. https://commons.wikimedia.org/wiki/File:Delta-9-tetrahydrocannabinol.png. Published 2006. Accessed March 24, 2021.
- Structure of delta-8-tetrahydrocannabinol. Wikimedia Commons. https://commons.wikimedia.org/wiki/File:Delta-8-tetrahydrocannabinol.png. Published 2006. Accessed March 24, 2021.
- Structure of cannabidiol. Wikimedia Commons. https://commons.wikimedia.org/wiki/File:Cannabidiol.png. Published 2006. Accessed March 24, 2021.
Back to Top