
Expired activity
Please go to the PowerPak
homepage and select a course.
Nephrology Rounds: The Role of the Pharmacist in the Management of Anemia in Chronic Kidney Disease Patients
INTRODUCTION
Anemia is common in patients with chronic kidney disease (CKD) and contributes to increased morbidity and mortality, especially in advanced stages.1 The treatment of anemia in patients with CKD is often challenging due to concerns about the safety of current agents, patient variation in responses to current agents, lack of agreement on treatment targets, debate regarding how to integrate a patient-centric approach in the context of one-size-fits-all algorithms, and suboptimal coordination between members of the healthcare team managing the anemia. Current treatment options of iron supplementation and erythropoiesis stimulating agents (ESAs) may be challenged in the near future by hypoxia inducible factor prolyl-hydroxylase (HIF-PH) inhibitors which are currently under development.2 Pharmacists will play a critical role on the interprofessional team to provide direct patient care, educate other healthcare professionals, make formulary decisions, and design treatment algorithms that integrate existing and potentially new therapies to optimize care for CKD patients. The goal of this activity is to enhance pharmacist understanding of the pathophysiologic processes that contribute to anemia in patients with CKD, the scientific and clinical rationales for targeting prolyl hydroxylase (PH) , and current evidence supporting the potential for HIF stabilization/PH inhibition to address unmet needs among patients with CKD anemia so they may be better prepared to perform their role as a members of the interprofessional team caring for patients with CKD.
SECTION 1: Anemia in Chronic Kidney Disease
Epidemiology of Anemia in CKD
Chronic kidney disease is a slow, progressive loss of kidney function. While it’s estimated that 15% of the general population in the United States (US) is affected, CKD may be more widespread than is recognized as it often has no symptoms and goes undetected and undiagnosed until the disease is well advanced.3 It is not uncommon for a person to have lost up to 50% of renal mass before changes in serum creatinine occur and therefore, when CKD is first detected.4 High blood pressure and diabetes are the primary causes of CKD, and it often occurs within the context of multiple comorbidities. Almost half of individuals with CKD also have diabetes and self-reported cardiovascular disease (CVD).5 CKD is staged according to estimated glomerular filtration rate (eGFR) and degree of urinary albumin excretion (UAE; Table 1).
| Table 1. Staging of chronic kidney disease |
| Stage |
eGFR (ml/min/1.73 m2) |
UAE (mg/day) |
| G1 |
≥90 |
|
| G2 |
60-89 |
|
| G3a |
45-59 |
|
| G3b |
30-44 |
|
| G4 |
15-29 |
|
| G5 |
<15 |
|
| A1 |
|
<30 |
| A2 |
|
30-300 |
| A3 |
|
>300 |
| “G” stage refers to glomerular filtration rate ─ lower eGFR indicates worse stage of disease; “A” stage refers to the degree of albuminuria ─ higher degree of albuminuria indicates high risk of CKD progression; eGFR: estimated glomerular filtration rate; UAE: urinary albumin excretion. Staging according to the 2012 Kidney Disease Improving Global Outcomes Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease.6 |
Chronic kidney disease is slightly more common in women than in men (16% vs 13%) and is estimated to be more common in non-Hispanic blacks than in non-Hispanic whites (18% vs 13%). Compared to Caucasians, African Americans are 3 times more likely to develop end-stage renal disease (ESRD) and Hispanic Americans are 35% more likely to develop ESRD than non-Hispanics.3,5
Each year, kidney disease kills more people than breast or prostate cancer.5,7 In patients with advanced CKD, complications associated with anemia and oxygen delivery contribute to increased morbidity and mortality.1 Cardiovascular disease, for example, is a common and serious complication that is inherently linked to insufficient tissue oxygenation.8
Pathogenesis of Anemia in CKD
As the glomerular filtration rate (GFR) declines, complications of CKD become more prevalent and more problematic. Anemia typically develops once the GFR falls below 45 ml/min/1.73 m2 and is present in >50% of patients once the GFR is less than 15 ml/min/1.73 m2.9 The cause of anemia in patients with CKD is multifactorial, but primarily driven by decreased production of erythropoietin, a hormone that stimulates red blood cell production (see section below for further discussion). Other mechanisms include iron deficiency, systemic inflammation, blood loss, and decreased red blood cell lifespan.2,9
Iron is a necessary co-factor in the production of hemoglobin, the oxygen carrying protein in red blood cells. Iron deficiency contributes to anemia of CKD and can be absolute or functional in nature. In absolute deficiency, there are insufficient stores and/or circulating iron available for erythropoiesis, slowing the formation of new red blood cells. Functional iron deficiency occurs when iron cannot be extracted from its stores to be utilized for erythropoiesis. Under normal physiologic conditions, small amounts of iron (~1 mg/day) are absorbed via the gastrointestinal tract. After uptake into the enterocyte, ferroportin transports iron into the bloodstream where it binds transferrin. Transferrin bound iron travels throughout the bloodstream, providing iron for hemoglobin synthesis in the bone marrow and storing iron as ferritin in the liver and reticuloendothelial macrophages.
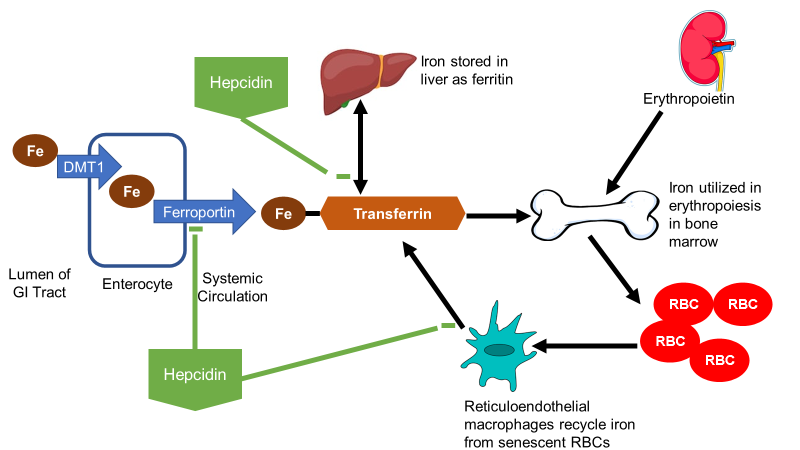
Figure 1. Erythropoiesis, iron metabolism, and hepcidin. Iron is transported into enterocytes by Divalent Metal Transporter 1 (DMT). Ferroportin is the efflux transporter responsible for iron absorption into systemic circulation. Here, transferrin binds free iron to transport it to the liver for storage as ferritin and bone marrow for incorporation into hemoglobin in proerythroblasts. Erythropoietin is produced by the kidney which is the first stimulus to the bone marrow to produce new red blood cells (RBCs). As RBCs meet their lifespan, iron is recycled into reticuloendothelial macrophages which can transfer the iron back to transferrin via ferroportin. Hepcidin is a hormone produced by the liver in response to increasing systemic iron and inflammation. It causes internalization of ferroportin, thereby inhibiting iron absorption from the GI tract and inhibiting iron utilization from storage forms. 10-12
Ferroportin also regulates iron release from stores as it is present on hepatocytes and macrophages. The role of hepcidin in regulating iron absorption and utilization has become a focus of new therapeutic modalities. Hepcidin is a hormone produced in the liver that binds ferroportin, causing internalization, thereby preventing iron absorption at the enterocyte and preventing iron utilization from stores.13 Hepcidin is increased by inflammation and increased systemic iron exposure as a homeostatic feedback loop to prevent iron overload. In CKD, hepcidin is increased due to decreased renal elimination as well as chronic inflammation which leads to both absolute (decreased iron absorption from the gastrointestinal tract) and functional (decreased iron release from macrophage and hepatocyte stores) iron deficiency.14
Anemia in CKD is also regulated by hypoxia-inducible factor (HIF). HIF is a group of endogenous transcription factors that responds to tissue hypoxia by increasing erythropoietin production, increasing erythropoietin receptor expression, decreasing hepcidin production, increasing DMT1 expression, and increasing transferrin receptor expression on proerythrocytes. The net result of these transcriptional changes are increased iron absorption, iron utilization, and erythropoiesis.2 Under normal oxygen environment, HIF is rapidly degraded by prolyl hydroxylase (PH) into an inactive form; under hypoxic conditions, however, it is activated (Figure 2).
