
Expired activity
Please go to the PowerPak
homepage and select a course.
Pharmacotherapy Review 2021: Primary and Secondary Prevention of Cardiovascular Disease in the Ambulatory Setting
INTRODUCTION
Cardiovascular (CV) disease is the leading cause of disease burden worldwide and its prevalence is increasing, even within countries where it was previously declining.1 The prevalence of CV disease in the United States (defined as coronary heart disease, heart failure, or stroke) is 9.0%, and this increases to 48.0% when hypertension is included.2
Strategies for the primary and secondary prevention CV disease are multifaceted and are guided by evidence demonstrating efficacy in reducing atherosclerotic CV disease (ASCVD). Developed by the American Heart Association (AHA), Life’s Simple 7 (Figure 1) defines modifiable CV risk factors that people can improve through lifestyle changes to help achieve ideal CV health.3 These strategies should be the foundation of CV disease prevention and treatment.
| Figure 1. Life's Simple 7 — Risk Factors People Can Improve Through Lifestyle Changes to Help Achieve Ideal Cardiovascular Health3 |
 |
Implementing evidence-based treatments for treatment and prevention of CV disease in the ambulatory setting is an essential component of patient care, and those are the focus of this Pharmacotherapy Reviews 2021 installment. Pharmacists and other health professionals should be knowledgeable and empowered to identify, recommended, and implement pharmacotherapy approaches that reduce CV risk for patients with common chronic conditions, including hypertension, dyslipidemia, and type 2 diabetes. Evidence continues to evolve and expands, refines, and further informs our treatment approaches.
HYPERTENSION
The long-term health CV consequences of uncontrolled hypertension (e.g., coronary artery disease, stroke, kidney disease) are well described. Measuring blood pressure (BP) for the purpose of identifying new-onset hypertension or to assess BP control in patients with hypertension is a standard of care at nearly every patient care encounter. Despite this practice, hypertension-associated mortality has been rising in the United States,4 while BP control rates have been declining.5 The U.S. Surgeon General released a Call to Action to Control Hypertension in 2020 to heighten awareness of this situation.6 The asymptomatic nature of hypertension, coupled with the staggering health risk justifies its nickname, “the silent killer.”
The American College of Cardiology (ACC) and the AHA, most recently released their hypertension guideline in 2017.7 This guideline replaced the previous Joint National Committee (JNC) reports, which had not been systematically updated as a government-sanctioned guideline since the JNC7 report in 2003.
Blood Pressure Values
The blood pressure categorization in the 2017 ACC/AHA guideline uses a threshold of ≥130/80 mm Hg to define hypertension (Table 1).7 However, the clinical diagnosis of hypertension can be made only when the average of 2 or more correctly measured BP values meet or exceed this threshold during 1 clinical encounter, with confirmation during a second clinical encounter, and after secondary causes are ruled out. Importantly, confirming hypertension using out-of-office BP measurements (e.g., home BP measurements) is also recommended.7 Data suggest that 1 week of home BP measurements may be better than office-based or 24-hour ambulatory BP measurements for diagnosing hypertension.8
| Table 1. ACC/AHA Categorization of Blood Pressure7 |
| Classificationa |
Systolic BP (mm Hg) |
|
Diastolic BP (mm Hg) |
| Normal |
<120 |
and |
<80 |
| Elevated |
120–129 |
or |
<80 |
| Stage 1 hypertension |
130–139 |
or |
80–89 |
| Stage 2 hypertension |
≥140 |
or |
≥90 |
Abbreviations used: ACC/AHA, American College of Cardiology/American Heart Association; BP, blood pressure
aIf systolic and diastolic BP values yield different classifications, the highest category is used for determining a classification. |
A BP goal of <130/80 mm Hg is appropriate for all patients, especially those age 65 years or older.7 For certain older adults who are not living independently, are frail, have a high burden of comorbidities, and/or have limited life expectancy, a higher BP goal value may be selected based on a patient-centered and team-based approach to decision making. Prior to the 2017 ACC/AHA recommendations, higher BP goals (e.g., <140/90 mm Hg) were identified, leaving some clinicians uncertain of whether to use <130/80 mm Hg as the goal. As discussed below, evidence suggests that achieving systolic BP values of 120–129 mm Hg in most patients with hypertension reduces risk of ASCVD better than treating patients to higher target thresholds.
The largest randomized controlled trial that evaluated lower versus higher BP goals was the Systolic Blood Pressure Intervention Trial (SPRINT).9 In SPRINT, 9,351 patients with hypertension and additional CV risk factors were randomized to intense (systolic BP goal <120 mm Hg) or standard (systolic BP goal <140 mm Hg) treatment. The trial was stopped early after a median of 3.3 years because patients randomized to intense treatment had a 25% relative reduction in risk of CV events (myocardial infarction, stroke, heart failure, or CV death). The mean systolic BP in the intense arm was 121.4 mm Hg, supporting a systolic BP goal of <130 mm Hg. A subsequent SPRINT analysis estimated that patients randomized to intense treatment had improved long-term survival by up to 3 years.10 Other meta-analyses included additional long-term prospective clinical trials have supported the recommended <130/80 mm Hg BP goal in most patients.11,12
Treatment Recommendations
Initial treatment recommendations for hypertension are described in Figure 2.7 Lifestyle modifications are recommended for all patients, especially those with elevated BP or hypertension.7 Lifestyle modifications proven to lower BP include weight loss (if overweight or obese), a healthy diet (e.g., the Dietary Approaches to Stopping Hypertension eating plan), sodium reduction, dietary potassium supplementation, physical activity, and alcohol restriction. For patients with stage 1 or stage 2 hypertension, antihypertensive pharmacotherapy (Table 2) is recommended in addition to lifestyle modifications. Two exceptions are patients with a history of stroke or primary-prevention patients without diabetes or chronic kidney disease who have a 10-year ASCVD risk of <10%; for these patients, lifestyle modifications can be used without antihypertensive drug therapy if hypertension remains in stage 1.
| Table 2. Common Antihypertensive Medications7 |
| Drug Class (common agents) |
Mechanisms of Action |
Comments/Considerations |
ACEi
(benazepril, lisinopril, ramipril) |
Inhibits angiotensin converting enzyme and decreases production of angiotensin II, which decreases aldosterone and sodium retention, and thereby decreases vasoconstriction |
- May cause a dry cough
- Never use in combination with an ARB
- Can cause hyperkalemia and may raise serum creatinine (usually minimal)
- Do not use in bilateral renal artery stenosis, history of angioedema, or pregnancy
|
ARB
(irbesartan, losartan, olmesartan, valsartan) |
Blocks the angiotensin II receptor, which decreases aldosterone and sodium retention, and thereby decreases vasoconstriction |
- Never use in combination with an ACEi
- Can cause hyperkalemia and may raise serum creatinine (usually minimal)
- Do not use in bilateral renal artery stenosis or pregnancy
|
Dihydropyridine CCB
(amlodipine, felodipine) |
Blocks calcium receptors, which causes arterial vasodilation |
- May cause peripheral edema (dose related)
