
Expired activity
Please go to the PowerPak
homepage and select a course.
An Interprofessional Approach to Managing Multidrug-Resistant Bacterial Infections
I. Overview of MDR GNB and MDR GPB Infections
In 2019, the Centers for Disease Control and Prevention (CDC) published a report, Antibiotic Resistance Threats in the United States, listing and categorizing various types of drug-resistant pathogens.(CDC 2019a) Among the 18 antibiotic resistance threats listed, Gram-negative bacteria (GNB) such as carbapenem-resistant Acinetobacter and carbapenem-resistant Enterobacteriaceae (CRE) were categorized as “Urgent Threats” (require urgent and aggressive action) and extended spectrum beta-lactamase (ESBL) producing Enterobacteriaceae (ESBL-E) and multidrug-resistant (MDR) Pseudomonas aeruginosa (MDR-Pa) categorized as “Serious Threats” (require prompt and sustained action). These four types of drug-resistant infections are among the more common and most devastating infections observed, particularly as hospital-acquired infections, and represent an important area where health care professional education is needed.
- Carbapenem-resistant Acinetobacter: resistance to carbapenems in addition to baseline resistance to many antibiotic classes leaving limited or no antibiotic options.(CDC 2019a)
- Carbapenem-resistant Enterobacteriaceae (CRE): resistance to at least one of the carbapenem antibiotics (ertapenem, meropenem, doripenem, or imipenem) or produces a carbapenemase.(CDC 2019b)
- Extended-spectrum beta-lactamase-producing Enterobacteriaceae (ESBL-E): resistance via a group of enzymes that hydrolyze penicillins and extended spectrum/third generation cephalosporins (e.g., ceftriaxone), and aztreonam.(Paterson 2005)
- Multidrug-resistant Pseudomonas aeruginosa (MDR Pa): resistance to at least one agent in at least three antibiotic classes.(Magiorakos 2012)
According to the report, Antibiotic Resistance Threats in the United States (CDC 2019a), among 18 antibiotic resistance threats listed, many include Gram-positive bacteria (GPB) such as methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Enterococcus (VRE), and drug-resistant Streptococcus pneumoniae (DRSP) to be a “Serious Threat”. Given the high prevalence, associated morbidity and mortality, and in particular, the limited treatment options, we will focus on MRSA and VRE infections in this continuing education monograph.
- Methicillin-resistant Staphylococcus aureus (MRSA): resistance to methicillin (oxacillin) and considered resistant to other beta-lactam antibiotics (except ceftaroline).(CLSI 2020)
- Vancomycin-resistant Enterococcus (VRE): resistance to vancomycin and commonly resistant to other antibiotics (e.g., ampicillin).(CDC 2019a)
Epidemiology: Prevalence and disease burden trends
Multidrug resistant organisms (MDRO) are responsible for a growing epidemic causing substantial morbidity and mortality around the United States (US) and globally, as well as increased hospital costs. The prevalence of MDRO has steadily increased during the last several decades in the US. Though the true burden of MDRO infections remains uncertain, likely to due to underreporting of national rates, it has been estimated they cause >2.8 million antibiotic-resistant infections and 35,000 deaths each year in the US alone.(CDC 2019a) Prevalence of MDRO can vary greatly in the US based on the health care setting and geography. For example, according to the CDC, VRE first appeared in the eastern portion of the US in the early 1990s followed by western US a few years later.