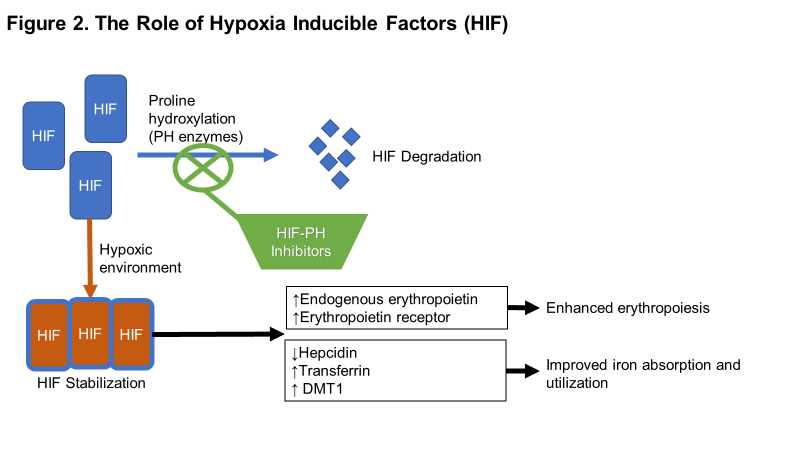
Figure 2. The role of hypoxia-inducible factors in erythropoiesis. Prolyl hydroxylase (PH) enzymes rapidly degrade HIF subunits in the presence of oxygen. Inhibition of HIF-PH mimics the hypoxic environment, whereby HIF subunits are stabilized and cause transcription and subsequent translation of erythropoietic response as indicated. 2
Erythropoiesis and CKD Anemia
The major driver of anemia in patients with CKD is decreased production of erythropoietin, a hormone normally produced by the peritubular interstitial cells of the kidney. As renal mass declines (measured by declining GFR), so does production of erythropoietin. Under normal physiologic conditions, erythropoietin stimulates proerythroblasts in the bone marrow to differentiate ultimately into new red blood cells.12 This process of erythropoiesis is disrupted in CKD leading to decreased formation of new red blood cells.
A number of other factors augment erythropoiesis. Availability of iron for erythropoiesis is one of the most critical and becomes dysregulated in CKD (as above). Decreased folate, decreased vitamin B12, hyperparathyroidism, aluminum toxicity, and use of angiotensin converting enzyme inhibitors (ACEi) are other factors that disrupt erythropoiesis in CKD and diminish response to erythropoiesis stimulating agents.
Clinical Manifestations
The severity of anemia correlates with the clinical manifestations. In most patients, fatigue will set in as the hemoglobin declines below 12 to 13 g/dL and the severity of fatigue increases as hemoglobin declines. Other symptoms that may develop as hemoglobin continues to decline include dyspnea, orthopnea, headache, and cold intolerance. Signs of anemia include decreased red blood cell count, decreased hemoglobin/hematocrit, tachycardia, and pallor.
While every organ system is at risk of hypoxic damage, the heart is particularly susceptible to chronic anemia. Over time, left ventricular hypertrophy will develop in patients with anemia which can contribute to new or worsening heart failure. Anemia and CKD are each independent risk factors for death due to cardiovascular disease.15
The case example with questions and faculty commentary that follows will tie back to this section, illustrating how key concepts might be applied by the care team and its members in the clinical setting.
CASE 1a, Bill
Bill is a 55-year old office worker with stage G4 A3 CKD secondary to type 2 diabetes mellitus who is seen in the nephrology clinic for routine follow up of his CKD. His history also includes hypertension and heart failure with preserved ejection fraction. He complains of frequent fatigue and shortness of breath but denies chest pain. Medications include: lisinopril 40 mg PO daily, carvedilol 12.5 mg PO twice daily, empagliflozin 100 mg PO daily, metformin 1000 mg PO twice daily, and furosemide 40 mg PO daily. His physical exam reveals blood pressure 148/92 mm Hg and 2+ pedal edema, but is otherwise unremarkable. Laboratory data include normal electrolytes, blood urea nitrogen (BUN) 45 mg/dL, creatinine 2.4 mg/dL, estimated GFR (eGFR) 22 ml/min/1.73 m2, Hb 8.9 g/dL, normal white blood cell (WBC) and platelet counts.
CASE QUESTIONS
PAUSE AND REFLECT: Assess this case and consider the case questions based on the activity content thus far, then listen to the faculty commentary.
- What clinical manifestations of anemia does Bill have?
- What are the likely mechanisms of anemia in Bill?
- What other laboratory parameters would be useful to evaluate Bill’s anemia?
- What long-term complications of anemia is Bill at high risk of developing?
|
SECTION 2: Current and Emerging Strategies to Address Anemia in CKD
Iron Therapy
Iron supplementation is required in absolute iron deficiency and can be administered via oral or intravenous routes. Available formulations of oral iron differ in their respective elemental iron content (Table 2). Bioavailability is poor; generally, 10-15% of elemental iron is absorbed. This process is dependent on the presence of gastric acid. Medications that reduce gastric pH (e.g., proton pump inhibitors, histamine2 receptor blockers) and certain foods (e.g., calcium rich foods, eggs) decrease oral iron absorption. It is recommended that patients take iron on an empty stomach for this reason, but if gastrointestinal side effects are limiting adherence, it can be taken with food (bioavailability will be reduced). Ascorbic acid may be administered concomitantly with oral iron supplementation to increase bioavailability.16 Ascorbic acid is proposed to increase the reduction of ferric to ferrous iron, facilitating transport via DMT1 on the apical membrane of enterocytes. Oral iron therapy is complicated by frequent gastrointestinal adverse effects; stomach cramping, constipation, nausea, metallic taste, and dark colored stool are all common.17 Non-adherence is a major concern as 40-60% of patients stop taking oral iron due to adverse effects and frequency of dosing.18,19 Drug-drug interactions are a concern with oral iron as well because of its propensity to adsorb other medications in the gastrointestinal tract, thereby preventing absorption. The absorption of fluoroquinolones, tetracyclines, levofloxacin, and bisphosphonates are all reduced when taken with iron supplements. Oral iron should be initiated in patients with non-dialysis CKD and mild-to-moderate iron deficiency. The recommended dosing for adults is 200 mg of elemental iron per day, in two or three divided doses. It may take 3-6 months for complete repletion of iron stores with oral iron therapy. However, oral iron is inexpensive and more convenient than intravenous administration.
| Table 2. Comparison of oral iron products |
| Oral Iron Product (Brand name) |
Dose (Iron Content) mg |
Elemental Iron (%) |
| Ferrous sulfate |
325 (65)
195 (39) |
20 |
| Ferrous sulfate ER |
525 (105) |
20 |
| Ferrous fumarate |
325 (107)
195 (64) |
33 |
| Ferrous gluconate |
325 (39) |
12 |
| Polysaccharide iron |
150 (150)
50 (50) |
100 |
Ferric citrate
(Auryxia) |
210 (210) |
100 |
Intravenous iron is the preferred route of administration in dialysis-dependent CKD patients, those with severe deficiency, or those that have failed a 3-6-month trial of oral iron. Table 3 summarizes the different intravenous iron products available in the US. Intravenous iron is complicated by infusion reactions. These can range from flushing and headache to altered hemodynamics (hypotension and hypertension are possible) to anaphylaxis. Anaphylaxis is most concerning for dextran formulations. Non-dextran formulations have a low risk of anaphylaxis, with iron sucrose being the lowest.20 Another concern with intravenous iron is a risk of infectious disease. Intravenous iron can slow innate immune response and increase bacterial growth, properties that create a theoretical risk of increased infection.21 While clinical data are conflicting on whether routine intravenous iron administration actually imparts a higher risk of infection in these patients, it is prudent to avoid intravenous iron in patients with an active systemic infection.