- The preferred type of CCB in hypertension
|
| Nondihydropyridine CCB (diltiazem, verapamil) |
Blocks calcium receptors, which results in arterial vasodilation; blocks the atrioventricular node and decreases cardiac output |
- May cause bradycardia and/or constipation
- Avoid routine use with a beta-blocker because of increased risk of bradycardia/heart block
- Do not use in patients with heart failure with reduced ejection fraction
- May result in drug-drug interactions due to moderate inhibition of CYP3A4
|
Thiazides
(chlorthalidone, hydrochlorothiazide) |
Initially produces a diuretic effect, but long-term decreases peripheral vascular resistance |
- Chlorthalidone may be more potent than hydrochlorothiazide and is preferred in resistant hypertension
- Can cause hyponatremia and hyperuricemia
|
MRA
(eplerenone, spironolactone) |
Directly inhibits aldosterone, which decreases sodium retention, and thereby decreases vasoconstriction |
- May cause hyperkalemia (some cases can be severe), spironolactone may cause gynecomastia
- Very effective in resistant hypertension
|
Beta-blockers
(bisoprolol, carvedilol, metoprolol succinate) |
Blocks beta-1 (some block beta-2) receptors, resulting in sinus and atrioventricular node blocking, decreased renin release from the kidney, which results in vasodilation and decreased cardiac output |
- May cause bradycardia and exercise intolerance
- Nonselective agents can exacerbate asthma
- Abrupt discontinuation can cause rebound hypertension
|
| Abbreviations used: ACEi, angiotensin converting enzyme inhibitor; ARB, angiotensin receptor blocker; CCB, calcium channel blocker; CYP, cytochrome P-450; MRA, mineralocorticoid receptor antagonist |
| Figure 2. Initial Treatment of Hypertension7 |
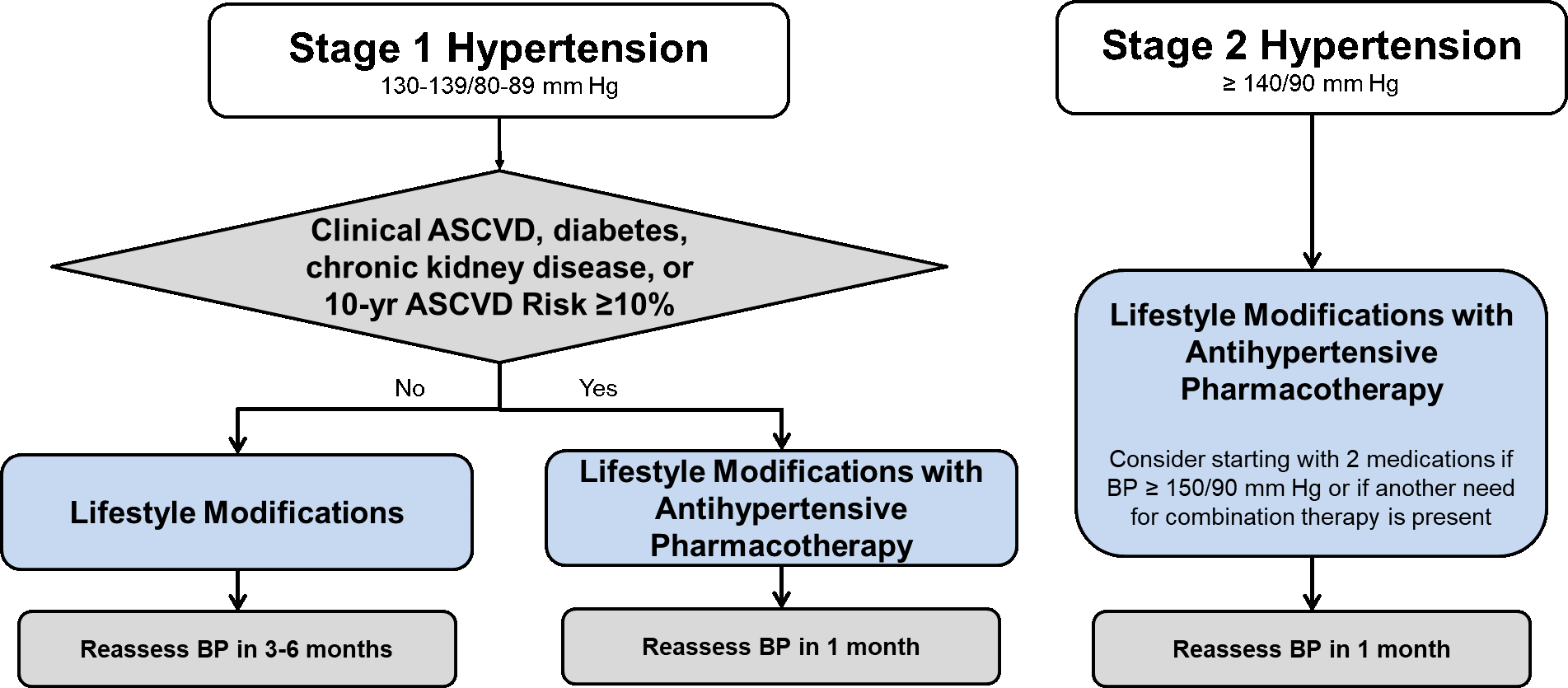 |
| Abbreviations used: ASCVD, atherosclerotic cardiovascular disease; BP, blood pressure |
Risk of ASCVD can be estimated in primary-prevention patients using the Pooled Cohort Equations. These are exclusively for determining baseline risk in primary-prevention patients with LDL-C values <190 mg/dL who are not on lipid-lowering therapy. The 10-year risk of ASCVD can be estimated for patients age 40–79 years, and lifetime risk of ASCVD is estimated for patients age 20–59 years. The following patient characteristics are needed for calculation: age, sex, race, systolic BP, total cholesterol, HDL cholesterol, smoking status, history of diabetes, and whether treated with antihypertensive medication. These estimates should be used by clinicians to inform clinician–patient risk discussions and to guide treatment choices. Other calculators have been developed using the Pooled Cohort Equations that accommodate patients who are already treated with LDL-C lowering therapy and provide specific treatment recommendations.
Selecting antihypertensive medications should be based on evidence from CV outcome trials. With hypertension, many antihypertensive agents have been shown to reduce CV events and guide recommendations (Table 3). Landmark clinical trials have evaluated patients with and without comorbidities (compelling indications) that are associated with increased CV risk and require a specific approach to medication selection.
| Table 3. 2017 ACC/AHA Recommended Antihypertensive Pharmacotherapy Based on Compelling Indications7 |
| Compelling Indication |
Evidence-Based Pharmacotherapya |
| None |
ACEi or ARB, CCB, or thiazide |
| Heart failure with reduced ejection fraction |
ACEi or ARB with an evidence-based beta-blockerb; diuretic if edema, MRA if needed as additional therapy |
| Heart failure with preserved ejection fraction |
ACEi or ARB with an evidence-based beta-blockerc |
| Stable ischemic heart disease |
Evidence-based beta-blocker with an ACEi or ARB; CCB, thiazide, and/or MRA if needed as additional therapy |
| Diabetes mellitus |
ACEi or ARB, CCB, or thiazide |
| Chronic kidney disease |
ACEi or ARB |
| Secondary stroke prevention |
Thiazide or thiazide with ACEi |
Abbreviations used: ACEi, angiotensin converting enzyme inhibitor; ARB, angiotensin receptor blocker; CCB, calcium channel blocker; MRA, mineralocorticoid receptor antagonist
aShould always be used in combination with lifestyle modifications
bBisoprolol, carvedilol, or metoprolol succinate
cBisoprolol, carvedilol, metoprolol succinate or tartrate, nadolol, propranolol, or timolol |
For patients without a compelling indication, an angiotensin converting enzyme inhibitor (ACEi), angiotensin receptor blocker (ARB), calcium channel blocker (CCB), or thiazide are proven and recommended first-line agents, without any single agent clearly being preferred ahead of another. However, a CCB or thiazide may be preferred for Black patients treated with monotherapy because of a greater magnitude of BP lowering in this group compared with an ACEi or ARB. However, this difference dissipates once combination antihypertensive therapy is used. Most patients with hypertension require more than 1 antihypertensive agent, and these first-line agents can be used in combination, with the exception that an ACEi and ARB should not be used together because of unjustified risk of adverse effects.7
The evidence base evaluating antihypertensive pharmacotherapy in patients with compelling indications is extensive. For these comorbidities, selection of an antihypertensive regimen is well delineated (Table 3). Beta-blockers are not first-line agents for patients without a compelling indication because they do not reduce CV events as much as an ACEi, ARB, CCB, or thiazide. However, a beta-blocker is a proven treatment as a component of a first-line antihypertensive regimen for patients with a compelling indication of stable ischemic heart disease (e.g., prior myocardial infarction, acute coronary syndrome, stable ischemic heart disease).
Noteworthy Within-Antihypertensive-Class Differences
Dihydropyrine CCBs (e.g., amlodipine) are superior to nondihydropyridines (diltiazem and verapamil) as monotherapy.13 This aligns with prescribing patterns, as most clinicians will choose a dihydropyridine CCB for hypertension ahead of a nondihydropyridine because they are better tolerated. The most common side effect of a dihydropyridine CCB is peripheral edema. This adverse effect results from arterial vasodilation that occurs with CCB therapy that is not balanced by venous vasodilation, leading to a pressure imbalance between arteries and veins. While not harmful, this imbalance can cause fluid leaking through capillaries and peripheral edema. Unfortunately, patients who start a dihydropyridine CCB have a higher risk of subsequently starting a loop diuretic.14 This is most likely to “treat” peripheral edema. This practice is futile because peripheral edema caused by a CCB is not responsive to diuretic therapy; this should be treated with CCB dose reduction or stopping the CCB.
Hydrochlorothiazide is the most frequently prescribed thiazide. However, chlorthalidone is a more potent antihypertensive on a milligram-per-milligram basis and has a longer half-life. For patients with resistant hypertension who are treated with hydrochlorothiazide, guidelines recommend switching to chlorthalidone as a strategy to further reduce BP.7,15 However, this recommendation is controversial. A large observational cohort study evaluated 750,225 patients who were prescribed hydrochlorothiazide or chlorthalidone.16 There were no differences in CV events, but those on chlorthalidone had a higher risk of electrolyte abnormalities, renal adverse effects, and new-onset diabetes. These findings should be confirmed with other analysis but question the preferred use of chlorthalidone for hypertension.
