
Expired activity
Please go to the PowerPak
homepage and select a course.
INTRODUCTION
Fibrodysplasia ossificans progressiva (FOP) is an ultra-rare disease, with an estimated prevalence of 1 per 2 million worldwide. It is characterized by disabling impairments due to abnormal bone deposition and by a substantially shortened lifespan in the range of 40 to 55 years.1-4 Similar to treatments for many other rare and ultra-rare disorders, available therapies for FOP have typically focused on providing supportive care for presenting symptoms. With initiatives and incentives for developing drugs for rare diseases, new therapies are on the horizon for FOP. These therapies include palovarotene, garetosmab, and rapamycin. This activity will provide an overview of FOP, introduce potential new therapies, and identify managed care considerations for treatment of this ultra-rare disorder.
What Is FOP?
Definition and Epidemiology of FOP
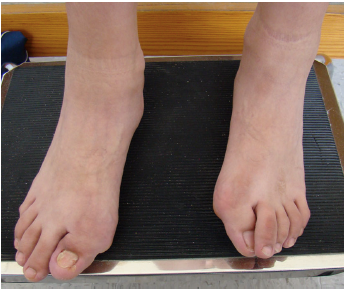
FOP is an autosomal dominant genetic disorder of abnormal bone deposition. Hallmarks of FOP include congenital malformation of the great toes and transformation of fibrous and connective tissues (muscle, ligaments, tendons, fascia) into bone, forming heterotopic ossification (HO; see Table5 and Figure 12). HO may be spontaneous or in response to minor (e.g., intramuscular injections, contusions, etc.) or major physical trauma.2,3,5 FOP is also associated with episodic flare-ups of pain, soft tissue swelling, stiffness, and decreased mobility usually heralding the new formation of HO.2,3,6 As the disease progresses and restrictions in mobility due to HO mount, people with FOP typically experience substantial declines in the physical aspects of quality of life.2 As physical abilities decline, an escalating variety of self-care and mobility devices (reachers, canes, walkers, etc.) are necessary to maintain function. Powered wheeled mobility is common by age 30 years.3,7,9 Ultimately, FOP results in a shortened lifespan (approximately 40-55 years) for which cardiorespiratory failure secondary to thoracic insufficiency syndrome is a common cause of mortality.1,4
| Table. Common Features Exhibited in People With FOP5 |
| Feature |
% of People with Feature |
| Heterotopic ossification |
≈100% |
| Inflammatory soft-tissue swellings |
≈100% |
| Bilateral congenital hallux valgus malformations |
>97% |
| Osteochondromas |
≈90% |
| Cervical spine fusions |
≈80% |
| Short, broad femoral neck |
≈70% |
| Scoliosis |
≈65% |
| Thumb malformations |
≈50% |
| Scalp nodules |
≈40% |
| FOP=fibrodysplasia ossificans progressiva. |
| Figure 1. Examples of Great Toe Malformations in People With FOP2 |
 |
Reproduced with permission of copyright holder
FOP=fibrodysplasia ossificans progressiva. |
Considered an ultra-rare disease, there are an estimated 800 confirmed cases of FOP worldwide.3 Although there is a dearth of detailed epidemiological data on FOP due at least in part to its rarity, studies from various countries suggest a lack of predisposition for FOP based on racial, ethnic, or geographic factors.8,9 Basic research into the pathophysiology of FOP has led to an understanding of the genetic basis of the disease. With that understanding, molecular targets for pharmacologic interventions have been identified and new agents are on the horizon for the treatment of FOP.10,11
Flare-ups and Long-term Patient Impact
In one of the more comprehensive descriptions of FOP flare-ups on an international scope, Pignolo et al described the natural history of FOP, which built upon prior smaller natural history studies.6 A large majority (approximately 71%) of the 500 respondents reported having a flare-up in the preceding 12 months with an average of 1.9 ± 0.1 flare-ups in that timeframe.6 Respondents described the primary symptoms of flare-ups as pain, swelling, decreased mobility, and stiffness, and most respondents (72%) confirmed flare-up episodes within 2 days.6 Flare-ups were attributed to injury, viral infection, or overuse, as well as intramuscular vaccinations that led to ossification in more than 80% of such subjects.6 The site of the flare-up affected the amount of pain, swelling, and disability experienced by patients. Flare-ups in the hips, knees, and back produced the most pain, and the greatest swelling was reported in flare-ups of the back, knees, and neck. Flare-ups negatively impacted movement and overall function in approximately 70% of patients; the most disabling locations were the shoulders, hips, neck, and back.6 Approximately 47% of patients reported progression without flare-ups, thus flare-up symptoms did not need to be present for disease progression to be observed.6 In another natural history study of the disease, progression of FOP, defined by the formation of HO, resulted in substantial decreases in joint mobility and physical function.3 Ultimately, ossification restricts the normal expansion of the rib cage, which can lead to cardiorespiratory failure at a young age.1 Describing the clinical details of the disease is necessary to perform objective analyses of treatments. The subjective perspective of a disease can also provide important insights. In that vein, 2 people with FOP shared their perspectives on the disease with personal essays that clinicians may find informative and inspiring (Sidebar).12
Patient Perspectives on Living With FOP
“FOP has given me an extra appreciation for the little things in life, because the little things are what FOP has gradually taken away from me behind the scenes. Things like getting myself in or out of a chair, dressing myself, running around with friends, exercising, walking up or down stairs, taking a taxi or hitching a ride with a friend are all things that I've had to let go of being able to do. It's crazy to deal with something as volatile as FOP and not lose yourself along the way, but I've always said that FOP is part of what I am, but no part of who I am.” – Ian L. Cali12
