
Expired activity
Please go to the PowerPak
homepage and select a course.
Cultivating Cultural Competency in Pharmacy Practice
INTRODUCTION
At the core of each person are their inherited traits as well as the choices that they make about their lifestyles (e.g., diet, exercise, leisure activities). Their health is further marked by their exposure to healthy or risky behaviors based on the places where they live, work, worship, learn or play. Our socioeconomic status, race and ethnicity, gender, age, and communities define our culture and shape our lives including our attitudes toward healthcare. As clinicians, we cannot assume that all patients have the same healthcare beliefs, values, and approach to healthcare. Each patient we encounter will have a unique health situation, social determinants will influence their exposure to healthy conditions and their cultural backgrounds will shape their health beliefs and behaviors. For this reason, it is important for the clinician to be able to recognize how differences in ethnicity and traditions may impact the patient-provider relationship, specifically when there is discordance between provider and patient ethnicity or language. Providers must learn the attitude, knowledge and skills to be culturally competent in order to provide effective, safe and compassionate quality health care.
Cultural competence has evolved from merely learning information and making assumptions about patients based on their backgrounds to focusing on the development of skills that follow the principles of patient-centered care. This encompasses the qualities of compassion, empathy, and responsiveness to the needs, values and preferences of the individual patient. Cultural competence aims to take things a step further by expanding the repertoire of knowledge and skills classically defined as patient-centered to encompass those that are especially useful in cross-cultural interactions. This includes eliciting the patient’s understanding of his or her condition, assessing decision-making preferences and the role of family, determining the patient’s views about traditional medicine versus complementary and alternative medicine, and building trust. Multiple societal, ethical, professional, and legal reasons exist for clinicians to be culturally competent. This manuscript will discuss the rational for cultural competency in health care, as well as provide tools for self-evaluation while providing guidance to develop a culturally competent approach to healthcare.
DEFINITIONS RELATED TO CULTURAL COMPETENCY
It has been stated that our culture defines us. However, it is often difficult to interact with others when we do not understand their background or culture. Culture can be defined in many ways but in its broadest sense culture is cultivated behavior that is the totality of a person's learned, accumulated experience which is socially transmitted, or more briefly, behavior through social learning.1 A culture is a way of life of a group of people that consists of the behaviors, beliefs, values, and symbols that they accept, generally without thinking about them, and are passed along by communication and imitation from one generation to the next. The Institute of Medicine (IOM) defines culture as “the accumulated store of shared values, ideas (attitudes, beliefs, values, and norms), understandings, symbols, material products, and practices of a group of people. Culture has both material and non-material aspects.”2 Once the definition of culture is understood one can work toward developing cultural competence. Competence is defined as having the capacity to function effectively as an individual within the context of the cultural beliefs, behaviors, and needs presented by consumers and their communities. Cultural competency then is the attitudes, knowledge, skills, and values that an individual has and uses in working effectively in a cross-cultural environment.3
While we must address health at the individual level, providers and policymakers must also understand and address healthcare at the community and population level. For this reason, we need to define the terms community and community competency. Communitiesmay be defined as organized groups of people with a shared identity that exist around racial and ethnic groups, socioeconomic position, religion, age, gender, language, as well as other cultural ties. Community competency encompasses cultural competency; however, it also recognizes the unique role of communities as a type of culture. Within a community competency framework, at the core of a community are history, context, geography and culture.4 What is the difference between cultural competency and community competency? Cultural competency helps clinicians understand the individual and allows for care to be patient centered. Community competency provides a broader context for clinicians to work with individuals and families, as it incorporates the influence of the population and environment on the individual. It is important for a provider to acknowledge the significant influence one’s community has on an individual.
In conversations involving cultural competency and throughout the literature the terms race and ethnicity are used repeatedly and often misrepresented. Imprecision in defining and using the terms race and ethnicity is apparent in the conflicting and overlapping terminologies used by the government when collecting and classifying statistical data. In some instruments, the federal government considers race and ethnicity to be distinct concepts; in other instruments, questions on race include racial, national origin, and ethnicity response options.5 Clarifying the terms is important to distinguishing the diversity of the US population. The IOM defines race as a “sociocultural concept wherein groups sharing certain physical characteristics are treated differently based on stereotypical thinking, discriminatory institutions and social structures, a shared worldview, and social myths.”The IOM explains ethnicity as a concept referring to a shared culture and way of life, especially reflected in language, religion, and material culture products.2 Table 1 lists other terms that are necessary to understand related to the concept of cultural competency.