Bedtime Dosing
The typical diurnal BP pattern in humans is a steady rise starting a few hours before awakening, followed by a peak several hours after awakening, with gradual decline throughout the day that continues for several hours after bedtime. This cycle repeats daily in most patients. Because the highest incidence of CV events has been observed to occur near the peak in BP, researchers developed the concept of “chronotherapeutic” antihypertensive dosing of medications to blunt the rise in BP and flatten the peak in CV events. One chronotherapeutic verapamil product was designed to be taken at bedtime, with a delayed onset and gradual release of medication beginning around the time of BP starts rise after bedtime. The double-blind prospective Controlled Onset Verapamil Investigation of Cardiovascular End Points (CONVINCE) trial evaluated this therapy versus the morning dosing of antihypertensive medications in 16,602 patients with hypertension and additional CV risk factors. No difference in CV events was found between the two groups, indicating lack of benefit of chronotherapy for hypertension.17
Some clinical trials have shown benefits of administering immediate-release medications at bedtime. The first was the Heart Outcomes Prevention Evaluation (HOPE) study, a double-blind, controlled trial that randomized 9,297 patients with high CV risk to ramipril or placebo at bedtime.18 Bedtime dosing of ramipril reduced the primary CV event endpoint by 22%; however, less than half of these patients had hypertension. One prospective, open-label study randomized 448 Spanish patients with diabetes to morning dosing of all antihypertensive medications or dosing of at least 1 antihypertensive medication at bedtime. This small study showed a 67% reduction in CV events with in the bedtime dosing group, but these results require confirmation using a larger study design.19
The very large Hygia Chronotherapy Trial evaluated CV outcomes with bedtime dosing of at least 1 antihypertensive agent versus morning dosing of all antihypertensive medications. This trial enrolled 19,084 Spanish patients with hypertension using an open-label design. Inclusion required 48-hour ambulatory BP measurements with ongoing 48-hour measurement used to assess efficacy. After a median follow-up of 6.3 years, the primary CV event endpoint was reduced 45% in the bedtime-dosing group.20
The results of the Hygia Chronotherapy Trial indicated that administering at least 1 antihypertensive medication at bedtime resulted in significant benefits. Suspiciously, many details were absent in publication of these results and study methods have been questioned. The authors did not provide guidance or descriptions of how many or which type antihypertensive medications were administered at bedtime. Patients and clinicians chose which and how many medications to administer at bedtime but were encouraged to administer CCB, ACEi, or ARB medications at bedtime and thiazides in the morning. Perhaps these results were too good to be true, as the European Heart Journal has published a letter of concern informing readers that the trial results are under investigation and that findings should be interpreted with caution.21 Clinicians should not routinely advise patients to administer at least 1 of their antihypertensive medications at bedtime unless this investigation refutes concerns.
DYSLIPIDEMIA
Dyslipidemia, similar to hypertension, can result in CV events and is typically asymptomatic. Elevated cholesterol, in particular low-density lipoprotein cholesterol (LDL-C), is the primary lipoprotein that leads to ASCVD. Although the optimal LDL-C value for a patient depends on their overall risk for ASCVD, almost 30% of adults in the United States have an LDL-C value ≥130 mg/dL.2
Treatment Recommendations
The AHA/ACC collaborated with 10 other professional societies to create the 2018 AHA/ACC/Multisociety cholesterol guideline.22 These recommendations built upon recommendations from the 2013 ACC/AHA guideline and evidence — statin-based LDL-C lowering is the standard of care for patients with hypercholesterolemia.23 The 2013 ACC/AHA cholesterol guideline defined 4 statin benefit groups of patients for whom LDL-C lowering with statin therapy was recommended based on landmark clinical trial evidence demonstrating CV event lowering. The 2018 AHA/ACC/Multisociety guidelines reaffirm therapy in these 4 groups and expand recommendations based on newer evidence with non-statins. These 4 groups are subcategorized as secondary prevention (patients with established ASCVD) or primary prevention (no history of ASCVD).
Secondary Prevention
Clinical ASCVD includes coronary artery disease (e.g., acute coronary syndrome, stable ischemic heart disease), cerebrovascular disease (ischemic stroke, transient ischemic attack), peripheral arterial disease, and other forms of clinical atherosclerosis (e.g., abdominal aortic aneurysm). Patients with these conditions are secondary prevention patients. Recommended treatment for secondary prevention is detailed in Figure 3.
| Figure 3. Treatment of Hypercholesterolemia in Patients With ASCVD (Secondary Prevention)22 |
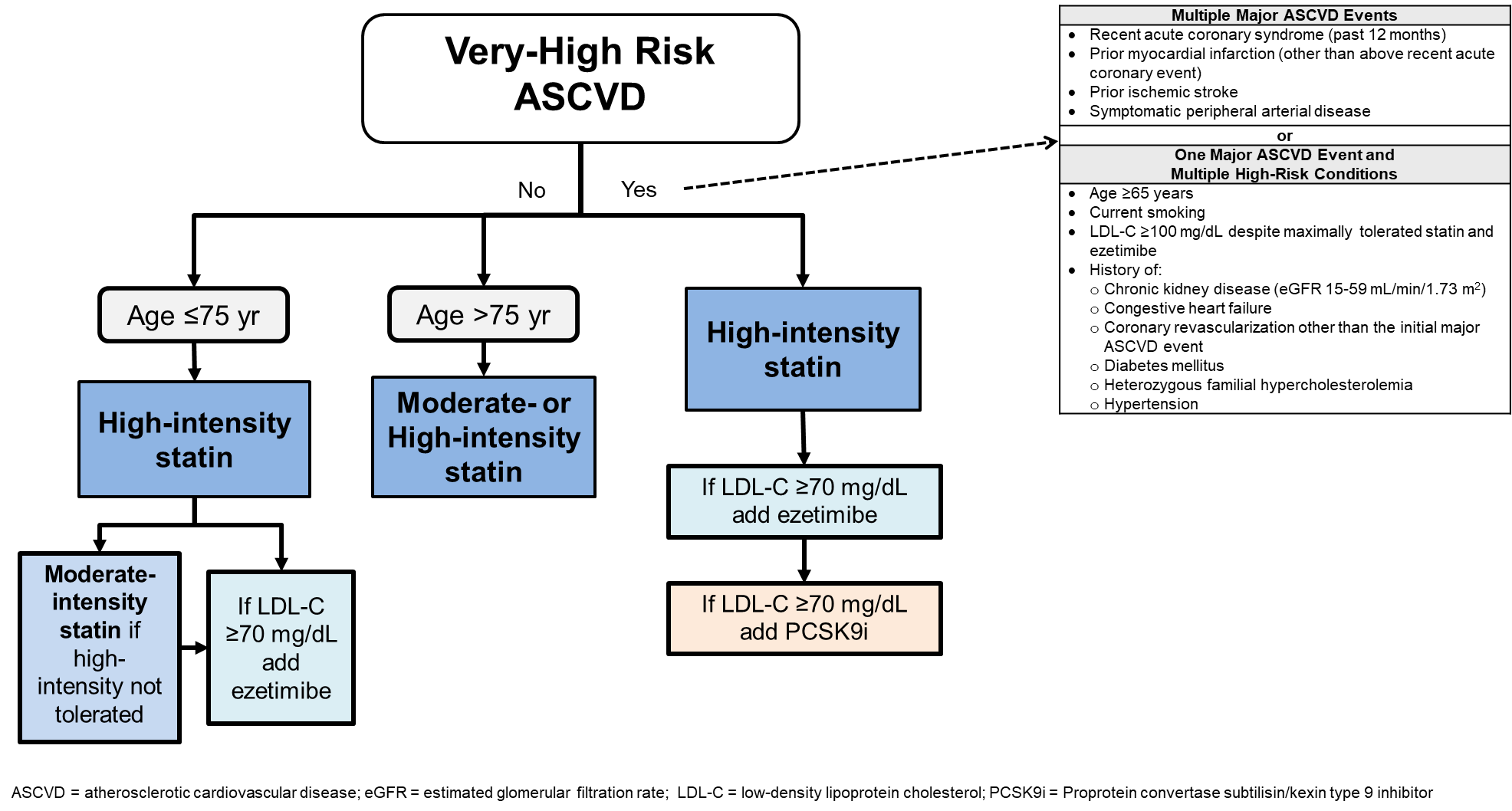 |
Statin therapy is recommended for all secondary prevention patients unless contraindicated. Secondary prevention patients who are adherent with their statin regimen have lower mortality than patients with lower adherence, highlighting the importance of therapy.24 High-intensity statin therapy (Table 4) is the preferred starting treatment option, but a moderate-intensity statin may be acceptable in older patients (>75 years of age) or if high-intensity statin therapy cannot be tolerated. Importantly, the 2018 AHA/ACC/Multisociety guidelines differentiates among secondary prevention patients who are very-high risk ASCVD. This includes patients with multiple forms of clinical ASCVD, or one form of clinical ASCVD with multiple high-risk conditions. Most secondary prevention patients are categorized as very-high risk because high-risk conditions typically precede clinical ASCVD events.