| Table 3. Comparison of intravenous iron products |
Iron Formulation
(Brand Name) |
Elemental Iron Content |
Standard Dosing |
Low-molecular-weight
iron dextran
(InFed) |
50 mg/mL |
100 mg/2 minutes |
Ferric gluconate
(Ferrlecit) |
12.5 mg/mL |
125 mg/10-60 minutes |
Iron sucrose
(Venofer) |
20 mg/mL |
100 mg/2-30 minutes |
Ferumoxytol
(Feraheme) |
30 mg/mL |
510 mg/>1 minute |
Ferric carboxymaltose
(Injectafer) |
50 mg/mL |
750 mg/15-30 minutes |
Initiation of iron therapy is dependent upon degree of anemia and iron deficiency. Laboratory parameters that are used to evaluate iron deficiency are shown in Table 4. The Kidney Disease Improving Global Outcomes (KDIGO) Clinical Practice Guideline for Anemia in Chronic Kidney Disease recommend initiating iron supplementation in adults if transferrin saturation (TSAT) is ≤30% and ferritin is ≤500 ng/ml.22
| Table 4. Iron laboratory parameters |
| Laboratory Parameter |
Normal Range |
Interpretation |
| Serum iron |
50-150 mcg/dL |
Amount of iron bound to transferrin |
| Serum ferritin |
>10-20 ng/mL |
Storage form of iron |
| Total iron binding capacity (TIBC) |
250-410 mcg/dL |
Capacity of transferrin to bind iron |
| Transferrin saturation (TSAT) |
M: 15-50%
F: 12-45% |
Reflects iron available for immediate erythropoiesis
Calculated as serum iron divided by TIBC |
New Strategies in Iron Management
There are three major areas of advancement in iron management:
(1) new data on intravenous iron utilization since the publication of the KDIGO guidelines in 2012;
(2) utility of dialysate iron for hemodialysis patients; and
(3) extended dosing interval oral iron therapy.
The Ferinject assessment in patients with Iron deficiency anaemia and Non-Dialysis-dependent Chronic Kidney Disease (FIND-CKD) trial evaluated intravenous ferric carboxymaltose to target a higher (400-600 ng/mL) or lower (100-200 ng/mL) ferritin compared to oral iron in patients with non-dialysis CKD not receiving an ESA.23 This was an open-label, multi-center, randomized, prospective study in 636 patients. The composite endpoint was initiation of other anemia treatments or a hemoglobin <10 g/dL for two consecutive values. Over a 52-week study period, patients receiving intravenous ferric carboxymaltose that targeted a higher ferritin (400-600 ng/mL) had a lower risk of the composite endpoint than patients with a lower target ferritin (100-200 ng/mL; HR 0.68, 95% CI: 0.45-1.05) and those receiving oral iron (HR 0.65, 95% CI: 0.44-0.95). Change in hemoglobin over the study was significantly higher in the intravenous ferric carboxymaltose high ferritin group (10.1 g/dL to 12.0 g/dL) compared to oral iron (10.2 g/dL to 11.5 g/dL; P=0.014). Serious adverse events were similar between the three groups. These results suggest that intravenous iron is more effective than oral iron in non-dialysis CKD patients in prolonging the time to ESA treatment and that higher ferritin targets are generally safe.
The Randomized Trial to Evaluate Intravenous and Oral Iron in Chronic Kidney Disease (REVOKE) trial compared the decline in renal function in patients with stage 3 or 4 CKD treated with oral ferrous sulfate or intravenous iron sucrose.24 This was an open-label, randomized, single-center study of 136 patients. The trial was stopped early because of safety concerns for the intravenous iron sucrose. There was an increased risk of serious cardiovascular events (adjusted incident rate ratio 2.51, 95% CI: 1.56-4.04) and increased risk of infection-related hospitalizations (adjusted incident rate ratio 2.12, 95% CI: 1.24-3.64). The change in measured GFR over two years was no different between the groups (between groups difference -0.35 ml/min/1.73 m2, 95% CI: -2.9 to 2.3). These results partly contradict those of the FIND-CKD trial, in that intravenous iron does not appear to be as safe as oral iron in non-dialysis CKD patients. However, the REVOKE trial was not designed to evaluate the efficacy of iron for anemia, but was rather focused on the impact it may have on CKD progression.
A number of observational studies have further evaluated the safety of intravenous iron in the same time period. Results have been conflicting: some have shown no increased risk of mortality or readmission for infection25, others have shown a lower risk of mortality26, and some a higher risk of infection-related hospitalization27 and mortality28. Notably, the signal for increased risk of infection-related hospitalization and mortality appear to be linked to larger doses of intravenous iron and bolus administration.28,29
The Proactive Intravenous Iron Therapy in Hemodialysis Patients (PIVOTAL) trial was designed to better assess the safety of high dose intravenous iron therapy specifically in hemodialysis patients.30 This was a multi-center, open-label, randomized, non-inferiority trial of high dose iron sucrose (mean 264 mg/month) compared to low dose iron sucrose (median 145 mg/month) in 2141 patients. The high dose group had iron administered proactively; patients were given iron sucrose 400 mg/month unless the ferritin exceeded 700 ng/mL or TSAT exceeded 40%. The low dose group received a ranging dose of 0-400 mg iron sucrose/month to maintain a ferritin >200 ng/mL and TSAT >20%. The composite endpoint included nonfatal myocardial infarction, nonfatal stroke, hospitalization for heart failure, or death. The high dose group had a lower risk of the composite endpoint (HR 0.95, 95% CI 0.73-1.00, P=0.04 for superiority) and also utilized significantly less erythropoiesis stimulating agent than the low dose group. Hospitalization for infection was 29.6% in the high dose group compared to 29.3% in the low dose group (P=0.92). This study, the largest and most rigorous in the hemodialysis population, demonstrates that high dose, proactive intravenous iron is not only safe, but provides cardiovascular benefit in anemia of CKD.
Ferric pyrophosphate citrate (FPC; Triferic) is an iron product that is delivered via the dialysate solution in hemodialysis patients.31,32 There are many benefits to this form of administration: low doses of iron administered frequently avoid iron overload and sequestration, decreased risk of infusion reactions from intravenous iron, decreased gastrointestinal adverse effects of oral iron, and mitigates concerns of adherence. FPC directly delivers iron to transferrin which also allows for more effective utilization by developing erythrocytes. In placebo controlled clinical trials, FPC has been shown to maintain hemoglobin concentrations, reduce the dose of ESAs and reduce the amount of intravenous iron in hemodialysis patients.31,32 One patient (0.3%) developed a hypersensitivity reaction in the Continuous Replacement Using Iron Soluble Equivalents (CRUISE) trials, but other adverse effects were not serious or not attributable to iron therapy. FPC is only indicated for treatment of iron deficiency anemia in patients receiving in-center hemodialysis.33
Traditional dosing strategies for oral iron in CKD patients that are iron deficient and anemic target 200 mg elemental iron per day in 2-3 divided doses. Commonly, ferrous sulfate 325 mg (65 mg elemental iron) by mouth three times daily is prescribed. All formulations of oral iron have 10-15% bioavailability for the elemental iron content. Thus, ferrous sulfate 325 mg given three times per day would result in 19.5-29.25 mg elemental iron absorbed each day. Recent evidence challenges this three times per day dosing scheme and suggests a once daily or every other day regimen.34,35 The mechanism behind this change is that multiple doses per day upregulate hepcidin, which downregulates ferroportin and decreases oral iron bioavailability.36 Clinical studies have shown that once daily, or even every other day, oral iron dosing increases the fractional absorption of iron. However, these studies have been conducted in relatively healthy, young females with iron deficiency without anemia. Extrapolation to the CKD population is difficult with these data because patients with CKD already have an upregulation of hepcidin, often have multiple co-morbidities, and quickly develop iron deficient anemia. While less frequent dosing may optimize the fraction of elemental iron absorbed, patients with CKD, severe iron deficiency, or overt anemia may still require more frequent dosing to increase the absolute amount of elemental iron absorbed. For example, ferrous sulfate 325 mg administered every other day with a maximal bioavailability of 15% would provide 4.9 mg elemental iron per day. Data from Moretti and colleagues show that fractional iron absorption is reduced by 35-45% when administered multiple times per day.36 Assuming a decrease in bioavailability from 15% to 7.5% (a 50% relative decline), ferrous sulfate 325 mg administered three times daily would provide 14.6 mg elemental iron per day; nearly 3-fold more elemental iron per day than the alternate dosing scheme. Nonetheless, three times per day iron has many downsides including poor tolerability, drug-drug interactions, and poor compliance. Pharmacists should consider these factors as well as altered absorption with multiple daily dosing when devising a patient-specific iron regimen.