“My life was falling apart at the seams. Nothing was stopping this monster raging inside of me. My life as I knew it was changed forever. This not only affected me, but my family as well. Life was now different. I went from mostly independent to becoming dependent on others for all activities of daily living. . . . With the help of my family I learned that FOP may have forced me to do things completely differently, but it did not take my family . . . I learned life was definitely not going to be easy. A lot of changes were made but this was our life now and we were going to do everything in our power to make it a good one.” – Laura Rossano12
|
Genetic Cause of FOP
FOP has a clear genetic basis identified as a heterozygous mutation of the gene coding for the activin A receptor type I (ACVR1).13 A specific mutation (c.617G>A; p.R206H) of the ACVR1 gene has been observed in patients with classical presentation of FOP.13 The resulting mutation of the ACVR1 protein results in overactivity of the receptor, which leads to FOP’s hallmark presentation of bone formation.5,8,13 In particular, the ACVR1 mutations found in FOP alter the function of the protein, activin A, transforming it from an ACVR1 antagonist to an agonist. Through a biochemical cascade, this transformation results in the unregulated HO observed in FOP.5,8,11,13
Diagnosis
Because FOP is so very rare, misdiagnosis is common. Up to 90% of people with FOP experience misdiagnosis, sometimes with devastating consequences.14 For example, diagnostic procedures, particularly biopsies, can precipitate regional or even widespread HO and result in disabling postural abnormalities and the loss of range of motion and mobility.14 Early recognition of the clinical hallmarks of FOP can spare affected individuals the harms associated with the uncertainty of missed and delayed diagnosis and the morbidity that often results from unnecessary procedures.
Typical clinical features
One of the more prominent and identifiable features of FOP is congenital malformation of the great toes.6,14,15 In addition, soft tissue swellings, which may resemble tumors (and lead to misdiagnosis), are often present.14,15 The presence of both features (malformed great toe and soft tissue nodules) should lead to the differential diagnosis of FOP, particularly if additional evidence, such as ossification at immunization sites, is present.14,15 Typically, HO initially manifests in the upper back and neck and later affects the trunk and limbs. The usual pattern of progression is from cranial to caudal, axial to appendicular, and proximal to distal. Eventually, HO deposition fuses the axial skeletal segments and spans joints to form an extensive network of extra-skeletal bone that causes a near total immobilization of the body.5
Importance of genetic testing
With the risk of misdiagnoses potentially causing permanent disabilities, genetic testing to confirm the diagnosis of FOP is important. All people with FOP will have a mutation in the ACVR1 gene.9 In individuals with the classic presentation of FOP (i.e., congenital malformation of the big toe, progressive HO), a particular mutation (c.617G>A; p.R206H) will be present; other mutations are possible with different FOP presentations.13 As an autosomal dominant genetic disease, FOP can be inherited from the mother or father; the likelihood that a child inherits the condition from a parent with FOP is 50%.16 With the substantial impact of FOP on those who inherit the condition, as well as the potentially life-threatening risks to women with FOP who become pregnant,16 genetic counseling should be considered.5,9 As outlined by Pignolo et al, risks to pregnant women with FOP include FOP flare-ups; breathing difficulties, particularly during later stages of pregnancy; general anesthesia for typically necessary Caesarian delivery; phlebitis and pulmonary embolism; and typical childbirth complications that also may affect pregnant women without FOP.16
Standard of Care for FOP: Preventing Flare-ups and Managing Quality of Life
Preventing Trauma
Because trauma can induce flare-ups and HO, measures to prevent trauma should be implemented to reduce risk. Although complete prevention of trauma may not be possible, vigilance is crucial to avoid the risk of physical trauma, because even a minor injury can trigger flare-ups.9,16 Safety measures may include home modification, using ambulatory assistance devices, and wearing protective headgear.9 Passive range of motion activities (i.e., when another person performs the motion for the person with FOP) should be avoided.9,16 Lower impact activities, such as exercises and activities conducted in water are recommended.9 Of particular importance is the avoidance of intramuscular injections, which are known to precipitate HO episodes.9,16 When administering dental care, special strategies should be employed to avoid overstretching the jaw.9,16 Attempts to surgically remove nodules and HO sites must also be avoided because such surgical procedures are likely to induce rampant new bone deposition.9,16
Managing Trauma When It Occurs
Any fall or soft tissue trauma can precipitate HO and worsen symptoms. Even when preventive measures are implemented, some incidental trauma will still occur in the course of daily life. Any fall by a person with FOP should be treated with prompt medical attention, and any trauma that involves head or neck injury should be considered a serious health issue until shown otherwise. When a soft-tissue injury occurs or in preparation for necessary surgery, a course of corticosteroids is often prescribed. A typical course of therapy would be prednisone 1 to 2 mg/kg/d as a single daily dose for a maximum of 4 days.9 Clinicians should note that using high-dose corticosteroids for trauma in FOP as a standard of care is based on expert opinion rather than clinical trials.