| Table 1. Terms Related to Cultural Competency6,7,8,9 |
| Term |
Definition |
| Health disparities |
Health status differences that occur in groups of people because of ethnicity, gender, race, socioeconomic status, disability, geographic area, culture, language or education level6 |
| Social determinants of health |
Conditions in the environments in which people are born, live, learn, work, play, worship, and age that affect a wide range of health, functioning, and quality-of-life outcomes and risks7 |
| Cultural humility |
A lifelong commitment to self-evaluation and self-critique in the context of the patient–provider relationship through patient-centered care8 |
| Cultural proficiency |
Occurs when provider and health care systems set a goal to view culture as a positive component of health rather than as simply something to understand to provide equitable patient care9 |
RATIONAL FOR CULTURAL COMPETENCE
Changes in demographics, health disparities and patient safety are among the reasons that cultural competency in healthcare is crucial. According to the U.S. Census Bureau’s 2019 data, 76.3% of the population identified as Caucasian, 13.4% as African American, 1.3% as American Indian or Alaska Native, 5.9% as Asian, 18.5% as Hispanic or Latino, 0.2% as Native Hawaiian or other Pacific Islander and 2.8% of the population identified as two or more races. In data from 2014-2018, 21.5% of families reported speaking a language other than English in their home.10 There is tremendous diversity of religious beliefs and practices in this country. According to the 2008 PEW report, nearly 92% of the population believed in the existence of God or a universal spirit with 70.6% reporting being Christian. Of the non-Christian faiths, 1.9% reported being Jewish, 0.9% Muslim, 0.7% Buddhist, and 0.7% identified as Hindu.11 Census data indicate that people of European American descent will no longer make up the majority of the population in the United States and projections for 2050 provide additional support for this shift depicting a demographic picture of the United States that is very different from today’s population. According to the 2017 National Population Projection, the U.S. population will be 70.1% Caucasian, 14.6% African American, 1.4% American Indian or Alaska Native, 8.4% Asian, 0.3% Native Hawaiian and Other Pacific Islander, and 25.7% will be Hispanic or Latino by the year 2050.12
Health disparities generally occur in populations who have systematically experienced a social, economic, or environmental disadvantage in society. Although the term disparitiesare often interpreted to mean racial or ethnic disparities, many dimensions of disparity exist in the United States, particularly in health. Gender, sexual identity, age, disability, socioeconomic status, and geographic location all contribute to an individual’s ability to achieve good health.7 One of the overarching goals of Healthy People 2020 is to eliminate health disparities that exist in the U.S. and achieve health equity. Throughout the next decade, Healthy People 2020 will assess health disparities by tracking rates of illness, death, chronic conditions, behaviors, and other types of outcomes in relation to demographic factors including race and ethnicity, gender, sexual identity and orientation, disability status and geographic location (urban versus rural).7 A healthcare provider’s cultural competency can help to achieve the Healthy People 2020 goals by addressing health disparities in their communities.
By understanding the needs of underserved patients and by identifying the unique resources available within these populations, the healthcare provider can positively impact a patient’s healthcare experience. For example, a healthcare provider who understands the importance of community support in a Latino patient seeking healthcare can include key community members as an active member during treatment and post-treatment care. An urban hospital explored the role of the promotora de salud (health promoter) who provided diabetes self-management education to Puerto Rican diabetics in her community. Respondents reported satisfaction with the program, increased ability to self-manage diabetes, and strengthened connections with other Latino diabetics. The authors concluded that the hospital and community-based partnership promotora model appeared to be effective for providing chronic disease self-management education in an urban community setting.13 By working with the patient’s cultural needs and expectations, the clinician can use otherwise overlooked support systems such as family, friends, and religious ties in a community with fewer or overtaxed resources. Additionally, the provider’s ability to empower patients through cultural competency will facilitate the development of trusting patient-provider relationships within the community.
Culture and language may also play a role in patient safety. A study that looked at hospitals across the country found that patients with limited English proficiency were more likely to be harmed versus their English-proficient counterparts when they experienced adverse events and that harm was more likely to be severe.14 Patient safety events that can result from the failure to address culture, language, and health literacy include diagnostics errors, missed screenings, unexpected negative responses to medication, harmful interactions with complimentary/alternative medicine, delayed treatment, inappropriate care transitions, and non-adherence.15 Consider this true patient scenario. A female Asian patient was noncommunicative with the physicians and staff during the first few days of her hospitalization which led to a delay in obtaining consent for surgery. The staff and physicians, concerned with privacy issues, generally spoke with the patient when family members were not present. It was not until a visiting chaplain of the same nationality explained the cultural requirement that a male be present for a female’s care that communications became successful between the providers and the patient.16 Cultural “incongruences” among patients and providers may lead to lack of adequate knowledge and ineffective or unsafe care. Culturally competent health care providers can remove this barrier.
