
Expired activity
Please go to the PowerPak
homepage and select a course.
Getting Up to “Speed” on the Drug Overdose Crisis
Introduction
“We make poison for people who don’t care. We probably have the most unpicky customers in the world.” — Jesse Pinkman in Breaking Bad1
America has a serious drug overdose crisis. Undoubtedly, anyone reading this already knew that. More than 700,000 people in the United States died from a drug overdose between 1999 and 2018.2 In 2017 alone, more than 70,000 people succumbed to a drug overdose.2
The factors contributing to the overdose crisis have shifted over the past two decades. While prescription drug overdoses fueled the epidemic in the early part of the millennium, deaths from prescription drugs have comprised a smaller percentage of the total opioid deaths in the past few years and may be declining overall.3 Nationwide, most overdose deaths still involve opioid drugs, but the major actors have transformed away from prescription drugs to heroin and fentanyl.4 However, non-opioids also pose a significant and growing risk. In 2017, the stimulant methamphetamine was the drug most frequently involved in deaths in 4 of the regions of the United States that include 19 states west of the Mississippi River.5
Overdose deaths due to another central nervous system (CNS) stimulant, cocaine, have also been a major contributor to drug overdose deaths. It consistently ranked as the second or third most frequent cause of drug overdose deaths nationwide for the last decade.4,5 Almost 24,000 people died as a result of CNS stimulants in 2017, far more than the number of heroin or prescription opioid-related deaths, although many CNS stimulant victims used products contaminated with fentanyl.6 Pharmacytaff should recognize that substances other than opioids are significant contributors to the drug overdose problem. Polydrug abuse, including abuse with prescription drugs, is a leading factor in fatalities.
This continuing education activity will review the problem of drug overdose and examine the shifting trends in overdose-related fatalities with an emphasis on CNS stimulants. Pharmacists and pharmacy technicians are rightly mindful of opioid painkiller overuse but also need to pay attention to misuse of other drug classes.
DRUG OVERDOSE DEATHS
Death due to opioid overdose has been termed a national epidemic.7 Through 2017, deaths from drug overdose continued to climb.3 Overdoses claimed 70,277 lives in 2017, continuing a steady 2-decade long increase, although the rate dropped by 4% in 2018.8 The age-adjusted rate of drug overdose deaths in 2017 (21.7 per 100,000) was 3.6 times the rate in 1999; all demographic groups were affected.8
In the early 2000s, prescription opioid analgesics were recognized as the primary driver of the overdose crisis. The last few years have seen the problem shift first to heroin and then to powerful synthetic opioids such as fentanyl, which is now the leading cause of overdose deaths in the United States. As fentanyl overdose deaths soar, overdose from other opioids, especially prescription drugs, are declining. For example, oxycodone was the leading cause of death in 2011, but dropped to sixth place in 2016; hydrocodone dropped from seventh to ninth over the same period.4 While national attention has focused on opioids, other drug classes have become more significant factors in claiming lives.
Replacing Opioids
CNS stimulants are exhibiting a resurgence. Cocaine has consistently been ranked second or third among drugs most frequently involved in overdose death over the past decade.4 The number of cocaine-related deaths more than doubled between 2011 and 2016; they accounted for almost 18% of overdose deaths in 2016, up from about 12% only a few years earlier.4 The age-adjusted rate of drug overdose deaths involving cocaine more than tripled (from 1.4 to 4.5 per 100,000 people) between 2012 and 2018, after having dropped over the previous 5-year period.8
Amphetamines are a class of stimulant drugs that encompasses those prescribed legally to treat conditions such as attention-deficit/hyperactivity disorder, narcolepsy, and obesity and those manufactured illegally. Overdose deaths from amphetamines have surged. Methamphetamine was the eighth leading drug involved in overdose deaths in 2011 and rose to fourth place in 2016, with deaths increasing more than 3.5-fold from 1,887 to 6,762 in that time frame. Nearly half of all drug overdose deaths in 2016 involved methamphetamine as a causative factor. The closely related stimulant amphetamine (the parent drug of the class) also returned to prominence, reappearing among the leading causes of overdose death for the first time in the decade in 2016 in 15th place. It rose to 14th place in 2017.4
The age-adjusted rate of drug overdose deaths involving psychostimulants increased an average of 30% per year from 2012 through 2018, to a rate of 3.9 per 100,000 in 2018.8 By comparison, the age-adjusted fatality rates for heroin and synthetic opioids (e.g., fentanyl) in 2018 were 4.7 and 9.9 per 100,000, respectively.8 Consequently, while national attention has been focused on opioids, which still dominate as causes of overdose death, CNS stimulant abuse has quietly become a new major public health concern.9
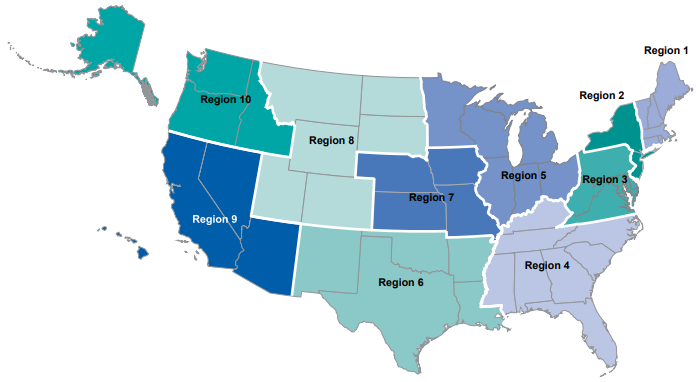
Significantly, while methamphetamine is the fourth leading cause of overdose deaths in the United States as a whole, in many parts of the country, methamphetamine ranked number 1 in 2017.5 The U.S. Department of Health and Human Services divides the country into 10 public health regions (see Figure 1). Fentanyl was the most frequently involved drug in the overdose deaths in 6 of the regions. In the other 4 regions (6, 8, 9, 10), methamphetamine was the drug most frequently involved in overdose deaths and was second in Region 7.5 These 5 regions include almost all of the country west of the Mississippi River. Methamphetamine was involved in 20% to 38% of overdose deaths in these 5 regions. Region 9 (Arizona, California, Hawaii, Nevada) had the highest rate. In contrast, methamphetamine was not among the 10 most frequently implicated drugs in either Region 1 (New England) nor Region 2 (New York/New Jersey); opioids and benzodiazepines predominated in these 2 regions.5
Figure 1. U.S. Department of Health and Human Services Regions5
STIMULANT ABUSE
Although the number of overdose deaths attributable to CNS stimulants is climbing, concern over stimulant abuse is not a new phenomenon. Concerns about amphetamine and methamphetamine were prominent in the 1930s and again in the 1990s. Cocaine dominated news cycles in the early 1900s and 1980s (especially the smoked free-base form known as “crack” because of the sound it emits when burning). Additional nicknames for cocaine, and other street drugs, are found in Table 1.