Erythropoiesis Stimulating Agents
A major driver of worse outcomes associated with anemia of CKD is cardiovascular disease, mediated by chronic myocardial hypoxia leading to left ventricular hypertrophy.8 Unfortunately, the mainstay treatment of anemia of CKD are erythropoiesis stimulating agents (ESAs), which are also associated with negative cardiovascular outcomes.37-40
Recombinant human erythropoietin was first released in the US in 1989, which was a major leap forward in the treatment of anemia in patients with CKD. Over 30 years later, multiple ESAs are available in the US (Table 5). However, their routine clinical use for anemia in CKD patients has come at a high cost, both financially and because of harmful adverse events. In 1998, the Normal Hematocrit Study identified a potential increased risk of cardiovascular events with epoetin alfa when targeting a normal hematocrit of 42% compared to 30%.38 Subsequently, the Correction of Hemoglobin and Outcomes in Renal Insufficiency (CHOIR) trial demonstrated a 34% increased risk of a composite of death, nonfatal myocardial infarction, hospitalization for heart failure and stroke in patients treated with epoetin to a target hemoglobin of 13.5 g/dL compared to 11.3 g/dL.37 While the Cardiovascular Risk Reduction by Early Anemia Treatment with Epoetin Beta (CREATE) trial did not show an increased cardiovascular risk of epoetin beta when targeting a hemoglobin of 13-15 g/dL compared to 10.5-11.5 g/dL, there was no cardiovascular benefit and improvements in quality of life were modest.39 Lastly, the Trial to Reduce Cardiovascular Events With Aranesp Therapy (TREAT) trial demonstrated a 2-fold increased risk of stroke with darbepoetin alfa targeting a hemoglobin of 13 g/dL compared to placebo control.40 Given these cardiovascular risks, the KDIGO guidelines recommend initiating an ESA when hemoglobin is below 9 g/dL and targeting an on-treatment hemoglobin of 10-11.5 g/dL.22 The Food and Drug Administration in the US is more restrictive, with labeled warnings not to exceed a hemoglobin of 11 g/dL in ESRD patients and 10 g/dL in patients with CKD.41 Considerable debate still exists surrounding the cause of increased cardiovascular risks; whether it is caused by the increased hemoglobin target or increased ESA dose to achieve that target is unknown.
| Table 5. Comparison of ESAs |
| ESA (Brand name) |
Dosing |
Notes |
| Epoetin alfa (Epogen) |
Dialysis: 50-100 units/kg IV three times per week
Non-Dialysis: 50-100 units/kg SubQ once weekly |
Can be given in once weekly doses
SubQ route uses ~20% less drug42 (cost saving) |
| Darbepoetin alfa (Aranesp) |
0.45 mcg/kg IV or SubQ once weekly |
~200:1 conversion from epoetin to darbepoetin
Can be given every 2 weeks |
| Methoxy polyethylene glycol epoetin beta (Mircera) |
0.6 mcg/kg IV or SubQ every 2 weeks |
CERA: Continuous erythropoietin receptor agonist
Longest acting ESA; can be given every 4 weeks |
| Epoetin alfa epbx (Retacrit) |
Dialysis: 50-100 units/kg IV three times per week
Non-Dialysis: 50-100 units/kg SubQ once weekly |
Biosimilar of Epogen
1:1 dose conversion to Epogen
~33% cost savingsa |
| a Cost savings based on average wholesale price of Retacrit compared to Epogen,43 however, actual cost savings may depend on institutional contracts with manufacturers and distributors. |
Aside from adverse cardiovascular events, ESAs can also cause hypertension, anti-erythropoietin antibody development, hypersensitivity reactions, pure red blood cell aplasia, and vascular access thrombosis. Because ESAs are a colony stimulating factor, there is a warning about increased risk of tumor progression. Dosing involves a titration of 25% increments to achieve the target hemoglobin every 2-4 weeks. This practice is reactive and often leads to hemoglobin values above or below the target range. The goal of ESAs is to reduce the risk of blood transfusions, which impart negative consequences for subsequent transplantation due to allosensitization. It is important to note that ESAs do not improve mortality in patients with CKD, and at current hemoglobin targets, it is unclear if they provide a quality of life improvement.
The case example with questions and faculty commentary that follows will tie back to this section, illustrating how key concepts might be applied by the care team and its members in the clinical setting.
CASE 1b, Bill, Continued.
Bill was evaluated for his anemia and found to be iron deficient (TSAT 12%, serum ferritin 112 ng/mL). Therapy with ferrous sulfate 325 mg by mouth every other day was initiated. He returns to clinic 3 months later and continues to complain of fatigue and shortness of breath despite an increased dose of furosemide, and repeat Hb was 8.8 g/dL.
In response to this finding, the pharmacist in the CKD clinic recommends initiating intravenous iron therapy and discontinuing the oral iron. Bill begins iron sucrose 100 mg intravenously twice per week for 10 doses. Four weeks later, Bill’s hemoglobin is 9.5 g/dL, and shortness of breath is resolved, but his fatigue is not significantly improving.
CASE QUESTIONS
PAUSE AND REFLECT: Assess this case and consider the case questions based on the activity content thus far, then listen to the faculty commentary.
- What dose of oral iron would you have recommended for Bill? Why?
- How long after initiation of oral iron would you reassess therapy? When would you re-check iron studies? What are your goal iron parameters?
- How should you monitor Bill during the iron infusions?
- When would you consider starting an ESA for Bill?
|
SECTION 3: HIF Stabilizers in Development
Overview of the Landscape
Stabilization of the HIF complex causes an increase in endogenous erythropoietin production, increased expression of erythropoietin receptors, transferrin receptors, suppression of hepcidin, increased iron absorption from the gut, and increased iron mobilization from stores.2 Pharmacologic stabilization can be achieved by inhibiting the prolyl hydroxylase (PH) enzymes involved in the breakdown of HIF-α. These HIF-PH inhibitors, also known as HIF stabilizers, are an emerging class of medications that may provide the next move forward in the management of anemia in patients with CKD. There are currently five HIF stabilizers in development (Table 6):
- roxadustat has completed phase III trials;
- molidustat, vadadustat, and desidustat have completed phase II trials and have phase III trials ongoing;
- depradustat has completed phase II studies and is moving into phase III.
Each of these agents is an orally-administered small molecule which provides a desirable alternative for patients compared to injectable ESAs. HIF stabilizers provide a more sustained release of endogenous erythropoietin, avoiding the initial peak concentrations with ESA administration.44 The adverse effect profiles have not demonstrated an increased risk of cardiovascular events, and recent data suggest that HIF stabilizers may improve major adverse cardiovascular events (MACE) compared to ESAs.45 However, HIF stabilization may also have some negative off-target effects. Vascular endothelial growth factor (VEGF) is upregulated by HIF stabilization and may contribute to an increased risk of angiogenesis and tumor formation. Results from current phase II and phase III trials do not demonstrate an increased risk of malignancies, but short follow-up periods may not be adequate to detect these events.
Roxadustat
Roxadustat is the HIF-PH inhibitor furthest along in clinical trials as of March 2020. It is a reversible inhibitor of HIF-PH that mimics the body’s normal response to hypoxia. Given a relatively short half-life of 10 hours and a dose schedule of three times per week, therapy with roxadustat allows for the HIF pathway to return to “normal” levels between dosing periods. This intermittent stimulation of the HIF pathway mirrors normal physiology and may reduce long-term adverse effects.