Health disparities and medication safety impact all areas of health care, including the practice of pharmacy. Culturally competent pharmaceutical care could result in more successful patient education, increases in patients’ health-seeking behaviors, more appropriate testing and screening, avoidance of drug complications, greater adherence to medical advice, and expanded choices and access to high-quality clinicians.17 Understanding the types of alternative and complimentary medications that are common in certain cultures is a key area where a pharmacist can have impact. By being knowledgeable about non-traditional therapies, pharmacists can avoid drug complications and unwanted interactions. When a counseling session can be individually tailored to the patient’s healthcare beliefs and behaviors, the message is likely to be better received and adherence can be improved. Pharmacists who understand genetic backgrounds and common health-related behaviors of various cultural groups may be better able to recommend appropriate testing, screening, and consider the unique effects certain medications will have on different genetic variants. For example, African Americans may not trust the healthcare system or research projects because of previous injustices such as the Tuskegee syphilis study. Being aware of injustices as a result of this study will help providers understand the concerns the African American culture may have when it comes to interactions with the health care system. When pharmacists and technicians can proficiently communicate with their patients and develop a trusting relationship, patients are more likely to increase their health-seeking behaviors. In addition, expanded choices and access to care become available to patients who no longer need to restrict themselves to a small pool of providers who share their cultural beliefs.
LEGAL AND ACCREDITATION REQUIREMENTS
Legal and regulatory issues surrounding cultural competency include understanding and interpreting various legal regulations and accreditation standards for healthcare organizations. Title VI of the Civil Rights Act “prohibits discrimination on the basis of race, color, and national origin in programs and activities receiving federal financial assistance.”18 In 2000, under Executive Order 13166 of Title VI, federal agencies became required to evaluate and develop services for persons with limited English proficiency and provide meaningful access to these services.19 Additionally, the Omnibus Budget Reconciliation Act of 1990 (OBRA’90) mandated that pharmacists provide the option of counseling to all Medicaid patients regarding their prescription medications.20 Cultural competence is essential if these laws are going to be upheld in the pharmacy.
In addition to legal requirements, the 2013 enhanced National CLAS Standards (Culturally and Linguistically Appropriate Services) provided a framework for health and healthcare organizations to promote health equity and remove health disparities for diverse populations. Fourteen standards were developed and organized into three main themes including maintaining a culturally competent workforce, language assistance services, and accountability and continuous improvement for culturally competent outcomes. As a result of these standards organizations were required to focus on communication and language assistance as stated in the below mandates.21
- Offer language assistance to individuals who have limited English proficiency and/or other communication needs at no cost to them
- Inform all individuals of the availability of language assistance services in their preferred language, verbally and in writing (Martti is an example of an on-demand translating service available at https://www.martti.us/)
- Ensure the competence of individuals providing language assistance
- Provide easy-to-understand print and multimedia materials and signage in the languages commonly used by the populations served
The Joint Commission, the primary national accrediting body for healthcare organizations, supports CLAS standards through requirements for effective communication, cultural competence, and patient-oriented care. This roadmap highlights the importance of integrating culturally competent care from admission to discharge. The Joint Commission also emphasizes leadership involvement and ongoing staff education related to cultural competency. 22 Additionally, several states have passed legislation requiring healthcare professionals to complete training in cultural competency.23 The incorporation of cultural competency into Joint Commission accreditation requirements and other legal mandates gives organizations and clinicians further rationale to move toward culturally competent care.
Professional practice standards further justify the need for pharmacists to be culturally compliant. The APhA Code of Ethics for Pharmacists and Oath of a Pharmacist both uphold cultural competence as a core value in pharmacy. Many of the ethical principles in the Code of Ethics relate to cultural competency. Specifically, the code of ethics requires that a pharmacist communicates with patients in terms that are understandable and respects personal and cultural differences among patients. A pharmacist is also required to respect the beliefs and values of other colleagues even if they are different from their own.24 While the Oath of a Pharmacist does not specifically address cultural competence, it is implied throughout. In considering the welfare of humanity and ensuring optimal outcomes for all patients, a pharmacist must be able to understand health beliefs, values, and behavioral differences in all cultures.25 Not only can pharmacists and pharmacy technicians uphold the legal, accrediting and regulatory requirements but they can encourage cultural competence among their colleagues, act as agents to eliminate discriminatory practices, improve health disparities, and ultimately improve patient care.