Before the 20th century, drugs, including cocaine and opium, were widely advertised and readily available; both medical and recreational use was common.10,11 These substances were regulated only at the state level — and many states had no regulations at all.11 The federal government largely limited its health concerns to communicable diseases and provision of health care to government dependents and the merchant marine.11 The federal government had no agencies that regulated medical and pharmaceutical practice, and physicians freely prescribed cocaine and morphine as treatments for pain and other conditions.10
| Table 1. Common Nicknames for Street Drugs12 |
| OPIOIDS & SEDATIVES |
| Benzodiazepines |
benzos, blue V, candy, downers, sleeping pills, tranks |
| Codeine |
Captain Cody, cody, schoolboy: when mixed as a syrup mixed with alcohol: lean, sizzurp, purple drank; when mixed with sedative glutethimide: doors and fours, loads, pancakes and syrup |
Fentanyl
(or fentanyl-laced heroin) |
apache, China girl, China white, dance fever, friend, goodfella, jackpot, murder 8, TNT, Tango & Cash |
| Heroin |
brown sugar, China white, chiva, dope, H, hell dust, horse, junk, negra, skag, skunk, smack, tar, thunder, white horse; when mixed with OTC drugs, cheese |
| Hydrocodone |
hydro, narco, vickies, vike, Watson-387 |
| Hydromorphone |
D, dillies, dust, footballs, juice, smack |
| Methadone |
amidone, fizzies, wafer; when mixed with MDMA: chocolate chip cookies |
| Morphine |
dreamer, emsel, first fine, God’s drug, hows, M, M.S., Miss Emma, Mister Blue, monkey, morf, morpho, unkie, white stuff |
| Oxycodone |
hillbilly heroin, kicker, O.C., oxycet, oxycotton, oxy, percs, roxy |
| STIMULANTS |
| Amphetamine |
bennies, black beauties, crosses, hearts, LA turnaround, speed, truck drivers, uppers |
| Cocaine |
blow, bump, crack, C, Charlie, coke, snow, toot, coca, soda cot, nose candy, dust |
| Ecstasy/MDMA |
Adam, beans, clarity, disco biscuit, E, eve, Molly, lover’s speed, peace, STP, X, XTC, uppers |
| Methamphetamine |
batu, biker’s coffee, black beauties, chalk, chicken feed, crank, crystal, fire, glass, go fast, ice, meth, methlies quick, shards, speed, stove top, tina, trash, tweak, whiz, yellow barn |
| Methylphenidate |
JIF, MPH, R-ball, skippy, the smart drug, vitamin R |
| MDMA=3,4-methylenedioxy-methamphetamine |
Cocaine
Cocaine is derived from the South American coca plant. Indigenous people, especially in the Amazon and Andes regions of South America, have used it for thousands of years for cultural and religious purposes and for the energizing effects from chewing coca leaves.13 Cocaine has also been used medicinally as an anesthetic since the late 1800s.11
Purified cocaine became commercially available in 1884, and problems were recognized soon afterwards.11 However, leading medical experts and popular opinion depicted cocaine as a remarkable, harmless stimulant. Within a year, leading pharmaceutical companies were offering cocaine products for sale, among them Parke-Davis, which offered 15 forms of coca and cocaine, including coca cigarettes.11 In 1886, Coca-Cola was introduced—by a pharmacist14—as a beverage offering the advantages of coca but lacking the danger of alcohol.11 By the end of the 19th century, abuse of cocaine and opium became a significant social issue.10 In 1910, then-President William Howard Taft sent a report to Congress indicating that cocaine posed the most serious drug problem America had ever faced.11
The earliest federal efforts to control the use of drugs was the Harrison Act in 1914, which principally relied on taxation for regulation10 but also made cocaine a prescription drug.11 The demand for cocaine gradually decreased as a result of the new laws and adverse publicity surrounding the drug. In 1930, the New York City Mayor’s Committee on Drug Addiction reported that “during the last 20 years cocaine as an addiction has ceased to be a problem.”11 Increasing use of amphetamines also contributed to reduced cocaine use.14 Of course, that assessment of cocaine did not remain true for long.