Antimicrobial resistance rates strongly correlate to the type of medical setting, hospital size, and tertiary-level of care. Other risk factors for developing MDRO infections can be multifactorial including older age, long duration of hospitalization including interinstitutional transfers such as nursing homes, frequent encounters with health care environments (i.e., hemodialysis units), presence of indwelling devices, prior history of surgery or invasive procedures, co-morbidities, selective pressure due to antimicrobial use, and transmission from those who are colonized or infected, for example, having frequent contact with health care personnel.(CDC 2020)
Drug resistant Gram-positive bacterial infections
MRSA is a cause for global concern and has been highly prevalent in many countries (Figure 1 and 2). It is the leading cause of mortality due to antibiotic-resistant infections in the US; rates are higher in the US than most other developed countries. From the late 1960s to early 2000, the rate of MRSA in hospitalized patients steadily increased with MRSA accounting for up to 59.5% of S. aureus isolates in intensive care units (ICUs) in 2003. MRSA now accounts for approximately 45% of all S. aureus invasive isolates (Figure 3, CDDEP 2021a), causing over 323,000 infections per year and over 10,000 deaths.(CDC 2019a)
| Figure 1. MRSA Prevalence in Select Countries (CDDEP 2021a) |
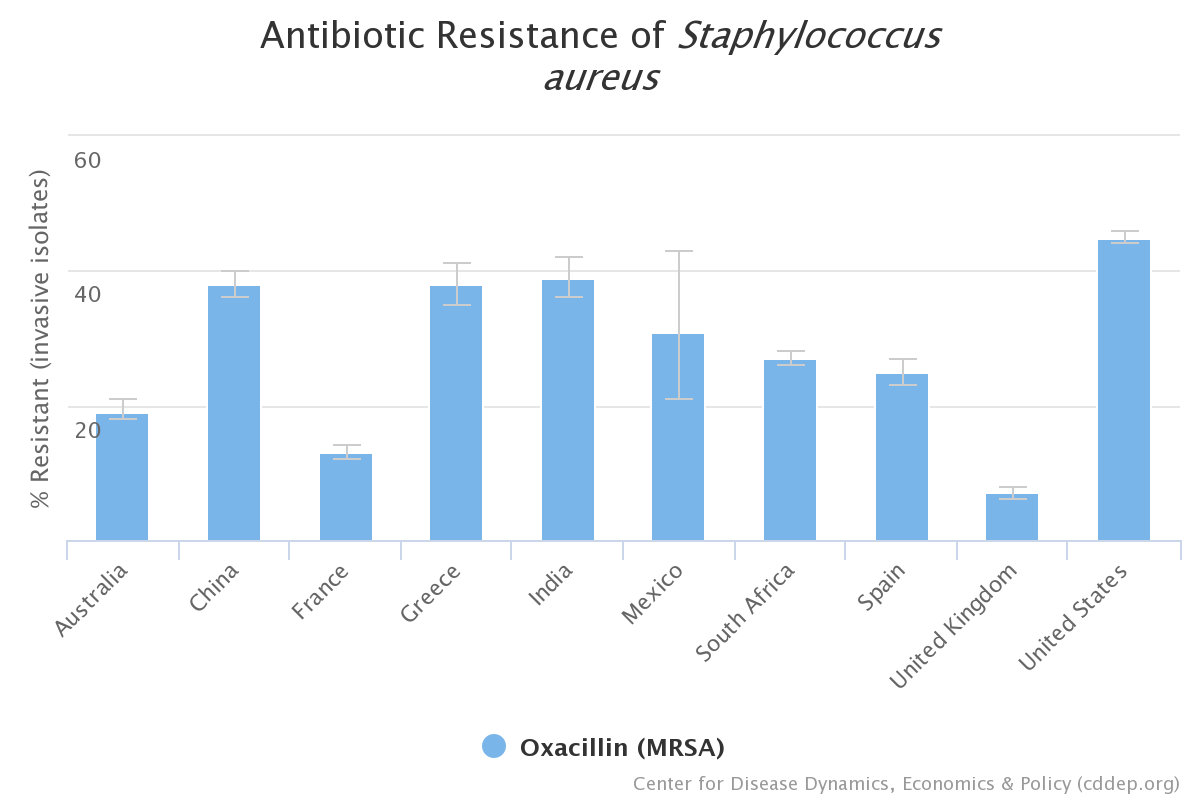 |
| Source: The Center for Disease Dynamics, Economics & Policy. Resistance Map: Antibiotic Resistance. 2021. https://resistancemap.cddep.org/AntibioticResistance.php. Date accessed: February 2, 2021. |
| Figure 2. Global Spread of MRSA (CDDEP 2021b) |
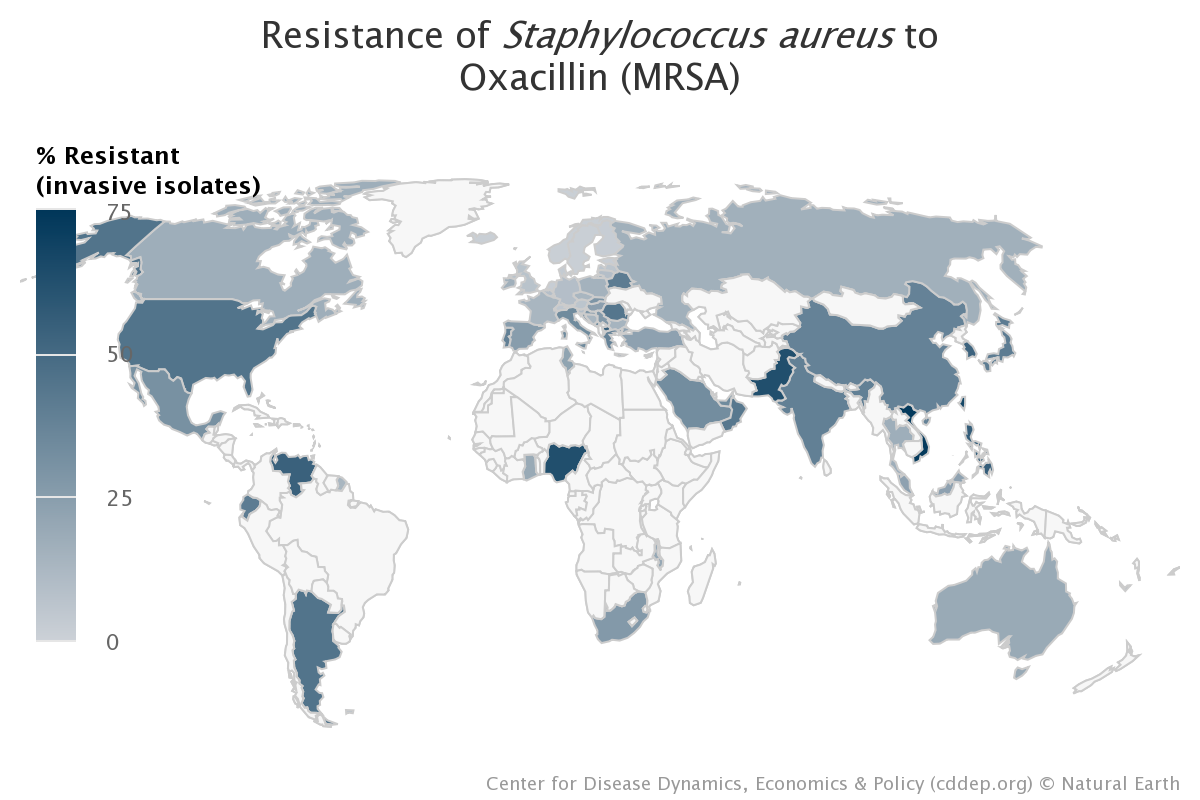 |
| Source: The Center for Disease Dynamics, Economics & Policy. Resistance Map: Antibiotic Resistance. 2021. https://resistancemap.cddep.org/AntibioticResistance.php. Date accessed: February 2, 2021. |
| Figure 3. Staphylococcus aureus Resistance, United States, 1999-2016 (CDDEP 2021c) |
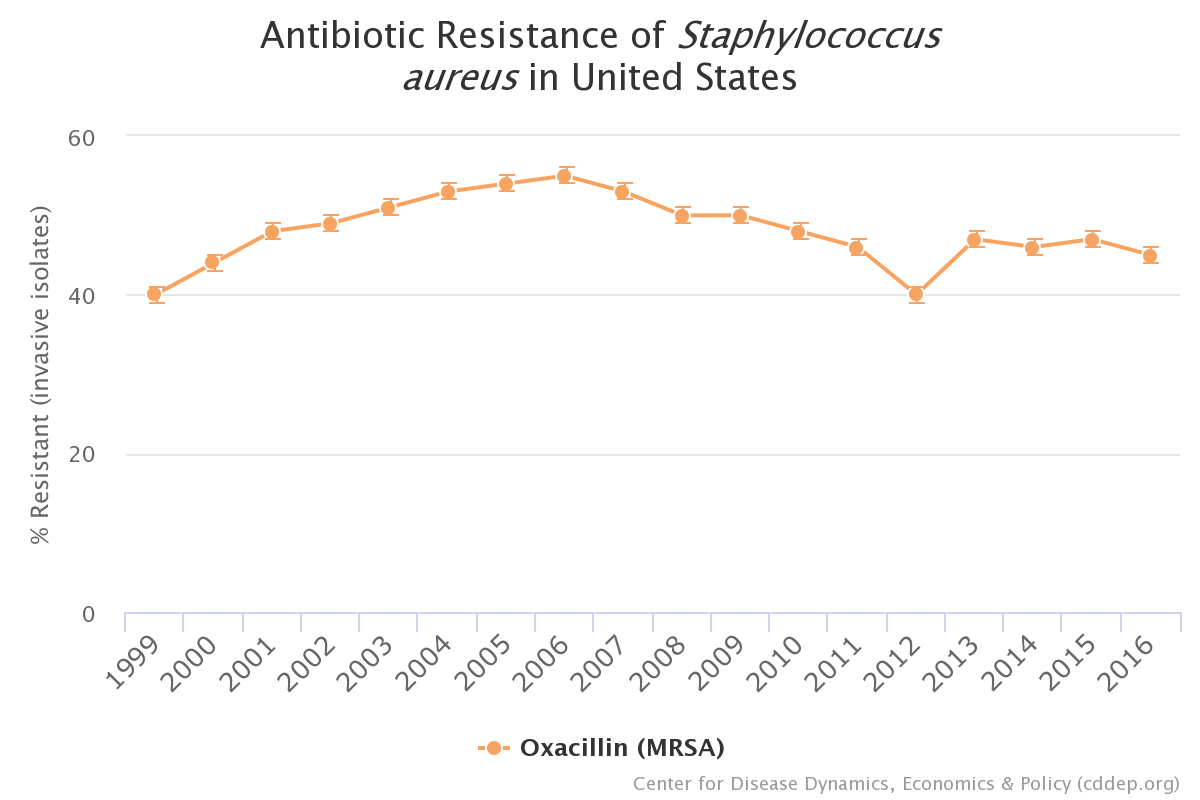 |
| Source: The Center for Disease Dynamics, Economics & Policy. Resistance Map: Antibiotic Resistance. 2021. https://resistancemap.cddep.org/AntibioticResistance.php. Date accessed: February 2, 2021. |
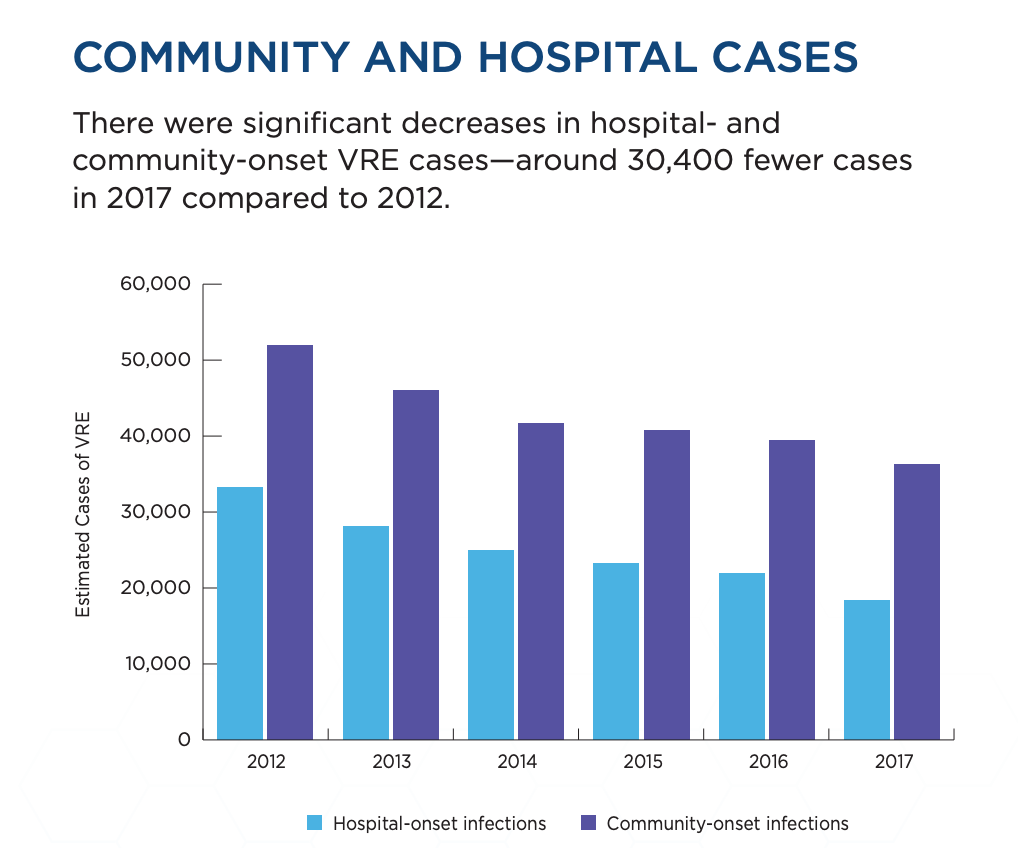
Enterococcus is a well-known cause of health care-associated infections which can include surgical-site infections, urinary tract infections (UTI), and bloodstream infections. In the US, Enterococcus causes over 54,000 infections and 5,400 deaths per year with approximately 30% of those cause caused by VRE among hospitalized patients.(CDC 2019a) The percentage of VRE in the US over time is highlighted in Figure 4. It should be noted however that there was a significant decrease in hospital- and community-onset VRE cases in 2017 compared to 2012 (Figure 5).
| Figure 4. Enterococcus faecium Resistance, United States, 1999-2016 (CDDEP 2021d) |
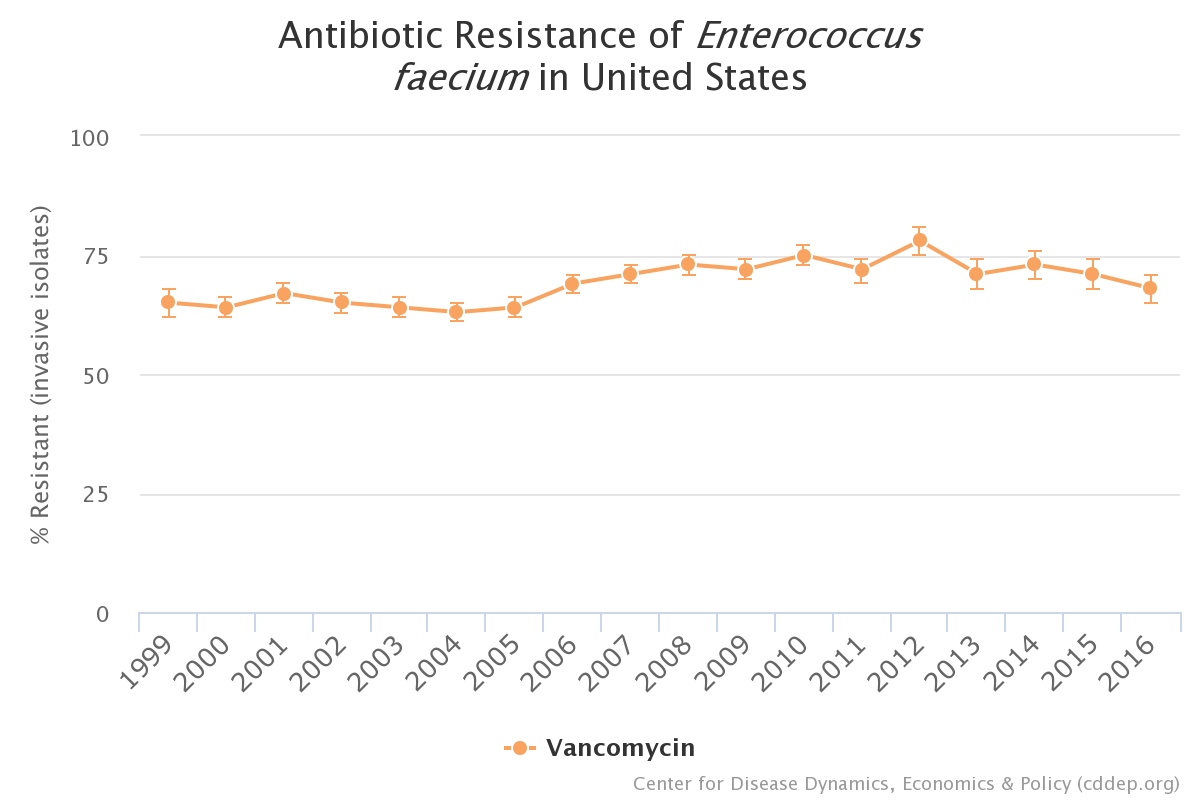 |
| Source: The Center for Disease Dynamics, Economics & Policy. Resistance Map: Antibiotic Resistance. 2021. https://resistancemap.cddep.org/AntibioticResistance.php. Date accessed: February 2, 2021. |
| Figure 5. Estimates Cases of VRE in Community and Hospital setting, United States, 2012-2017 (CDC 2019a) |
 |
| Source: The Center for Disease Dynamics, Economics & Policy. Resistance Map: Antibiotic Resistance. 2021. https://resistancemap.cddep.org/AntibioticResistance.php. Date accessed: February 2, 2021. |
PAUSE AND REFLECT: What types of drug-resistant Gram-positive infections do you see most frequently in your practice?