Two phase III clinical trials of roxadustat have been completed. A randomized, placebo-controlled, multi-site clinical trial in China evaluated roxadustat or placebo in 154 patients with CKD not on dialysis for 8 weeks.46 The primary endpoint was change in hemoglobin over 8 weeks. Roxadustat was dosed at 70 mg for weight 40 to <60 kg and 100 mg for weight ≥60kg and titrated to achieve a hemoglobin of 10-12 g/dL. The roxadustat group exhibited a mean increase in hemoglobin of 1.9±1.2 g/dL compared to a mean decrease of 0.4±0.8 g/dL in the placebo group (between-group difference 2.2 g/dL, 95% CI 1.9-2.6, P<0.001). Hepcidin declined significantly in the roxadustat group compared to placebo group (between-group difference -49.8 ng/ml, 95% CI -66.8 to -32.8, P<0.001) reflecting an increase in iron availability during erythropoiesis. Adverse events (AEs) that occurred in ≥5% of patients receiving roxadustat were peripheral edema, upper respiratory tract infection, hypertension, hyperkalemia and metabolic acidosis. The overall incidence of AEs was no different between roxadustat and placebo groups, however hyperkalemia was more common with roxadustat (16%) compared to placebo (8%) as was metabolic acidosis (12% vs. 2%).46
The second phase III trial was a prospective, randomized, open-label, multi-site, non-inferiority study comparing roxadustat to epoetin alfa in 305 patients receiving maintenance hemodialysis in China.47 The primary endpoint was change in hemoglobin from baseline to 26 weeks. Roxadustat was dosed at 100 mg for weight 45 to <60 kg and 120 mg for weight ≥60 kg and titrated to achieve a hemoglobin of 10-12 g/dL. Change in hemoglobin was 0.7±1.1 g/dL for roxadustat compared to 0.5±1.0 g/dL for epoetin alfa (between-group difference 0.2±1.2 g/dL, 95% CI -0.02 to 0.5g/dL) which met the a priori benchmark for non-inferiority. Hepcidin changed in the roxadustat group (-30.2 ng/mL, 95% CI -64.8 to -13.6), but not in the epoetin alfa group (-2.3 ng/mL, 95% CI -51.6 to 6.2). In an exploratory analysis, C-reactive protein (CRP), a marker of inflammation, had a significant interaction with the treatment effect. In patients with high baseline CRP, indicating high inflammatory burden, treatment with roxadustat was more effective than epoetin alfa, despite increased epoetin alfa doses in this group. These results have important implications as they suggest that roxadustat may be more effective than ESAs in patients with hyporesponsiveness to ESAs. Adverse effects were similar between groups, but roxadustat had more hyperkalemia (7.4% vs. 1%) and upper respiratory infections (18.1% vs. 11.0%) while epoetin alfa had more hypertension (12.3% vs. 16.0%).47
The collective results of these clinical trials indicate that roxadustat is effective and safe as a treatment of anemia in CKD non-dialysis and dialysis patients. Three additional ongoing international phase III trials will provide valuable additional evidence for this treatment in different geographic populations and add to the safety data. Concerns related to hyperkalemia associated with roxadustat need to be explored further. In the non-dialysis trial presented above, the mean change in serum potassium from baseline to end of treatment period was similar between roxadustat (4.98±0.64 mmol/L to 4.96±0.68 mmol/L) and placebo (5.03±0.47 mmol/L to 4.98±0.54 mmol/L).46 In the dialysis trial, the proportion of patients with a serum potassium >5.5 mmol/L was 26.5% at baseline and 24.1% at week 27 for roxadustat compared to 31.0% at baseline and 29.7% at week 27 for epoetin alfa.47 The mechanism of hyperkalemia with roxadustat is unknown.
Molidustat
Molidustat has undergone three phase II clinical trials, reported in aggregate as the DaIly orAL treatment increasing endOGenoUs Erythropoietin (DIALOGUE) 1, 2, and 4 studies.48 Each study was a randomized, controlled, multi-site, parallel group, 16-week phase IIb trial and had a primary endpoint of change in hemoglobin from baseline to the last 4 weeks of treatment. In the DIALOGUE 1 trial, 121 treatment naïve patients with CKD non-dialysis were treated with randomly assigned fixed doses of molidustat (once or twice daily) compared to placebo. The between-group difference for all molidustat doses compared to placebo for change in hemoglobin was 1.4 g/dL (95% CI 0.9 to 2.0). In the DIALOGUE 2 trial, 124 patients with CKD non-dialysis previously treated with darbepoetin alfa were assigned to 3 doses of molidustat compared to darbepoetin alfa. The between-group difference for all molidustat doses compared to darbepoetin for change in hemoglobin was 0.2 g/dL (95% CI -0.1 to 0.6). In the DIALOGUE 4 trial, 199 patients with CKD on dialysis previously treated with epoetin alfa were assigned 4 doses of molidustat compared to epoetin alfa. The between-group difference for all molidustat doses compared to epoetin alfa for change in hemoglobin was -0.3 g/dL (95% CI -0.7 to 0.1). The incidence of treatment-emergent adverse events was similar between molidustat and comparator groups across all three studies and were generally mild-to-moderate in severity. Common AEs were nasopharyngitis and diarrhea. Changes in iron metabolism were favorable in the molidustat group with decreases in hepcidin and ferritin, while increases in iron binding capacity were observed. These changes are consistent with the expected effects of HIF stabilization.48
Phase III clinical trials of molidustat are underway and will provide valuable information about optimal dosing and additional safety information.49
Dapradustat
Dapradustat has been evaluated in a prospective, randomized, double-blind, placebo-controlled, dose-ranging phase II study in 103 hemodialysis patients previously treated with epoetin alfa.50 Dapradustat was given three times per week for 4 weeks in varying doses. The change in hemoglobin over the study period was dose dependent: in the lower dapradustat dose groups (10-15 mg), hemoglobin remained consistent from the pre-study levels, whereas the higher dose groups (25-30 mg) the hemoglobin increased over the study period. In the placebo group, hemoglobin declined. On treatment serious adverse events were similar between dapradustat (10%) and placebo (11%). Given the results of this and other phase II trials of dapradustat, it has moved into the next phase of clinical development and currently has four phase III trials ongoing.
Vadadustat
Vadadustat was evaluated in a 16-week, open-label, phase II clinical trial of 94 patients with CKD on hemodialysis.51 Patients were previously receiving epoetin alfa and converted to one of three doses of vadadustat (once daily or three times per week). The primary endpoint was change in hemoglobin over the study period. There was no statistically significant change in hemoglobin from baseline to week 16 in any of the dose groups: 300 mg once daily (mean hemoglobin change -0.03±090 g/dL), 450 mg once daily (-0.07±0.97 g/dL), and 450 mg three times per week (-0.14±-1.12 g/dL). Thus, each dose was able to maintain hemoglobin within a desired range achieved by epoetin alfa prior to initiation of vadadustat. Twenty-two patients (23.4%) developed adverse effects deemed to be related to the study drug; none were serious. Most common adverse effects were gastrointestinal in nature (nausea, vomiting, diarrhea).
Desidustat
Desidustat was evaluated in a randomized, placebo-controlled, double-blind, 6-week phase II trial in 117 patients with CKD not on dialysis.52 The primary endpoint was change in hemoglobin over the study period. Mean hemoglobin increased 1.57 to 2.92 g/dL in a dose-dependent manner in the three desidustat groups, compared to a mean increase of 0.46 g/dL in the placebo group. There were 18 treatment emergent adverse events, but none was serious in nature.
| Table 6. Summary of HIF-PH inhibitors under development |
| Drug |
Dosinga |
Pharmacokinetics |
Common Adverse Events |
Current Phase |
| Roxadustat |
Three times per week |
t½ ~10 hours53 |
Upper respiratory infections
Hyperkalemia |
Completed two phase III trials; three additional phase III trials ongoing |
| Molidustat |
Once daily |
t½ ~10 hours54 |
Nasopharyngitis
Diarrhea |
Phase III trials ongoing |
| Dapradustat |
Once daily |
t½ ~2-4 hours55,56 |
Nausea |
Phase III trials ongoing |
| Vadadustat |
Once daily or three times per week |
t½ ~4.5 hours57
No significant
removal by
hemodialysis |
Gastrointestinal |
Phase III trials ongoing |
| Desidustat |
Once daily |
t½ ~7-13 hours58 |
Gastrointestinal
Headache |
Phase III trials ongoing |
| a Dosing reflects regimens from phase III trials; please refer to product labeling for dosing regimen following regulatory approval. |
Summary of HIF-PH inhibitors in Development
There are five HIF-PH inhibitors in development. It is important to recognize that each drug has been studied with doses titrated to hemoglobin target of ~10-12 g/dL. Inter-individual variability in dose response appears high, similar to ESA treatment. Should one or more of these agents receive FDA approval, pharmacists will be integral in implementing dose adjustment protocols to maintain target hemoglobin concentrations. Dosing schedule (once daily vs. three times per week) and side effect profiles are major differences between these drugs. Roxadustat appears to lower cholesterol in a dose-dependent manner, which has not been consistently observed with the other agents. The possibility that these agents increase the activity of VEGF, and therefore impart a higher risk of malignancy in the long-term, will be an important safety concern in phase III trials. However, vadadustat and dapradustat have shown no increases in VEGF during phase II trials.59-61 US clinicians should cautiously interpret clinical trial results from other countries (China, Japan, Europe, etc.) as previous studies in anemia management of CKD patients have shown differing outcomes by geographic region (e.g. CHOIR37 and CREATE39 trials).