In the 1960s, use of many psychoactive substances including cocaine increased.14 Other means of regulatory control followed, and domestic law enforcement became the primary means of controlling the nation’s substance abuse problems.10 Important landmarks in federal oversight of drugs of abuse were the passage of the Controlled Substances Act (CSA) in 1970 and the establishment of the Drug Enforcement Agency (DEA) in 1973 to enforce the CSA. DEA continues to enforce the CSA today. The CSA placed the control of select plants, drugs, and chemical substances under federal jurisdiction and established the now-familiar schedules for substances with abuse potential. Cocaine and the prescription amphetamines were placed in Schedule II at the time the CSA was enacted.10
Cocaine use began to surge again in the 1970s. A glut of cocaine led to markedly lower prices and dealers sought new ways to sell cocaine. A cheaper, smokable form, known as “crack,” made its entrance.14 Crack began to appear in the West Coast of the United States in 1980, spread to other areas of the country, and appeared to plateau by the end of the decade.13 At the peak of the cocaine epidemic in the mid-1980s, experts conservatively estimated that as many as 8 million Americans were using cocaine regularly and that 5% to 8% of them had developed a serious cocaine dependence.14 Federal drug convictions rose sharply between 1980 and 1986. An increase in the number of individuals convicted of federal drug offenses accounted for roughly half of the increase in the total number of convictions for all federal offenses during this period.10
A controversial response to the perceived crack epidemic was the Federal Anti-Drug Abuse Act (1986) which, among other features, established disparate sentencing guidelines for crack and powdered cocaine. The Act set a 100:1 disparity so that selling 5 grams of crack would carry the same penalty as selling 500 grams of powdered cocaine.15 Trafficking in small amounts of crack could result in harsh penalties (5 years in prison), while an equal amount of powdered cocaine would not carry a mandatory sentence. Congress justified this disparity by citing more serious social disruption produced by the more powerful crack and its alleged association with street crime.16
Opponents argued the law was racist.16 Crack has a relatively lower cost and was more accessible to poorer individuals who were more likely to be African American, while powdered cocaine was more expensive and was more likely to be used by more affluent whites. Congress’ intent in passing the Act was to target “serious” and “major” drug traffickers, but the mandatory penalties for crack were most often applied to street-level offenders. In 2010, the Fair Sentencing Act sought to diminish the disparity by reducing the weight ratio to 18:1 and eliminating the mandatory 5-year sentence for crack possession.16
A National Institute on Drug Abuse working group again cited cocaine as the most serious drug problem in the United States in 1994. It identified cocaine as the primary drug of abuse in 10 of the 17 cities reporting, and most drug treatment admissions were due to crack.17
In the 2000s, cocaine’s availability has fluctuated. The Colombian government was engaged in a war with revolutionary forces; it sprayed herbicides aerially and cut crops en masse to eliminate rebel hiding places, effectively reducing cocaine production. After a peace treaty was signed in 2016, cocaine eradication ceased, and production rose to its highest level in a decade. By 2019, the average retail price of cocaine had dropped significantly, and its purity had risen.17 The availability of cheaper, purer cocaine led to an increase in demand. The increasing supplies resulted in an increased prevalence of cocaine use in nearly all sociodemographic groups by the end of the decade, especially among women, Hispanics, and educated and low-income whites.17,18 Another possible factor in the cyclical reemergence of a cocaine—or any drug—problem may be “generational forgetting.” The passage of time erases the memory of a drug’s true risk and its effects on users and society. In addition, newer health professionals lack experience with treating the user.17
Amphetamines
Amphetamine was first synthesized in Germany in 1887 and was introduced into medicine in the 1920s to treat asthma, hay fever, and colds. Smith, Kline & French marketed the 1st amphetamine product, an amphetamine-based over-the-counter (OTC) decongestant inhaler in 1933 under the trade name Benzedrine.19 In 1937, Benzedrine tablets were approved as a prescription drug for treating narcolepsy, postencephalitic parkinsonism, depression, and later for weight loss. During World War II, the United States and British military supplied servicemen with amphetamine. After the War, use and misuse of amphetamine, especially the cheap easily available inhaler, became common.19 By the 1960s, physicians were prescribing large quantities of amphetamines, especially in dubious diet clinics; popularity of illicit stimulant use gained the reputation of “speed kills.”19,20 Amphetamine use peaked in the early 1970s, then declined rapidly to 60% below original rates when the CSA categorized stimulants as Schedule II controlled substances, making them more difficult to prescribe.19
Methamphetamine was first synthesized in Japan in 1893 from the precursor ephedrine.21 It was not widely used until World War II, when German, English, American, and Japanese military personnel were given the drug to enhance endurance and alertness and to ward off fatigue.14
Methamphetamine first gained popularity in the United States in the late 1960s.10 In the 1970s, methamphetamine use was largely confined to California and Oregon, where it was manufactured illicitly mostly by motorcycle gangs and used mostly by Caucasian men. The practice of carrying methamphetamine in the crankcase of a motorcycle gave way to the nickname “crank.”22 In the 1980s, methamphetamine was largely produced by motorcycle gangs in the west and southwest. Use was predominately by Caucasian men (especially truck drivers and blue-collar workers). New forms such as “ice,” which could be heated and inhaled as a vapor similar to “crack,” emerged initially in Hawaii and spread eastward.
Methamphetamine abuse rose in the 1990s as cocaine’s declined.10 Large clandestine labs produced methamphetamine, but home-made meth was also available from numerous small labs located in homes, vehicles, and other locations. These labs were easy for authorities to detect by the strong odor produced during the processing of meth. Production and use became concentrated in rural areas where the labs could be more easily concealed. Meth was commonly produced from legally available precursors such as pseudoephedrine obtained from pharmacies and other retailers. Larger laboratories (“superlabs”) also appeared, especially in western states and Mexico, and the customer base expanded to other demographic groups.22
The Combat Methamphetamine Epidemic Act (CMEA) was enacted in 2006 as a response to growing concern over clandestine methamphetamine manufacture.23 A few years earlier, some states had begun to restrict sales of precursors.24 One of the CMEA’s purposes was to restrict OTC retail sale of methamphetamine precursors, such as products containing ephedrine, pseudoephedrine, and phenylpropanolamine.23 (FDA subsequently withdrew ephedrine and phenylpropanolamine due to their toxicity.) The CMEA’s provisions include23
- Daily sales limits and 30-day purchase limits (3.6 g and 9 g of pseudoephedrine base, respectively)
- Placement of product out of direct customer access
- Sales logbooks
- Customer identification verification using a government-issued form of identification
- Employee training
- Self-certification of sellers
The written or electronic logbook of pseudoephedrine sales must contain the drug’s name and quantity sold; purchaser’s name and address; and date and time of sale, which must be verified by the seller. The purchaser must sign the log. The seller must maintain the log for 2 years. The purchaser must present a state or federal photo identification, although alternatives are acceptable (e.g., Native American tribal document).The seller must verify that the identification corresponds to the information entered into the log.23 Some states (e.g., Oregon) went further and required prescriptions for pseudoephedrine-containing products.