CULTURE COMPETENCY MODELS
Several models are often used in healthcare to describe and understand cultural competency. These include the Cultural Competence Continuum, the Purnell Model for Cultural Competence and the Process of Cultural Competence in Delivery of Healthcare Services. While these models differ in their approach, a common theme to all of them signifies that cultural competency is a process rather than an achievement. Each of the three models will be explored below.
Cultural Competence Continuum
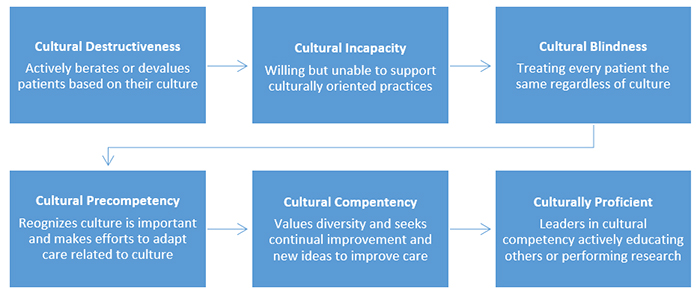
In this model, possible ways to respond to cultural differences are described in order to help a clinician recognize where they are in the process of becoming more culturally competent. Six stages are described in a stepladder model starting with cultural destructiveness and ascending toward cultural proficiency. These six stages are outlined in Figure 1. At each level the principles of valuing difference, self-assessment, building cultural knowledge, and changing current practices can be applied as growth along the ladder continues. When progress is made at each level in implementing attitudes and practices change in the desired direction, one becomes more culturally competent. 26
Figure 1. Stages of Cultural Competency in the Cultural Competence Continuum26
Process of Cultural Competence in Delivery of Healthcare Services
In this model, five constructs with an interdependent relationship describe the developing process of cultural competence: cultural awareness, cultural knowledge, cultural skill, cultural encounters and cultural desire. Through self-assessment of cultural and professional biases and beliefs, clinicians develop increased cultural awareness. This self-awareness helps clinicians to recognize the risk of imposing personal beliefs in patient care. As clinicians learn more about beliefs and practice, disease epidemiology, and the efficacy and acceptance of therapies that are found in diverse cultures, they expand their cultural knowledge. They acquire cultural skills as they learn how to collect subjective information and social histories as well as conduct physical assessments that are relevant to different cultures. For example, in Asian cultures the practices of coining (coins dipped in oil, heated, and then rubbed on skin) and cupping(heated glass cups placed on skin to create a vacuum) or pinching of skin in order to draw out illnesses is a common practice. These practices may produce bruises, burns, or welts on the skin that might be confused with signs of physical abuse. Being aware of these cultural practices will allow for expansion of cultural knowledge and help the clinician acquire the cultural skills to appropriately assess the patient. The increased opportunity for cultural encounters through directly interacting with individuals and families from diverse groups helps to have practical experience with cultural norms and variations as well as language needs. At the intersection of awareness, knowledge, skills, and encounters is cultural desire. When clinicians want to learn and grow in the process of cultural competency and do not feel obligated to care for diverse cultures, they expand their cultural desire.27
Purnell Model for Cultural Competence
The Purnell model explores the relationship of family, community, and the global society as they influence the individual person. The model outlines 12 different cultural beliefs and traits that may affect an individual and are often interconnected, such as healthcare practices, spirituality, communication styles, and workforce issues. Refer to Table 2 for a list of the 12 domains of the Purnell model. This model illustrates that healthcare providers often experience a learning process related to their cultural consciousness. In this continuum, providers may move from being unconsciously incompetent (not aware of lack of competence), consciously incompetent (aware of lack of competence), consciously competent (aware of improving competence) toward unconscious competence. When a provider is unconsciously competent, they have been able to integrate skills, knowledge, and awareness of the varying cultural, familial, and broader community influences on a patient with fluency.28
| Table 2. Twelve Domains of the Purnell Model for Cultural Competence28 |
| Domain |
Characteristics |
| Heritage |
Concepts related to the country of origin, current residence, the effects of the topography of the country of origin and current residence, economics, politics, reasons for emigration, educational status, and occupations |
| Communication |
Concepts related to dominant language and dialects, non-verbal communication, clock versus social time, use of names |
| Family roles |
Concepts related to head of household, gender roles, child rearing practices, roles of aged and extended family members |
| Workforce |
Concepts related to autonomy, acculturation, assimilation, gender roles, ethnic communication styles, and individualism |
| Biocultural ecology |
Includes skin color variation, physical stature, genetics, hereditary and drug metabolism differences |