Drug resistant Gram-negative bacterial infections
Increased prevalence of infections caused by drug-resistant GNB continues to be a public health concern. In a study that looked at 890 US hospitals from 2012-2017, the incidence of hospital-onset and community-onset infection from MDR-Pa and carbapenem-resistant Acinetobacter declined by 20-40%. The incidence of infections from CRE remained stable; however, the incidence of ESBL-E increased more than 50% which was primarily driven by community-acquired cases. E. coli accounted for 86% of the overall increase in ESBL-E infections.(Jernigan 2020; Tamma 2020)
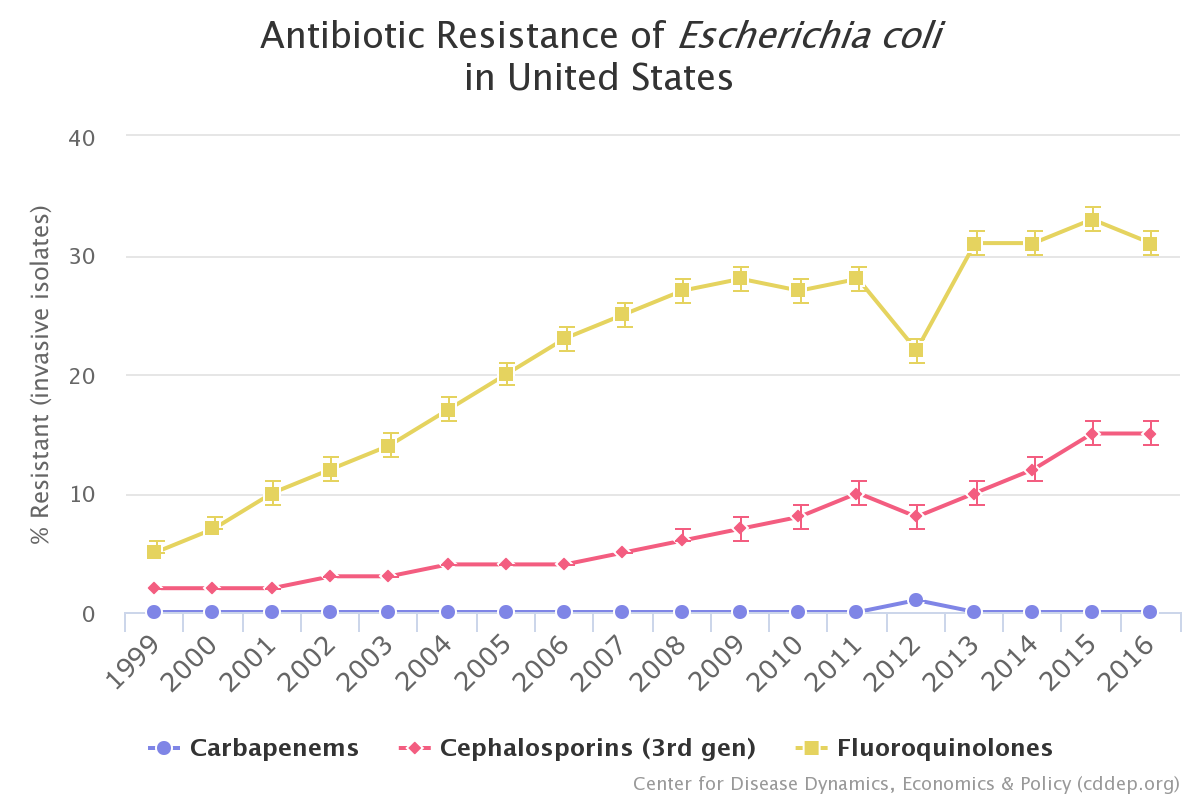
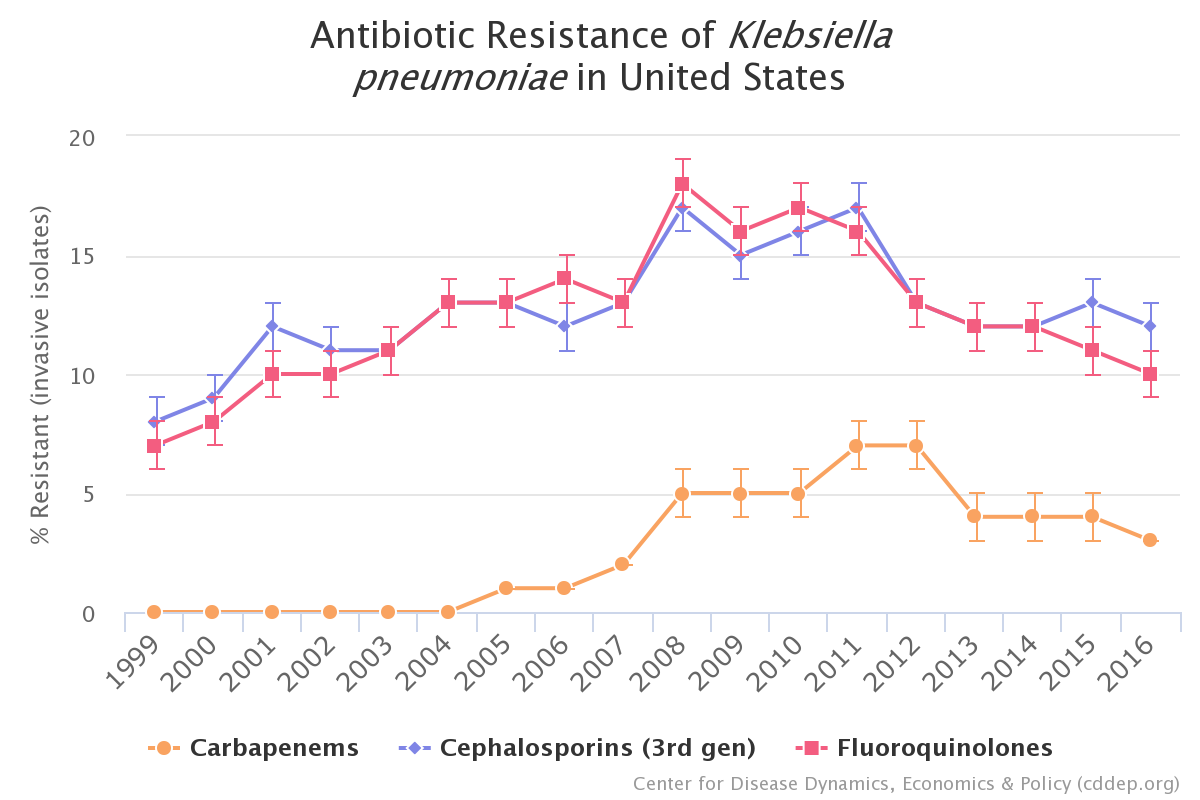
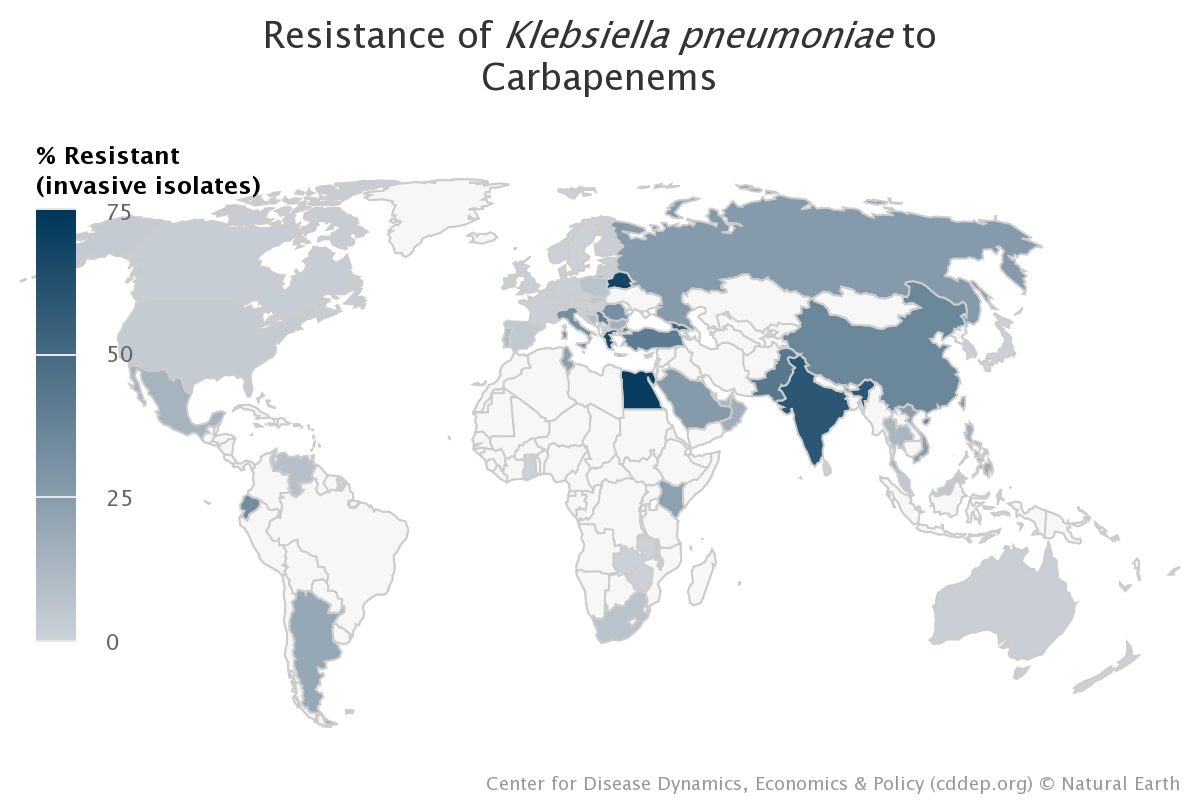
Resistance among Enterobacteriaceae (i.e., E. coli and Klebsiella spp.) has been increasing over both time (Figure 6 and 7) and space across the US with Klebsiella pneumoniae carbapenemase (KPC)-producing CRE found in most of the country.(CDC 2019a) Globally, KPC-producing CRE remains more common in Greece, Belarus, Egypt and India (Figure 8). These organisms pose a threat to patients primarily in health care facilities. Treatment options for these resistant organisms are limited and lead to significant excess morbidity and mortality. The CDC estimates that ESBL-E and CRE combine to cause over 200,000 infections per year and over 10,000 deaths per year in the US.(CDC 2019a)
| Figure 6. Escherichia coli Resistance, United States, 1999-2016(CDDEP 2021e) |
 |
| Source: The Center for Disease Dynamics, Economics & Policy. Resistance Map: Antibiotic Resistance. 2021. https://resistancemap.cddep.org/AntibioticResistance.php. Date accessed: February 2, 2021. . |
| Figure 7. Klebsiella pneumoniae Resistance, United States, 1999-2016(CDDEP 2021f) |
 |
| Source: The Center for Disease Dynamics, Economics & Policy. Resistance Map: Antibiotic Resistance. 2021. https://resistancemap.cddep.org/AntibioticResistance.php. Date accessed: February 2, 2021. |
| Figure 8. Global Klebsiella pneumoniae Carbapenems Resistance(CDDEP 2021g) |
 |
| Source: The Center for Disease Dynamics, Economics & Policy. Resistance Map: Antibiotic Resistance. 2021. https://resistancemap.cddep.org/AntibioticResistance.php. Date accessed: February 2, 2021. |
Carbapenem-resistant Acinetobacter baumannii (CRAB) remains a challenging threat to hospitalized patients given its ability to frequently contaminate health care facility surfaces and medical equipment. Estimates by CDC show that carbapenem-resistant Acinetobacter accounts for approximately 8,500 infections in hospitalized patients with estimated 700 deaths annually in the US.(CDC 2019a). In-hospital mortality was noted to be significantly higher in those with carbapenem and ampicillin-sulbactam – resistant (CASR) Acinetobacter baumannii compared to those with non-CASR A. baumannii infections (43% vs 20%, p<0.001).(Chopra 2013) Other studies have shown that the mortality rate for CRAB infections such as hospital-acquired pneumonia or bloodstream infections can approach 60-70%.(Wong 2017) Unfortunately, antimicrobials for CRAB are limited and far from perfect due to increasing resistance rates.
Pseudomonas aeruginosa, susceptible and MDR strains, are a well-known cause of health care-associated infections similar to the types caused by ESBL-E and CRE. In the US, MDR-Pa is estimated to cause over 32,600 infections in hospitalized patients yearly with an estimated 2,700 deaths.(CDC 2019a) Data from other sources such as the National Health Care Safety Network (NHSN), report a prevalence of MDR strains among P. aeruginosa as high as 22% in 2007(Kallen 2010), however the estimated rate has decreased to 9% as of 2018.(CDC, Antibiotic Resistance and Safety Portal) P. aeruginosa is intrinsically resistant to commonly used antibiotics with MDR further limiting treatment options.
PAUSE AND REFLECT: What types of drug-resistant Gram-negative infections do you see most frequently in your practice?
Types of infections caused by MDR GPB and GNB
MDRO infections have similar clinical manifestations as infections caused by susceptible organisms. Management and outcomes, however, can differ depending on the degree of resistance and the availability of certain targeted treatments (Table 1).
| Table 1. Infection types and associated multi-drug resistant organisms. |
| Types of Infection |
MDR organism |
| CNS (post-neurosurgical) |
MRSA, A. baumannii |
| Pulmonary (hospital-acquired pneumonia, ventilator-associated pneumonia) |
P. aeruginosa, A. baumannii, ESBL, CRE, MRSA, VRE |
| Endovascular |
MRSA, VRE |
| Intra-abdominal |
ESBL, CRE, VRE, P. aeurginosa, |
| Urinary tract |
ESBL, CRE, VRE, P. aeruginosa |
| Skin and soft tissue |
MRSA |
| Surgical site infections |
P. aeruginosa, A. baumannii, ESBL, CRE, MRSA, VRE |
| Wounds |
P. aeruginosa, A. baumannii, ESBL, CRE, MRSA, VRE |
| Central-line associated bloodstream infection (CLABSI) |
P. aeruginosa, A. baumannii, ESBL, CRE, MRSA, VRE |
| CNS, central nervous system; MRSA, methicillin-resistant Staphylococcus aureus; ESBL extended-spectrum beta-lactamase-producing Enterobacteriaceae; CRE, carbapenem-resistant Enterobacteriaceae; VRE, vancomycin-resistant Enterococcus |
General management of MDR GNB and GPB infections
Prior to identification of the organism and susceptibility, empiric treatment can be considered based on the patient’s clinical presentation and condition. Depending on the type of infection present, the empiric treatment should be guided by the community or hospital’s local susceptibility patterns for the most common types of pathogens.
The spectrum of activity should also be guided by the type of infection present (i.e., treatment for health care associated pneumonia would warrant a broader coverage than a simple cystitis or a simple non-purulent cellulitis in a young healthy patient which may not warrant gram-negative coverage but rather a first-generation cephalosporin like cefazolin).
Per the Infectious Diseases Society of America (IDSA), the following should be considered when determining the type of empiric treatment(Tamma 2020):
- Patient’s previous organism and susceptibility in the last six months
- Presence of antibiotic exposures in the past 30 days (i.e., if patient was recently treated with a piperacillin-tazobactam, then a gram-negative agent from a different class that offers similar spectrum of activity should be considered)
If the site of infection requires a surgical intervention (i.e., washout or incision and drainage), then it is imperative that the intervention occurs in conjunction with antibiotic use. Cultures from the site of concern should also be sent to help target antimicrobials.
Once the pathogen is identified and antimicrobial susceptibility is available, the antibiotic should be narrowed and targeted accordingly.