| Table 4. Statin Intensity for Available Statin Medications68 |
| |
High Intensity
(≥50% LDL-C lowering) |
Moderate Intensity
(30–49% LDL-C lowering) |
Low Intensity
(<30% LDL-C lowering) |
| Primary statins |
Atorvastatin 40–80 mg
Rosuvastatin 20–40 mg |
Atorvastatin 10–20 mg
Rosuvastatin 5–10 mg
Simvastatin 20–40 mg |
Simvastatin 10 mg |
| Other statins |
|
Pravastatin 40–80 mg
Lovastatin 40–80 mg)
Fluvastatin XL 80 mg
Fluvastatin 40 mg twice daily
Pitavastatin 1–4 mg |
Pravastatin 10–20 mg
Lovastatin 20 mg
Fluvastatin 20–40 mg |
| Abbreviation used: LDL-C, low-density lipoprotein cholesterol |
The overall approach in secondary prevention is starting high-intensity statin therapy and reassessing LDL-C in 4 to 12 weeks. If LDL-C is at or above the threshold of 70 mg/dL, intensifying statin therapy is recommended. For patients who remain at or above the LDL-C threshold of 70 mg/dL, or those who do not tolerate higher statin doses, adding ezetimibe (Table 5) is recommended. Ezetimibe has been shown in the Improved Reduction of Outcomes: Vytorin Efficacy International Trial (IMPROVE-IT) to provide modest additional LDL-C lowering and a modest further reduction in CV event risk when added to statin therapy.25
| Table 5. Description of LDL-C Lowering Medications22,69 |
| Drug Classes (agents) |
Mechanisms of Action |
% LDL-C Lowering |
Evidence Showing CV Event Reduction |
Safety Considerations |
| Statin (atorvastatin, fluvastatin, lovastatin, pitavastatin, pravastatin, rosuvastatin, simvastatin) |
Competitively inhibits HMG-CoA reductase which inhibits cholesterol synthesis, resulting in increased LDLR expression and increased cholesterol removal |
18–55 |
Numerous trials in primary and secondary prevention |
- Muscle-related side effects
- Drug-drug interactions (agent specific)
|
| Cholesterol absorption inhibitor (ezetimibe) |
Blocks the Niemann-Pick C1-Like 1 receptor and inhibits cholesterol absorption, leading to decreased delivery of cholesterol to the liver and increased cholesterol removal |
13–20 |
One trial in secondary prevention (with a statin) |
- Small increased risk of elevated hepatic transaminases when used with a statin
|
| Bile acid sequestrant (colesevelam, colestipol, cholestyramine) |
Binds intestinal bile acids, impedes reabsorption, and upregulates cholesterol 7-α-hydroxylase, resulting in increased conversion of cholesterol to bile acids, increased cholesterol demand in the liver, increased LDLRs and increased cholesterol removal |
15–30 |
One clinical trial in primary prevention men |
- Can raise serum triglyceride values
- Gastrointestinal side effects are common
|
Citrate lyase inhibitor
(bempedoic acid) |
Inhibits adenosine triphosphate-citrate lyase and decreases of cholesterol synthesis in the liver |
15–24 |
One ongoing trial in patients unable to tolerate a statin |
- Can cause hyperuricemia
- Increased risk of tendon rupture
- Maximum dose of simvastatin 20 mg and pravastatin 40 mg when used concurrently
|
PCSK9 Inhibitor
(alirocumab, evolocumab) |
Binds PCSK9, which normally promotes LDLR degradation, resulting in increased LDLRs and increased cholesterol removal |
43–64 |
Two trials in very high-risk secondary prevention (with a statin) |
|
| Abbreviations used: CV, cardiovascular; HMG-CoA, 3-hydroxy-3-methylglutaryl-coenzyme A; LDL-C, low density lipoprotein cholesterol; LDLR, LDL receptor; PCSK9, proprotein convertase subtilisin kexin type 9 |
The Further Cardiovascular Outcomes Research with PCSK9 Inhibition in Subjects with Elevated Risk (FOURIER)26 and ODYSSEY-Outcomes27 trials have demonstrated that adding a proprotein convertase subtilisin kexin type 9 inhibitor (PCSK9i) to a statin, with or without ezetimibe, provides large reductions in LDL-C and CV event risk in very-high risk secondary prevention patients. The magnitude of benefit appears much greater with the addition of a PCSK9i compared with ezetimibe. However, the 2018 AHA/ACC/Multisociety guidelines recommend adding ezetimibe before a PCSK9i based on cost and because many very-high risk ASCVD patients will achieve an LDL-C <70 mg/dL with ezetimibe.22,28 This is consistent with 2021 American Diabetes Association recommendations.29
Primary Prevention
Three of the four statin benefit groups are primary prevention. Similar to secondary prevention, statin therapy to lower LDL-C is the primary pharmacologic strategy (Figure 4).22
| Figure 4. Treatment of Hypercholesterolemia in Primary Prevention22 |
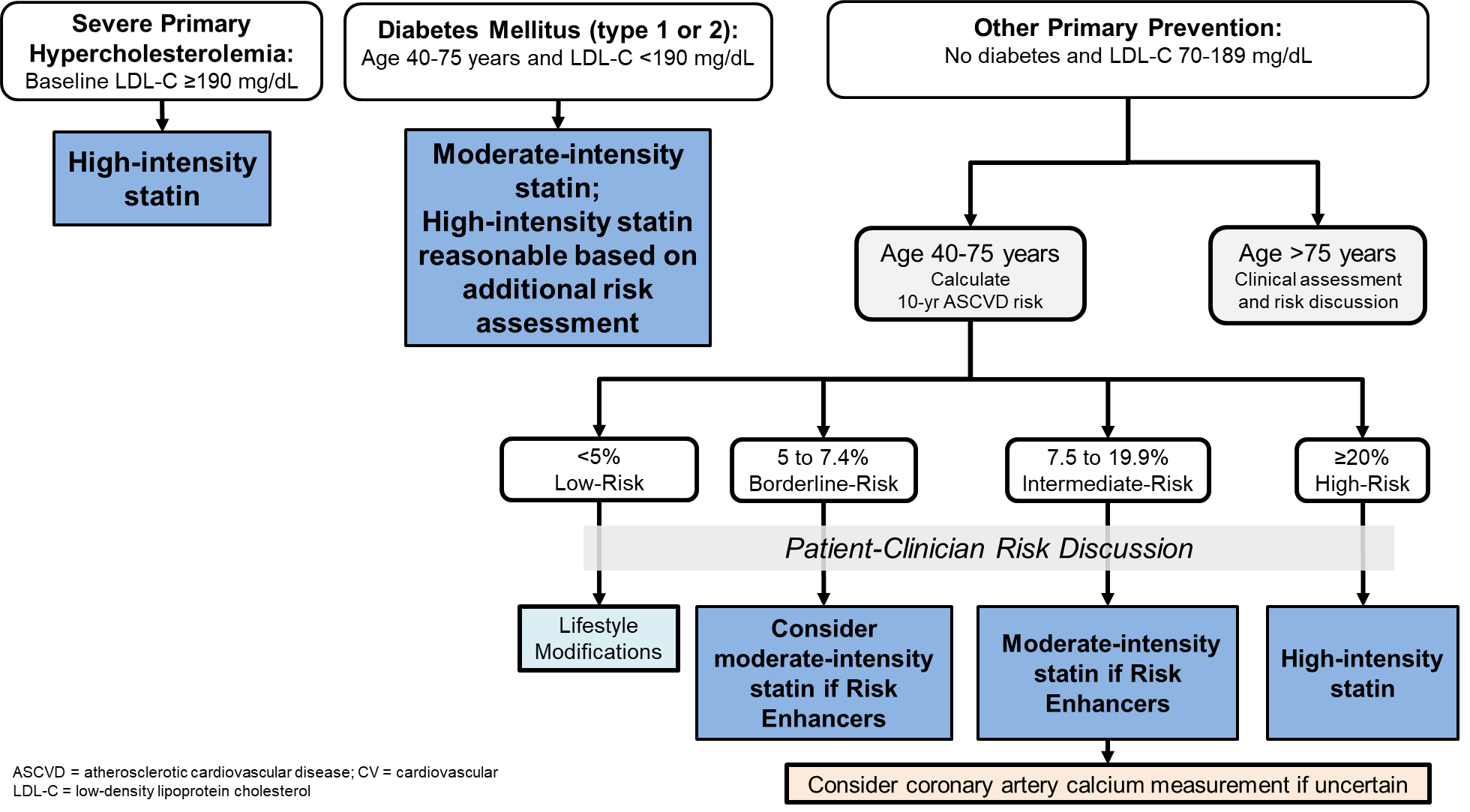 |
Patients with severe primary hypercholesterolemia have a baseline LDL-C ≥190 mg/dL. Many of these patients have genetic hypercholesterolemia (e.g., heterozygous [FH]) and all have an increased ASCVD risk throughout their lifetime. High-intensity statin therapy is strongly recommended, followed by reassessment of LDL-C in 4 to 12 weeks. If LDL-C is at or above the threshold of 100 mg/dL, intensifying statin therapy is recommended. For patients still at or above the LDL-C threshold of 100 mg/dL, or if higher doses are not tolerated, adding ezetimibe, a bile acid sequestrant, and/or a PCSK9i is recommended.
