
Expired activity
Please go to the PowerPak
homepage and select a course.
GLP-1 Receptor Agonists for the Management of Type 2 Diabetes: Pharmacist Focus on the Evolving Treatment Landscape
The Role of GLP-1 RAs in the Management of Type 2 Diabetes and Cardiovascular Risk: Putting it All Together - Part 3 (Monograph)
INTRODUCTION
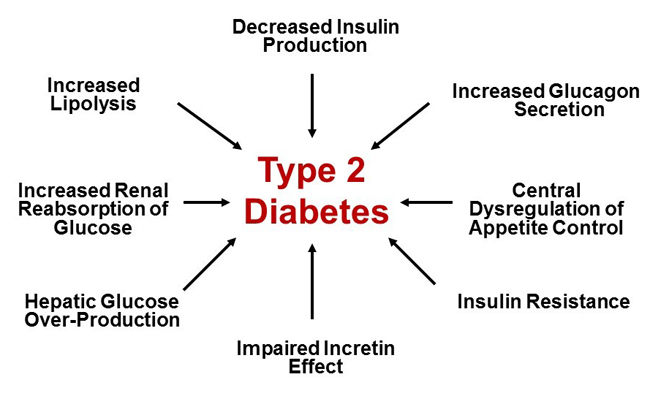
According to the Centers for Disease Control and Prevention, approximately 30.3 million people live with diabetes in the United States (U.S.).1 For people living with diabetes, optimization of glycemic control is one of several treatment approaches central to avoiding or delaying the complications of diabetes. Traditionally, type 2 diabetes mellitus (T2D) has been described by the “triumvirate” of: 1) impaired insulin secretion due to declining pancreatic β-cell function; 2) insulin resistance leading to decreased glucose uptake by peripheral tissues (muscle and adipose); and 3) increased glucose production by the liver due to excessive gluconeogenesis.2 The “triumvirate” has expanded in recent years to include additional pathophysiologic defects at play in people with T2D. The “ominous octet,” which includes 8 key pathophysiologic defects found to be present in T2D, is illustrated in Figure 1.3 Newer medication classes, such as glucagon-like peptide-1 receptor agonists (GLP-1 RAs) and sodium-glucose co-transporter 2 (SGLT-2) inhibitors, target some of the more recently identified defects described in the “ominous octet.” Agents from these medication classes are increasingly recommended in clinical practice guidelines and recommendations. This is due, at least in part, to recent outcome trial data supporting the use of select GLP-1 RAs and SGLT-2 inhibitors to mitigate cardiovascular and renal risks in at-risk patients. Given the increasing emphasis on the use of GLP-1 RAs in clinical practice, it is important that all members of the healthcare team, including pharmacy professionals, understand current recommendations and patient-specific considerations for use. This review begins with a summary of recent guidance on the use of GLP-1 RAs in patients with T2D followed by an overview of clinical considerations for use. Lastly, concepts discussed within this review will be applied to a case scenario.
| Figure 1. The Ominous Octet: Multiple Pathophysiologic Defects in Type 2 Diabetes3 |
 |
RECENT GUIDANCE ON THE USE OF GLP-1 RAs IN PATIENTS WITH T2D
In consideration of recently reported cardiovascular and renal outcome data, multiple organizations have published updated guidance over the last several years regarding the use of glucose-lowering agents in patients with T2D to mitigate cardiovascular and renal risks. The following sections provide a brief summary of key guidance published since 2018.
American College of Cardiology Expert Consensus Decision Pathway on Novel Therapies for Cardiovascular Risk Reduction in Patients with T2D and Atherosclerotic Cardiovascular Disease
In 2018, the American College of Cardiology (ACC) published an expert consensus decision pathway on the use of novel therapies, namely GLP-1 RAs and SGLT-2 inhibitors, to reduce cardiovascular risk in patients with T2D.4 The guidance stresses that not only should patients with T2D and established atherosclerotic cardiovascular disease (ASCVD) receive traditional interventions to lower cardiovascular risk (e.g., lifestyle interventions; antiplatelet therapy; optimization of blood pressure, lipids, and glucose) but they should also use glucose-lowering agents with evidence of cardiovascular risk reduction.