Methamphetamine laboratories declined by nearly one-half in the first few years after the CMEA was enacted. Their prevalence rose again in 2008 due to 2 developments. First, community-based producers developed new techniques for small-scale methamphetamine production. Second, “smurfing” emerged, meaning producers recruited groups of individuals to purchase the legally allowable amount of pseudoephedrine products at multiple stores, and these were aggregated for large-scale production.25 The rise in abuse in the 2000s was also the result of changes in the precursor chemicals being used for synthesis (e.g., phenyl-2-propanone [“P2P”] and methylamine) and the influx of large quantities of meth from Asian sources. There has also been a shift to the smoked crystalline form of meth instead of injectable methods.24
Methamphetamine continues to be readily available throughout the United States. Today, most of the methamphetamine found in the United States is produced clandestinely in large laboratories in Mexico and smuggled across the border; transnational criminal organizations control much of the U.S. supply.24,26 Seizures of domestic methamphetamine laboratories have been declining. The price per gram of methamphetamine decreased more than 13% between January 2012 and March 2017, while its purity increased from 87.9% to 93.2%. 26 The large supply of low-cost, high-purity methamphetamine has helped stimulate the increase in methamphetamine use.26,27
In an effort to curb distribution of methamphetamine, DEA instituted a program in 2020, Operation Crystal Shield. It is directing resources to areas considered transportation hubs where methamphetamine is trafficked in bulk and distributed throughout the United States.28 DEA believes that nearly all the methamphetamine in the United States enters through the southwest border. It is then transported by truck or personal vehicles to major transportation centers around the country. Methamphetamine is often found in multidrug loads alongside other abused substances such as cocaine, heroin, and fentanyl. Operation Crystal Shield efforts are focused on 8 cities: Atlanta, Dallas, El Paso, Houston, Los Angeles, New Orleans, Phoenix, and St. Louis.28
STIMULANT USE AND RISKS
Unlike the sedating opioids, amphetamines and cocaine are CNS stimulants. The dangers associated with stimulants are largely cardiovascular and psychiatric in contrast to the respiratory depression produced by the opioids. Both amphetamines and cocaine exert significant effects on monoamine neurotransmitters; these contribute to their euphoriant effects and toxicity. The amphetamines primarily act by increasing monoamine release, especially dopamine, from presynaptic stores along with some uptake inhibition.29
Methamphetamine has greater effects on the CNS than amphetamine. Methamphetamine crosses the blood-brain barrier more rapidly than amphetamine and has a larger effect on increasing synaptic dopamine concentrations than amphetamine.29,30 Cocaine inhibits catecholamine reuptake and also has a local anesthetic effect (through blockade of sodium and potassium channels) on nerves and the heart. The local anesthetic action can impair cardiac impulse conduction and contractility.31
Pharmacists are reminded that the opioid reversal agent, naloxone, is ineffective in a CNS stimulant overdose situation, unless there is polydrug use (see “New Trends” section below). Naloxone is an opiate receptor antagonist and is effective only against opiate/opioid drugs.
Cocaine
Cocaine and other stimulants may be administered through a variety of routes (oral ingestion, nasal insufflation [snorting], intravenous (IV) injection, inhalation of smoke vapors [smoking/inhalation], and less commonly, vaginally, rectally, or sublingually).14
Generally, smoking and IV use of cocaine rapidly evoke similarly intense responses. Oral ingestion and intranasal administration are slower delivery mechanisms, producing lower and more gradually rising blood levels and less intense subjective responses. With IV cocaine or smoked crack cocaine, a highly concentrated dose is rapidly delivered to the brain; onset of action may occur in as little as 5 to 10 seconds.22 Cocaine’s duration of action is brief, 5 to 20 minutes for nonoral routes.14
Cocaine is seldom taken by mouth in the United States (people in other parts of the world do take it by mouth) since first-pass hepatic biotransformation metabolizes 70% to 80% percent of the dose and substantially diminishes the drug’s effects. Addicts generally consider inhalation to be the most desirable route, since it produces the highest peak drug blood levels and most potent subjective effects without many of the hazards associated with IV injection.