The case example with questions and faculty commentary that follows will tie back to this section, illustrating how key concepts might be applied by the care team and its members in the clinical setting.
CASE 2, Jim
Jim is a 44-year old male (68 inches, 150 pounds) who is on chronic hemodialysis secondary to type 1 diabetes mellitus. His past medical history also includes peripheral vascular disease status post right total metatarsal amputation (6 months ago) and left below knee amputation (2 years ago), chronic osteomyelitis of the right lower extremity, stage 3 sacral decubitus ulcer, peripheral neuropathy, chronic pain, and orthostatic hypotension. Most recent labs show a hemoglobin 7.8 g/dL, TSAT 22%, ferritin 1552 ng/mL, C-reactive protein 88.5 mcg/mL and erythrocyte sedimentation rate 72 mm/hour. Jim has been receiving escalating doses of epoetin alfa which was increased 4 weeks prior from 12,000 units IV three times per week to 15,000 units IV three times per week. He also receives intravenous ferric gluconate 62.5 mg once weekly.
CASE QUESTIONS
PAUSE AND REFLECT: Assess this case and consider the case questions based on the activity content thus far, then listen to the faculty commentary.
- What would you do with Jim’s epoetin alfa dose: continue unchanged, increase or decrease, and why?
- What would you do with Jim’s IV ferric gluconate dose: continue unchanged, increase or decrease, and why?
- What other interventions might be appropriate to increase Jim’s hemoglobin?
- Might Jim be a candidate for a HIF stabilizer agent if one or more receive FDA approval Why or why not?
|
SECTION 4: Pharmacists as Key Members of the Nephrology Care Team
Overview of Nephrology Care Team and Pharmacist’s Roles
Pharmacists are essential members of the interprofessional nephrology care team. Their expertise in medication management is critical in a patient population with multiple comorbidities, altered pharmacokinetics, and polypharmacy. Nephrology pharmacists can provide a variety of value-added services, including but not limited to:
- medication history and reconciliation at outpatient appointments and upon inpatient admission;
- medication adherence assessments and intervention to improve adherence;
- comprehensive medication management with a focus on achieving guideline directed medical therapies for CKD, diabetes mellitus, and cardiovascular diseases;
- provide renal dosing adjustments of all medications;
- monitor for and manage drug-drug interactions; and
- minimize polypharmacy and pill burden.
- pharmacists should also evaluate new and existing clinical services using continuous quality improvement principles.
The role of pharmacists in CKD is supported by a number of studies. A systematic review of pharmacists’ interventions in CKD included 37 studies with 4,743 patients.62 In the 8 controlled studies, including 744 CKD patients, pharmacy intervention reduced composite of ESRD and mortality in those with diabetes (14.8 vs 28.2 per 100 patient-years, P<0.001; 60% relative risk reduction), reduced hospitalizations (1.8 ± 2.4 vs 3.1 ± 3.0, P=0.02) and increased target hemoglobin attainment (69.8% vs 43.9%, P=0.0001). In the 5 studies that reported humanistic outcomes, pharmacy intervention improved health related quality of life (HRQOL) in dimensions of general health (28% improvement, P<0.001) and social functioning (26% improvement, P<0.001) and improvements in energy, daily activities, and general well-being were reported (P<0.05 for all). Others have shown improved renal survival (HR 0.64, 95% CI: 0.48–0.85) and a cost savings of $1,931/patient-year with multidisciplinary care including pharmacy services.63 A higher rate of guideline-directed medication therapy and a 51% reduction in all-cause mortality was observed in a prospective cohort study.64 Multidisciplinary clinics including pharmacists have shown a slower decline in renal function (GFR declined at 2.52 ml/min/1.73 m2 per year in historical control vs 1.17 ml/min/1.73 m2 per year with multidisciplinary care, P<0.0001).65 Given this accumulation of evidence, it is apparent that interprofessional care including pharmacist-based medication optimization is critical to improve the health of patients with CKD.
One of the major driving forces that has led to pharmacist-based care in CKD is the integration of pharmacists into anemia management. Given the high costs of drugs used for this condition (ESAs) and significant complications that can be associated with therapy, pharmacists were able to carve out this niche in nephrology clinics. Once involved, their roles have been expanding (as above). Table 7 below summarizes the evidence for pharmacist involvement in anemia management in CKD.
| Table 7. Pharmacist-based anemia management in CKD |
| Study |
Design |
Major Findings |
| To LL, et al. Am J Health Sys Pharm. 2001.66 |
Retrospective, before/after study of pharmacist vs physician anemia management in hemodialysis patients over 6-month period |
• Hematocrit was 36.2% ± 3.5% for pharmacists and 35.4% ± 3.3% for physicians (P=0.20).
• Epoetin alfa utilization was 7.7 million units with pharmacists vs 8.5 million units with physicians (P=0.37) |
| Quercia RA, et al. Hosp Pharm. 2000.67 |
Drug use evaluation of pharmacist-led anemia management in hemodialysis patients |
• Hematocrit <31% decreased from 32% to 14%
• Cost avoidance from using epoetin alfa overfill was $91,148/year
• Cost avoidance from pharmacy management of anemia was $203,985/year |
| Kimura T, et al. Biol Pharm Bull. 2004.68 |
Observational before/after study of pharmacist vs physician management of anemia in hemodialysis (Japan) |
• On target hematocrit improved from 17% to 78%
• Epoetin alfa utilization decreased 30%, with 26% cost reduction |
| Walton T, et al. Hosp Pharm. 2005.69 |
Observational: pharmacist vs US averages |
• 80% of pharmacist-managed patients had hemoglobin at target (>11 g/dL at the time) compared to 75% in US average
• Epoetin alfa utilization decreased from 16,000 units/week in US average to 9,300 units/week with pharmacist management
• $3,000 cost savings per patient per year |
| Bucaloiu ID, et al. Managed Care Interface. 2007.70 |
Observational: pharmacist vs primary care physician anemia management |
• Reduced epoetin alfa utilization 44% (P=0.0001)
• Maintained hemoglobin in target range more often (69.8% vs 43.9%, P=0.0001) |
| Joy MS, et al. Pharmacotherapy. 2007.71 |
Observational: re-engineered multidisciplinary clinic led by pharmacist |
• 78% of patients achieved hemoglobin goal compared to 41% of historical patients |
In summary, pharmacist-based anemia management has been shown to improve target hemoglobin attainment and decrease ESA utilization and cost.
The case example with questions and faculty commentary that follows will tie back to this section, illustrating how key concepts might be applied by pharmacists and the care team in the clinical setting.
CASE 3, Margie
Margie is a 55-year old African American female (65 inches, 204 pounds) who works part-time at a local school. She presents to her routine nephrology clinic appointment with no complaints. Margie has a past medical history of type 2 diabetes mellitus, chronic kidney disease stage IIIB A3, hypertension, atrial fibrillation, and heart failure with reduced ejection fraction of 30-35%. Physical exam reveals a blood pressure of 152/88 mm Hg, heart rate of 105 beats per minute, 1+ pedal edema, irregularly irregular heart rhythm and is otherwise unremarkable. Recent labs show a hemoglobin A1C of 9.2%, eGFR 38 ml/min/1.73 m2, TSAT 18%, ferritin 112 ng/mL, hemoglobin 10.7 g/dL.
Medications: aspirin 81 mg daily, apixaban 5 mg twice daily, labetalol 400 mg twice daily, nifedipine ER 90 mg once daily, glyburide XL 10 mg daily in the morning, metformin 1000 mg twice daily, esomeprazole 40 mg daily.
You are the pharmacist in the nephrology clinic reviewing this patient’s chart to address her anemia.