The ACC document, which was endorsed by the American Diabetes Association (ADA), outlined a variety of considerations for use of these agents in patients with ASCVD, including considerations that may warrant selection of either a GLP-1 RA or an SGLT-2 inhibitor for cardiovascular risk reduction (Table 1).4 The ACC document additionally provided a series of “opportunities” in which clinicians may consider starting a GLP-1 RA or an SGLT-2 inhibitor with demonstrated cardiovascular benefit4 :
- In a patient with T2D and ASCVD;
- At the time of diagnosis of clinical ASCVD in a patient with T2D on a drug regimen that does not include a GLP-1 RA or an SGLT-2 inhibitor with demonstrated cardiovascular benefit;
- At the time of diagnosis of T2D in a patient with clinical ASCVD; and
- At hospital discharge after admission for an ASCVD- or diabetes-related clinical event.
| Table 1. Considerations for Using GLP-1 RAs and SGLT-2 Inhibitors for Cardiovascular Risk Reduction: American College of Cardiology Recommendations4 |
| Consider Using a GLP-1 RA First when Patient and Clinician Priorities Include: |
Consider Using an SGLT-2 Inhibitor First when Patient and Clinician Priorities Include: |
| Reducing MACE and cardiovascular death |
Reducing MACE and cardiovascular death |
| Substantial weight loss |
Preventing heart failure hospitalization |
| Once-weekly dosing |
Reducing blood pressure |
| When eGFR is consistently < 45 mL/min/1.73 m2 |
Orally administered therapy |
Consider alternative agents if:
• Persistent nausea, even at low doses
• History of pancreatitis
• History of gastroparesis
• History of MEN2 or medullary thyroid cancer
• History of proliferative retinopathy (semaglutide) |
Consider alternative agents if:
• Significant CKD
• History of prior amputation, severe PAD, neuropathy, or foot ulcers (canagliflozin)
• History of recurrent genital candidiasis
• History of diabetic ketoacidosis
• History of osteoporosis (canagliflozin) |
| CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; GLP-1 RA, glucagon-like peptide-1 receptor agonist; MACE, major adverse cardiovascular events; MEN2, multiple endocrine neoplasia type 2; PAD, peripheral arterial disease; SGLT-2, sodium-glucose co-transporter 2. |
While several cardiovascular and renal outcome studies have been reported since publication of the 2018 ACC decision pathway, the document remains useful in terms of providing patient-specific considerations when determining which class of medications to select in a person with T2D.
Update to Management of Hyperglycemia in T2D: A Consensus Report by the ADA and the European Association for the Study of Diabetes
The ADA and the European Association for the Study of Diabetes (EASD) also revised their joint consensus on the management of hyperglycemia in T2D in 2018.5 The 2018 update focused heavily on the use of glucose-lowering agents to mitigate cardiovascular and renal risks in the context of meeting individualized glycemic goals.