II. Defining Drug Resistance
Drug resistance among GNB and GPB is of particular concern given the various resistance mechanisms they can harbor and the limited therapeutic options effective against serious MDR GNB and GPB infections (Tables 2 and 3). GNB can both upregulate (chromosomally-mediated) and acquire (plasmid-mediated) these resistance genes. Among the many resistance mechanisms, beta-lactamases are the most common and highly concerning. Both ESBL and KPC production by GNB such as E. coli and Klebsiella spp. confers high-level resistance to most (and sometimes all) beta-lactam antibiotics including last line agents such as carbapenems (i.e., CRE). MDR-Pa also has the ability to produce beta-lactamases along with other mechanisms such as porin loss and efflux pumps that confer resistance to multiple antibiotic drug classes. For both S. aureus and enterococci, target site replacement is the most common and highly concerning. Acquisition of mecA gene by S. aureus allows it to encode for PBP2a, a substitute transpeptidase for original PBP target site with low affinity for all beta-lactams (except ceftaroline) resulting in a MRSA phenotype. Resistance with MRSA can have concomitant resistance mechanisms versus other commonly used anti-staph antibiotics (e.g., clindamycin) further complicating the choice for treatment. Enterococci most problematically confers resistance against vancomycin via acquisition of van gene (vanA most commonly). Most commonly, the vancomycin target binding site D-Ala-D-Ala is replaced with D-Ala-D-lactate, drastically decreasing the affinity of vancomycin and eliminating its clinical utility. These mechanisms, especially in critically ill patients, pose a grave threat to achieving favorable clinical outcomes given the need for less effective antibiotic therapy (e.g., vancomycin instead of nafcillin or cefazolin for S. aureus).
| Table 2. Mechanisms of Resistance in GNB(Peleg 2010) |
| Mechanism |
Action |
Examples of Affected Antibiotics |
| Beta-lactamases |
Degradation of beta-lactam ring |
All beta-lactams including carbapenems |
| Efflux pumps |
Expels antibiotic from bacteria prior to exerting its effect |
Beta-lactams, fluoroquinolones, aminoglycosides, tetracyclines |
| Porin channel loss |
Reduces level of antibiotic within bacteria by preventing movement through the cell membrane |
Beta-lactams including carbapenems |
| Antibiotic-modifying enzymes |
Render the antibiotic incapable of interacting with its target site of action |
Aminoglycosides |
| Target site mutations |
Prevent the antibiotic from binding to its site of action |
Fluoroquinolones |
| Ribosomal mutations |
Prevent the antibiotic from inhibiting bacterial protein synthesis |
Tetracyclines, aminoglycosides |
| Metabolic bypass mechanisms |
Use an alternative resistant enzyme to bypass the antibiotic inhibitory effect |
Sulfonamides, trimethoprim |
| Mutations in the lipopolysaccharide |
Prevents polymyxin antibiotics from binding to their target site of action |
Polymyxins |
| Table 3. Mechanisms of Resistance in GPB(Munita 2015) |
| Mechanism |
Action |
Examples of Affected Antibiotics |
| Drug inactivation (beta-lactamase) |
Hydrolyze beta-lactam ring |
Penicillins (most S. aureus) |
Target replacement
S. aureus
Enterococci |
mecA gene encodes for PBP2a as substitute for original PBP target
van gene cluster (e.g. vanA) encodes for D-Ala-D-Ala to D-Ala-D-lactate |
All beta-lactams except ceftaroline (MRSA)
Vancomycin (VRE) |
| Target modification |
Genes encode modified sites of actions, prevent antibiotic binding |
Ceftaroline (S. aureus)
Penicillin, ampicillin (Enterococci)
Linezolid (S. aureus, Enterococci) |
| Change in cell surface adaption |
Multiple genes involved in resistance phenotype |
Vancomycin (VISA)
Daptomycin (S. aureus, Enterococci) |
PAUSE AND REFLECT: What initially guides your management when it comes to empirically starting antibiotics for a MDR GPB or GNB infection?
III. Therapies for MDR GNB and MDR GPB
MDR GPB therapeutics
Overall, the number of therapeutic options for treatment of serious MRSA and VRE infections is limited. Long-standing antibiotic agents currently available for serious infections include vancomycin, telavancin, ceftaroline, daptomycin, and linezolid. Other agents for mild-to-moderate MRSA infections or as later-line alternatives include clindamycin, doxycycline, minocycline, trimethoprim-sulfamethoxazole, tigecycline, quinupristin-dalfopristin, and rifampin (in combination with another anti-MRSA antibiotic).(Liu 2011; Stevens 2014) For VRE, agents for mild infections such as UTIs or other alternatives include fosfomycin, nitrofurantoin, doxycycline, tigecycline, and quinupristin-dalfopristin (not active against E. faecalis).(Heintz 2010) The limited number of safe and effective options, especially for serious infections, reaffirms the need for new and better therapeutic options for treatment of MDR GPB. Recently approved options active against MRSA and VRE will be discussed in the next section. A quick reference table is available below regarding current mainstay and novel therapeutics for MDR GPB (Table 4).
Vancomycin
Vancomycin is a glycopeptide antibiotic that exerts its pharmacologic activity by blocking glycopeptide polymerization by binding to the D-Ala-D-Ala portion of the bacterial cell wall thereby inhibiting bacterial cell wall synthesis. Historically, vancomycin requires therapeutic drug monitoring by obtaining trough levels, but this is not optimal in terms of safety (higher nephrotoxicity) and effectiveness (poor predictor) as compared to area under the curve (AUC)-based monitoring(Rybak 2009; Finch 2017; Prybylski 2015; Neely 2018). Frequent AUC monitoring is more appropriate for hemodynamically unstable patients.(Rybak 2020) Vancomycin has been the drug of choice for treatment of serious MRSA infections for decades. This includes bacteremia, endocarditis, pneumonia, central nervous system (CNS) infections, bone/joint infections, and severe skin/soft tissue infections. This is based on years of clinical evidence and experience as well as recommendations from the 2011 guidelines for treatment of MRSA infections by the IDSA.(Liu 2011)
Telavancin
Telavancin is another glycopeptide antibiotic with a similar mechanism of action as vancomycin. Additionally, it has a mechanism that involves disruption of membrane potential and changes cell permeability. It is indicated as an alternative agent for use in complicated skin and soft tissue infections caused by GPB including MRSA as well as hospital-acquired/ventilator-associated bacterial pneumonia caused by S. aureus, both with data for concurrent S. aureus bacteremia.(Telavancin PI 2016) Several trials have demonstrated telavancin to be at least as effective as vancomycin for treatment of skin and soft tissue infections caused by MRSA without increased nephrotoxicity.(Stryjewski 2008; Stryjewski 2006; Holubar 2020)
Ceftaroline
Ceftaroline is a fifth-generation cephalosporin beta-lactam antibiotic with broad antibacterial activity. It is currently approved for community-acquired pneumonia and skin and soft tissue infections (including MRSA), both with concurrent bacteremia. Ceftaroline has specifically become an attractive option for use against MRSA bacteremia/endocarditis as the only beta-lactam with MRSA activity. It is not approved by the US Food and Drug Administration (FDA) for those indications, but clinical evidence has been emerging that it poses as a viable effective option for refractory MRSA bacteremia.(Zasowski 2017; Burnett 2016; White 2017) Additionally, the use of ceftaroline in combination with other agents such as daptomycin is a potential option for severe MRSA bacteremia.(McCreary 2019)
Daptomycin
Daptomycin is cyclic lipopeptide antibiotic with potent activity against GPB including MRSA and VRE. It is approved for treatment of skin and soft tissue infections and S. aureus bacteremia including right-sided infective endocarditis. It is also recommended for other infections including MRSA bone/joint infections and VRE bacteremia/endocarditis.(Liu 2011; Baddour 2015) Daptomycin is a first-line alternative agent to vancomycin for the treatment of MRSA bacteremia. However, some studies have shown associated reduced clinical failure and 30-day mortality along with reduced risk of nephrotoxicity when compared with vancomycin.(Smith 2014; Claeys 2015; Moise 2016) Labeled dosing for this indication is 6 mg/kg, but expert recommendations suggest 8-10 mg/kg based on pharmacokinetic/pharmacodynamic (PK/PD) models for complicated MRSA bacteremia (including endocarditis) for improved efficacy against isolates with reduced daptomycin susceptibility.(Liu 2011; Baddour 2015) Recent data have specifically suggested a survival advantage when using high dose (10 mg/kg) daptomycin for VRE bacteremia as compared to standard doses (6 mg/kg).(Britt 2017) The E. faecium breakpoint set forth by CLSI has subsequently been revised to reflect this exposure-response relationship.(CLSI 2020) Caution is necessary when using daptomycin as it is inactivated by pulmonary surfactant and therefore should not be used for any type of pneumonia.(Daptomycin PI 2017)
Linezolid
Linezolid is an oxazolidinone antibiotic with broad activity against GPB including MRSA and VRE. It is approved for a wide variety of indications including skin and soft tissue infections, community-acquired pneumonia, hospital-acquired pneumonia (including MRSA), and VRE infections including bacteremia. Linezolid is considered a first-line treatment for VRE bacteremia, MRSA pneumonia (along with vancomycin), and skin and soft tissue infections. Of the agents discussed thus far for serious MDR GPB infections, linezolid is the only one also available as an oral formulation for systemic infections. It is approximately 100% bioavailable, which offers a convenient oral option for certain serious infections once a patient has clinically improved and is able to take oral medications. Duration of treatment may be limited, though due to toxicities that can generally occur after two weeks of therapy (e.g. thrombocytopenia).(Linezolid PI 2017)
Tedizolid
Tedizolid is a newer oxazolidinone antibiotic FDA approved for clinical use in June 2014 for treatment of acute bacterial skin and skin structure infections. It has potent activity against multiple GPB (including MDR strains) such as Streptococcus species, Enterococcus faecalis, and S. aureus (including MRSA).(Tedizolid PI 2016) Although not on its FDA labeling, tedizolid is highly active in vitro against E. faecium (VRE) and even other resistance phenotypes such as linezolid-resistant enterococci and S. aureus. Tedizolid is 4- to 16-fold more potent in vitro than linezolid for most clinically important GPB.(Burdette 2015) The proposed advantages for tedizolid over linezolid from a pharmacologic perspective include no labeled warning for hematologic toxicity (e.g., thrombocytopenia) or drug interactions with serotonergic or adrenergic agents. It is also dosed once daily with high bioavailability allowing for 1:1 intravenous (IV) to oral dosing conversion (200 mg daily IV or PO).(Tedizolid PI 2016) Two phase 3 clinical trials assessing tedizolid’s efficacy (for 6 days) for skin infections demonstrated non-inferiority to linezolid (for 10 days) including the MRSA subgroup.(Moran 2014; Prokocimer 2013) Tedizolid is a potent antibiotic with activity against a wide range of MDR GPB. More clinical evidence and experience will be necessary to understand its place for the treatment of serious invasive MDR GPB infections.
Dalbavancin
Dalbavancin is a long-acting lipoglycopeptide FDA approved in May 2014. Its antibacterial spectrum of activity encompasses Streptococcus species, Enterococcus faecalis (vancomycin-susceptible), and S. aureus (including MRSA). Currently, dalbavancin is indicated for the treatment of acute bacterial skin and skin structure infections due to GPB.(Dalbavancin PI 2016) The main advantage of this antibiotic is the long half-life of approximately 345 hours. This allows for both the single-dose regimen (1500 mg one dose) and two-dose regimen (1000 mg x1, then 500 mg one week later). In both phase 3 clinical trials, dalbavancin proved to be non-inferior to standard vancomycin/linezolid therapy or non-inferior to the two-dose dalbavancin regimen (experimental group: dalbavancin 1500 mg x1 dose). Early clinical improvement (FDA-designated primary outcome) was also numerically similar between the groups in the MRSA subset.(Dunne 2016; Boucher 2014) Dalbavancin offers a unique treatment modality of a single dose regimen for management of complicated bacterial skin and soft tissue infection (including MRSA) that would otherwise require multi-day regimens of other IV antibiotics (e.g., vancomycin).
Oritavancin
Oritavancin is another long-acting lipoglycopeptide FDA approved in August 2014 for the treatment of acute bacterial skin and skin structure infections caused by GPB. Its spectrum of activity includes Streptococcus species, Enterococcus faecalis (vancomycin-susceptible), and S. aureus (including MRSA).(Oritavancin PI 2016) Although not in the FDA approved labeling, oritavancin also has significant activity against another MDR GPB – VRE.(Johnson 2015) There is even early emerging clinical experience for the use of oritavancin for more invasive infections although more data are needed before routine recommendations can be made for its use outside of skin and soft tissue infections.(Johnson 2015) Oritavancin is also novel, similar to dalbavancin, with a half-life of approximately 245 hours which allows for it to be given as a single-dose regimen (1200 mg x 1 dose). In two phase 3 clinical trials, oritavancin was non-inferior to standard therapy (i.e., vancomycin) for acute bacterial skin and skin structure infections. This similarity in clinical outcomes was maintained for the MRSA subgroup.(Corey 2014; Corey 2015) Along with dalbavancin, oritavancin offers a novel treatment modality of a single dose IV complete regimen for bacterial skin and soft tissue infections including MRSA. Further data are necessary to understand its utility for VRE infections.