CASE 3 QUESTIONS
PAUSE AND REFLECT: Assess this case and consider the case questions based on the activity content thus far, then listen to the faculty commentary.
- What is your next step in addressing Margie’s anemia?
- What other services can a pharmacist provide Margie during this encounter? What would you prioritize?
- What kind of patient education would you provide for Margie?
|
SUMMARY SECTION
The landscape of anemia management in chronic kidney disease is rapidly evolving. New iron dosing strategies, novel iron formulations, and a new class of medications will be affecting clinical practice in the next 5 years. Pharmacists will be essential members of the care team as they help practitioners and patients navigate these changes to realize optimal therapeutic outcomes for patients in a cost-effective manner.
» Case Questions Transcript
REFERENCES
- Shih HM, Wu CJ, Lin SL. Physiology and pathophysiology of renal erythropoietin-producing cells. J Formos Med Assoc. 2018;117(11):955-963.
- Gupta N, Wish JB. Hypoxia-Inducible Factor Prolyl Hydroxylase Inhibitors: A Potential New Treatment for Anemia in Patients With CKD. Am J Kidney Dis. 2017;69(6):815-826.
- Centers for Disease Control and Prevention. National Chronic Kidney Disease Fact Sheet. https://www.cdc.gov/kidneydisease/publications-resources/2019-national-facts.html. Published 2019. Accessed 3/16/2020.
- Gounden V, Jialal I. Renal Function Tests. [Updated 2019 Apr 3]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507821/.
- National Institute of Diabetes and Digestive and Kidney Diseases: Kidney Disease Statistics for the United States. https://www.niddk.nih.gov/health-information/health-statistics/kidney-disease. Published 2016. Accessed 3/16/2020.
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney inter., Suppl. 2013; 3: 1–150.
- Xu J, Murphy SL, Kochanek KD, Bastian BA. Deaths: Final Data for 2013. Natl Vital Stat Rep. 2016;64(2):1-119.
- Tanaka T, Eckardt KU. HIF Activation Against CVD in CKD: Novel Treatment Opportunities. Semin Nephrol. 2018;38(3):267-276.
- Stauffer ME, Fan T. Prevalence of anemia in chronic kidney disease in the United States. PLoS One. 2014;9(1):e84943.
- Andrews NC. Disorders of iron metabolism. N Engl J Med. 1999;341(26):1986-1995.
- Wilson K, Sloan JM. Iron-Deficiency Anemia. N Engl J Med. 2015;373(5):485.
- Kolesar JM. Novel approaches to anemia associated with cancer and chemotherapy. Am J Health Syst Pharm. 2002;59(15 Suppl 4):S8-11.
- Nemeth E, Tuttle MS, Powelson J, et al. Hepcidin regulates cellular iron efflux by binding to ferroportin and inducing its internalization. Science. 2004;306(5704):2090-2093.
- Ganz T, Nemeth E. Iron Balance and the Role of Hepcidin in Chronic Kidney Disease. Semin Nephrol. 2016;36(2):87-93.
- Al-Ahmad A, Rand WM, Manjunath G, et al. Reduced kidney function and anemia as risk factors for mortality in patients with left ventricular dysfunction. J Am Coll Cardiol. 2001;38(4):955-962.
- Teucher B, Olivares M, Cori H. Enhancers of iron absorption: ascorbic acid and other organic acids. Int J Vitam Nutr Res. 2004;74(6):403-419.
- Tolkien Z, Stecher L, Mander AP, Pereira DI, Powell JJ. Ferrous sulfate supplementation causes significant gastrointestinal side-effects in adults: a systematic review and meta-analysis. PLoS One. 2015;10(2):e0117383.
- Cancelo-Hidalgo MJ, Castelo-Branco C, Palacios S, et al. Tolerability of different oral iron supplements: a systematic review. Curr Med Res Opin. 2013;29(4):291-303.
- Gereklioglu C, Asma S, Korur A, Erdogan F, Kut A. Medication adherence to oral iron therapy in patients with iron deficiency anemia. Pak J Med Sci. 2016;32(3):604-607.
- Wang C, Graham DJ, Kane RC, et al. Comparative Risk of Anaphylactic Reactions Associated With Intravenous Iron Products. Jama. 2015;314(19):2062-2068.
- Brewster UC, Perazella MA. Intravenous iron and the risk of infection in end-stage renal disease patients. Semin Dial. 2004;17(1):57-60.
- Kidney Disease: Improving Global Outcomes (KDIGO) Anemia Workgroup. KDIGO Clinical Practice Guideline for Anemia in Chronic Kidney Disease. Kidney Int Suppl. 2012;2(4):279-335.
- Macdougall IC, Bock AH, Carrera F, et al. FIND-CKD: a randomized trial of intravenous ferric carboxymaltose versus oral iron in patients with chronic kidney disease and iron deficiency anaemia. Nephrol Dial Transplant. 2014;29(11):2075-2084.
- Agarwal R, Kusek JW, Pappas MK. A randomized trial of intravenous and oral iron in chronic kidney disease. Kidney Int. 2015;88(4):905-914.
- Ishida JH, Marafino BJ, McCulloch CE, et al. Receipt of Intravenous Iron and Clinical Outcomes among Hemodialysis Patients Hospitalized for Infection. Clin J Am Soc Nephrol. 2015;10(10):1799-1805.
- Kuo KL, Hung SC, Liu JS, Chang YK, Hsu CC, Tarng DC. Iron supplementation associates with low mortality in pre-dialyzed advanced chronic kidney disease patients receiving erythropoiesis-stimulating agents: a nationwide database analysis. Nephrol Dial Transplant. 2015;30(9):1518-1525.
- Freburger JK, Ellis AR, Kshirsagar AV, Wang L, Brookhart MA. Comparative short-term safety of bolus versus maintenance iron dosing in hemodialysis patients: a replication study. BMC Nephrol. 2014;15:154.
- Miskulin DC, Tangri N, Bandeen-Roche K, et al. Intravenous iron exposure and mortality in patients on hemodialysis. Clin J Am Soc Nephrol. 2014;9(11):1930-1939.
- Brookhart MA, Freburger JK, Ellis AR, Wang L, Winkelmayer WC, Kshirsagar AV. Infection risk with bolus versus maintenance iron supplementation in hemodialysis patients. J Am Soc Nephrol. 2013;24(7):1151-1158.
- Macdougall IC, White C, Anker SD, et al. Intravenous Iron in Patients Undergoing Maintenance Hemodialysis. N Engl J Med. 2019;380(5):447-458.
- Fishbane SN, Singh AK, Cournoyer SH, et al. Ferric pyrophosphate citrate (Triferic) administration via the dialysate maintains hemoglobin and iron balance in chronic hemodialysis patients. Nephrol Dial Transplant. 2015;30(12):2019-2026.
- Gupta A, Lin V, Guss C, Pratt R, Ikizler TA, Besarab A. Ferric pyrophosphate citrate administered via dialysate reduces erythropoiesis-stimulating agent use and maintains hemoglobin in hemodialysis patients. Kidney Int. 2015;88(5):1187-1194.
- Triferic Package Insert. Rockwell Medical Inc. Wixom MI. Updated 3/2018.
- Stoffel NU, Zeder C, Brittenham GM, Moretti D, Zimmermann MB. Iron absorption from supplements is greater with alternate day than with consecutive day dosing in iron-deficient anemic women. Haematologica. 2019.
- Stoffel NU, Cercamondi CI, Brittenham G, et al. Iron absorption from oral iron supplements given on consecutive versus alternate days and as single morning doses versus twice-daily split dosing in iron-depleted women: two open-label, randomised controlled trials. Lancet Haematol. 2017;4(11):e524-e533.
- Moretti D, Goede JS, Zeder C, et al. Oral iron supplements increase hepcidin and decrease iron absorption from daily or twice-daily doses in iron-depleted young women. Blood. 2015;126(17):1981-1989.
- Singh AK, Szczech L, Tang KL, et al. Correction of anemia with epoetin alfa in chronic kidney disease. N Engl J Med. 2006;355(20):2085-2098.
- Besarab A, Bolton WK, Browne JK, et al. The effects of normal as compared with low hematocrit values in patients with cardiac disease who are receiving hemodialysis and epoetin. N Engl J Med. 1998;339(9):584-590.