Statin therapy is recommended in patients with type 1 or type 2 diabetes, age 40–75 years, with an LDL-C <190 mg/dL.22 Some clinicians misinterpret this group to only include patients with type 2 diabetes, but evidence demonstrates CV event lowering in primary prevention patients with type 1 or type 2 diabetes.30,31 The strongest and extensive evidence-based recommendation is for moderate-intensity statin therapy in this group.29
When additional CV risk warrants more aggressive LDL-C lowering, high-dose statin therapy can be instituted if this is supported in a patient–clinician discussion. While there is no universal definition of additional CV risk, ASCVD risk factors, increased age, 10-year risk of ASCVD, and diabetes-specific risk enhancing factors should be considered.22
LDL-C lowering with statin therapy is recommended in patients younger than 40 years of age or older than 75 years of age. However, evidence supporting treating those in these age groups are not extensive; most primary prevention patients with diabetes in clinical trials were 40–75 years of age. Statin therapy should be considered in these younger and older patients based on a patient–clinician discussion that is informed by CV risk, life expectancy, and other patient-specific factors.
Other primary prevention patients between the age of 40–75 years, without diabetes and with an LDL-C of 70–189 mg/dL require individual risk assessment to ascertain need for statin therapy. The Pooled Cohort Equations are recommended to estimate 10-year risk of ASCVD. If <5%, patients are low risk, have not been studied in long-term CV outcome trials, and should follow healthy lifestyle modifications alone. If ≥20%, patients are high-risk, and high-intensity statin therapy is recommended.
Patients with 10-year ASCVD risk of 7.5% to 19.9% are intermediate-risk. Moderate-intensity statin therapy should be implemented if a patient–clinician risk discussion favors treatment. This discussion should be informed by the presence of risk-enhancing factors (see below).22 Borderline-risk patients have a 10-year ASCVD risk score of 5% to 7.4% and are treated like intermediate-risk. However, the strength of recommendation for statin therapy is low because of a paucity of studies of borderline-risk patients.
Risk-Enhancing Factors
Risk-enhancing factors are characteristics that are associated with an increased risk of ASCVD but are not included in the Pooled Cohort Equations calculation (Table 6).22
| Table 6. 2018 AHA/ACC/Multisociety Defined-Risk-Enhancing Factors in Borderline- and Intermediate-Risk Primary Prevention Patients68 |
Patient Characteristics |
- Family history of premature ASCVDa
- LDL-C, 160–189 mg/dL (or non–HDL-C 190–219 mg/dL)
- Metabolic syndrome
- High-risk race/ethnicities (e.g., South Asian ancestry)
|
| Medical History |
- Chronic kidney disease (eGFR 15–59 mL/min/1.73 m2 with or without albuminuria, and not dialysis or kidney transplantation)
- Chronic inflammatory conditions (e.g., rheumatoid arthritis, HIV)
- Premature menopause (<40 years), pregnancy-associated conditions that increase later ASCVD risk (e.g., preeclampsia)
|
| Lipid/Biomarkers |
- Persistently elevated, primary hypertriglyceridemia (≥175 mg/dL)
- Abnormal biomarkers if measured:
- High-sensitivity C-reactive protein ≥2.0 mg/L
- Lipoprotein(a) ≥50 mg/dL
- Apolipoprotien B ≥130 mg/dL
- Ankle brachial index <0.9
|
Abbreviations used: LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; ASCVD, atherosclerotic cardiovascular disease; eGFR, estimated glomerular filtration rate; HIV, human immunodeficiency virus
amale primary relative, age <55 years; female primary relative, age <65 years |
When the decision to treat an intermediate-risk primary prevention patient (10-year ASCVD risk of 7.5% to 19.9%) is unclear, coronary artery calcium (CAC) measurement should be considered.22 CAC should not be considered in patients on statin therapy or in other statin benefit groups. CAC scoring can strongly inform ASCVD risk prediction, regardless of race, gender, or ethnicity. The presence of coronary arterial calcification is a germane component of clinical ASCVD and can be detected by CAC measurement. There is a direct proportional relationship between CAC scores and CV events.32 Therefore, CAC measurement can identify patients with emerging ASCVD and further informs the decision to implement statin treatment.
CAC is measured with an outpatient test that uses computed tomography to detect calcium deposits in coronary arteries. For intermediate-risk patients who are age 55 years or older and not on statin therapy, it is reasonable to start statin therapy if CAC score above 0. For all other ages, statin therapy is reasonable if CAC score is ≥100, or if the score is in the 75th percentile or higher.
LDL-C Goal Values
LDL-C is the primary target of therapy in hypercholesterolemia.22 However, there is debate regarding the most appropriate goals. The 2018 AHA/ACC/Multisociety cholesterol guideline does not identify LDL-C goals. Rather, achieving a 30% to 49% LDL-C reduction from baseline with moderate-intensity statin therapy and a ≥50% LDL-C reduction from baseline with high-intensity statin therapy are recommended. LDL-C thresholds of 70 mg/dL and 100 mg/dL are identified for patients with clinical ASCVD and severe primary hypercholesterolemia, respectively. However, a threshold is a value that if not achieved should direct clinicians to further intensify LDL-C lowering.
Other organizations recommend the use of specific LDL-C goals.33,34 The European Society of Cardiology/European Atherosclerosis Society (ESC/EAS) guidelines were published in 2019. They recommend specific LDL-C goals, with goals as low as <40 mg/dL in some very-high risk ASCVD patients. Despite these differences, there are several similarities between the 2018 AHA/ACC/Multisociety and 2019 ESC/EAS guidelines.35 Most patients will be treated the same way regardless of which is used, with a trend that ESC/EAS recommendations may lead to more aggressive LDL-C lowering therapy.
New Medications
Bempedoic acid is a novel LDL-C lowering agent that acts through citrate lyase inhibition (Table 5). It exclusively works in the liver to inhibit cholesterol production. Bempedoic acid 180 mg orally daily was approved in 2020 in combination with lifestyle modifications and maximally tolerated statin therapy in patients with heterozygous FH or ASCVD for additional LDL-C lowering. It is available alone and in a fixed-dose combination product with ezetimibe. When added to statin or ezetimibe therapy, bempedoic acid provides an additional LDL-C lowering in the 20% or greater range.36-38
An ongoing CV outcome clinical trial is evaluating bempedoic acid in patients unable to tolerate statin therapy. A 2020 consensus statement from the American Association of Clinical Endocrinologists and American College of Endocrinology has included bempedoic acid as a nonstatin medication that can be helpful to achieve treatment goals when further reduction in LDL-C is needed.39 However, until CV event lowering is demonstrated, the role of bempedoic acid in therapy will be limited, but the drug may be an option for some patients needing further LDL-C lowering in combination or in place of with other standard therapies.
Inclisiran is a small-interfering RNA therapy that selectively blocks PCSK9 protein production. When added to a statin, it provides an additional LDL-C lowering of 50% to 52% in patients with ASCVD and 40% in those with heterozygous FH.40,41 Inclisiran is a subcutaneous injection administered by a health professional (not self-administered) as a single initial dose, followed by a second dose at 3 months and additional doses every 6 months thereafter. Inclisiran is likely to be approved in 2021. The unique administration of inclisiran creates an opportunity for treatment to be administered in a pharmacy similar to vaccines.42 A large ongoing CV outcomes trial in patients with ASCVD is ongoing.
Evinacumab is a novel fully human monoclonal antibody against angiopoietin-like 3. This medication lowers LDL-C cholesterol up to 47% when added to statin-based therapy in patients with either homozygous or heterozygous FH.43,44 Administered as an intravenous infusion, the product is not expected to be approved until after 2021.