MDR GNB therapeutics
Antibiotic treatments for drug-resistant GNB vary based on the resistance mechanism. As such, there may be some overlap of treatment options, but the approach generally differs when treating infections caused by ESBL-E, CRE, MDR-Pa, or MDR-Acinetobacter. Overall, treatment options include beta-lactam antibiotics (e.g., carbapenems or piperacillin/tazobactam), polymyxins (colistin and polymyxin B), tigecycline, aminoglycosides, fosfomycin, and combination antibiotic therapy. The limited number of effective options underlies the need for new and better therapeutic options for treatment of MDR GNB – recently approved options will be discussed in the next section. A quick reference table is available below regarding current mainstay and novel therapeutics for MDR GNB (Table 6).
Beta-lactams
Carbapenems are generally considered the treatment of choice for serious infections caused by ESBL-E. This is based on clinical evidence that demonstrated a lower relative risk of mortality for carbapenems in comparison to alternative antibiotics (non-beta-lactam/beta-lactamase inhibitors [BL/BLI]) for treatment of ESBL-E bacteremia. For CRE infections, meropenem can be used only if ertapenem resistance, meropenem-susceptible and carbapenemase testing results are either not available or negative. This is generally because the majority of CRE infections resistant to ertapenem, but susceptible to meropenem, are caused by organisms that do not produce carbapenemases.(Vardakas 2012; Tamma 2020)
The use of piperacillin-tazobactam has been long debated for use in treating infections caused by ESBL-E if susceptible to piperacillin-tazobactam. However, a randomized clinical trial (RCT) at 26 sites and 9 countries found that among patients with ESBL-E bloodstream infection, the use of piperacillin-tazobactam compared to meropenem did not result in a noninferior 30-day mortality essentially questioning the use of piperacillin-tazobactam in this setting.(Harris 2018) Thus, per most recent IDSA guidelines, it is recommended to avoid the use of piperacillin-tazobactam for ESBL-E infections, even if susceptible to piperacillin-tazobactam. However, if piperacillin-tazobactam was initiated for empiric treatment for non-invasive infection (i.e., simple cystitis) and the patient demonstrates clinical improvement, then no change or extension of the antibiotic regimen is recommended. These recommendations were largely made due to piperacillin-tazobactam's diminished effect on invasive ESBL-E infections as well as the possibility of inaccurate piperacillin-tazobactam minimum inhibitory concentration (MIC) in the presence of ESBL enzymes.(Tamma 2020)
Ceftolozane/tazobactam is a novel cephalosporin/BLI combination FDA approved in December 2014. Its antibacterial spectrum of activity encompasses Streptococcus spp., various Enterobacteriaceae (including ESBL-E and AmpC beta-lactamase producers), and P. aeruginosa (including MDR strains). It is currently approved for complicated intra-abdominal infections and complicated UTIs (including pyelonephritis) as of 2014, and most recently, for hospital-acquired bacterial pneumonia and ventilator-associated bacterial pneumonia as of 2019.(Ceftolozane/tazobactam PI 2020) In a phase 3 RCT assessing ceftolozane/tazobactam versus levofloxacin for UTI, ceftolozane/tazobactam proved superior for microbiologic and clinical cure.(Wagenlehner 2015) In a phase 3 RCT evaluating efficacy against meropenem for intra-abdominal infections, ceftolozane/tazobactam was non-inferior to meropenem, including drug-resistant Gram-negative strains.(Solomkin 2015) Both phase 3 RCTs included strains of ESBL-E which offers useful insight to treatment of resistant infections. Additionally, multiple retrospective cohort studies have demonstrated the effectiveness of ceftolozane/tazobactam for the treatment of MDR-Pa and preference over older more toxic agents such as polymyxins and aminoglycosides.(Gallagher 2018; Pogue 2020) The clinical evidence and potent in vitro activity makes ceftolozane/tazobactam a first-line option for treatment of MDR-Pa infections as well as a potential carbapenem-sparing regimen for ESBL-E infections.(Giacobbe 2018) It is recommended as a first-line treatment option for MDR-Pa.(Tamma 2020)
Ceftazidime/avibactam is a cephalosporin/novel BLI combination FDA approved in February 2015. It is the first BL/BLI approved to treat CRE and MDR-Pa infections.(Noval 2020; Zhanel 2013). It has potent broad-spectrum activity against various GNB including drug-resistant strains such as ESBL-E, CRE (KPC-producers), AmpC-producing GNB, and MDR-Pa. Indications include complicated UTI (including pyelonephritis), complicated intra-abdominal infections, and hospital-acquired and ventilator-associated pneumonia.(Ceftazidime/avibactam PI 2018) Notably, a RCT was done that evaluated ceftazidime/avibactam versus best-available therapy (mostly carbapenem monotherapy) for treatment of ceftazidime-resistant infections (mostly complicated UTI). Ceftazidime/avibactam had a similar rate of clinical cure to meropenem which provides high-quality evidence for the treatment of drug-resistant infections.(Carmeli 2016) A retrospective cohort study conducted by Shields and colleagues demonstrated the superiority of ceftazidime/avibactam versus other antibiotic therapy for CRE (specifically Klebsiella pneumoniae) bacteremia.(Shields 2017) The CRACKLE study was a prospective, multicenter, observational study assessing ceftazidime-avibactam or colistin for CRE infections. Ceftazidime/avibactam was superior to colistin with lower probability of all-cause hospital mortality.(van Duin 2018) More data are emerging regarding the development of resistance and treatment failure due to risk factors such as infections with KPC-3 producing CRE, evidence of pneumonia or if receipt of renal replacement therapy.(Shields 2018) Currently, ceftazidime/avibactam is recommended as a first-line treatment option for MDR-Pa and CRE.(Tamma 2020)
Meropenem/vaborbactam is an anti-pseudomonal carbapenem/novel BLI combination approved by the FDA in August 2017. Vaborbactam protects meropenem from degradation by certain beta-lactamases, most importantly KPC, and adds to the already broad-spectrum Gram-negative activity of meropenem. This latest antibiotic is FDA approved for the treatment of complicated UTI (including acute pyelonephritis). It was evaluated in a phase 3 RCT versus piperacillin/tazobactam and proved to be non-inferior in terms of clinical cure and microbiologic eradication.(Meropenem/vaborbactam PI 2017) Another phase 3 RCT (TANGO II) assessing meropenem/vaborbactam versus best available therapy for CRE infections was stopped early due to the risk-benefit consideration (in favor of meropenem/vaborbactam), therefore the decision was made that randomization to best available therapy should cease. In TANGO II, meropenem/vaborbactam was associated with decreased mortality, increased clinical cure, and lower rates of nephrotoxicity compared to best available therapy for CRE infections.(Petty 2018; Wunderink 2017) Meropenem/vaborbactam was also shown to retain its activity against strains producing KPC mutants resistant to ceftazidime/avibactam.(Wilson 2019; Novelli 2020) Additionally, vaborbactam was shown to reduce meropenem MICs of strains that exhibited reduced meropenem susceptibility due to production of ESBL or AmpC-type beta-lactamases.(Lomovskaya 2017; Novelli 2020) As more experience and evidence amounts for meropenem/vaborbactam, its utility will also grow, and we now have another effective option for the treatment of KPC-producing CRE infections. It is currently recommended as a first-line option for KPC-producing CRE.(Tamma 2020)
Given the variable susceptibility of MDR-Pa, the treatment must be individualized and based on in vitro susceptibility testing. Anti-pseudomonal beta-lactams that may be active versus MDR-Pa and that pose viable options include carbapenems (except ertapenem), ceftazidime, cefepime, aztreonam, piperacillin/tazobactam, ceftolozane/tazobactam and ceftazidime/avibactam. There are no compelling data that suggest one agent is superior to another, therefore selection of a beta-lactam will vary for empiric therapy based on local antibiograms and for definitive therapy based on isolate-specific susceptibility testing.
Polymyxins
The emergence of MDR organisms has triggered the reemergence of an older class of antibiotics—polymyxins. Colistin and polymyxin B are the two agents used clinically. They have broad-spectrum bactericidal activity against Gram-negative aerobic bacilli. It is one of the last-line therapeutic options for MDR GNB, including Acinetobacter species, P aeruginosa, and CRE particularly with pandrug resistance against beta-lactam antibiotics. Nephrotoxicity and neurotoxicity are the major limitations that preclude their widespread use. There are differences that are clinically important when deciding on systemic use of colistin versus polymyxin B (Table 4). Although there is more experience with colistin, polymyxin B seems to have a more favorable PK and safety (i.e., nephrotoxicity) profile.(Kassamali 2015; Tsuji 2019) Colistin may be more useful for UTIs or urosepsis over polymyxin B. Despite the availability of newly approved antibiotics, the utility of polymyxins may continue to be necessary as the incidence of MDR organisms grows in the US and worldwide.
| Table 4. Colistin versus Polymyxin B(Tsuji 2019, Kassamali 2015) |
| Colistin |
Polymyxin B |
• Prodrug, colistimethate sodium (CMS) must be hydrolyzed to be active colistin
• Delays in attainment of therapeutic colistin levels
• CMS is rapidly eliminated renally
• Difficult to safely achieve target levels |
Given as active drug and peak concentrations achieved more rapidly |
| Requires renal dose adjustments |
Not renally excreted
No renal dose adjustments |
Increased nephrotoxicity with colistin as compared to polymyxin B
Limited literature but potential safety advantage for polymyxin B |
| CMS excreted in high concentrations in the urine where converted to colistin |
Polymyxin B achieves poor urinary concentrations and inferior to other agents (e.g., aminoglycosides) for clearance of bacteriuria |
| Comparative efficacy is difficult to study – various factors effect outcomes such as severity of illness of patients studied, variety of dosing regimens, and antibiotic combinations given for treatment of MDR GNB. Few studies are available that study colistin versus polymyxin B. No clear data favoring one agent over the other for clinical use. Per recent guidelines(Tsuji 2019), polymyxin B is preferred for use in invasive infections due to superior PK characteristics and decreased potential for nephrotoxicity whereas colistin is preferred for treatment of lower UTIs given renal clearance of CMS. |
Fluoroquinolones
Levofloxacin and ciprofloxacin possess activity against a variety of Gram-negative bacteria including P. aeruginosa and are also one of the few oral antibiotics with activity against P. aeruginosa. Unlike levofloxacin, ciprofloxacin has limited activity against Streptococcus pneumoniae and thus, cannot be used for a community-acquired pneumonia. FDA box warnings include tendonitis, tendon rupture, CNS effects with other adverse reactions such as QTC prolongation and photosensitivity. Thus, per FDA, it should be used when benefits outweigh potential risks even for treatment for acute sinusitis, acute bronchitis or uncomplicated UTIs.(FDA 2016) Clinicians can consider its use for non-invasive, simple, non-bacteremia infections (i.e., simple cystitis) for an MDR GNB infection susceptible to fluoroquinolones - another “carbapenem-sparing” agent.
Delafloxacin, a novel anionic fluoroquinolone was FDA approved in 2017 for the indication of acute bacterial skin and soft tissue infections. It is currently the only agent with in vitro activity against MRSA and P. aeruginosa. Additionally, it has in vitro activity against certain anaerobes such as Bacteroides fragilis. Serious adverse reactions are similar to the above fluoroquinolones mentioned.(Delafloxacin PI 2017) Its role for treatment of serious MDR GPB or GNB infection remains to be defined.