| High-risk behaviors |
Use of drugs or alcohol, lack of exercise, high-risk sexual practices |
| Nutrition |
Having adequate food, food choices, rituals or taboos around food, food during illness and for health promotion |
| Pregnancy/childbearing |
Fertility practices, birth control methods, birthing practices, post-partum treatment |
| Death rituals |
Rituals and behaviors to prepare for death or burial |
| Spirituality |
Religious practices and use of prayer |
| Healthcare practice |
Beliefs in acute or preventive care, magico-religious beliefs, biomedical beliefs, self-medicating practices, mental illness views, organ donation/transplant |
| Healthcare practitioner |
Status, use and perception of healthcare providers |
SELF-EVALUATION OF CULTURAL COMPETNECY
The process of self-evaluation may begin with the simple act of a practitioner reflecting on the values and beliefs that shape their worldview, their perceptions of health and illness, and the existence of stereotypes or myths about other cultures. To assist in this process, self-assessment instruments have been developed to guide individuals in their reflection of cultures, values and beliefs. A variety of assessment tools designed for use by individual practitioners are available in both written and online formats. Although there are no correct answers, these instruments provide individuals the opportunity to identify personal attitudes, values and beliefs that do not foster cultural competence. By becoming aware of these issues, the individual can make plans to improve upon or change these characteristics and move toward a more culturally competent approach to providing healthcare.
For clinicians seeking to understand their own biases, the mnemonic “ASKED” is useful in helping them work with patients from a variety of cultures. The mnemonic summarizes the Process of Cultural Competence in the Delivery of Health care Services Model described above. The following questions are asked in this mnemonic: 29
- Awareness: Am I aware of my personal biases and prejudices towards a cultural group different than mine?
- Skill: Do I have the skill to conduct a cultural assessment in a culturally sensitive manner?
- Knowledge: Do I have knowledge of the client’s worldview and the field of biocultural ecology?
- Encounters: How many face-to-face and other encounters have I had with clients from diverse cultural backgrounds?
- Desire: Do I really want to be culturally competent?
Various on-line assessment tools are described below:
- Self-Assessment Checklist for Personnel Providing Primary Healthcare Services is a 37-item questionnaire that assesses four domains including physical environment, communication style, materials and resources and values/attitudes. It can be accessed on line at https://nccc.georgetown.edu/documents/Checklist%20PHC.pdf.
- Cultural Competence Self-Assessment Tool is a 7-item questionnaire that was developed by the Center for Cross Cultural Health designed to help an individual assess their strengths and weaknesses in addressing the cultural diversity of patients and colleagues. It is available at https://docs.ucare.org/filer_public/files/culturalcompetenceselfassessment.pdf.
- The Implicit Association Test was founded in 1998 by Project Implicit to foster awareness of implicit social cognition, thoughts and feelings outside of conscious awareness and control. There are 15 different tests to uncover one’s unconscious bias. The test is available at https://implicit.harvard.edu/implicit/takeatest.html.
Regardless of which tool is used, an assessment of cultural competency should be conducted periodically on an ongoing, long-term basis. Individuals are always on a cultural-competency continuum, with varying levels of awareness, knowledge and skills. Periodic use of these tools can help identify directions one is moving on the continuum in order to make necessary adjustments.
STEPS TO IMPROVE CULTURAL COMPETENCY
The first step to become more culturally competent is to examine your own cultural background. In her book, Cultural Diversity in Health and Illness, Spector lists some questions to consider to better understand one’s cultural heritage and its effects on health care perceptions.30 The questions below include many from Spector’s work, as well as some more general cultural background questions.31
- What is your cultural heritage?
- Where did your parents/grandparents/great grandparents come from?
- What were/are some foods, celebrations, rituals, clothing, etc. that were meaningful to your family and symbolized your cultural background?
- How do you define health?
- How do you keep yourself healthy?
- How do you define illness?
- What causes illness?
- What would you define as a minor, or non-serious medical problem?
- How do you know when a given health problem does not need medical attention?
- What health problems do you self-diagnose?
- Who do you seek for help with minor health problems? Major health problems?
- Do you use over the counter medications? Which ones and when?
- Who makes health care decisions in your family?
- What expectations are there for caring for an elderly relative?