Optimizing Function and Improving Quality of Life
Quantitative data on quality-of-life issues in people with FOP are limited due to the extremely low incidence rate.2,7 Two available studies, each with a very small number of subjects (8 and 15), suggest that decreases in daily living function correspond with decreases in quality-of-life measures.2,7 People with FOP typically benefit from strategies to optimize function with possible improvement of quality of life. Optimizing available range of motion, mobility, and respiratory function are important considerations when managing FOP and are similar to strategies used to prevent trauma. Strategies to improve/maintain respiratory function, such as singing, swimming, and incentive spirometry, may be employed in efforts to manage thoracic insufficiency syndrome and other respiratory issues.5
Standard of Care for FOP: Managing Symptoms
In the International Clinical Council on FOP report on current treatment strategies for FOP, pharmacologic treatments are designated in 3 classes.9 Class I drugs are used to control symptoms associated with FOP flare-ups and include the corticosteroid, prednisone; the nonsteroidal anti-inflammatory drugs (NSAIDs), ibuprofen and indomethacin; and the cyclooxygenase-2 inhibitor, celecoxib. Class I drugs focus on decreasing inflammation associated with flare-ups. The recommended pharmacologic treatment of flare-ups is to initiate prednisone within 24 hours of the onset of flare-up at 2 mg/kg/d (≤100 mg/d) for 4 days. A course of NSAID or celecoxib would follow the discontinuation of prednisone. Prednisone should generally not be used for flare-ups on the chest or trunk because it is difficult to judge the exact onset of a new flare-up. Although prednisone may be effective initially, flare-ups in these locations are often relentless and severe rebound may ensue when prednisone is tapered and stopped. Many patients have tragically become steroid dependent from such use (F. Kaplan, personal communication, January 11, 2021).9 Class II drugs are those that are approved for non-FOP indications but are believed to have benefit for some of the symptoms associated with FOP (i.e., off-label use). Class II drugs include the leukotriene receptor antagonist, montelukast; the mast cell stabilizer, cromolyn; the aminobisphosphonates, pamidronate and zoledronate; and the selective tyrosine kinase inhibitor, imatinib.9,17 Class III drugs are those under investigation in clinical trials such as palovarotene, garetosmab, saracatinib, and rapamycin (discussed in more detail in the following section). Clinicians should note that clinical trials of palovarotene and garetosmab have previously been paused based on safety concerns. The concerns for garetosmab are more serious because fatal adverse reactions were observed in the phase 2 LUMINA-1 trial.18 For palovarotene, the US Food and Drug Administration (FDA) placed partial clinical holds for pediatric patients in 2 clinical trials of the drug due to apparent early growth plate closure in some patients.19 Rapamycin (or sirolimus) is an immunosuppressant currently approved for use to prevent organ rejection in renal transplant and for the treatment of lymphangioleiomyomatosis.20 Most recently, a phase 2 clinical trial of rapamycin opened in Japan based on research conducted on induced pluripotent stems cells obtained from people with FOP.10
Rehabilitation Considerations
Independence can be preserved and restored with the thoughtful assistance of a rehabilitation team. Team members include physiatrists; occupational, speech language, and physical therapists; orthotists; seating and positioning specialists; rehabilitation engineers; and other specialists. Compensatory approaches can go a long way to preserving function. Strategies and equipment to ease the challenges of dressing include avoidance of clothing with button or zipper closures in favor of pull-on garments, elastic waistbands, and Velcro closures. Sock donners, elastic shoelaces, and long-handled shoehorns and modified reachers are often helpful. Raised toilet seats, custom-angled commodes, bedside urinals, and bidets all enable toileting. Home modifications include widened doorways, tub and bath benches (which may be customized), grab bars, ramps, and manual and power lifts. Personal hygiene and grooming may necessitate long-handled sponges, combs, electric toothbrushes, water pics, and oral suction devices. Dining and meal preparation may be facilitated by electrical can and jar openers, cutting boards with spikes to hold food while it is prepared or cut, long-handled eating utensils and straws, and rotating shelves (e.g., lazy Susans). To facilitate sleep and ensure skin integrity, specialized mattresses and overlays may be used to redistribute pressure and tilt table beds that rotate from vertical to horizontal for pressure relief may be employed.9,21,22 Ambulatory devices such as canes, walkers, crutches, and/or custom shoes and inserts are essential aids for walking. For more severe limitations, power wheelchairs outfitted with customized seating and functions (i.e., power seat elevation, anterior and posterior tilt and recline) are often required. Lap trays with computer mounts allow participation in work, school, and social engagements. Environmental control units (which may be integrated as computer and phone applications) operate appliances, lights, doors, and televisions.9,21,22 Vans may be customized to allow individuals with FOP to safely travel while seated in their power chairs.