Use of IV street drugs is associated with sharing of unsterile needles which can lead to wound abscess, sepsis, thrombosis, human immunodeficiency virus (HIV) and hepatitis B or C infection, lung infections (tuberculosis, pneumonia), endocarditis, and renal infarction. However, smoking may not produce as intense a “rush” as injection, and crack users complain of throat ailments and a productive cough with black sputum. Nasal insufflation is also associated with adverse effects such as atrophy of the nasal mucosa, nasal septum perforation or necrosis, loss of the sense of smell, sinusitis, nosebleeds, and swallowing problems.14
Cocaine toxicity results in many adverse effects related to its local anesthetic, vasoconstrictive, sympathomimetic, psychoactive, and prothrombotic mechanisms. The drug can affect all organs. The major toxicity is derived from cocaine’s sympathomimetic effects. The most common presentation of cocaine toxicity in hospitals is acute agitation; chest pain is the most frequent cocaine-related complaint in emergency departments. Myocardial ischemia is also common. Among the most severe complications are hemorrhagic and ischemic . Hyperthermia is also observed. Although cocaine’s duration of action is short, it is metabolized to benzoylecgonine and ecgonine methyl ester, which may persist in the body for up to 24 hours, producing prolonged or delayed symptoms.32
Cocaine obtained on the street may be adulterated with other drugs. Common examples include caffeine, diltiazem, hydroxyzine, lidocaine, and phenacetin.33 Dealers may cut drugs to give the impression that the drug is of better quality. Adulterants may mask a poor quality drug by adding substances with similar pharmacologic properties, potentiating the drug’s effects, or mimicking the taste.33 Diluents may also be added to increase profits.32,33 One unusual contaminant found commonly in seized samples is levamisole. This anthelminthic agent and immunomodulator has been used in animals and humans to treat inflammatory conditions and cancer. It can produce leukopenia, agranulocytosis, and vascular complications. Levamisole may enhance catecholamine neurotransmission by inhibiting uptake, metabolism, or ganglionic activity and is partially metabolized to an amphetamine-like compound, thereby heightening CNS stimulants’ effects.34
Methamphetamine
Methamphetamine abuse is most commonly in the form of IV injection, snorting, or smoking as the purified form known as “ice.” The euphoria produced by methamphetamine is longer than that of cocaine, lasting 4 to 6 hours for an IV injection and 8 to 24 hours following inhalation. As with cocaine, IV use of methamphetamine is associated with greater severity of medical and social problems compared with other routes of administration.14
The “high” from methamphetamine both starts and fades quickly. As a result, users often take repeated doses in a “binge and crash” pattern. In some cases, methamphetamine users engage in a form of binging known as a “run,” giving up food and sleep while continuing to take the drug every few hours for up to several days.35
Tachycardia and hypertension are common in methamphetamine users. Methamphetamine abuse is often accompanied by chest pain and accounts for a large proportion of emergency department visits.22,29 Other common emergency department presentations associated with the methamphetamine use are mental health problems, trauma, skin infections, and dental pathology (considered a hallmark indicator of methamphetamine abuse), and less frequently, seizures and stroke.22 Many methamphetamine users develop intracranial hemorrhage and ischemic stroke, and these can induce seizures. Chronic methamphetamine abuse is associated with psychiatric disturbances such as depressive symptoms and suicidal ideation, paranoia, aggressive behavior, psychotic episodes, and self-injurious behaviors.19,29 In some users, psychosis may persist for several months or longer even after sustained abstinence.
Methamphetamine-related mortality is frequently due to catastrophic neurologic or cardiac complications. A study of autopsies found that the most common cause of death in methamphetamine-positive patients was multiorgan system dysfunction, followed by cardiovascular or cerebrovascular disease, traumatic shock, asphyxiation, and exsanguination. Methamphetamine can also indirectly produce death through events such as trauma, homicide, or suicide.29
Studies have provided evidence that chronic methamphetamine use is also associated with substantial neurotoxicity and cognitive impairment.22,29,36 The cognitive impairment includes defects in memory, attention, and executive function. The combination of addiction and impairment frequently contributes to psychosocial issues, including legal issues, high-risk behaviors, and social problems such as loss of family support and housing instability; these have high public health and social costs.36 Methamphetamine abusers also frequently participate in illegal behaviors such as crime and violence that tend to result in increased incarcerations and other contact with the criminal justice system. The majority of U.S. law-enforcement agencies report methamphetamine as their primary drug problem with similar rates of involvement by men and women. Methamphetamine is also associated with a serious risk of child abuse and neglect.22
Methamphetamine users are considered to be among the most difficult patients to treat because of prolonged physiologic and psychological problems resulting from the drug’s neurotoxicity.22 In a news report, a physician at a psychiatric crisis center noted that he can no longer treat patients with schizophrenia because all his time is now spent with people using meth.37
Methamphetamine use may also worsen the progression and consequences of HIV/acquired immunodeficiency syndrome. Studies have suggested that HIV causes more injury to nerve cells and more cognitive problems in people who use methamphetamine than it does in nonusing patients with HIV.35
In addition to increased numbers of deaths, amphetamine-related hospitalizations increased almost 4-fold between 2008 and 2015 after declining in the 3 prior years. The increase in amphetamine-related hospitalizations was larger than hospitalizations associated with other abused substances. Amphetamine use is the 4th most common reason to seek drug treatment in the United States, exceeded only by alcohol, opioids, and marijuana.38
The manufacture and production of methamphetamine itself raises other concerns. Production often results in burn injuries, respiratory problems, poisoning, and fires because of the use of explosive, corrosive, and flammable chemicals. Disposal and spillage of these chemical also poses environmental risks.22
New Trends
A number of new trends have raised concerns about the risks associated with abuse. A dangerous, growing trend is the mixing of stimulants with the highly potent synthetic opioid fentanyl. Fentanyl is more commonly mixed with heroin, compounding the opioid overdose problem, but there has also been an expansion in the mixing of fentanyl with cocaine or methamphetamine.26,39
Mixing methamphetamine or cocaine with heroin to create a “speedball” or “goofball” is a long-time practice; users indicate it creates a prolonged and more intense high than using either drug alone. Users may mistakenly believe that the opposing actions of the 2 drugs will cancel adverse effects.39 Typically, large cocaine and methamphetamine seizures smuggled into the United States do not contain fentanyl or other opioids, but street-level illicit seizures almost always do,6 indicating that local dealers or users themselves combine the drugs.