Other agents
Due to its toxicity profile, most clinicians favor non-polymyxin therapy for CRAB infections. Therapeutics such as tigecycline, minocycline, amikacin and ampicillin-sulbactam have been shown to have in vitro activity against CRAB and are thus the mainstay therapy for both monotherapy and in combination. However, given concern for increasing resistance rates, there is a dire need for new therapeutic options for the treatment of CRAB infections.(Isler 2018; Viehman 2014) Nitrofurantoin and trimethoprim/sulfamethoxazole are recommended and preferred for treatment of ESBL-E uncomplicated cystitis.(Tamma 2020) Additionally, fosfomycin is recommended as an alternative treatment option for uncomplicated cystitis due to ESBL-producing E. coli.(Tamma 2020) Fosfomycin is currently available only as an oral agent (fosfomycin trometamol) in the US for the treatment of lower UTIs. It has broad spectrum coverage including urinary pathogens such as E. coli and enterococci. It is dosed for uncomplicated cystitis as 3 grams as a single dose given that it can achieve high urine and bladder tissue concentration for up to 2 days with only one dose. Although less evidence, oral fosfomycin has been also utilized for treatment of complicated cystitis with higher dosing (3 grams every 2-3 days for 3 doses).(Falagas 2016)
Newer antibiotic agents
Cefiderocol
Cefiderocol is a novel siderophore cephalosporin FDA approved in 2020 for treatment of cUTI and HABP/VABP.(Cefiderocol PI 2020) The mechanism of action is similar to other beta-lactams with the additional novel feature in that it binds to extracellular free iron and is actively transported across the outer cell membrane of bacteria into the periplasmic space using the bacterial siderophore iron uptake mechanism in addition to passive diffusion via porin channels. This novel mechanism and stability against various carbapenemases provide cefiderocol its broad-spectrum activity against MDR GNB, which includes activity against CRE, MDR-Pa, MDR A. baumannii, and Stenotrophomas maltophilia.(Yamano 2019) Use of cefiderocol for carbapenem-resistant GNB was evaluated in the CREDIBLE-CR trial, a multicenter, randomized, phase 3, open-label descriptive clinical study of cefiderocol or best available therapy. Clinical cure rates between both study groups were similar but notably there was an observed increase in all-cause mortality in the cefiderocol group at all time points. Acinetobacter baumannii or P. aeruginosa as a baseline pathogen was associated with higher mortality in the cefiderocol group.(El Lababidi 2020) Cefiderocol is currently recommended as an alternative option for treatment of infections caused by CRE and MDR-Pa.(Tamma 2020)
Imipenem/cilastatin/relebactam (IMI-REL)
IMI-REL is a combination of a well-known carbapenem, imipenem, plus a novel beta-lactamase inhibitor, relebactam. It was FDA approved in 2019 and currently has indications for treatment of cUTI, cIAI, hospital-acquired bacterial pneumonia and ventilator-associated bacterial pneumonia (HABP/VABP).(Imipenem/cilastatin/relebactam PI 2020) Relebactam restores activity of imipenem against MDR GNB including KPC-, ESBL-, and AmpC-producing Enterobacteriaceae and carbapenem-resistant P. aeruginosa. In addition to the RCT data driving its FDA approval, RESTORE-IMI 1 was a phase 3 RCT (N=47) assessing treatment for drug-resistant infections.(Motsch 2020) It compared IMI-REL alone versus imipenem plus colistin for imipenem-nonsusceptible infections, mostly P. aeruginosa and some MDR Enterobacterales, including patients with HABP/VABP, cIAI, and cUTI. Overall clinical response was similar between study groups while mortality was numerically lower in the IMI-REL group (28-day mortality:10% vs.30% [90% CI, -46.4, 6.7]). Additionally, nephrotoxicity was lower in the IMI-REL group vs. comparator (10% and 56%; p=.002). Although the clinical evidence for its use against MDR GNB is limited, it demonstrates potent activity against CRE and MDR-Pa. It is recommended as a first-line option for treatment of KPC-producing CRE and MDR-Pa.(Tamma 2020)
Lefamulin
Lefamulin is a novel pleuromutilin, first use in humans, FDA approved in 2019 as both IV and oral formulations for treatment of community-acquired bacterial pneumonia (CABP). It has a novel mechanism of action in which it inhibits protein synthesis by binding to the peptidyl transferase center of the 50S bacterial ribosome, thus preventing the binding of transfer RNA for peptide transfer.( Lefamulin PI 2019) In addition to activity against typical CABP organisms such as Streptococcus pneumoniae, Haemophilus influenzae, Mycoplasma pneumoniae, Legionella pneumophila, and Chlamydophila pneumoniae, it is active against both MRSA and VRE.(Veve 2018) As a novel drug class in humans, the novel mechanism of action of this drug is a promising feature as documented resistance and cross-resistance with other antibiotic classes is currently low. Use in other diseases outside of CABP (e.g., acute bacterial skin and skin structure infections [ABSSSI]) is limited, but emerging, and will require more evidence before consideration of routine clinical use.
Omadacycline
Omadacycline, an aminomethylcycline, is a novel once-daily tetracycline FDA approved in 2018 as both IV and oral formulations for the treatment of CABP and ABSSI. Omadacycline was specifically designed to overcome tetracycline resistance mechanisms. The mechanism is similar to other tetracyclines in that it binds to the 30S ribosomal subunit and blocks protein synthesis.(Omadacycline PI 2020) Increase in efflux pumps and production of ribosomal protection proteins are two major mechanisms of resistance against tetracyclines. Omadacycline retains activity by its ability to bypass these resistance mechanisms and lacks cross-resistance with other antibiotics. Omadacycline has broad-spectrum activity including covering many GPB, GNB, anaerobic, and atypical organisms as well as MDR strains. This includes in vitro activity against MRSA, VRE, ESBL-E, and Acinetobacter baumannii.(Barber 2018) This agent has favorable PK with once-daily dosing and good lung penetration, and no cases of C. difficile in clinical trials – making it a promising agent, although more clinical experience and evidence are needed before expanding its use for MDR GPB or GNB infections.(Barber 2018)
Eravacycline
Eravacycline is a synthetic tetracycline antibiotic approved by the FDA in August 2018 for the treatment of complicated intra-abdominal infection (cIAI).(Eravacycline PI 2020) Notably, the IGNITE2 phase 3 clinical trial found that eravacycline administered as an IV to oral transition therapy for the treatment of cUTIs did not achieve its primary endpoint of statistical non-inferiority compared to levofloxacin.(Tsai 2016) As a result, eravacycline has not been approved for this indication, and is only approved in its IV formulation. As with other tetracyclines, it inhibits protein synthesis by binding to the 30S ribosomal subunit, but is not significantly affected by efflux pumps or other tetracycline-specific resistance mechanisms. Eravacycline, like tigecycline, is active against most GNB, including some ESBL-E, some GPB including MRSA and VRE, and many anaerobes. One important exception to this broad spectrum of activity is Pseudomonas spp. However, eravacycline has demonstrated activity against some carbapenem-resistant GNB, creating interest in its potential to treat infections caused by CRE (including KPC-, MBL- and OXA-producers).(Livermore 2016) Particularly notable is that antimicrobial susceptibility testing indicates that eravacycline is more active against carbapenem-resistant Acinetobacter baumannii than comparable tetracyclines, levofloxacin, amikacin, tobramycin, and colistin.(Seifert 2018) While clinical data are limited for CRE and Acinetobacter, these data are promising, particularly given the limited options for infections caused by MDR Acinetobacter.
Plazomicin
Plazomicin is a once-daily aminoglycoside antibiotic which was engineered to overcome aminoglycoside-modifying enzymes, the most common aminoglycoside-resistance mechanism in Enterobacteriaceae. It has a relatively narrow spectrum of activity which includes several GNB (e.g., E. coli, K. pneumoniae, Proteus, Enterobacter species), but has limited activity versus most P. aeruginosa and Acinetobacter baumannii isolates and lacks activity against Enterococcus species, Stenotrophamonas maltophilia, and obligate anaerobes. It has demonstrated in vitro activity against ESBL-producing, aminoglycoside- resistant, and carbapenem-resistant isolates.(Plazomicin PI 2018) Plazomicin was approved by the FDA in June 2018 for the treatment of cUTIs based on the results of the phase 3 EPIC clinical trial, which demonstrated the non-inferiority of plazomicin compared to meropenem for treatment of cUTIs, including pyelonephritis.(Wagenlehner 2019) Monitoring creatinine clearance (CrCl) is recommended with use of plazomicin and therapeutic drug monitoring is recommended in patients with a CrCl <90 mL/min. Given its demonstrated efficacy in treatment of UTI and in vitro activity against CRE, it may be a plausible option for treatment of CRE UTI when other agents, including other aminoglycosides, are not active.
| Table 5. MDR Gram-positive organisms and current mainstay treatment agents |
| Gram-positive |
| Organism |
First Line Agents |
Alternative Agents |
| MRSA |
Vancomycin
Daptomycin
Linezolid
Ceftaroline |
Tedizolid
Dalbavancin
Oritavancin
Omadacycline
Lefamulin
Delafloxacin
Telavancin
Tigecycline
Doxycycline
Clindamycin
Trimethoprim-sulfamethoxazole
Minocycline |
| VRE |
Daptomycin
Linezolid |
Tedizolid
Fosfomycin PO (cystitis only)
Nitrofurantoin (cystitis only)
Doxycycline
Tigecycline
Quinupristin-dalfopristin
Oritavancin
Omadacycline
Eravacycline
Lefamulin |
| PO: oral route |
Table 6. MDR Gram-negative organisms and current mainstay treatment agents
(Adapted from Tamma PD, Aitken SL, Bonomo RA, et al. Infectious Diseases Society of America Antimicrobial Resistant Treatment Guidance: Gram-Negative Bacterial Infections. Clin Infect Dis. 2020 Oct 27:ciaa1478) |
| Gram-negative |
| Organism |
Source of infection |
First line agent |
Alternative agent |
| ESBL-E |
Cystitis |
Nitrofurantoin
Trimethoprim-sulfamethoxazole (TMP/SMX) |
Fluoroquinolones
Aminoglycosides
Fosfomycin PO (cystitis only)
Carbapenems |
| Pyelonephritis/cUTI |
Ertapenem
Meropenem
Imipenem-cilastatin
Ciprofloxacin
Levofloxacin
TMP/SMX |
|
| Systemic infections (non-urinary) |
Meropenem
Imipenem-cilastatin
Ertapenem |
| CRE |
Cystitis |
Fluoroquinolones
TMP/SMX
Nitrofurantoin
Single-dose aminoglycoside
Fosfomycin PO (cystitis only)
Meropenem* |
Ceftazidime-avibactam
Meropenem-vaborbactam
Imipenem-cilastatin-relebactam
Cefiderocol
Colistin |
| Pyelonephritis/cUTI |
Ceftazidime-avibactam
Meropenem-vaborbactam
Imipenem-cilastatin-relebactam
Cefiderocol
Meropenem* (extended-infusion) |
Aminoglycosides |
Systemic infection (non-urinary)
Resistance to ertapenem, susceptible to meropenem AND carbapenemase testing results not available or negative |
Meropenem (extended-infusion) |
Ceftazidime-avibactam |
Systemic infection (non-urinary)
Resistance to ertapenem, meropenem AND carbapenemase testing results not available or negative
Or
KPC identified (or carbapenemase positive) |
Ceftazidime-avibactam
Meropenem-vaborbactam
Imipenem-cilastatin-relebactam |
Cefiderocol
Tigecycline (for cIAI)
Eravacycline (for cIAI) |
| Metallo-β-lactamase (i.e., NDM, VIM, or IMP) carbapenemase identified |
Ceftazidime-avibactam + aztreonam
Cefiderocol |
Tigecycline (for cIAI)
Eravacycline (for cIAI) |
| OXA-48-like carbapenemase identified |
Ceftazidime-avibactam |
Cefiderocol
Tigecycline (for cIAI)
Eravacycline (for cIAI) |
| MDR-Pa |
Cystitis |
If susceptible -
Carbapenems (except ertapenem)
Ceftazidime
Cefepime
Aztreonam
Piperacillin/tazobactam
Fluoroquinolones
Ceftolozane/tazobactam
Ceftazidime/avibactam
Imipenem-cilastatin-relebactam
Cefiderocol
Aminoglycoside |
Colistin |
| Pyelonephritis/cUTI |
Ceftolozane/tazobactam
Ceftazidime/avibactam
Imipenem-cilastatin-relebactam
Cefiderocol |
Aminoglycosides |
| Systemic infections (non-urinary) |
Ceftolozane/tazobactam
Ceftazidime/avibactam
Imipenem-cilastatin-relebactam |
Cefiderocol
Aminoglycoside** |
| MDR-Acinetobacter |
|
Meropenem (extended-infusion)
Aminoglycosides
Ampicillin/sulbactam
Minocycline
Tigecycline
Eravacycline
Colistin, Polymyxin B
Fluoroquinolones
Cefiderocol |
*If ertapenem resistant, meropenem susceptible and carbapenemase testing n/a or negative
**only limited to uncomplicated blood stream infection (due to urinary source or catheter-related blood stream infection) with complete source control such as removal of infected vascular catheter
PO: oral route; cIAI: complicated intra-abdominal infection; cUTI: complicated urinary tract infection |
IV. Pharmacist’s role in managing MDR GNB and MDR GPB infections
The role of the physician, especially an infectious disease (ID) specialist, is generally well understood. The role of the pharmacist as a team member in managing complex MDR infections is less recognized, but highly valuable and worth noting. Pharmacists have a key role in optimizing therapy for MDR GNB and GPB. Pharmacists are integral members of the clinical team who can be readily consulted by physicians and other providers as the drug experts to provide knowledge about appropriate drug selection, dosing, and any other drug-related information crucial to making treatment decisions. There is a unique opportunity to educate health care providers and provide clinical expertise in order to contribute to the management of MDR infections. As the treatment complexity for MDR infections continues to expand, so does the role and value of the pharmacist on the medical team.