Sexuality is a healthy part of human interaction. Because of their unusual and inflexible postures, individuals with FOP may require the assistance of carefully placed pillows and bolsters as well as gentle approaches to guard against incidental physical trauma. Discussion of contraception and genetic counseling are appropriate.5,9 Recreational therapists may be helpful in making meaningful use of leisure time. Psychologists, social workers, and other mental health specialists can help affected individuals and family members adjust to the limitations and inconveniences imposed by FOP. Creative arts therapies (e.g., art therapy, music therapy, dance/movement therapy, drama therapy, poetry therapy) use arts-based methods and creative processes to ameliorate disability and illness and to optimize health and wellness. Early vocational planning is warranted.9
Aquatic therapy (warm water hydrotherapy) allows individuals to perform active range of motion, cardiopulmonary, and even resistive exercise in safe, low-impact environments. Warm water may provide pain relief. Modified lifts, elevators, or ramps may be necessary to enter and exit the pool.9,22 Anecdotal reports suggest that acetic acid iontophoresis may help restore some lost temporomandibular joint range of motion in FOP.9,22 Hearing impairment is common in FOP, possibly due to HO of the auditory ossicles. Children with FOP should have their hearing tested every other year, and hearing aids should be prescribed as indicated.9,23
Emerging Treatments for FOP
Progress in research on the underlying etiology and pathophysiology of FOP has accelerated drug development efforts. Those efforts have resulted in potential pharmacologic treatments for FOP that are in phase 2 or phase 3 clinical trials: palovarotene, garetosmab, rapamycin, and saracatinib. As outlined in Figure 2, the current understanding is that the biomolecular mechanisms of FOP result from gain-of-function mutations in ACVR1 that increase receptor activity and lead to chondrogenesis and HO.10 Emerging treatments for FOP focus on targets upstream (rapamycin, garetosmab) or downstream (palovarotene, saracatinib) from ACVR1 (Figure 2).10
| Figure 2. Overview of Biochemical Cascade Leading to HO in FOP and Targets for Current and Emerging FOP Drugs10 |
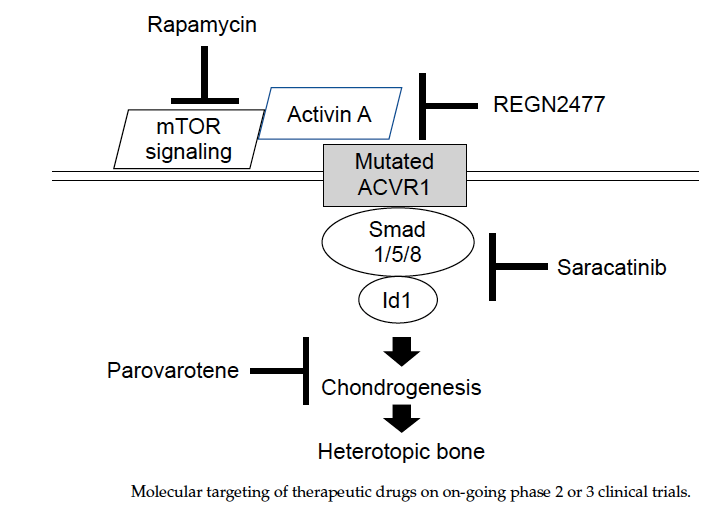 |
Reproduced with permission of copyright holder
ACVR1=activin A receptor type I; FOP=fibrodysplasia ossificans progressiva; HO=heterotopic ossification; mTOR=mechanistic target of rapamycin; REGN2477=garetosmab. |
Palovarotene
Palovarotene, a retinoic acid receptor (RAR)-γ agonist, has been previously investigated in clinical trials for the treatment of emphysema and was well tolerated in the study subjects, although not efficacious for emphysema.24 Through activation of RAR-γ, palovarotene inhibits chondrogenesis.10 With demonstrated effectiveness in animal models of FOP,25 palovarotene became a drug candidate for FOP. Preliminary results in a phase 2 study with 40 participants suggest that palovarotene may reduce the incidence of HO and the volume of new HO after flare-up without major adverse events (AEs).26 Given the extremely limited number of people with FOP worldwide, there has been a limited number of clinical trials and a limited number of participants in those trials. Case studies, therefore, may provide additional context for the clinical use of various agents in FOP. As of the writing of this monograph, 1 case report has been published with 1 patient in whom palovarotene was administered after orthopedic surgeries and minimal AEs were noted.27 As noted above, the FDA placed a clinical hold on pediatric dosing of palovarotene in an ongoing clinical trial following observations of early growth plate closure.19 Dosing was reinitiated in patients aged 14 years or older in March 2020.28 Investigators are considering the AE profiles of other RAR agonists and looking for the possibility of mucocutaneous toxicity, dry skin, and pancreatitis, among others possible side effects.10
REGN2477 (Garetosmab)
In FOP, mutations in the ACVR1 receptor transform the activity of the protein, activin A, from an antagonist to an agonist, which results in HO. Garetosmab, a fully human monoclonal antibody, targets activin A to halt the signaling cascade leading to HO.11,29 A phase 1 study of garetosmab in 40 women examined the pharmacokinetics at 4 intravenous doses and 1 subcutaneous dose. The study found dose-proportional increases in peak concentrations and no safety concerns were observed.29 Early results from the LUMINA-1 phase 2 trial with 44 participants were announced by the manufacturer in early 2020. The reported results included an approximate 25% decrease in new and existing bone lesions and an approximate 90% decrease in new lesions when comparing the garetosmab with placebo.30 To date (January 2021), the phase 2 results have not been presented at a medical conference or in a peer-reviewed publication. In October 2020, the manufacturer paused phase 2 of the LUMINA-1 trial after fatalities were reported in the open-label portion of the study in which all participants received the drug. No deaths were reported in the preceding 28-week double-blind portion of the study.18 The drug remains listed as an ongoing effort in the manufacturer’s pipeline as of January 2021.31
Rapamycin
The mechanistic target of rapamycin (mTOR) signaling pathway appears to be upregulated in FOP and the immunosuppressant, rapamycin, which inhibits mTOR1 kinase, was found to be effective in animal models of FOP.10 As an approved drug, there is a well-known history of use of rapamycin in humans and a corresponding knowledge of potential AEs.20 Rapamycin has been the focus of a phase 2 study in Japan that is similar to other FOP studies with an initial double-blind portion followed by an open-label portion in which all participants received the drug.10 A case study of 2 patients was recently published in which 1 patient received rapamycin on an acute, compassionate use basis and the other patient received rapamycin on a chronic basis following organ transplantation. Progression of FOP was observed in both patients although a range of reasons besides lack of efficacy could contribute to the case results.32 An abundance of caution, therefore, is necessary when interpreting case studies, particularly given the limited number of such studies, the limited number of patients, and the lack of control in the studies.