- Drueke TB, Locatelli F, Clyne N, et al. Normalization of hemoglobin level in patients with chronic kidney disease and anemia. N Engl J Med. 2006;355(20):2071-2084.
- Pfeffer MA, Burdmann EA, Chen CY, et al. A trial of darbepoetin alfa in type 2 diabetes and chronic kidney disease. N Engl J Med. 2009;361(21):2019-2032.
- FDA Drug Safety Communication: Modified dosing recommendations to improve the safe use of Erythropoiesis-Stimulating Agents (ESAs) in chronic kidney disease. http://www.fda.gov/Drugs/DrugSafety/ucm259639.htm. Published 2011. Updated 6/24/2011. Accessed 2/21/2017.
- Paganini EP, Eschbach JW, Lazarus JM, et al. Intravenous versus subcutaneous dosing of epoetin alfa in hemodialysis patients. Am J Kidney Dis. 1995;26(2):331-340.
- Epoetin alfa monograph. Lexicomp. Wolters Kluwer Clinical Drug Information Inc. Updated 3/23/2020.
- Provenzano R, Besarab A, Wright S, et al. Roxadustat (FG-4592) Versus Epoetin Alfa for Anemia in Patients Receiving Maintenance Hemodialysis: A Phase 2, Randomized, 6- to 19-Week, Open-Label, Active-Comparator, Dose-Ranging, Safety and Exploratory Efficacy Study. Am J Kidney Dis. 2016;67(6):912-924.
- Provenzano R, Fishbane S, Lee-Jen W, et al. Pooled Efficacy and Cardiovascular (CV) Analyses of Roxadustat in the Treatment of Anemia in CKD Patients on and Not on Dialysis (Abstract). J Am Soc Nephrol. 2019;30:B1.
- Chen N, Hao C, Peng X, et al. Roxadustat for Anemia in Patients with Kidney Disease Not Receiving Dialysis. N Engl J Med. 2019;381(11):1001-1010.
- Chen N, Hao C, Liu BC, et al. Roxadustat Treatment for Anemia in Patients Undergoing Long-Term Dialysis. N Engl J Med. 2019;381(11):1011-1022.
- Macdougall IC, Akizawa T, Berns JS, Bernhardt T, Krueger T. Effects of Molidustat in the Treatment of Anemia in CKD. Clin J Am Soc Nephrol. 2019;14(1):28-39.
- Akizawa T, Taguchi M, Matsuda Y, Iekushi K, Yamada T, Yamamoto H. Molidustat for the treatment of renal anaemia in patients with dialysis-dependent chronic kidney disease: design and rationale of three phase III studies. BMJ Open. 2019;9(6):e026602.
- Bailey CK, Caltabiano S, Cobitz AR, Huang C, Mahar KM, Patel VV. A randomized, 29-day, dose-ranging, efficacy and safety study of daprodustat, administered three times weekly in patients with anemia on hemodialysis. BMC Nephrol. 2019;20(1):372.
- Haase VH, Chertow GM, Block GA, et al. Effects of vadadustat on hemoglobin concentrations in patients receiving hemodialysis previously treated with erythropoiesis-stimulating agents. Nephrol Dial Transplant. 2019;34(1):90-99.
- Parmar DV, Kansagra KA, Patel JC, et al. Outcomes of Desidustat Treatment in People with Anemia and Chronic Kidney Disease: A Phase 2 Study. Am J Nephrol. 2019;49(6):470-478.
- Shibata T, Nomura Y, Takada A, et al. Evaluation of Food and Spherical Carbon Adsorbent Effects on the Pharmacokinetics of Roxadustat in Healthy Nonelderly Adult Male Japanese Subjects. Clin Pharmacol Drug Dev. 2019;8(3):304-313.
- Bottcher M, Lentini S, Arens ER, et al. First-in-man-proof of concept study with molidustat: a novel selective oral HIF-prolyl hydroxylase inhibitor for the treatment of renal anaemia. Br J Clin Pharmacol. 2018;84(7):1557-1565.
- Becker KA, Jones JJ. An Emerging Treatment Alternative for Anemia in Chronic Kidney Disease Patients: A Review of Daprodustat. Adv Ther. 2018;35(1):5-11.
- Hara K, Takahashi N, Wakamatsu A, Caltabiano S. Pharmacokinetics, pharmacodynamics and safety of single, oral doses of GSK1278863, a novel HIF-prolyl hydroxylase inhibitor, in healthy Japanese and Caucasian subjects. Drug Metab Pharmacokinet. 2015;30(6):410-418.
- Shalwitz R, Hartman CS, Flinn C, Shalwitz I, Logan DK. AKB-6548, a novel hypoxia-inducible factor prolyl hydroxylase inhibitor reduces hepcidin and ferritin while it increases reticulocyte production and total iron binding capacity in healthy adults. (Abstract). J Am Soc Nephrol. 2011;22:435A.
- Kansagra KA. Comparison of Pharmacokinetic Parameters of Desidustate in Pre-Dialysis Chronic Kidney Disease Indian patients and Australian Healthy Volunteers (Abstract). Kidney International Reports. 2019;4(7):S430-S431.
- Pergola PE, Spinowitz BS, Hartman CS, Maroni BJ, Haase VH. Vadadustat, a novel oral HIF stabilizer, provides effective anemia treatment in nondialysis-dependent chronic kidney disease. Kidney Int. 2016;90(5):1115-1122.
- Holdstock L, Meadowcroft AM, Maier R, et al. Four-Week Studies of Oral Hypoxia-Inducible Factor-Prolyl Hydroxylase Inhibitor GSK1278863 for Treatment of Anemia. J Am Soc Nephrol. 2016;27(4):1234-1244.
- Brigandi RA, Johnson B, Oei C, et al. A Novel Hypoxia-Inducible Factor-Prolyl Hydroxylase Inhibitor (GSK1278863) for Anemia in CKD: A 28-Day, Phase 2A Randomized Trial. Am J Kidney Dis. 2016;67(6):861-871.
- Salgado TM, Moles R, Benrimoj SI, Fernandez-Llimos F. Pharmacists' interventions in the management of patients with chronic kidney disease: a systematic review. Nephrol Dial Transplant. 2012;27(1):276-292.
- Chen PM, Lai TS, Chen PY, et al. Multidisciplinary care program for advanced chronic kidney disease: reduces renal replacement and medical costs. The American journal of medicine. 2015;128(1):68-76.
- Chen YR, Yang Y, Wang SC, et al. Effectiveness of multidisciplinary care for chronic kidney disease in Taiwan: a 3-year prospective cohort study. Nephrol Dial Transplant. 2013;28(3):671-682.
- Bayliss EA, Bhardwaja B, Ross C, Beck A, Lanese DM. Multidisciplinary team care may slow the rate of decline in renal function. Clin J Am Soc Nephrol. 2011;6(4):704-710.
- To LL, Stoner CP, Stolley SN, Buenviaje JD, Ziegler TW. Effectiveness of a pharmacist-implemented anemia management protocol in an outpatient hemodialysis unit. Am J Health Syst Pharm. 2001;58(21):2061-2065.
- Quercia R, Abrahams R, White C. Cost avoidance and clinical benefits derived from a pharmacy-managed anemia program. Hospital Pharmacy. 2000;36(2):169-175.
- Kimura T, Arai M, Masuda H, Kawabata A. Impact of a pharmacist-implemented anemia management in outpatients with end-stage renal disease in Japan. Biological & pharmaceutical bulletin. 2004;27(11):1831-1833.
- Walton T, Holloway K, Knauss M. Pharmacist-Managed Anemia Program in an Outpatient Hemodialysis Population. Hospital Pharmacy. 2005;40:1051-1056.
- Bucaloiu ID, Akers G, Bermudez MC, et al. Outpatient erythropoietin administered through a protocol-driven, pharmacist-managed program may produce significant patient and economic benefits. Managed care interface. 2007;20(6):26-30.
- Joy MS, Candiani C, Vaillancourt BA, Chin H, Hogan SL, Falk RJ. Reengineering clinical operations in a medical practice to optimize the management of anemia of chronic kidney disease. Pharmacotherapy. 2007;27(5):734-744.
Back to Top