The ADA/EASD recently published a 2019 update to the 2018 consensus report.6 A simplified version of the algorithm for use of glucose-lowering agents in T2D is illustrated in Figure 2. It should be noted that Figure 2 is a simplified representation of the overall approach recommended by the ADA/EASD and includes only recommendations up to the point of dual antihyperglycemic therapy. This algorithm is additionally included in the 2020 ADA Standards of Medical Care in Diabetes and is discussed in additional detail below. Please refer to the full 2020 ADA Standards of Care for additional details and recommendations regarding intensification of therapy beyond dual antihyperglycemic therapy.7
| Figure 2. American Diabetes Association/European Association for the Study of Diabetes Recommendations for Intensification to Dual Glucose-Lowering Therapy6,7 |
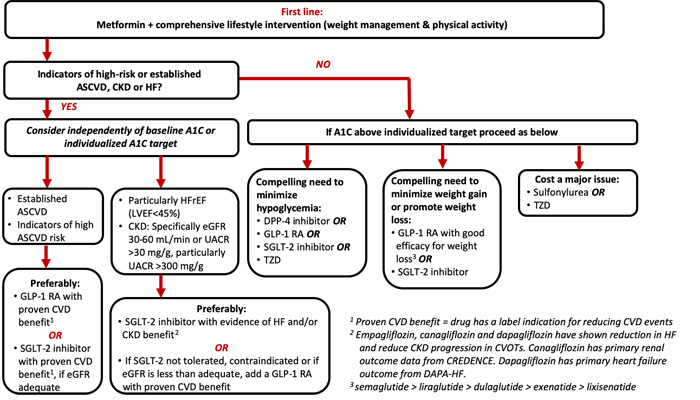 |
| A1C, glycated hemoglobin; ASCVD, atherosclerotic cardiovascular disease; CKD, chronic kidney disease; CVD, cardiovascular disease; DPP-4, dipeptidyl peptidase-4; eGFR, estimated glomerular filtration rate; GLP-1 RA, glucagon-like peptide-1 receptor agonist; HF, heart failure; HFrEF, heart failure with reduced ejection fraction; LVEF, left ventricular ejection fraction; SGLT-2, sodium-glucose co-transporter 2; TZD, thiazolidinedione, UACR, urinary albumin-to-creatine ratio. |
ADA Standards of Medical Care in Diabetes
The ADA annually updates its Standards of Medical Care in Diabetes. The 2020 Standards of Medical Care include some notable updates related to patient-centered care and the use of glucose-lowering agents.7 Notably, the Standards of Care emphasize a shared decision-making approach in which patients and caregivers are actively involved in care decisions as integral members of the care team. The Standards note that the goal of provider-patient communication is to establish a collaborative relationship that allows for the assessment of self-management barriers without blaming patients for “noncompliance” or “nonadherence” when outcomes are less than optimal.7 To emphasize this approach to care, the 2020 Standards include a “decision cycle for patient-centered glycemic management in type 2 diabetes.” The ADA recommends that the decision cycle be undertaken at least once or twice annually to reevaluate patient needs and avoid clinical inertia such that patient-specific treatment goals can be achieved.7 Figure 3 provides a simplified summary of the decision cycle.7
| Figure 3. Key Elements of the Decision Cycle for Patient-Centered Glycemic Management in Type 2 Diabetes*7 |
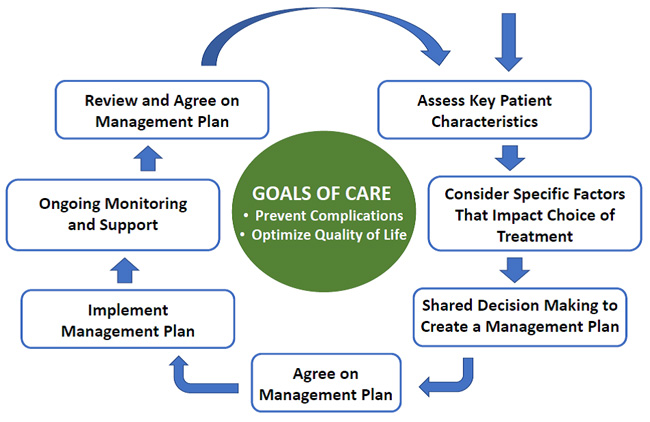 |
| * Undertake the decision cycle regularly (at least once or twice per year) |
The ADA continues to recommend metformin in conjunction with lifestyle interventions as first-line therapy in patients with T2D.7 In line with the overall theme of patient-centered care, the ADA’s recommendations for intensification beyond metformin monotherapy include careful consideration of patient- and drug-related factors when determining the best regimen for a given patient.7 The following sections will discuss the overall approach to intensification of glucose-lowering agents, as illustrated in Figure 2, with an emphasis on the role of GLP-1 RAs within the current recommendations.