Other Emerging Therapeutics
As the molecular mechanisms underlying the pathology of FOP are elucidated, additional therapeutic approaches are expected and could include repurposing currently approved or investigational drugs as potential therapeutics in FOP.11 One investigational drug, saracatinib, which was found to be effective in animal models of FOP, recently advanced as the focus of a phase 2A study.10 The compound was previously studied as a cancer treatment and is also being considered as a potential treatment for other diseases such as Parkinson disease and idiopathic pulmonary fibrosis.33,34 Similar to rapamycin mentioned above, using an approved drug for a new indication has benefits with respect to drug development costs and knowledge of AEs. As another example, imatinib, a tyrosine kinase inhibitor with indications for a variety of leukemias, other cancers, and other conditions,35 was recently the subject of a report involving 7 pediatric cases of FOP.17 The drug appeared to be well-tolerated in those patients and appeared to reduce flare-up intensity in the participants.17 Again, as with other case reports, although the small number of participants and lack of placebo control limit the conclusions that can be made from the results, the studies point to a need for further investigation.
Managed Care Perspectives on Novel Therapeutics for Rare Diseases
The costs of prescription drugs continues to rise and to require greater proportions of healthcare spending.36,37 Concerns about the cost of prescription drugs have existed for many years, and those concerns are shared by the general public, governments, and health insurance companies.38,39 The National Health Expenditure Data from the Centers for Medicare & Medicaid Services reported that 2019 prescription drug spending in the United States was $369.7 billion, which was an increase of 5.7% compared with 2018,36 and a report by the IQVIA Institute for Human Data Science estimated that drug spending will increase to $405 to $435 billion in 2023.37 Although these numbers only briefly encapsulate the complicated issue of drug costs, they provide a framework to understand how much is being spent each year.
Prescription drug costs may be even more of a concern with specialty drugs (including those for rare and ultra-rare diseases), which account for many of the top 10 most expensive drugs in the United States and worldwide.40,41 At least part of the high cost of specialty drugs can be attributed to orphan drug legislation, which has provided manufacturers with financial incentives (e.g., extended market exclusivity) to develop drugs to treat rare and ultra-rare diseases.42 In the United States, some of the incentives provided by the Orphan Drug Act of 1983 are 7 years of market exclusivity, tax credits of up to 50% for research and development costs, and a grants program to support clinical trials.43 The typical managed care analysis of drugs for inclusion in formulary, therefore, may be skewed when considering treatments for rare and ultra-rare diseases due to the low prevalence of the diseases and the typically high costs of treatments (including ancillary care). Furthermore, as with other drugs, payers need to evaluate available clinical trial data in the target population along with any cost-effectiveness data. Payers may claim that a single patient with a rare or ultra-rare condition can dramatically negatively impact their budgets. When managed care organizations consider novel therapeutics for rare diseases, the financial effects on patients and their families/caregivers should not be overlooked because coverage for the drugs can be a major obstacle for patients.44-46 Alternative perspectives suggest that overall spending on orphan drugs has stabilized over recent years and the overall impact on payers’ budgets may not be substantial.47,48 Divino et al determined that spending on orphan drugs (in 2014 dollars) rose from $15 billion in 2007 to $30 billion in 2013, which amounted to 4.8% and 8.9% of total drug spending in those years, respectively.47 In the 2018 report on orphan drugs from the IQVIA Institute for Human Data Science, Aitken and Kleinrock describe how orphan drugs accounted for 9.6% of total drug sales in 2017.48 As detailed in the report, analysis of spending on orphan drugs should consider that some orphan drugs have non-orphan indications.48
Meeting patients’ needs and ensuring patient access to orphan drugs are also important considerations. Even with the establishment of orphan drug programs and more comprehensive healthcare coverage, patients in Europe with rare and ultra-rare diseases may not have access to these medicines,49 thus, ensuring innovation in orphan drug development while guaranteeing patient access may warrant alternative approaches to current policies.50,51 Those approaches may include increased involvement of patient advocacy groups and nonprofit organizations, price negotiations, patent reform, and new legislation while also focusing on improving patient access.49,50,52 As can be seen, the appropriate pricing of orphan drugs will continue to be an issue of discussion.50,51 Whether or not major changes in policies occur in the near future, managed care organizations must work within current frameworks with the goal to provide optimal care to patients without burdening those patients with overbearing costs, all while keeping an eye on future trends in the changing healthcare landscape.