Stimulants and opioids are usually administered intravenously either together or sequentially.39 An observation underscores the seriousness of this practice: between 2000 and 2015, the rate of cocaine-related deaths involving opioids rose almost 4-fold, while the rate of cocaine-related deaths not involving opioids was slightly lower in 2015 than it was in 2000, after a slight rise earlier in the millennium.40
Users mix methamphetamine with fentanyl to achieve the same effect as traditional “speedballs,” but fentanyl’s high potency increases the danger.26 Data from the Centers for Disease Control and Prevention show that deaths involving methamphetamine or cocaine with opioids substantially increased from 2016 to 2017. Almost two-thirds of opioid overdose deaths in 2018 involved concomitant use of at least 1 common nonopioid drug. This indicates that polydrug abuse is a significant contributor to the current problem of overdose fatalities.41
Suppliers may have mixed stimulants with opioids without the user’s knowledge, thereby increasing the user’s risk of developing opioid dependence.26 The presence of fentanyl could also be the result of sloppy manufacturing or could be a deliberate action intended to create a larger market among individuals who have developed a craving for the new high.42
The incidence of stimulant/fentanyl use had been primarily concentrated in areas with high cocaine use, such as Florida, New York, Massachusetts, and Maryland.26 However, it has now moved into states where opioids predominate, such as Ohio and West Virginia, and to areas where there has not been a major presence of either opioids nor stimulants, such as Arkansas, Washington, and Missouri.26
The co-administration of fentanyl and a stimulant, whether voluntary or involuntary, increases overdose risk. Typically, stimulant users do not consider themselves opioid users and are unlikely to carry naloxone to reverse an opioid overdose, increasing their vulnerability.42 The steepest rise in cocaine-related overdose deaths nationwide was among people 45 to 54 years old, who may be especially vulnerable because of years of declining health from drug use.42
The increasing use of traditional stimulants and the added risk of co-administration of fentanyl are not the only troubling new trends. Newer stimulants (see Table 2) also pose a growing health concern, although not of the same magnitude as cocaine and amphetamines. Synthetic cathinones are usually consumed in pill or capsule form but occasionally are smoked or insufflated. Synthetic cathinones are commonly misrepresented and/or sold as substitutes for MDMA, Molly, Ecstasy, or other substituted amphetamines and are especially popular in the rave and club settings.26
These substances are appealing because they provide users with short boosts of energy and euphoria. A troubling aspect of synthetic stimulants is that users may be unaware of a given product’s contents and potency. This potentially exposes users to additional and potentially serious health risks, compounded by the lack of scientific information about these products’ effects and appropriate treatments when toxicity occurs.26
| Table 2. New Synthetic Stimulants43,44 |
| Drug Class |
Examples |
| Cathinones |
- mephedrone (4-methylmethcathinone)
- methylenedioxypyrovalerone (MDPV)
- methylone (3,4-methylenedioxy-N-methylcathinone)
- “Bath salts”
|
| 2C-phenethylamines |
- 2C-E (Europa, aquarust, hummingbird)
- 2C-B (nexus, 2’s, toonies, bromo, spectrum, venus)
- 2C-T-7 (blue mystic, T7, beautiful, tripstay, tweety-bird mescaline)
- 25I-NBOMe (N-bomb, smiles, 25I, 25C, 25B)
|
BENZODIAZEPINES
Although they are neither stimulants nor opioids, benzodiazepines are increasingly abused agents.45 Overdose deaths related to benzodiazepines rose more than 4-fold between 1996 and 2013. Emergency department visits also increased 3-fold for benzodiazepines over a similar period (2004 to 2011). Pharmacists may have noticed a corresponding increase in benzodiazepine prescribing during this time frame; the number of prescribed benzodiazepines dosage units increased 3-fold between 2004 and 2011.45,46 Significantly, the proportion of patients who were prescribed a benzodiazepine along with an opioid analgesic increased
Research indicates that people who abused benzodiazepines and opioids together were more likely to be using opioids for a longer period of time, using higher doses of opioids and were more likely to be polydrug abusers compared with people who used only opioids.47 While benzodiazepines rarely cause clinically significant respiratory depression on their own, they can worsen opioid-induced respiratory depression and can markedly increase the risk of overdose death from opioids.46,47 In 2015, 23% of people who died of an opioid overdose also tested positive for benzodiazepines, and a North Carolina study found that people who received prescriptions for an opioid and a benzodiazepine were 10 times more likely to die than people who received an opioid alone.49
Users are also increasingly combining benzodiazepines with stimulants (amphetamines, cocaine, “Ecstasy”) to lessen some of their undesirable effects (e.g., anxiety, irritation, insomnia).45,50 This is yet another example of the growing risk of polydrug abuse. Pharmacists should be on the alert for the combined prescribing and use of these drugs and signs of benzodiazepine diversion.48
CONCLUSION
Concern about drug abuse and its consequences have existed for more than a century. Over the past 2 decades, overdose deaths have become the leading cause of accidental deaths in the United States.51 The current focus on overdose deaths is on opioids, which continue to be a major cause of overdose fatalities. Prescription opioids dominated in the early 2000s, but fentanyl and its more potent analogs now pose the greatest overall threat nationally. Pharmacists have seen a decline in the number of opioid prescriptions, and deaths from drug overdose declined by 4% in 2018, reversing a 20-year trend.8 However, pharmacists must not be misled into thinking that the drug abuse problem is synonymous with opioids and that reducing prescription opioid prescribing and dispensing will eliminate the problem.
Instead, as health care professionals, pharmacists must recognize that the number of overdose deaths remains high and that the nature of substance abuse is changing. In part, this results partly from a shift to nonopioid products, especially CNS stimulants that have become the leading causes of overdose deaths in some areas of the United States. Two previous instances of a rise in abuse of amphetamines in the 20th century were due, in part, to the selling, prescribing, and dispensing of OTC decongestants and prescription diet drugs. More recently, illegal methamphetamine production from OTC pseudoephedrine has contributed to abuse of stimulants. These examples show how pharmacists can be directly involved in the proliferation of abuse, even unwittingly or unwillingly. Users in the current epidemic primarily use methamphetamine illegally manufactured in large quantities in other countries, especially Mexico, and smuggled into the United States. Cocaine has also witnessed an ebb and flow in the seriousness of the overdose problem over the past century. These trends illustrate that pharmacists must remain vigilant about stimulant misuse.
More relevant to pharmacists is that prescription drugs remain an important cause of drug overdoses. Pharmacists are no doubt familiar with the frequent use of benzodiazepines, as many have observed an uptick in prescribing. One addiction specialist has warned that what is being seen today with benzodiazepines is reminiscent of what occurred with opioids in the 1990s.52 Overprescribing of agents tends to normalize their use among patients, who start to believe the medications are safe regardless of where they obtain them or how much they use. Most troubling today is the increase in prescribing and use of benzodiazepines in combination with other drugs, especially opioids. Some states have responded by enacting prescribing guidelines for benzodiazepines similar to guidelines for opioids. Pharmacists should expect more states to follow.