Patients with indicators of high-risk or established ASCVD, chronic kidney disease, or heart failure
According to the ADA, when considering an agent for add-on to metformin background therapy, the first recommended consideration is whether or not the patient has indicators of high-risk or established ASCVD, chronic kidney disease (CKD), or heart failure (Figure 2).7 If a patient meets these criteria, it is recommended that the addition of an agent with evidence for cardiovascular or renal risk reduction be considered independent of the patient’s current A1C or A1C target. That is, the ADA recommends that one of these agents be considered as add-on therapy irrespective of the need for glucose lowering. The ADA also states that these recommendations are actionable whenever these comorbidities become new clinical considerations regardless of background glucose-lowering medications.7 The following further describes drug-specific recommendations from the ADA based on whether ASCVD or CKD/heart failure predominates clinically.
When ASCVD predominates: ASCVD is considered to predominate if a patient has established ASCVD or if they have indicators of high ASCVD risk. Indicators of high risk include being 55 years of age or older with coronary, carotid, or lower extremity artery stenosis of more than 50% or with left ventricular hypertrophy.7 In patients who meet these criteria, the ADA preferably recommends use of a GLP-1 RA with proven cardiovascular benefit or an SGLT-2 inhibitor with proven cardiovascular benefit provided they have adequate kidney function. At the time of this writing, liraglutide is the only GLP-1 RA with a labeled indication to reduce the risk of major adverse cardiovascular events (MACE), yet several other GLP-1 RAs have shown significant reduction in MACE, as summarized in Table 2.8-13 For a detailed discussion of cardiovascular outcome trials (CVOTs) completed with agents from the GLP-1 RA class, please refer to the companion lesson titled: “What do we Currently Know about the Cardiovascular Benefits of GLP-1 RAs? A Primer for Pharmacists.”
| Table 2. Cardiovascular Outcome Trials of Currently Available GLP-1 RAs8-13 |
| |
ELIXA
(n = 6068) |
LEADER
(n = 9340) |
SUSTAIN-6
(n = 3297) |
EXSCEL
(n = 14,752) |
REWIND
(n = 9901) |
PIONEER 6
(n = 3183) |
| Agent |
Lixisenatide |
Liraglutide |
Semaglutide |
Exenatide XR |
Dulaglutide |
Oral semaglutide |
| Median follow-up (years) |
2.1 |
3.8 |
2.1 |
3.2 |
5.4 |
1.3 |
| Metformin use (%) |
66 |
76 |
73 |
77 |
81 |
77 |
| Prior CVD (%) |
100 |
81.3 |
58.8 |
73.1 |
31.5 |
85 |
| Mean baseline A1C (%) |
7.7 |
8.7 |
8.7 |
8.0 |
7.2 |
8.2 |
| Primary outcome |
4-point MACE
1.02
(0.89–1.17) |
3-point MACE
0.87
(0.78–0.97) |
3-point MACE
0.74
(0.58–0.95) |
3-point MACE
0.91
(0.83–1.00) |
3-point MACE
0.88
(0.79–0.99) |
3-point MACE
0.79
(0.57–1.11)* |
| Cardiovascular death |
0.98
(0.78–1.22) |
0.78
(0.66–0.93) |
0.98
(0.65–1.48) |
0.88
(0.76–1.02) |
0.91
(0.78–1.06) |
0.49
(0.27–0.92) |
| MI |
1.03
(0.87–1.22) |
0.86
(0.73–1.00) |
0.74
(0.51–1.08) |
0.97
(0.85–1.10) |
0.96
(0.79–1.15) |
1.18
0.73–1.90) |
| Stroke |
1.12
(0.79–1.58) |
0.86
(0.71–1.06) |
0.61
(0.38–0.99) |
0.85
(0.70–1.03) |
0.76
(0.61–0.95) |
0.74
(0.35–1.57) |
| All-cause mortality |
0.94
(0.78–1.13) |
0.85
(0.74–0.97) |
1.05
(0.74–1.50) |
0.86
(0.77–0.97) |
0.90
(0.80–1.01) |
0.51
(0.31–0.84) |
| Worsening nephropathy |
- |
0.78
(0.67–0.92) |
0.64
(0.46–0.88) |
- |
0.85
(0.77–0.93) |
- |
A1C, glycated hemoglobin; CVD, cardiovascular disease; GLP-1 RAs, glucagon-like peptide-1 receptor agonists; MACE, major adverse cardiovascular events; MI, myocardial infarction; XR, extended release.