Specific peer-reviewed data on the financial impact of FOP is not readily available because an extraordinarily limited number of people and families are affected. In an FDA Listening Session on FOP, patients and families shared their experiences, including the impact on daily and family activities as well as the economic burden.53 One family described the need to find a job with sufficient flexibility to take a child with FOP on multiple trips per week to up to 10 specialists. Other families described the challenges of structuring daily family time around assisting their family member with typically routine activities such as getting dressed, using the bathroom, and repositioning their children throughout the night at 2-hour intervals.53 It is reasonable to infer that the financial ramifications (including direct and indirect costs) of FOP on patients and their families are substantial based on the financial impact from other rare and ultra-rare diseases.54,55
CONCLUSION
Currently, FOP is an ultra-rare condition without effective medical therapies to slow or halt the progression of the disease. Symptom management focuses on supportive care for individuals with FOP, including rehabilitation and drugs to treat flare-ups. Research on the pathophysiology of FOP has led to several potential therapies—palovarotene, garetosmab, rapamycin, saracatinib— which are in various stages of clinical trials. Managed care considerations for the treatment of FOP and other rare and ultra-rare diseases include a range of factors such as patient access to medications, cost of therapy, efficacy, and cost-effectiveness.
REFERENCES
- Kaplan FS, Zasloff MA, Kitterman JA, et al. Early mortality and cardiorespiratory failure in patients with fibrodysplasia ossificans progressiva. J Bone Joint Surg Am. 2010;92(3):686-691. doi:10.2106/JBJS.I.00705
- Ortiz-Agapito F, Colmenares-Bonilla D. Quality of life of patients with fibrodysplasia ossificans progressiva. J Child Orthop. 2015;9(6):489-493. doi:10.1007/s11832-015-0704-6
- Pignolo RJ, Baujat G, Brown MA, et al. Natural history of fibrodysplasia ossificans progressiva: cross-sectional analysis of annotated baseline phenotypes. Orphanet J Rare Dis. 2019;14(1):98. doi:10.1186/s13023-019-1068-7
- Gencer-Atalay K, Ozturk EC, Yagci I, et al. Challenges in the treatment of fibrodysplasia ossificans progressiva. Rheumatol Int. 2019;39(3):569-576. doi:10.1007/s00296-018-4179-x
- Akesson LS, Savarirayan R. Fibrodysplasia ossificans progressiva. In: Adam MP, Ardinger HH, Pagon RA, et al, eds. GeneReviews®. University of Washington, Seattle. June 11, 2020. Accessed December 3, 2020. https://www.ncbi.nlm.nih.gov/books/NBK558090
- Pignolo RJ, Bedford-Gay C, Liljesthröm M, et al. The natural history of flare-ups in fibrodysplasia ossificans progressiva (FOP): a comprehensive global assessment. J Bone Miner Res. 2016;31(3):650-656. doi:10.1002/jbmr.2728
- Nakahara Y, Kitoh H, Nakashima Y, et al. Longitudinal study of the activities of daily living and quality of life in Japanese patients with fibrodysplasia ossificans progressiva. Disabil Rehabil. 2019;41(6):699-704. doi:10.1080/09638288.2017.1405083
- Faruqi T, Dhawan N, Bahl J, et al. Molecular, phenotypic aspects and therapeutic horizons of rare genetic bone disorders. Biomed Res Int. 2014;2014:670842. doi:10.1155/2014/670842
- Kaplan FS, Al Mukaddam M, et al. The medical management of fibrodysplasia ossificans progressiva: current treatment considerations. Proc Intl Clin Council FOP. 2019;1:1-111. Accessed February 9, 2021. https://d3n8a8pro7vhmx.cloudfront.net/ifopa/pages/212/attachments/original/1559059247/FOP_TREATMENT_GUIDELINES_June_2019.pdf?1559059247
- Kitoh H. Clinical aspects and current therapeutic approaches for FOP. Biomedicines. 2020;8(9):325. doi:10.3390/biomedicines8090325
- Cappato S, Giacopelli F, Ravazzolo R, Bocciardi R. The horizon of a therapy for rare genetic diseases: a “druggable” future for fibrodysplasia ossificans progressiva. Int J Mol Sci. 2018;19(4):989. doi:10.3390/ijms19040989
- Cali IL, Rossano L. Fibrodysplasia ossificans progressiva: the patient voice. Bone. 2018;109:291-294. doi:10.1016/j.bone.2017.05.017
- Kaplan FS, Xu M, Seemann P, et al. Classic and atypical fibrodysplasia ossificans progressiva (FOP) phenotypes are caused by mutations in the bone morphogenetic protein (BMP) type I receptor ACVR1. Hum Mutat. 2009;30(3):379-390. doi:10.1002/humu.20868