There are several other recommendations that clinicians can undertake when striving for cultural competence. Consider implementing several of the actions below as you continue along your journey towards cultural competence.
- Immerse yourself in a neighborhood/community that is unfamiliar to you. Explore the community just as it is part of your daily routine. This may mean going to the grocery store, clinic, convenience stores or local restaurants to get a taste of the culture. You can also consider learning a second language or reading memoirs or non-fictional stories about other cultures.32
- Talk with people of diverse backgrounds. Volunteer at community centers or soup kitchens. Try to be involved in social interactions such as interacting at parties, religious services and cultural events. A real challenge is to put yourself in a situation where you are the only one of your cultural group.32
- Attend diversity focused conferences. Get formal training on diversity-related research and practice issues and meet potential collaborators at conferences focused specifically on diversity issues.32
- Read about culture specific disease states and evidence-based interventions. Racial and ethnic disparities have been found in many disease states, such as heart disease, cancer, cerebrovascular disease, HIV/AIDS, asthma, and diabetes.33 These racial differences in response to pharmacologic and other therapeutic regimens may reflect genetic differences, differences in the pathogenesis of diseases, and environmental factors, such as differences in diet and health-related behaviors. Becoming familiar with how culture affects specific disease states and the different responses to various treatments will improve the health outcomes for diverse patients.
- Connect with cultural leaders. In many cultures there is an intersection between spirituality, religion and health. Reaching out to religious leaders of various cultures may help the clinician to determine this intersection and focus on ways to best address the patient’s illness. Several studies have shown that addressing the spiritual needs of the patient may enhance recovery from illness.34 Learning about the practices of traditional healers is another avenue to explore different health beliefs and practices. Each culture has its own terminology for their traditional healers some of these include curanderos, shamans, herbalists, folk healers, and diviners. Exploring the services of a local community health center may help to locate these types of different traditional heathers.
In the clinical setting, it is important to recognize how an individual patient experiences and understands their health. This view may be very different from the Western biomedical model which proposes that there is a pathophysiologic or etiologic reason for disease. In many cultures the source and meaning of illness may be attributed to a variety of other causes such as spiritual or religious influences, social factors and the environment.35 The clash of cultures between patient and provider can sometimes cause confusion about the true causes of an illness and the effects of a treatment. To help identify cultural differences in a clinical setting, clinicians can ask patients questions to help elucidate these differences in beliefs. One patient assessment tool that has been particularly useful to clinicians is often referred to as Kleinman’s Questions. The model consists of eight questions designed to elicit the patient’s cultural perspective on his or her illness.29 The questions are listed in Table 3.
| Table 3. Kleinman’s Questions29 |
|
Question
|
|
What do you think has caused your problem?
|
|
Why do you think it started when it did?
|
|
What does your sickness do to you? How does it work?
|
|
How severe is your sickness? Will it have a short or long duration?
|
|
What kind of treatment should you receive?
|
|
What are the most important results you hope to receive from this treatment?
|
|
What are the chief problems your sickness has caused you?
|
|
What you do you fear about your sickness?
|
Learning a patient’s view about their specific illness and immersing yourself in different cultures by doing some of the activities discussed above may help to break down barriers associated with cross-cultural communication.
CROSS-CULTURAL COMMUNICATION SKILLS
Effective communication skills required to work with patients from diverse cultures include looking for both nonverbal and verbal cues. Clinicians can often gain clues for how to interact with patients by observing their behaviors and following their mannerisms. Eye contact is a good example of how cultural groups greatly differ in the use of nonverbal communication. In most dominant cultures in the United States, eye contact is a sign of being honest and trustworthy. In many Eastern and some Caribbean cultures, meeting another’s eyes can be perceived as rude or aggressive. Asians and Hispanic/Latinos regard a person who makes eye contact as angry or unapproachable.36 Being aware of the cultural influences on eye contact can help a health care provider avoid judgment about a client’s character. In addition to differing preferences of eye contact, patients will have varying preferences of personal space and physical contact. In some cultures, patients prefer only a handshake or a nod of acknowledgment for greetings, whereas in other cultures, patients will welcome a light tap on the shoulder or even a hug. For example, a Japanese woman may reach out to a female pharmacist, but shy away from her male colleague. In contrast, for many African Americans touch is an essential part of health care.31 If language is not a problem, space and touch issues can be addressed with honest and direct dialogue by stating, “Is it okay if I touch your arm?” This can prevent misunderstandings and awkward situations. Facial expressions may also have the potential to be misleading. Nodding and saying yes may seem an indication of understanding; however, in some Southeast Asian cultures it simply indicates the person is paying attention and being polite. Requesting that the patient demonstrate understanding by repeating what has been told can ensure that the correct message has been received.31
Verbal cues include recognizing whether patients prefer to be called using their first name or last name or a more formal greeting. Some patients embrace the opportunity to talk and get to know their provider before jumping into medical information.30 Using vocabulary that is consistent with the culture of a patient can help providers gain the trust and respect of their patients. Expecting pharmacists and technicians to become fluent in all the languages and cultural customs of the patients they serve is impractical. However, it may be useful to learn more about the client population in which they interact with on a consistent basis. Being skilled in active listening and displaying empathy can assist providers in being effective in cross-cultural communication interactions.