*P<0.001 for noninferiority; P=0.17 for superiority. |
When CKD or heart failure predominates: For patients with clinically predominant CKD or heart failure, use of an SGLT-2 inhibitor with evidence of reducing heart failure and/or CKD progression are preferably recommended.7 If an SGLT-2 inhibitor cannot be taken due to a contraindication to therapy, drug intolerance, or insufficient kidney function, the ADA recommends the addition of a GLP-1 RA (Figure 2). These recommendations are particularly recommended in patients with heart failure with reduced ejection fraction (left ventricular ejection fraction < 45%) and in CKD patients with an estimated glomerular filtration rate (eGFR) of 30 to 60 mL/min/1.73 m2 or a urinary albumin-to-creatinine ratio (UACR) above 30 mg/g.7
Patients without indicators of high-risk or established ASCVD, CKD, or heart failure
For patients without indicators of high-risk or established ASCVD, CKD, or heart failure, the addition of glucose-lowering agents is based on the need for additional glucose lowering to meet individualized A1C goals.7 As shown in Figure 2, the decision of which agent(s) to add to the regimen is based on 1 or more of 3 primary considerations: 1) need to minimize hypoglycemia, 2) need to minimize weight gain or promote weight loss, and 3) need to minimize medication costs. In consideration of their low risk of contributing to hypoglycemia and the potential for weight loss with treatment, GLP-1 RAs are recommended for consideration when it is desired to minimize hypoglycemia risk or minimize weight gain/promote weight loss.7 For patients for whom the cost of newer medications is prohibitive, the ADA recommends use of sulfonylureas and thiazolidinediones.
Patients requiring injectable glucose-lowering therapy to meet individualized glycemic goals
Another key figure within the 2020 ADA Standards of Care relates to intensification of injectable glucose-lowering agents in patients with T2D.7 Figure 4 provides a simplified summary of the ADA’s recommendations. Notably, the ADA recommends that, in patients requiring an injectable agent to meet individualized goals, an injectable GLP-1 RA be considered preferentially over insulin in most patients.7 If patients are already on an injectable GLP-1 RA or if insulin is preferred, however, it is recommended that patients be initiated on basal insulin. Information is provided below about combination products that contain both a GLP-1 RA and basal insulin that can be considered in select patients who could benefit from combination injectable therapy.14,15
| Figure 4. American Diabetes Association Recommendations for Intensifying to Injectable Therapies7 |
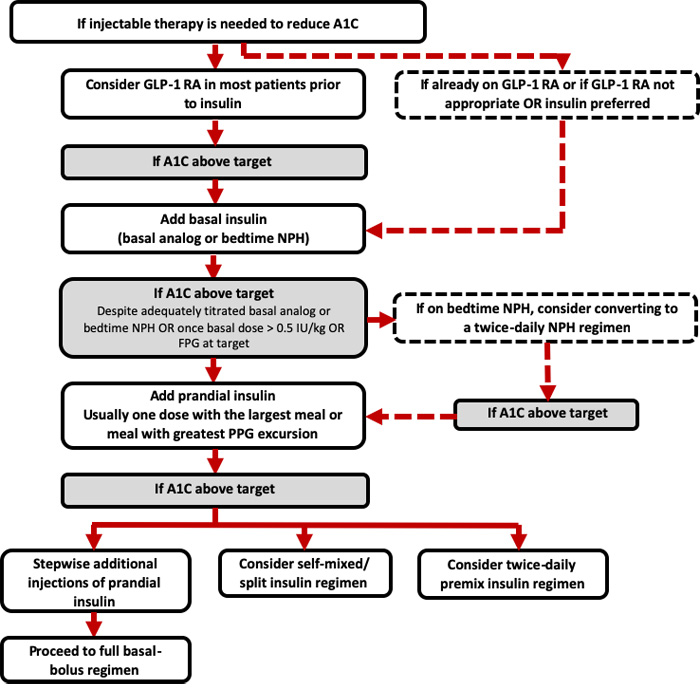 |
| A1C, glycated hemoglobin; FPG, fasting plasma glucose; GLP-1 RA, glucagon-like peptide-1 receptor agonist; NPH, neutral protamine Hagedorn; PPG, postprandial glucose. |
Summary of ADA Standards of Medical Care
The following are key treatment recommendations from the 2020 ADA Standards of Medical Care regarding the pharmacologic approach to glycemic treatment7 :
- Metformin is the preferred initial pharmacologic agent for the treatment of T2D.