Treatment of Moderately Elevated Triglycerides and CV Benefits
The 2018 AHA/ACC/Multisociety guidelines reserve the use of triglyceride-lowering medications (fibrates, omega-3 fatty acids) for triglycerides values ≥500 mg/dL.22 Under this circumstance, treatment is to decrease risk of pancreatitis. However, patients with lesser triglyceride elevations (150–499 mg/dL) appear to have residual risk for ASCVD. In these patients, the benefits of further triglyceride lowering, in addition to statin-based LDL-C lowering, has been suggested as beneficial. It is important to note that the addition of niacin or a fibrate to a statin is not recommended because CV outcome trials have demonstrated no additional benefits, and risk of adverse effects is increased with these combination regimens.22,29
There are 2 FDA-approved omega-3 fatty acid medications. One product is icosapent ethyl, it and contains only EPA. The other product is omega-3 acid ethyl esters; it contains both EPA and DHA. Icosapent ethyl contains only ethyl esters of omega-3 fatty acid, eicosapentanoic acid (EPA). Both are dosed at 2 grams twice daily or 4 grams daily, with a primary indication to lower very high triglycerides ≥500 mg/dL. Both should be administered with a fat-containing meal to assure maximum absorption.
Omega-3 fatty acid medications have been evaluated in large CV outcome trials. One landmark meta-analysis of 10 clinical trials with 77,917 patients demonstrated no significant reductions in CV events.45 However, when 2 recent large trials (ASCEND and VITAL) were added, small benefits in some CV endpoints were seen.46,47 Most of these trials used mixtures of omega-3 fatty acids that contained EPA and docosahexanoic acid (DHA). However, the JELIS trial used EPA only and had the most significant CV benefits.48 DHA can also increase LDL-C, whereas EPA does not. These findings suggested that CV event lowering may be optimal with EPA only, not with both EPA and DHA, as contained in most omega-3 fatty acid products. However, the most recent CV outcome studies, the REDUCE-IT and STRENGTH trials, were not included in this meta-analysis.
CV Outcome Trials With Omega-3 Fatty Acids
The REDUCE-IT trial was a double-blind CV outcome trial that randomized 8,179 patients with ASCVD or primary prevention diabetes (with additional CV risk factors) to icosapent ethyl 2 grams twice daily or placebo in addition to statin therapy.49 All patients had LDL-C values of 41–100 mg/dL and fasting triglyceride values of 150–499 mg/dL (± 10%). After a mean of 4.9 years, CV events were reduced 25% with icosapent ethyl. These robust findings led to FDA approval of icosapent ethyl for CV event lowering in combination with statin therapy for patients with clinical ASCVD or primary prevention diabetes and additional CV risk factors, when triglycerides are 150–499 mg/dL.
The STRENGTH trial was a double-blind CV outcome trial that used a carboxylic acid omega-3 fatty acids product that contained EPA and DHA.50 STRENGTH randomized 13,078 patients with ASCVD or high-risk primary prevention patients (including diabetes), and triglyceride values of 180–499 mg/dL to omega-3 carboxylic acids 4 grams/day or placebo in addition to statin therapy. This study was stopped due to futility, as there was no difference in CV events between treatments.
Clinicians should be aware of the CV benefits of EPA-only omega-3 fatty acids (icosapent ethyl) in secondary prevention patients or primary prevention patients with diabetes. This should be recommended when triglyceride values are 150–499 mg/dL despite maximal statin therapy and ideal LDL-C lowering.22,51 The mechanism explaining how EPA lowers CV event is not fully understood but is related to triglyceride lowering. Importantly, clinicians should not extend the benefits of EPA-only omega-3 fatty acids to the over-the-counter fish oil products or prescription omega-3 ethyl esters, because they contain both EPA and DHA, for which CV event lowering benefits have not been demonstrated.
ANTITHROMBOTIC THERAPY
Antiplatelet agents (e.g., aspirin, clopidogrel) are the primary antithrombotic therapy used to prevent ASCVD in patients with CV risk. Some high CV risk patients may also be treated with an anticoagulant (e.g., warfarin, apixaban, rivaroxaban) based on other comorbidities. Due to bleeding risk, especially with combination therapy, these agents must be used in situations for which evidence demonstrates that benefits outweigh risks. Several ACC/AHA guidelines are available for clinicians, and many focus on specific disease populations.
Secondary Prevention
Antiplatelet Therapy
Low-dose aspirin (75–100 mg daily) is currently the foundational antiplatelet agent for prevention of recurrent CV events in patients with clinical ASCVD. Aspirin is highly recommended in AHA guidelines for patients with stable ischemic heart disease, peripheral arterial disease (PAD), and non-cardioembolic ischemic stroke, unless contraindicated.52-54 Clopidogrel alone and dipyridamole with aspirin are evidence-based alternatives to aspirin monotherapy for patients with prior ischemic stroke.52 The use of aspirin with ticagrelor has been shown to reduce death and recurrent stroke than aspirin alone for the first 30 days after acute stroke, but its use is associated with a higher risk of bleeding.55 Combination therapy using an antiplatelet agent with an anticoagulant is not generally recommended based on uncertain evidence demonstrating benefits and a significant increase in major bleeding.
Antiplatelet With Anticoagulant Therapy
Several studies have evaluated the combination of aspirin with an anticoagulant agent in patients requiring secondary prevention. The COMPASS trial was a landmark clinical trial that evaluated 27,395 patients with stable ASCVD in a double-blind, prospective CV outcome trial. Patients were randomized to the combination of rivaroxaban 2.5 mg twice daily with aspirin 100 mg daily, rivaroxaban 5 mg twice daily monotherapy, or aspirin 100 mg daily monotherapy. This study was stopped early after 23 months because of a significant difference in the primary endpoint (CV death, stroke, or MI) favoring the rivaroxaban plus aspirin group. However, this benefit was offset by an increased risk of major bleeding events and limited the broader use of this combination antithrombotic strategy in secondary prevention.
The VOYAGER PAD was a double-blind trial in 6,564 patients with PAD who had undergone revascularization.56 Patients in this trial were randomized to rivaroxaban (2.5 mg twice daily) plus low-dose aspirin or placebo plus aspirin for 3 years. The primary efficacy endpoint (acute limb ischemia, major amputation for vascular causes, MI, ischemic stroke, or CV death) was reduced 15% in the rivaroxaban with aspirin arm with no difference in the primary safety endpoint of major bleeding using Thrombolysis in Myocardial Infarction criteria (but there was a significant increase using International Society on Thrombosis and Haemostasis major bleeding criteria). These studies provide strong evidence that aspirin with rivaroxaban is efficacious in patients with PAD after a revascularization procedure.
The benefits of aspirin with rivaroxaban in VOYAGER PAD should not be extrapolated to other anticoagulants. Estimating equivalent doses of warfarin or another direct oral anticoagulant is not reasonable. This evidence-based treatment strategy in secondary prevention patients with PAD exclusively applies to aspirin with rivaroxaban.
Primary Prevention
Aspirin has been evaluated for primary prevention of ASCVD in multiple landmark CV outcome trials. These placebo-controlled trials have not demonstrated a reduction in the primary endpoint of CV events with aspirin therapy. Meta-analyses of these trials demonstrated a small reduction in MI in men and stroke in women that is offset by increased bleeding risk. Therefore, the U.S. Preventive Services Task Force in 2016 provided moderate/weak recommendations to consider aspirin for primary prevention in a narrow range of patients (age 50–69).57
Three large CV outcome clinical trials that evaluated the use of aspirin in primary prevention were published in 2018.58-60 These trials evaluated more than 47,000 patients who were either intermediate-risk for ASCVD or had a diabetes. Only 1 study, ASCEND, demonstrated a reduction in the primary endpoint of CV events, and it exclusively included patients age ≥40 years with diabetes.58 In all 3 of these trials, the risk of major bleeding was higher with aspirin.
A subsequent meta-analysis incorporated these data in an analysis of 13 randomized, placebo-controlled trials comparing aspirin with placebo in 164,225 primary prevention patients.61 In this analysis, aspirin was associated with an 11% reduction in major CV events, but a 43% increase in major bleeding.
In 2019, ACC/AHA released a guideline on the primary prevention of CV disease,62 which recommends that low-dose aspirin (75–100 mg orally daily)
- might be considered among select adults age 40–70 years who are at higher ASCVD risk but not at increased bleeding risk
- should not be administered on a routine basis for the primary prevention of ASCVD among adults age >70 years
- should not be administered among adults of any age who are at increased risk of bleeding
Data and recommendations identify a narrow population of patients who may benefit from aspirin therapy for primary prevention.
DIABETES MEDICATIONS AND CV RISK
Diabetes is a major independent risk factor for ASCVD; CV risk reduction strategies are thus important for all patients with diabetes. In 2008, the FDA required that all new glucose-lowering medications conduct ongoing CV outcome trials.63 The resulting CV outcome data for glucose-lowering medications in type 2 diabetes significantly influences selection of pharmacotherapy.