Pharmacists must remain vigilant for misuse and diversion of all controlled substances, not just opioids, and be active participants in the national debate on the ramifications of drug abuse and strategies for mitigation.
References
- The i Paper. “30 of the Best Walter White and Jesse Pinkman quotes from Breaking Bad ahead of El Camino’s release.” September 27, 2019. Available at: https://inews.co.uk/culture/television/walter-white-quotes-breaking-bad-jesse-pinkman-el-camino-release-637665. Accessed on: May 12, 2020.
- National Institute on Drug Abuse. Overdose Death Rates. March 2020. Available at: https://www.drugabuse.gov/related-topics/trends-statistics/overdose-death-rates, May 12, 2020.
- Hedegaard H, Miniño AM, Warner M. Drug overdose deaths in the United States, 1999–2017. NCHS Data Brief, no 329. Hyattsville, MD: National Center for Health Statistics. November 2018. Available at: https://www.cdc.gov/nchs/products/databriefs/db329.htm. Accessed on: May 12, 2020.
- Hedegaard H, Bastian BA, Trinidad JP, Spencer MR, Warner M. Drugs most frequently involved in drug overdose deaths: United States, 2011–2016. National Vital Statistics Reports; vol 67 no 9. Hyattsville, MD: National Center for Health Statistics. December 12, 2018. Available at: https://www.cdc.gov/nchs/data/nvsr/nvsr67/nvsr67_09-508.pdf. Accessed on: May 13, 2020.
- Hedegaard H., Bastian BA, Trinidad JP, Spencer MR, Warner M. Regional Differences in the Drugs Most Frequently Involved in Drug Overdose Deaths: United States, 2017. National Vital Statistics Reports; vol 68 no 12. Hyattsville, MD: National Center for Health Statistics. October 12, 2019. Available at: https://www.cdc.gov/nchs/data/nvsr/nvsr68/nvsr68_12-508.pdf. Accessed on: May 13, 2020.
- Vestal C. The Pew Charitable Trusts. As the Opioid Crisis Peaks, Meth and Cocaine Deaths Explode. May 13, 2019. Available at: https://www.pewtrusts.org/en/research-and-analysis/blogs/stateline/2019/05/13/as-the-opioid-crisis-peaks-meth-and-cocaine-deaths-explode. Accessed on: May 13, 2020.
- U.S. Department of Health and Human Services. What is the U.S. Opioid Epidemic? September 4, 2019. Available at: https://www.hhs.gov/opioids/about-the-epidemic/index.html. Accessed on: May 13, 2020.
- Hedegaard H, Miniño AM, Warner M. Drug overdose deaths in the United States, 1999–2018. NCHS Data Brief, no 356. Hyattsville, MD: National Center for Health Statistics. January 2020. Available at: https://www.cdc.gov/nchs/products/databriefs/db356.htm. Accessed on: May 13, 2020.
- Al-Tayyib A, Koester S., Langegger S, Raville L. Heroin and methamphetamine injection: an emerging drug use pattern. Subst Use Misuse. 2017;52(8):1051-1058.
- Sacco LN. Drug Enforcement in the United States: History, Policy, and Trends. Congressional Research Service. October 2, 2014. Available at: https://fas.org/sgp/crs/misc/R43749.pdf. Accessed on: May 13, 2020.
- Musto DF. Opium, cocaine and marijuana in American history. Sci Am. 1991;265(1):40-47.
- DrugAbuse.com: American Addiction Centers. List of Street Names for Drugs. Available at: https://drugabuse.com/addiction/list-street-names-drugs/. Accessed on: May 13, 2020.
- DrugAbuse.com: American Addiction Centers. Crack History and Statistics. Available at: https://drugabuse.com/crack-history-and-statistics/. Accessed on: May 13, 2020.
- Substance Abuse and Mental Health Services Administration. Treatment for Stimulant Abuse Disorders. Treatment Improvement Protocol (TIP) Series, No. 33. 1999. Available at: https://www.ncbi.nlm.nih.gov/books/NBK64333/. Accessed on: May 13, 2020.
- GovTrack.us. H.R. 5484 (99th): Anti-Drug Abuse Act of 1986. Available at: https://www.govtrack.us/congress/bills/99/hr5484. Accessed on: May 13, 2020.
- American Civil Liberties Union. Cracks in the System: Twenty Years of the Unjust Federal Crack Cocaine Law. October 2006. Available at: https://www.aclu.org/sites/default/files/pdfs/drugpolicy/cracksinsystem_20061025.pdf. Accessed on: May 13, 2020.
- Maxwell JC. Is cocaine coming back? a commentary. Subst Use Misuse. 2020;55(2):345-348.
- Kerridge BT, Chou SP, Pickering RP, et al. Changes in the prevalence and correlates of cocaine use and cocaine use disorder in the United States, 2001-2002 and 2012-2013. Addict Behav. 2019;90:250-257.
- Rasmussen N. America’s first amphetamine epidemic 1929–1971: a quantitative and qualitative retrospective with implications for the present. Am J Public Health. 2008;98(6): 974-985.
- Owen F. No Speed Limit: The Highs and Lows of Meth. New York: St. Martin’s Griffin; 2007.
- MethOIDE. The University of Arizona Family & Community Medicine. Origin and History. Available at: https://methoide.fcm.arizona.edu/infocenter/index.cfm?stid=164. Accessed on: May 13, 2020.
- Gonzales R. Mooney L, Rawson RA. The methamphetamine problem in the United States. Annu Rev Public Health. 2010;31:385-398.
- U.S. Drug Enforcement Administration. CMEA (Combat Methamphetamine Epidemic Act). Available at: https://www.deadiversion.usdoj.gov/meth/q_a_cmea.htm. Accessed on: May 13, 2020.
- Maxwell JC, Brecht ML. Methamphetamine: here we go again? Addict Behav. 2011;36(12):1168–1173.
- United States Government Accountability Office. State Approaches Taken to Control Access to Key Methamphetamine Ingredient Show Varied Impact on Domestic Drug Labs. January 2013. Available at: https://www.gao.gov/assets/660/651709.pdf. Accessed on: May 13, 2020.