CONCLUSION
The influence of culture on healthcare encompasses understanding social determinants of health and how environments and community influences help shape the health of individuals and families. The United States with its culturally diverse society, health disparities, and patient-safety concerns is faced with unique opportunities and challenges in patient care. To work in this environment, clinicians should understand the legal and regulatory issues related to cultural competency and their commitment to the profession requires the fair and equal treatment of all patient populations. To excel in diverse patient care, pharmacists and technicians need the knowledge and skills to elicit patients’ explanation of their health status, recognize potential cultural influences on healthcare beliefs and practices, and communicate effectively with patients from different cultures. Self-assessments can reveal helpful information about one’s own attitudes, values, and capacity to provide culturally appropriate services to patients and communities. The process to cultural competency is a continual journey for the clinician that requires ongoing assessment and active steps to improve knowledge, skills and attitudes. The ability for providers to navigate compassionately and effectively in a diverse population can help create a safe and positive healthcare environment for diverse patients to receive care and will become critical as the landscape of the nation in which we practice continues to become increasingly culturally diverse.
REFERENCES
- Hofstede, G. Cultures and Organizations: Software of the mind. New York, NY: McGraw Hill; 1997.
- Institute of Medicine (U.S.) Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care. Smedley BD, Stith AY, Nelson AR. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. Washington (DC): National Academies Press (US); 2003.
- S. Department of Health and Human Services, The Office of Minority Health. What is Cultural Competency? Accessed December 5, 2020 from http://www.infanthearing.org/coordinator_toolkit/section9/36_cultural_competency.pdf#:~:text=US%20Department%20of%20Health%20and%20Human%20Services%2C%20The,professionals%20that%20enables%20effective%20work%20in%20cross-cultural%20situations.
- Robinson R. Community development model for public health applications: overview of a model to eliminate population disparities. Health Prom Pract. 2005;6(3):338-46.
- Agency for Healthcare Research and Quality. Race, Ethnicity, and Language Data: Standardization for Health Care Quality Improvement. Accessed December 5, 2020 from https://www.ahrq.gov/research/findings/final-reports/iomracereport/reldata1.html.
- Carter-Pokras O, Baquet C. What is a “health disparity”? Public Health Rep. 2002;20:426-34.
- Office of Disease Prevention and Health Promotion. Social Determinants of Health. Accessed December 5, 2020 from https://www.healthypeople.gov/2020/topics-objectives/topic/social-determinants-of-health.
- Tervalon M, Murray-Garcia J. Cultural humility versus cultural competence: a critical discussion in defining physician training outcomes in multicultural education. J Health Care Poor Underserved.1998;9:117-24.
- National Alliance for Hispanic/Latino Health. A Primer for Cultural Proficiency: Towards Quality Health Care Services for Hispanic/Latinos. Washington, DC: National Alliance for Hispanic/Latino Health; 2001.
- S. Census Bureau Quick Facts United States. Accessed December 5, 2020 from https://www.census.gov/quickfacts/fact/dashboard/US/AGE775219.
- New Report from the Pew Forum on Religion & Public Life Finds Religion in U.S. is Non-Dogmatic, Diverse and Politically Relevant. Accessed December 5, 2020 from https://www.pewtrusts.org/en/about/news-room/press-releases-and-statements/2008/06/23/new-report-from-the-pew-forum-on-religion-public-life-finds-religion-in-us-is-nondogmatic-diverse-and-politically-relevant#:~:text=The%20Pew%20Forum%20on%20Religion%20%26%20Public%20Life,which%20is%20funded%20by%20The%20Pew%20Charitable%20Trusts.
- The United States Census Bureau. 2017 National Population Projections Tables: Main Series. Accessed December 5, 2020 from https://www.census.gov/data/tables/2017/demo/popproj/2017-summary-tables.html.