Metformin is widely accepted as the first-line medication for most patients with type 2 diabetes based on evidence demonstrating reductions in CV events and mortality.29,64,65 The sodium-glucose cotransporter-2 inhibitor (SGLT2i) and glucagon-like peptide-1 receptor agonist (GLP1-RA) medications have been extensively studied in CV outcome trials.66 Most of the patients in these trials were treated with metformin already. Although within-class differences are evident among individual products, these medication classes have both been shown to reduce CV events (Table 7). Several SGLT2i medications have also demonstrated reductions in progression of renal disease and reductions in heart failure among patients with and without heart failure.
| Table 7. Evidence-Based Effects of SLGT2i And GLP1-RA Medications That Should Be Considered Within Patient-Clinician Priorities for Treatment66 |
| Benefits |
SGLT2i
(canagliflozina,b, dapagliflozinc, empagliflozina, ertugliflozin) |
GLP1-RA
(albiglutide, dulaglutidea, exenatide, liraglutidea, lixisenatide, semaglutidea) |
| Major adverse cardiovascular event risk lowering |
+++ |
+++ |
| Heart failure prevention |
+++ |
|
| Weight loss |
+ |
+++ |
| Renal disease progression prevention |
+++ |
+ |
| Contraindications |
- History of serious hypersensitivity reaction to drug
- Pregnancy or breastfeeding
- On dialysis
- eGFR <30 mL/min/1.73 m2 (dapagliflozin)
- ESRD (dapagliflozin and empagliflozin)
- Severe renal impairment (empagliflozin)
|
- History of serious hypersensitivity reaction to drug
- Pregnancy or breast feeding
- Severe renal impairment or end-stage renal failure (exenatide, lixisenatide)
- Personal or family history of medullary thyroid cancer
- Personal or family history of multiple endocrine neoplasia, type 2
|
| Cautions |
- Discontinue ≥3 days before a planned surgery to prevent postoperative ketoacidosis
- Wean or stop sulfonylurea or glinide and consider reducing total daily insulin dose by 20% when starting therapy if A1C is controlled or history of hypoglycemia
- May contribute to intravascular volume contraction; consider stopping or reducing diuretic dose.
- Use with caution in patients with prior amputation, severe peripheral neuropathy, severe peripheral vascular disease, or active diabetic foot ulcers or soft tissue infections.
- Possible increased risk of bone fractures (canagliflozin)
|
- Hypoglycemia risk increased with insulin, sulfonylureas, or glinides.
- May delay gastric emptying
- Care should be taken in patients with prior gastric surgery, including bariatric surgery
|
| Adverse effects |
- Genital fungal infections
- Urinary tract infections
- Euglycemic diabetic ketoacidosis
- Lower limb ulcerations and soft tissue infections
|
- Nausea, vomiting, diarrhea, headache, weakness, or dizziness
- Weight loss
- Injection site reactions
|
Abbreviations used: SGLT2i, sodium-glucose cotransporter-2 inhibitor; GLP1-RA, glucagon-like peptide-1 receptor agonist
+ indicates the magnitude of evidence supporting the benefit
aFDA-labeled indication to reduce major adverse cardiovascular events
bFDA-labeled indication to reduce kidney disease progression
cFDA-labeled indication to reduce heart failure |
Long-term CV and renal benefits of SGLT2i and GLP1-RA medications are robust. To assist clinicians in selecting evidence-based treatments for type 2 diabetes, both the ACC and AHA published guidance documents in 2020.66,67 The ACC document is an expert consensus decision pathway (Figure 5), and AHA is a Scientific Statement. Both recommend that clinicians evaluate patient-specific risk for ASCVD and renal disease when selecting an SGLT2i or GLP1-RA and select drugs with proven benefit (Table 7).These recommendations are mostly aligned with the 2021 American Diabetes Association recommedations.29 However, the American Diabetes Association clearly identified metformin as first-line therapy while the ACC and AHA recommendations do not explicitly address the preferred used of metformin first.
| Figure 5. ACC-Recommended Evidence-Based Selection of Newer Medications for Type 2 Diabetes Based On Cardiovascular and Kidney Disease Risk66 |
|
CONCLUSION
The progress in understanding and managing CV disease as outlined in this program is fundamental to practice of pharmacy. By staying current with concepts of pathophysiology, prevention, and treatment of these conditions, pharmacists can contribute to improved patient care and better lives for patients with conditions such as hypertension, dyslipidemia, and type 2 diabetes.
REFERENCES
- Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular diseases and risk factors, 1990-2019: update from the GBD 2019 study. J Am Coll Cardiol. 2020;76(25):2982-3021.
- Virani SS, Alonso A, Benjamin EJ, et al. Heart disease and stroke statistics—2020 update: a report from the American Heart Association. Circulation. 2020;141(9):e139-e596.
- American Heart Association. My Life Check - Life's Simple 7. Accessed March 12, 2021. https://www.heart.org/en/healthy-living/healthy-lifestyle/my-life-check--lifes-simple-7.
- Nambiar L, LeWinter MM, VanBuren PC, Dauerman HL. Decade-long temporal trends in U.S. hypertension-related cardiovascular mortality. J Am Coll Cardiol. 2020;75(20):2644-2646.
- Muntner P, Hardy ST, Fine LJ, et al. Trends in blood pressure control among US adults with hypertension, 1999-2000 to 2017-2018. JAMA. 2020;324(12):1190-1200.
- U.S. Department of Health and Human Services. The Surgeon General’s Call to Action to Control Hypertension. Washington, DC: U.S. Department of Health and Human Services, Office of the Surgeon General; 2020. Accessed March 12, 2021. https://www.cdc.gov/bloodpressure/docs/SG-CTA-HTN-Control-Report-508.pdf
- Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2018;71(19):e127-e248.
- Schwartz JE, Muntner P, Kronish IM, et al. Reliability of office, home, and ambulatory blood pressure measurements and correlation with left ventricular mass. J Am Coll Cardiol. 2020;76(25):2911-2922.
- Sprint Research Group. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373(22):2103-2116.
- Vaduganathan M, Claggett BL, Juraschek SP, Solomon SD. Assessment of long-term benefit of intensive blood pressure control on residual life span: secondary analysis of the Systolic Blood Pressure Intervention Trial (SPRINT). JAMA Cardiol. 2020;5(5):576-581.
- Bundy JD, Li C, Stuchlik P, et al. Systolic blood pressure reduction and risk of cardiovascular disease and mortality: a systematic review and network meta-analysis. JAMA Cardiol. 2017;2(7):775-781.
- Kitagawa K, Yamamoto Y, Arima H, et al. Effect of standard vs intensive blood pressure control on the risk of recurrent stroke: a randomized clinical trial and meta-analysis. JAMA Neurol. 2019.
- Suchard MA, Schuemie MJ, Krumholz HM, et al. Comprehensive comparative effectiveness and safety of first-line antihypertensive drug classes: a systematic, multinational, large-scale analysis. Lancet. 2019;394(10211):1816-1826.
- Savage RD, Visentin JD, Bronskill SE, et al. Evaluation of a common prescribing cascade of calcium channel blockers and diuretics in older adults with hypertension. JAMA Intern Med. 2020;180(5):643-651.
- Carey RM, Calhoun DA, Bakris GL, et al. Resistant hypertension: detection, evaluation, and management: a scientific statement from the American Heart Association. Hypertension. 2018;72(5):e53-e90.
- Hripcsak G, Suchard MA, Shea S, et al. Comparison of cardiovascular and safety outcomes of chlorthalidone vs hydrochlorothiazide to treat hypertension. JAMA Intern Med. 2020;180(4):542-551.
- Black HR, Elliott WJ, Grandits G, et al. Principal results of the Controlled Onset Verapamil Investigation of Cardiovascular End Points (CONVINCE) trial. JAMA. 2003;289(16):2073-2082.
- Yusuf S, Sleight P, Pogue J, Bosch J, Davies R, Dagenais G. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. The Heart Outcomes Prevention Evaluation Study Investigators. N Engl J Med. 2000;342(3):145-153.
- Hermida RC, Ayala DE, Mojon A, Fernandez JR. Influence of time of day of blood pressure-lowering treatment on cardiovascular risk in hypertensive patients with type 2 diabetes. Diabetes Care. 2011;34(6):1270-1276.
- Hermida RC, Crespo JJ, Dominguez-Sardina M, et al. Bedtime hypertension treatment improves cardiovascular risk reduction: the Hygia Chronotherapy Trial. Eur Heart J. 2020;41:4565-4576.
- Relates to: 'bedtime hypertension treatment improves cardiovascular risk reduction: Hygia Chronotherapy Trial'. Eur Heart J. 2020;41(16):1600.
- Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;139(25):e1082-e1143.
- Cholesterol Treatment Trialists Collaboration, Fulcher J, O'Connell R, et al. Efficacy and safety of LDL-lowering therapy among men and women: meta-analysis of individual data from 174,000 participants in 27 randomised trials. Lancet. 2015;385(9976):1397-1405.