- U.S. Department of Justice, Drug Enforcement Administration. 2018 National Drug Threat Assessment. October 2018. Available at: https://www.dea.gov/sites/default/files/2018-11/DIR-032-18%202018%20NDTA%20final%20low%20resolution.pdf. Accessed on: May 13, 2020.
- Shukla RK, Crump JL, Chrisco ES. An evolving problem: methamphetamine production and trafficking in the United States. Int J Drug Policy. 2012;23(6):426-435.
- U.S. Department of Justice. DEA Announces Launch of Operation Crystal Shield. February 20, 2020. Available at: https://www.justice.gov/opa/pr/dea-announces-launch-operation-crystal-shield. Accessed on: May 13, 2020.
- Vearrier D, Greenberg MI, Miller SN, et al. Methamphetamine: history, pathophysiology, adverse health effects, current trends, and hazards associated with the clandestine manufacture of methamphetamine. Dis Mon. 2012;58(2):38-89.
- Goodwin JS, Larson GA, Swant J, et al. Amphetamine and methamphetamine differentially affect dopamine transporters in vitro and in vivo. J Biol Chem. 2009;284(5):2978-2989.
- Billman GE. Cocaine: a review of its toxic actions on cardiac function. Crit Rev Toxicol. 1995;25(2): 113-132.
- Zimmerman JL. Cocaine intoxication. Crit Care Clin. 2012;28(4):517-526.
- Broséus J, Gentile N, Esseiva P. The cutting of cocaine and heroin: a critical review. Forensic Sci Int. 2016;262:73-83.
- Larocque A, Hoffman RS. Levamisole in cocaine: unexpected news from an old acquaintance. Clin Toxicol. 2012;50(4):231-241.
- National Institute on Drug Abuse. Methamphetamine. Revised May 2019. Available at: https://www.drugabuse.gov/publications/drugfacts/methamphetamine. Accessed on: May 13, 2020.
- Panenka WJ, Procyshyn RM, Lecomte T, et al. Methamphetamine use: a comprehensive review of molecular, preclinical and clinical findings. Drug Alcohol Depend. 2013;129(3):167-179.
- Goodnough A. New York Times. A New Drug Scourge: Deaths Involving Meth Are Rising Fast. December 17, 2019. Available at: https://www.nytimes.com/2019/12/17/health/meth-deaths-opioids.html. Accessed on: May 13, 2020.
- Winkelman TNA, Admon LK, Jennings L, et al. Evaluation of amphetamine-related hospitalizations and associated clinical outcomes and costs in the United States. JAMA Netw Open. 2018;1(6):e183758.
- Ellis MS, Kasper ZA, Cicero TJ. Twin epidemics: the surging rise of methamphetamine use in chronic opioid users. Drug Alcohol Depend. 2018;193:14-20.
- Jones CM, Baldwin GT, Compton WM. Recent increases in cocaine-related overdose deaths and the role of opioids. Am J Public Health. 2017;107(3):430-432.
- Gladden RM, O’Donnell J, Mattson CL, Seth P. Changes in opioid-involved overdose deaths by opioid type and presence of benzodiazepines, cocaine, and methamphetamine — 25 states, July-December 2017 to January-June 2018. MMWR Morb Mortal Wkly Rep. 2019;68(34):737-744.
- Ungar L. Kaiser Health News. Not Yesterday’s Cocaine: Death Toll Rising From Tainted Drug. November 25, 2019. Available at: https://khn.org/news/not-yesterdays-cocaine-death-toll-rising-from-tainted-drug/?utm_source=&utm_medium=email&utm_campaign=26240. Accessed on: May 13, 2020.
- United Nations Office on Drug and Crime. World Drug Report 2019: Booklet 4. June 2019. Available at: https://wdr.unodc.org/wdr2019/prelaunch/WDR19_Booklet_4_STIMULANTS.pdf. Accessed on: May 13, 2020.
- Keller A. DrugRehab.com By Advanced Recovery Systems. 2C-E and Other 2C Drugs. Available at: https://www.drugrehab.com/addiction/drugs/hallucinogens/2c-e/. Accessed on: May 13, 2020.
- Votaw VR, Geyer R, Rieselbach MM, McHugh RK. The epidemiology of benzodiazepine misuse: a systematic review. Drug Alcohol Depend. 2019;200:95-114.
- Hwang CS, Kang EM, Kornegay CJ, et al. Trends in the concomitant prescribing of opioids and benzodiazepines, 2002-2014. Am J Prev Med. 2016;51(2):151-160.
- Calcaterra SL, Severtson SG, Bau GE, et al. Trends in intentional abuse or misuse of benzodiazepines and opioid analgesics and the associated mortality reported to poison centers across the United States from 2000 to 2014. Clin Toxicol. 2018;56(11):1107-1114.
- Maust DT, Lin LA, Blow FC. Benzodiazepine use and misuse among adults in the United States. Psychiatr Serv. 2019;70(2):97-106.
- National Institute on Drug Abuse. Benzodiazepines and Opioids. Revised March 2018. Available at: https://www.drugabuse.gov/drugs-abuse/opioids/benzodiazepines-opioids. Accessed on: May 13, 2020.
- O’Brien CP. Benzodiazepine use, abuse, and dependence. J Clin Psychiatry. 2005;66 Suppl 2:28-33.
- Centers for Disease Control and Prevention. Opioid Overdose. Revised May 5, 2020. Available at: https://www.cdc.gov/drugoverdose/index.html. Accessed on: May 13, 2020.
- Vestal C. The Pew Charitable Trusts. These Pills Could Be Next U.S. Drug Epidemic, Public Health Officials Say. July 18, 2018. Available at: https://www.pewtrusts.org/en/research-and-analysis/blogs/stateline/2018/07/18/these-pills-could-be-next-us-drug-epidemic-public-health-officials-say. Accessed on: May 13, 2020.
Back to Top