- Kitterman JA, Kantanie S, Rocke DM, Kaplan FS. Iatrogenic harm caused by diagnostic errors in fibrodysplasia ossificans progressiva. Pediatrics. 2005;116(5):e654-e661. doi:10.1542/peds.2005-0469
- Kaplan FS, Xu M, Glaser DL, et al. Early diagnosis of fibrodysplasia ossificans progressiva. Pediatrics. 2008;121(5)e1295-e1300. doi:10.1542/peds.2007-1980
- Pignolo RJ, Shore EM, Kaplan FS. Fibrodysplasia ossificans progressiva: clinical and genetic aspects. Orphanet J Rare Dis. 2011;6:80. doi:10.1186/1750-1172-6-80
- Kaplan FS, Andolina JR, Adamson PC, et al. Early clinical observations on the use of imatinib mesylate in FOP: a report of seven cases. Bone. 2018;109:276-280. doi:10.1016/j.bone.2017.07.019
- Regeneron provides update on the garetosmab phase 2 LUMINA-1 Trial in fibrodysplasia ossificans progressiva (FOP). News release. Regeneron; October 30, 2020. Accessed January 1, 2021. https://investor.regeneron.com/static-files/d920a235-a4d4-411c-bd6d-fa2be52e0b5c
- Ipsen initiates partial clinical hold for palovarotene IND120181 and IND135403 studies. News release. Ipsen; December 6, 2019. Accessed February 11, 2021. https://www.ipsen.com/press-releases/ipsen-initiates-partial-clinical-hold-for-palovarotene-ind120181-and-ind135403-studies
- Rapamune [package insert]. Philadelphia, PA: Wyeth Pharmaceuticals, Inc; 2017.
- Levy C, Berner TF, Sandhu PS, et al. Mobility challenges and solutions for fibrodysplasia ossificans progressiva. Arch Phys Med Rehabil. 1999;80(10):1349-1353. doi:10.1016/S0003-9993(99)90043-6
- Levy CE, Frasca Berner T, Bendixen R. Rehabilitation for individuals with fibrodysplasia ossificans progressiva. Clin Rev Bone Miner Metab. 2005;3:251-256. doi:10.1385/BMM:3:3-4:251
- Levy CE, Lash AT, Janoff HB, Kaplan FS. Conductive hearing loss in individuals with fibrodysplasia ossificans progressiva. Am J Audiol. 1999;8(1):29-33. doi:10.1044/1059-0889(1999/011)
- Stolk J, Stockley RA, Stoel BC, et al. Randomised controlled trial for emphysema with a selective agonist of the γ-type retinoic acid receptor. Eur Respir J. 2012;40(2):306-312. doi:10.1183/09031936.00161911
- Chakkalakal SA, Uchibe K, Convente MR, et al. Palovarotene inhibits heterotopic ossification and maintains limb mobility and growth in mice with the human ACVR1R206H fibrodysplasia ossificans progressiva (FOP) mutation. J Bone Miner Res. 2016;31(9):1666-1675. doi:10.1002/jbmr.2820
- Kaplan FS, Hsaio EC, Baujat G, et al. Efficacy and safety of palovarotene in fibrodysplasia ossificans progressiva (FOP): a randomized, placebo-controlled, double-blind study [Abstract #FR0334]. Bone Miner Res. 2017;32(suppl 1):S114. doi:10.1002/jbmr.3363
- Singh S, Kidane J, Wentworth KL, et al. Surgical management of bilateral hip fractures in a patient with fibrodysplasia ossificans progressiva treated with the RAR-γagonist palovarotene: a case report. BMC Musculoskelet Disord. 2020;21(1):204. doi:10.1186/s12891-020-03240-2
- Ipsen provides update on palovarotene clinical programs. News release. Ipsen; March 26, 2020. Accessed January 1, 2021. https://www.ipsen.com/press-releases/ipsen-provides-update-on-palovarotene-clinical-programs
- Vanhoutte F, Liang S, Ruddy M, et al. Pharmacokinetics and pharmacodynamics of garetosmab (anti-activin A): results from a first-in-human phase 1 study. J Clin Pharmacol. 2020;60(11):1424-1431. doi:10.1002/jcph.1638
- Regeneron announces encouraging garetosmab phase 2 results in patients with ultra-rare debilitating bone disease. PR Newswire; January 9, 2020. Accessed January 4, 2021. https://www.prnewswire.com/news-releases/regeneron-announces-encouraging-garetosmab-phase-2-results-in-patients-with-ultra-rare-debilitating-bone-disease-300984302.html
- A powerful research and development engine: pipeline. Regeneron; January 27, 2021. Accessed February 10, 2021. https://www.regeneron.com/pipeline
- Kaplan FS, Zeitlin L, Dunn SP, et al. Acute and chronic rapamycin use in patients with fibrodysplasia ossificans progressiva: a report of two cases. Bone. 2018;109:281-284. doi:10.1016/j.bone.2017.12.011
- Therapeutics: saracatinib. Alzforum; October 17, 2019. Accessed January 4, 2021. https://www.alzforum.org/therapeutics/saracatinib
- Parry J. New clinical trial evaluates saracatinib in idiopathic pulmonary fibrosis. Yale School of Medicine; January 13, 2020. Accessed January 4, 2021. https://medicine.yale.edu/news-article/22289
- Gleevec [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corporation; 2020.