Pharmacists have a major role in management of antimicrobial stewardship programs.(Barlam 2016) Antimicrobial stewardship in hospitals around the country has become increasingly important as antimicrobial resistance grows and new antibiotic agents come to market. As presented by the 2019 CDC’s Core Elements of Hospital Antibiotic Stewardship Programs, a pharmacist leader is listed as an essential component along with an ID physician leader.(CDC 2019) While an ID-trained pharmacist may lead the efforts of an antimicrobial stewardship program, pharmacists throughout the hospital are key personnel in carrying out the daily designated duties and cognitive functions such as assessing appropriateness of antibiotic use. Two core components of an antimicrobial stewardship program include preauthorization and/or prospective audit and feedback. Both are areas in which every pharmacist can impact the success of a stewardship program, especially when monitoring the use of newer antibiotic agents. Other key pharmacist-led duties include, but are not limited to, routine education for medical teams and development of clinical guidelines/protocols to systematically improve antibiotic utilization.(Barlam 2016) Lastly, pharmacists have an important role on a hospital’s Pharmacy and Therapeutics Committee where decisions are made about formulary additions and restrictions. A pharmacist’s knowledge about new and emerging antibiotics can be valuable when making decisions about adding new antibiotics to the hospital formulary and their role for hospitalized patients.
PAUSE AND REFLECT: What ways do you see interprofessional collaboration between physicians and pharmacists in your practice?
ID Physician and Pharmacist Discussion
Question 1. Nav, in the monograph, you discuss the role of the pharmacist in managing MDR GNB and GPB infections. How do you as the pharmacist collaborate with infectious disease and other physicians to address issues that are relevant to these infections?
Question 2. Can you discuss how you use shared decision-making to take that next step in working with other HCPs to ensure infection control and prevention objectives can be met?
Question 3. How do each of you integrate antimicrobial stewardship practices when managing patients with COVID-19 co-infection?
Question 4. Pinki, what are your thoughts on the physician’s role relative to infection control to prevent the transmission of MDRO?
Resources
Tamma PD, Aitken SL, Bonomo RA, et al. Infectious Diseases Society of America Antimicrobial Resistant Treatment Guidance: Gram-Negative Bacterial Infections. Clin Infect Dis. 2020 Oct 27:ciaa1478. doi: 10.1093/cid/ciaa1478. Epub ahead of print. PMID: 33106864.
References
Baddour LM, Wilson WR, Bayer AS, et al. Infective endocarditis in adults: diagnosis, antimicrobial therapy, and management of complications. Circulation. 2015;132:1435-86.
Barber KE, Bell AM, Wingler MJB, et al. Omadacycline enters the ring: a new antimicrobial contender. Pharmacotherapy. 2018;38(12):1194-1204.
Barlam TF, Cosgrove SE, Abbo LM, et al. Implementing an Antibiotic Stewardship Program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin Infect Dis. 2016;62:e51-e77.
Bhatt PJ, Shiau S, Brunetti L, et al. Risk factors and outcomes of hospitalized patients with severe COVID-19 and secondary bloodstream infections: a multicenter, case-control study. Clin Infect Dis. 2020;ciaa1748. Advance online publication. https://doi.org/10.1093/cid/ciaa1748.
Boucher HW, Wilcox M, Talbot GH, et al. Once-weekly dalbavancin versus daily conventional therapy for skin infection. N Engl J Med. 2014;370(23):2169-2179.
Britt NS, Potter EM, Patel N, et al. Comparative effectiveness and safety of standard-, medium-, and high-dose daptomycin strategies for the treatment of vancomycin-resistant enterococcal bacteremia among Veterans Affairs patients. Clin Infect Dis. 2017;64:605-613.
Burdette SD, Trotman R. Tedizolid: the first once-daily oxazolidinone class antibiotic. Clin Infect Dis. 2015;61:1315-1321.
Burnett YJ, Echevarria K, Traugott KA. Ceftaroline as salvage monotherapy for persistent MRSA bacteremia. Ann Pharmacother. 2016;50:1051-1059.
Cai T, Mazzoli S, Mondaini N, et al. The role of asymptomatic bacteriuria in young women with recurrent urinary tract infections: to treat or not to treat? Clin Infect Dis. 2012;55(6):771-777.
Cai T, Verze P, Brugnolli A, et al. Adherence to European Association of Urology guidelines on prophylactic antibiotics: an important step in antimicrobial stewardship. European Urology. 2016;69(2):276-283.
Carmeli Y, Armstrong J, Laud PJ, et al. Ceftazidime-avibactam or best available therapy in patients with ceftazidime-resistant Enterobacteriaceae and Pseudomonas aeruginosa complicated urinary tract infections or complicated intra-abdominal infections (REPRISE): a randomised, pathogen-directed, phase 3 study.Lancet Infect Dis. 2016;16(6):661-673.
CDDEP2021a-g. The Center for Disease Dynamics, Economics and Policy. Resistance Map: Antibiotic Resistance. 2021. Available at https://resistancemap.cddep.org/AntibioticResistance.php.
Cefiderocol [prescribing information]. Shionogi Inc. Florham Park, NJ 07932. 2020. Available at https://www.shionogi.com/content/dam/shionogi/si/products/pdf/fetroja.pdf.
Ceftazidime and avibactam [package insert]. Allergan USA, Inc. Madison, NJ 07940. 2018. Available at https://media.allergan.com/actavis/actavis/media/allergan-pdf-documents/product-prescribing/Avycaz_Final_PI_CBE-0_10_2019.pdf.
Ceftolozane/Tazobactam [prescribing information]. Merck & Co., Inc. Whitehouse Station, NJ 08889. 2015-2020. Available at https://www.merck.com/product/usa/pi_circulars/z/zerbaxa/zerbaxa_pi.pdf.
Centers for Disease Control and Prevention. Antibiotic Resistance Threats in the United States, 2019. Available at https://www.cdc.gov/drugresistance/pdf/threats-report/2019-ar-threats-report-508.pdf. Published 2019. [CDC 2019a]
Centers for Disease Control and Prevention. Antibiotic Resistance and Patient Safety Portal, 2018. Available at https://arpsp.cdc.gov/. Last reviewed June 8, 2020.
Centers for Disease Control and Prevention. Antibiotic/Antimicrobial Resistance, 2020. Available at https://www.cdc.gov/drugresistance/index.html Last reviewed July 20, 2020
Centers for Disease Control and Prevention. Core Elements of Hospital Antibiotic Stewardship Programs. Atlanta, GA: US Department of Health and Human Services, CDC; 2019. Available at https://www.cdc.gov/antibiotic-use/healthcare/pdfs/hospital-core-elements-H.pdf.
Centers for Disease Control and Prevention. Healthcare-associated Infections: CRE Technical Information. Available at https://www.cdc.gov/hai/organisms/cre/technical-info.html. Last reviewed November 22, 2019. [CDC 2019b]
Centers for Disease Control and Prevention. Infection Control – Prevention of Transmission of Multidrug Resistant Organisms. Available at https://www.cdc.gov/infectioncontrol/guidelines/mdro/recommendations.html. Last reviewed November 5, 2015.
Chopra T, Marchaim D, Awali RA, et al. Epidemiology of bloodstream infections caused by Acinetobacter baumannii and impact of drug resistance to both carbapenems and ampicillin-sulbactam on clinical outcomes. Antimicrob Agents Chemother. 2013;57(12):6270-6275.
Claeys KC, Smith JR, Casapao AM, et al. Impact of the combination of daptomycin and trimethoprim-sulfamethoxazole on clinical outcomes in methicillin-resistant Staphylococcus aureus infections. Antimicrob Agents Chemother. 2015;59(4):1969-1976.
Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing. 30th ed. CLSI standard M100. Wayne, PA: Clinical and Laboratory Standards Institute; 2020.
Corey GR, Good S, Jiang H, et al. Single-dose oritavancin versus 7-10 days of vancomycin in the treatment of gram-positive acute bacterial skin and skin structure infections: the SOLO II noninferiority study. Clin Infect Dis. 2015;60:254-262.
Corey GR, Kabler H, Mehra P, et al. Single-dose oritavancin in the treatment of acute bacterial skin infections. N Engl J Med. 2014;370:2180-2190.
Dalbavancin [prescribing information]. Allergan USA, Inc. Madison, NJ 07940. 2018. Available at https://media.allergan.com/actavis/actavis/media/allergan-pdf-documents/product-prescribing/Dalvance_Final_PI_10_2018.pdf.
Daptomycin [prescribing information]. Merck Sharp & Dohme Corp. Whitehouse Station, NJ 08889. 2015-2020. Available at https://www.merck.com/product/usa/pi_circulars/c/cubicin/cubicin_pi.pdf.
Delafloxacin [prescribing information]. Melinta Therapeutics, Inc. Lincolnshire, IL 60069. 2017.Available at https://www.baxdela.com/docs/baxdela-prescribing-information.pdf.
Dunne MW, Puttagunta S, Giordano P, et al. A randomized clinical trial of single-dose versus weekly dalbavancin for treatment of acute bacterial skin and skin structure infection. Clin Infect Dis. 2016;62:545-551.
El Lababidi RM and Rizk JG. Cefiderocol: a siderophore cephalosporin. Ann Pharmacother. 2020;54(12):1215-1231.
Eravacycline [prescribing information]. Tetraphase Pharmaceuticals Inc. Watertown, MA 02472. 2020. Available at https://www.xerava.com/assets/pdf/prescribinginformation.pdf.
Falagas ME, Vouloumanou EK, Samonis G, Vardakas K. Fosfomycin. Clin Microbiol Rev. 2016;29(2):321-347.
Finch NA, Zasowski EJ, Murray KP, et al. A quasi-experiment to study the impact of vancomycin area under the concentration-time curve-guided dosing on vancomycin-associated nephrotoxicity. Antimicrob Agents Chemother. 2017;61(12):e01293-01317.
Food and Drug Administration. FDA Drug Safety Communication: FDA advises restricting fluoroquinolone antibiotic use for certain uncomplicated infections; warns about disabling side effects that can occur together, 2016. Available at https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-fda-advises-restricting-fluoroquinolone-antibiotic-use-certain. Last reviewed September 25, 2018.
Gallagher J, Satlin MJ, Elabor A, et al. Ceftolozane-Tazobactam for the treatment of multidrug-resistant Pseudomonas aeruginosa infections: a multicenter study. Open Forum Infect Dis. 2018;5(11):ofy280.
Giacobbe DR, de Rosa FG. Bassetti M, del Bono V. Ceftolozane/tazobactam: place in therapy. Expert Rev Anti Infect Ther. 2018;16(4):307-320.
Harris PNA, Tambyah PA, Lye DC, et al. Effect of piperacillin-tazobactam vs meropenem on 30-day mortality for patients with E coli or Klebsiella pneumoniae bloodstream infection and ceftriaxone resistance: a randomized clinical trial. JAMA. 2018;320(10):984-994.
Heintz BH, Halilovic J, Christensen CL. Vancomycin-resistant enterococcal urinary tract infections. Pharmacotherapy. 2010;30:1136-1149.
Holubar M, Meng L, Alegria W, Deresinski S. Bacteremia due to methicillin-resistant Staphylococcus aureus: an update on new therapeutic approaches. Infect Dis Clin. 2020;34(4):849-861.
https://labeling.pfizer.com/ShowLabeling.aspx?id=649.
Imipenem/Cilastatin/Relebactam [prescribing information]. Merck & Co Inc. Whitehouse Station, NJ 08889. 2019-2020. Available at https://www.merck.com/product/usa/pi_circulars/r/recarbrio/recarbrio_pi.pdf.
Isler B, Doi Y, Bonomo RA, Paterson DL. New treatment options against carbapenem-resistant Acinetobacter baumannii infections. Antimicrob Agents Chemother. 2018;63(1):e01110-1118.
Jernigan JA, Hatfield KM, Wolford H, et al. Multidrug-resistant bacterial infections in US hospitalized patients, 2012–2017. New Engl J Med. 2020;382(14):1309-1319.
Johnson J, Feeney ER, Kubiak DW, et al. Prolonged use of oritavancin for vancomycin-resistant Enterococcus faecium prosthetic valve endocarditis. Open Forum Infect Dis. 2015;2(4):ofv156.