- Deitrick L, Paxton H, Rivera A, et al. Understanding the role of the promotora in a Latino diabetes education program. Qual Health Res. 2010;20(3):386-99.
- Divi C, Koss R, Schmaltz S, Loeb J. Language proficiency and adverse events in US hospitals: a pilot study. Int J Qual Health Care. 2007;19(2):60-7.
- Brach C, Fraser I. Reducing disparities through culturally competent health care: an analysis of the business case. Qual Manag Health Care. 2002;10(4):15-28.
- The Doctors Company. Challenges of Cultural Diversity in Healthcare: Protect Your Patients and Yourself. Accessed December 6. 2020 from https://www.thedoctors.com/articles/challenges-of-cultural-diversity-in-healthcare-protect-your-patients-and-yourself/.
- Brach C, Fraser I. Can cultural competency reduce racial and ethnic health disparities? A review and conceptual model. Med Care Res Rev. 2000;57:181-220.
- S. Department of Justice. Overview of Title VI of the Civil Rights Act of 1964. Accessed December 6, 2020 from https://www.justice.gov/crt/fcs/TitleVI-Overview.
- Limited English Proficiency (LEP.gov). Executive Order 13166. Accessed December 6, 2020 from https://www.lep.gov/executive-order-13166.
- Shah MB, King S, Patel A. Intercultural disposition and communication competence of future pharmacists. Am J Pharm Educ. 2004;68(5):111-12.
- S. Department of Health and Human Services. National Standards for Culturally and Linguistically Appropriate Services (CLAS) in Health and Health Care. Accessed December 6, 2020 from https://thinkculturalhealth.hhs.gov/assets/pdfs/EnhancedNationalCLASStandards.pdf.
- The Joint Commission. Advancing Effective Communication, Cultural Competence, Patient- and Family- Centered Care. A Roadmap for Hospitals. Accessed December 6, 2020 from https://www.jointcommission.org/-/media/tjc/documents/resources/patient-safety-topics/health-equity/aroadmapforhospitalsfinalversion727pdf.pdf?db=web&hash=AC3AC4BED1D973713C2CA6B2E5ACD01B.
- S. Department of Health and Human Services. Tracking CLAS. Accessed December 6, 202 from https://thinkculturalhealth.hhs.gov/clas/clas-tracking-map.
- American Pharmacist Association. Code of Ethics. Accessed December 6, 2020 from https://www.pharmacist.com/code-ethics.
- American Pharmacist Association. Oath of a Pharmacist. Accessed December 6, 2020 from https://www.pharmacist.com/oath-pharmacist.
- Cross, T. Bazron B, Dennis K, Isaacs M. Towards a Culturally Competent System of Care. CASSP Technical Assistance Center, Georgetown University Child Development Center. Accessed December 7, 2020 from https://spu.edu/~/media/academics/school-of-education/Cultural%20Diversity/Towards%20a%20Culturally%20Competent%20System%20of%20Care%20Abridged.ashx.
- Campinha-Bacote J. The process of cultural competence in the delivery of healthcare services: a model of care. J Transcult Nurs. 2002;13(3):181-4.
- Purnell L. The Purnell model for cultural competence. J Multi Nurs Health. 2005;11(2):7-15.
- S. Department of Health and Human Services. Transforming the Face of Health Professions through Cultural and Linguistic Competence Education: The Role of the HRSA Centers of Excellence. Accessed December 8, 2020 from https://www.hrsa.gov/sites/default/files/culturalcompetence/cultcompedu.pdf.
- Spector, R. Cultural Diversity in Health and Illness, 4th ed. Stamford, CT: Appleton & Lange; 1996.
- Zweber A. Cultural competence in pharmacy practice. Am J Pharm Educ. 2002;66:172-76.
- Clay, R. How Do I become more culturally competent? Grad Psych Mag. 2010;9(24).
- Institute of Medicine Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. Washington, DC: National Academy Press; 2002.
- Mueller P, Plevak D, Rummans T. Religious involvement, spirituality, and medicine: implications for clinical practice. Mayo Clinic Proceedings. 2001;76(12):125-35.
- Anita C, MA, Sargent C. Blending Western biomedicine with local healing practice. AMA J Ethics. 2016;18(7):691-97.
- World Economic Forum. The Impact of Making Eye Contact Around the World. Accessed December 9, 2020 from https://www.weforum.org/agenda/2015/02/the-impact-of-making-eye-contact-around-the-world/.
Back to Top