- NHE Fact Sheet. Centers for Medicare & Medicaid Services. NHE Fact Sheet; December 16, 2020. Accessed January 4, 2021. https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/NHE-Fact-Sheet
- Aitken M, Kleinrock M. Medicine Use and Spending in the U.S.: A Review of 2018 and Outlook to 2023. Parsippany, NJ: The IQVIA Institute for Human Data Science; 2019. Accessed February 10, 2021. https://www.iqvia.com/insights/the-iqvia-institute/reports/medicine-use-and-spending-in-the-us-a-review-of-2018-and-outlook-to-2023
- Walker J. Patients struggle with high drug prices. The Wall Street Journal. December 31, 2015. Accessed January 4, 2021. https://www.wsj.com/articles/patients-struggle-with-high-drug-prices-1451557981
- High-Priced Drugs: Estimates of Annual Per-Patient Expenditures for 150 Specialty Medications. Washington, DC: American’s Health Insurance Plans; 2016. Accessed February 10, 2021. https://www.ahip.org/report-high-priced-drugs-expenditures
- Anderson LA (reviewer). Specialty drugs: 10 of the most expensive. Drugs.com; October 20, 2019. Accessed January 4, 2021. https://www.drugs.com/slideshow/top-10-most-expensive-drugs-1274
- Chase L. The 10 most expensive drugs in the U.S., period. GoodRx; August 25, 2020. Accessed January 4, 2021. https://www.goodrx.com/blog/most-expensive-drugs-period
- Cremers S, Aronson JK. Drugs for rare disorders. Br J Clin Pharmacol. 2017;83(8):1607-1613. doi:10.1111/bcp.13331
- Orphan Drug Act, Pub L No. 97-414, 96 Stat 2049-2057. Accessed February 10, 2021. https://www.fda.gov/media/99546/download
- Robinson SW, Brantley K, Liow C, Teagarden JR. An early examination of access to select orphan drugs treating rare diseases in health insurance exchange plans. J Manag Care Spec Pharm. 2014;20(10):997-1004. doi:10.18553/jmcp.2014.20.10.997
- Chambers JD, Kim DD, Pope EF, et al. Specialty drug coverage varies across commercial health plans in the US. Health Aff. 2018;37(7):1041-1047. doi:10.1377/hlthaff.2017.1553
- Chambers JD, Panzer AD, Kim DD, et al. Variation in US private health plans’ coverage of orphan drugs. Am J Manag Care. 2019;25(10):508-512.
- Divino V, DeKoven M, Kleinrock M, et al. Orphan drug expenditures in the United States: A historical and prospective analysis, 2007-18. Health Aff (Millwood). 2016;35(9):1588-1594. doi:10.1377/hlthaff.2016.0030
- Aitken M, Kleinrock M. Orphan Drugs in the United States (Part One): Growth Trends in Rare Disease Treatments. The IQVIA Institute for Human Data Science; October 17, 2018. Accessed February 10, 2021. https://www.iqvia.com/insights/the-iqvia-institute/reports/orphan-drugs-in-the-united-states-growth-trends-in-rare-disease-treatments
- Heard JM, Vrinten C, Schlander M, et al. Availability, accessibility and delivery to patients of the 28 orphan medicines approved by the European Medicine Agency for hereditary metabolic diseases in the MetabERN network. Orphanet J Rare Dis. 2020;15(1):3. doi:10.1186/s13023-019-1280-5
- Luzzatto L, Hyry HI, Schieppati A, et al. Outrageous prices of orphan drugs: a call for collaboration. Lancet. 2018;392(10149):791-794. doi:10.1016/S0140-6736(18)31069-9
- Ollendorf DA, Chapman RH, Pearson SD. Evaluating and valuing drugs for rare conditions: no easy answers. Value Health. 2018;21(5):547-552. doi:10.1016/j.jval.2018.01.008
- Cohen JP, Awatin JG. Patient access to orphan drugs. Expert Opin Orphan Drugs. 2017;5(12):923-932. doi:10.1080/21678707.2017.1402676
- FDA listening session on FOP: fibrodysplasia ossificans progressiva (FOP). International Fibrodysplasia Ossificans Progressiva Association; July 23, 2019. Accessed January 11, 2021. Executive summary available at: https://www.ifopa.org/fda_listening_session_on_fop
- Tribble SJ, Lupkin S. Sky-high prices for orphan drugs slam American families and insurers. Kaiser Health News; January 17, 2017. Accessed January 13, 2021. https://khn.org/news/sky-high-prices-for-orphan-drugs-slam-american-families-and-insurers
- Angelis A, Tordrup D, Kanavos P. Socio-economic burden of rare diseases: a systematic review of cost of illness evidence. Health Policy (New York). 2015;119(7):964-979. doi:10.1016/j.healthpol.2014.12.016