Kallen AJ, Hidron AI, Patel J, et al. Multidrug resistance among gram-negative pathogens that caused healthcare-associated infections reported to the National Healthcare Safety Network, 2006–2008. Infect Control Hosp Epidemiol. 2010;31(5):528-531.
Kassamali Z and Danziger L. To B or not to B, that is the question: Is it time to replace colistin with polymyxin B? Pharmacotherapy. 2015;35:17-21.
Langford BJ, So M, Raybardhan S, et al. Bacterial co-infection and secondary infection in patients with COVID-19: a living rapid review and meta-analysis. Clin Microbiol Infect. 2020;26(12):1622–1629.
Lefamulin [prescribing information]. Nabriva Therapeutics US Inc. King of Prussia, PA 19406. 2019. Available at https://www.xenleta.com/pdf/xenleta-prescribing-information.pdf.
Linezolid [prescribing information]. Pharmacia and Upjohn. New York, NY 10017. 2020. Available at https://labeling.pfizer.com/showlabeling.aspx?id=649.
Liu C, Bayer A, Cosgrove SE, et al. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin Infect Dis. 2011;52:1-38.
Livermore DM, Mushtaq S, Warner M, Woodford N. In vitro activity of eravacycline against carbapenem-resistant Enterobacteriaceae and Acinetobacter baumannii. Antimicrob Agents Chemother. 2016;60(6):3840-3844.
Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268-281.
McCreary E, Kullar R, Geriak M, et al. Multicenter cohort of patients with methicillin-resistant Staphylococcus aureus bacteremia receiving daptomycin plus ceftaroline compared with other MRSA treatments. Open Forum Infect Dis. 2019;7(1):ofz538.
Meropenem/Vaborbactam [prescribing information]. Melinta Therapeutics, Inc. Lincolnshire, IL 60069. 2017. Available at https://www.vabomere.com/media/pdf/vabomere-us-prescribing-information.pdf.
Moise PA, Culshaw DL, Wong-Beringer A, et al. Comparative effectiveness of vancomycin versus daptomycin for MRSA bacteremia with vancomycin MIC >1 mg/L: a multicenter evaluation. Clin Thera. 2016;38(1):16-30.
Moran GJ, Fang E, Corey GR, et al. Tedizolid for 6 days versus linezolid for 10 days for acute bacterial skin and skin-structure infections (ESTABLISH-2): a randomized double-blind, phase 3, non-inferiority trial. Lancet Infect Dis. 2014;14:696-705.
Motsch J, Murta de Oliveira C, Stus V, et al. RESTORE-IMI 1: a multicenter, randomized, double-blind trial comparing efficacy and safety of imipenem/relebactam vs colistin plus imipenem in patients with imipenem-nonsusceptible bacterial infections. Clin Infect Dis. 2020;70:1799-1808.
Neely MN, Youn G, Kato L, Kraler L. Prospective trial on the use of trough concentration versus area under the curve to determine therapeutic vancomycin dosing. Antimicrob Agents Chemother. 2018;62(2):AAC.02042-17.
Nicolle LE, Gupta K, Bradley SF, et al. Clinical practice guideline for the management of asymptomatic bacteriuria: 2019 update by the Infectious Diseases Society of America. Clin Infect Dis. 2019;68(10):e83-e110.
Noval M, Banoub M, Claeys KC, Heil E. The battle is on: new beta-lactams for the treatment of multidrug-resistant Gram-negative organisms. Curr Infect Dis Rep. 2020;22(1).
Novelli A, del Giacomo P, Rossolini GM, Tumbarello M. Meropenem/vaborbactam: a next generation β-lactam β-lactamase inhibitor combination. Expert Rev Anti Infective Ther. 2020;18(7):643-655.
Omadacycline Injection and Tablets [prescribing information]. Allergan USA, Inc. Madison, NJ 07940. 2020. Available at https://media.allergan.com/actavis/actavis/media/allergan-pdf-documents/product-prescribing/Teflaro-USPI-09_2019-2.pdf.
Oritavancin [prescribing information]. Melinta Therapeutics, Inc. Lincolnshire, IL 60069. 2019.Available at https://www.orbactiv.com/pdfs/orbactiv-prescribing-information.pdf.
Paterson DL, Bonomo RA. Extended-spectrum beta-lactamases: a clinical update. Clin Microbiol Rev. 2005;18(4):657-686.
Peleg AY, Hooper DC. Hospital-acquired infections due to gram-negative bacteria. N Engl J Med. 2010;362:1804-1813.
Petty LA, Henig O, Patel TS, et al. Overview of meropenem-vaborbactam and newer antimicrobial agents for the treatment of carbapenem-resistant Enterobacteriaceae. Infect Drug Resist. 2018;11:14611472.
Plazomicin [prescribing information]. Cipla USA, Inc. Warren, NJ. 07059. 2018. Available at https://www.zemdri.com/assets/pdf/Prescribing-Information.pdf.
Pogue JM, et al. Ceftolozane/tazobactam vs polymyxin or aminoglycoside-based regimens for the treatment of drug-resistant Pseudomonas aeruginosa. Clin Infect Dis. 2020;71(2):304-310.
Prokocimer P, De Anda C, Fang E, et al. Tedizolid phosphate vs linezolid for treatment of acute bacterial skin and skin structure infections: the ESTABLISH-1 randomized trial. JAMA. 2013;309:559-569.
Prybylski JP. Vancomycin trough concentration as a predictor of clinical outcomes in patients with Staphylococcus aureus bacteremia: a meta-analysis of observational studies. Pharmacotherapy. 2015;35:889-898.
Rawson TM, Moore LS, Zhu N, et al. Bacterial and fungal co-infection in individuals with coronavirus: a rapid review to support COVID-19 antimicrobial prescribing. Clin Infect Dis. 2020;ciaa530.
Rybak MJ, Le J, Lodise TP, et al. Therapeutic monitoring of vancomycin for serious methicillin-resistant Staphylococcus aureus infections: A revised consensus guideline and review by the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists. Am J Health Syst Pharm. 202077(11):835-864.
Rybak MJ, Lomaestro B, Rotschafer JC, et al. Therapeutic monitoring of vancomycin in adult patients: A consensus review of the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, and the Society of Infectious Diseases Pharmacists. Am J Health Sys Pharm. 2009;66:82-98.
Shields RK, Nguyen MH, Chen L, et al. Ceftazidime-avibactam is superior to other treatment regimens against carbapenem-resistant Klebsiella pneumoniae bacteremia. Antimicrob Agents Chemother. 2017;61(8).
Shields RK, Nguyen MH, Chen L, et al. Pneumonia and renal replacement therapy are risk factors for ceftazidime-avibactam treatment failures and resistance among patients with carbapenem-resistant Enterobacteriaceae infections. Antimicrob Agents Chemother. 2018;62(5):e02497-17.
Smith JR, Claeys KC, Barber KE, et al. High-dose daptomycin therapy for Staphylococcal endocarditis and when to apply it. Curr Infect Dis Rep. 2014;16:429.
Solomkin J, Hershberger E, Miller B, et al. Ceftolozane/tazobactam plus metronidazole for complicated intra-abdominal infections in an era of multidrug resistance: results from a randomized, double-blind, phase 3 trial (ASPECT-cIAI). Clin Infect Dis. 2015;60(10):1462-1471.
Stevens DL, Bisno AL, Chambers HF, et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clin Infect Dis. 2014;59:e10-52.
Stryjewski ME, Graham DR, Wilson SE, et al. Telavancin versus vancomycin for the treatment of complicated skin and skin-structure infections caused by gram-positive organisms. Clin Infect Dis. 2008;46(11):1683-1693.
Stryjewski ME, O'Riordan WD, Chu VH, Warren BL. Telavancin versus standard therapy for treatment of complicated skin and skin structure infections caused by gram-positive bacteria: FAST 2 study. Antimicrob Agents Chemother. 2006;50(3):862-867.
Tamma PD, Aitken SL, Bonomo RA, et al. Inectious Diseases Society of America Antimicrobial Resistant Treatment Guidance: Gram-Negative Bacterial Infections. Clin Infect Dis. 2020 Oct.
Tedizolid [prescribing information]. Merck & Co., Inc. Whitehouse Station, NJ 08889.2015-2020. Available at https://www.merck.com/product/usa/pi_circulars/s/sivextro/sivextro_pi.pdf.
Telavancin [prescribing information]. Cumberland Pharmaceuticals Inc. Nashville, TN 37203. 2020. Available at https://www.vibativ.com/public/pdf/PrescribingInformation.pdf.
Tsai L, Zervos M, Miller L, et al. Intravenous eravacycline with transition to oral therapy for treatment of complicated urinary tract infections including pyelonephritis: Results from a randomized, double-blind, multicenter, phase 3 trial (IGNITE2). Presented at: ASM Microbe; June 16-20, 2016; Boston. Available at https://www.tphase.com/wp-content/uploads/2019/04/Tsai_2016_ASM-Microbe-264.pdf.
Tsuji BT, Pogue JM, Zavascki AP, et al. International Consensus Guidelines for the Optimal Use of the Polymyxins: Endorsed by the American College of Clinical Pharmacy (ACCP), European Society of Clinical Microbiology and Infectious Diseases (ESCMID), Infectious Diseases Society of America (IDSA), International Society for Anti‐infective Pharmacology (ISAP), Society of Critical Care Medicine (SCCM), and Society of Infectious Diseases Pharmacists (SIDP). Pharmacotherapy. 2019;39(1):10-39.
van Duin D, Lok JJ, Earley M, et al. Colistin versus ceftazidime-avibactam in the treatment of infections due to carbapenem-resistant Enterobacteriaceae. Clin Infect Dis. 2018;66(2):163-171.
Vardakas KZ, Tansarli GS, Rafailidis PI, Falagas M. Carbapenems versus alternative antibiotics for the treatment of bacteraemia due to Enterobacteriaceae producing extended-spectrum β-lactamases: a systematic review and meta-analysis. J Antimicrob Chemother. 2012;67(12):2793-2803.
Veve MP, Wagner JL. Lefamulin: Review of a promising novel pleuromutilin antibiotic.
Pharmacotherapy. 2018;38(9):935-946.
Viehman J, Alexander M, Nguyen H, Doi Y. Treatment options for carbapenem-resistant and extensively drug-resistant Acinetobacter baumannii infections. Drugs. 2014;74(12):1315-1333.
Wagenlehner FM, Umeh O, Steenbergen J, et al. Ceftolozane-tazobactam compared with levofloxacin in the treatment of complicated urinary-tract infections, including pyelonephritis: a randomised, double-blind, phase 3 trial (ASPECT-cUTI). Lancet. 2015;385(9981):1949-1956.
Wagenlehner FME, Cloutier DJ, Komirenko AS, et al. Once-daily plazomicin for complicated urinary tract infections. N Engl J Med. 2019;380:729-740.
Watkins RR, Deresinski S. Omadacycline: A novel tetracycline derivative with oral and intravenous formulations. Clin Infect Dis. 2019;69(5):890-896.
White BP, Barber KE, Stover KR. Ceftaroline for the treatment of methicillin-resistant Staphylococcus aureus bacteremia. Am J Health Syst Pharm. 2017;74(4):201-208.
Wilson WR, Kline E, Jones CE, et al. Effects of KPC variant and porin genotype on the in vitro activity of meropenem-vaborbactam against carbapenem-resistant Enterobacteriaceae. Antimicrob Agents Chemother. 2019; 63(3):e02048-18.
Wong D, Nielsen TB, Bonomo RA, et al. Clinical and pathophysiological overview of Acinetobacter infections: a century of challenges. Clin Microbiol Rev. 2017;30(1):409-447.
Wunderink R, Giamarellos-Bourboulis E, Rahav G, et al. Meropenem-vaborbactam vs. best available therapy for carbapenem-resistant Enterobacteriaceae infections in TANGO II: Primary outcomes by site of infection. Open Forum Infect Dis. 2017;4(suppl_1):S536-S537.
Yahav D, Giske CG, Grāmatniece A, et al. New β-lactam-β-lactamase inhibitor combinations. Clin Microbiol Rev. 2020;34(1):e00115-20.
Yamano Y. In vitro activity of cefiderocol against a broad range of clinically important Gram-negative bacteria. Clin Infect Dis. 2019;69(Suppl 7):S544-S551.
Zasowski EJ, Trinh TD, Claeys KC, et al. Multicenter observational study of ceftaroline fosamil for methicillin-resistant Staphylococcus aureus bloodstream infections. Antimicrob Agents Chemother. 2017;61(2):e02015-16.
Zhanel GG, Lawson CD, Adam H, et al. Ceftazidime-avibactam: a novel cephalosporin/β-lactamase inhibitor combination. Drugs. 2013;73(2):159-177.
Back to Top