- Rodriguez F, Maron DJ, Knowles JW, Virani SS, Lin S, Heidenreich PA. Association of statin adherence with mortality in patients with atherosclerotic cardiovascular disease. JAMA Cardiol. 2019;4(3):206-213.
- Cannon CP, Blazing MA, Giugliano RP, et al. Ezetimibe added to statin therapy after acute coronary syndromes. N Engl J Med. 2015;372(25):2387-2397.
- Sabatine MS, Giugliano RP, Keech AC, et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. 2017;376(18):1713-1722.
- Schwartz GG, Steg PG, Szarek M, et al. Alirocumab and cardiovascular outcomes after acute coronary syndrome. N Engl J Med. 2018;379(22):2097-2107.
- Virani SS, Akeroyd JM, Nambi V, et al. Estimation of eligibility for proprotein convertase subtilisin/kexin type 9 inhibitors and associated costs based on the FOURIER Trial (Further Cardiovascular Outcomes Research With PCSK9 Inhibition in Subjects With Elevated Risk): insights from the Department of Veterans Affairs. Circulation. 2017;135(25):2572-2574.
- American Diabetes A. 10. Cardiovascular disease and risk management: standards of medical care in diabetes–2021. Diabetes Care. 2021;44(suppl 1):S125-S150.
- Collins R, Armitage J, Parish S, Sleigh P, Peto R. MRC/BHF Heart Protection Study of cholesterol-lowering with simvastatin in 5963 people with diabetes: a randomised placebo-controlled trial. Lancet. 2003;361(9374):2005-2016.
- Cholesterol Treatment Trialists Collaborators, Kearney PM, Blackwell L, et al. Efficacy of cholesterol-lowering therapy in 18,686 people with diabetes in 14 randomised trials of statins: a meta-analysis. Lancet. 2008;371(9607):117-125.
- Greenland P, Blaha MJ, Budoff MJ, Erbel R, Watson KE. Coronary calcium score and cardiovascular risk. J Am Coll Cardiol. 2018;72(4):434-447.
- Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020;41:111-188.
- Newman CB, Blaha MJ, Boord JB, et al. Lipid management in patients with endocrine disorders: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2020;105(12):dgaa674.
- Orringer CE, Tokgozoglu L, Maki KC, Ray KK, Saseen JJ, Catapano AL. Transatlantic lipid guideline divergence: same data but different interpretations. J Am Heart Assoc. 2020;9(21):e018189.
- Ray KK, Bays HE, Catapano AL, et al. Safety and efficacy of bempedoic acid to reduce LDL cholesterol. N Engl J Med. 2019;380(11):1022-1032.
- Laufs U, Banach M, Mancini GBJ, et al. Efficacy and safety of bempedoic acid in patients with hypercholesterolemia and statin intolerance. J Am Heart Assoc. 2019;8(7):e011662.
- Ballantyne CM, Banach M, Mancini GBJ, et al. Efficacy and safety of bempedoic acid added to ezetimibe in statin-intolerant patients with hypercholesterolemia: a randomized, placebo-controlled study. Atherosclerosis. 2018;277:195-203.
- Handelsman Y, Jellinger PS, Guerin CK, et al. Consensus statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the management of dyslipidemia and prevention of cardiovascular disease algorithm - 2020 executive summary. Endocr Pract. 2020;26(10):1196-1224.
- Ray KK, Wright RS, Kallend D, et al. Two phase 3 trials of inclisiran in patients with elevated LDL cholesterol. N Engl J Med. 2020;382(16):1507-1519.
- Raal FJ, Kallend D, Ray KK, et al. Inclisiran for the treatment of heterozygous familial hypercholesterolemia. N Engl J Med. 2020;382(16):1520-1530.
- Dixon DL, Saseen JJ. Pharmacist-administered long-acting injectable PCSK9 service: a solution to improve patient access and adherence. J Am Pharm Assoc (2003). 10 December 2020; 10.1016/j.japh.2020.12.009.
- Rosenson RS, Burgess LJ, Ebenbichler CF, et al. Evinacumab in patients with refractory hypercholesterolemia. N Engl J Med. 2020;383(24):2307-2319.
- Raal FJ, Rosenson RS, Reeskamp LF, et al. Evinacumab for homozygous familial hypercholesterolemia. N Engl J Med. 2020;383(8):711-720.
- Aung T, Halsey J, Kromhout D, et al. Associations of omega-3 fatty acid supplement use with cardiovascular disease risks: meta-analysis of 10 trials involving 77917 individuals. JAMA Cardiol. 2018;3(3):225-234.
- Manson JE, Cook NR, Lee IM, et al. Marine n-3 fatty acids and prevention of cardiovascular disease and cancer. N Engl J Med. 2019;380(1):23-32.
- Bowman L, Mafham M, Wallendszus K, et al. Effects of n-3 fatty acid supplements in diabetes mellitus. N Engl J Med. 2018;379(16):1540-1550.
- Yokoyama M, Origasa H, Matsuzaki M, et al. Effects of eicosapentaenoic acid on major coronary events in hypercholesterolaemic patients (JELIS): a randomised open-label, blinded endpoint analysis. Lancet. 2007;369(9567):1090-1098.
- Bhatt DL, Steg PG, Miller M, et al. Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia. N Engl J Med. 2019;380(1):11-22.
- Nicholls SJ, Lincoff AM, Garcia M, et al. Effect of high-dose omega-3 fatty acids vs corn oil on major adverse cardiovascular events in patients at high cardiovascular risk: the STRENGTH randomized clinical trial. JAMA. 2020;324(22):2268-2280.
- Orringer CE, Jacobson TA, Maki KC. National Lipid Association scientific statement on the use of icosapent ethyl in statin-treated patients with elevated triglycerides and high or very-high ASCVD risk. J Clin Lipidol. 2019;13(6):860-872.
- Kernan WN, Ovbiagele B, Black HR, et al. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45(7):2160-2236.
- Fihn SD, Blankenship JC, Alexander KP, et al. 2014 ACC/AHA/AATS/PCNA/SCAI/STS focused update of the guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines, and the American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2014;64(18):1929-1949.
- Gerhard-Herman MD, Gornik HL, Barrett C, et al. 2016 AHA/ACC guideline on the management of patients with lower extremity peripheral artery disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2017;69(11):1465-1508.
- Johnston SC, Amarenco P, Denison H, et al. Ticagrelor and aspirin or aspirin alone in acute ischemic stroke or TIA. N Engl J Med. 2020;383(3):207-217.
- Bonaca MP, Bauersachs RM, Anand SS, et al. Rivaroxaban in peripheral artery disease after revascularization. N Engl J Med. 2020;382(21):1994-2004.
- Bibbins-Domingo K, Force USPST. Aspirin use for the primary prevention of cardiovascular disease and colorectal cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2016;164(12):836-845.
- Bowman L, Mafham M, Stevens W, et al. ASCEND: a study of cardiovascular events in diabetes: characteristics of a randomized trial of aspirin and of omega-3 fatty acid supplementation in 15,480 people with diabetes. Am Heart J. 2018;198:135-144.
- McNeil JJ, Wolfe R, Woods RL, et al. Effect of aspirin on cardiovascular events and bleeding in the healthy elderly. N Engl J Med. 2018;379(16):1509-1518.
- Gaziano JM, Brotons C, Coppolecchia R, et al. Use of aspirin to reduce risk of initial vascular events in patients at moderate risk of cardiovascular disease (ARRIVE): a randomised, double-blind, placebo-controlled trial. Lancet. 2018;392(10152):1036-1046.
- Zheng SL, Roddick AJ. Association of aspirin use for primary prevention with cardiovascular events and bleeding events: a systematic review and meta-analysis. JAMA. 2019;321(3):277-287.
- Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2019;140:e596-e646.
- Chong WH, Yanoff LB, Andraca-Carrera E, Thanh Hai M. Assessing the safety of glucose-lowering drugs — a new focus for the FDA. N Engl J Med. 2020;383(13):1199-1202.
- Holman RR, Paul SK, Bethel MA, Neil HA, Matthews DR. Long-term follow-up after tight control of blood pressure in type 2 diabetes. N Engl J Med. 2008;359(15):1565-1576.
- Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet. 1998;352(9131):837-853.
- Das SR, Everett BM, Birtcher KK, et al. 2020 Expert consensus decision pathway on novel therapies for cardiovascular risk reduction in patients with type 2 diabetes: a report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2020;76(9):1117-1145.
- Rangaswami J, Bhalla V, de Boer IH, et al. Cardiorenal protection with the newer antidiabetic agents in patients with diabetes and chronic kidney disease: a scientific statement from the American Heart Association. Circulation. 2020;142(17):e265-e286.
- Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2018;139:e1082-e1143.
- Web Supplement to the 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the management of blood cholesterol a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Accessed March 12, 2021. http://jaccjacc.acc.org/Clinical_Document/Cholesterol_GL_Web_Supplement.pdf.
Back to Top