- Once initiated, metformin should be continued as long as it is tolerated and not contraindicated; other agents, including insulin, should be added to metformin.
- A patient-centered approach should be used to guide the choice of pharmacologic agents; considerations include cardiovascular comorbidities, hypoglycemia risk, impact on weight, cost, risk for side effects, and patient preferences.
- Among patients with T2D who have established ASCVD or heart failure, an SGLT-2 or GLP-1 RA with demonstrated cardiovascular disease benefit is recommended as part of the glucose-lowering regimen independent of A1C and in consideration of patient-specific factors.
- For patients with T2D and diabetic kidney disease, consider use of an SGLT-2 inhibitor in patients with an eGFR ≥ 30 mL/min/1.73 m2 and a UACR > 30 mg/g, particularly in those with a UACR > 300 mg/g, to reduce the risk of CKD progression, cardiovascular events, or both. In patients with CKD who are at increased risk for cardiovascular events, use of a GLP-1 RA may reduce the risk of progression of albuminuria, cardiovascular events, or both.
- In patients with T2D who need greater glucose lowering than can be obtained with oral agents, GLP-1 RAs are preferred to insulin when possible.
- The medication regimen and medication-taking behavior should be reevaluated at regular intervals (every 3-6 months) and adjusted as needed to incorporate specific factors that impact the choice of treatment.
For additional details and discussion regarding pharmacologic approaches to glycemic management, please refer to the full 2020 ADA Standards of Medical Care.7
BRIEF OVERVIEW OF CURRENT GLP-1 RA PRODUCTS
GLP-1 RAs mimic a naturally occurring hormone that plays a role in glycemic control. The myriad of effects of endogenous glucagon-like peptide-1 (GLP-1) make it an attractive target for diabetes therapy. The following sections review the pharmacology and clinical characteristics of currently available GLP-1 RAs that should be considered when applying the clinical recommendations discussed above to individual patients with T2D.
Pharmacology of GLP-1 RAs
Endogenous GLP-1 is secreted from intestinal L-cells following oral nutrient intake. The beneficial effects of GLP-1 receptor activation on glycemia occur through several mechanisms: GLP-1 stimulates glucose-dependent insulin secretion from pancreatic ß-cells, suppresses inappropriately elevated glucagon secretion from pancreatic α-cells, delays gastric emptying, and induces satiety via a direct action in the central nervous system.16 Because the therapeutic potential of natural GLP-1 is limited due to its rapid degradation by the enzyme dipeptidyl peptidase 4 (DPP-4), GLP-1 analogs have been developed that are DPP-4 resistant.17
Currently available GLP-1 RAs can be divided generally into 2 main categories on the basis of their pharmacokinetics: short- and long-acting agents. Exenatide and lixisenatide both have relatively short half-lives and are considered short-acting GLP-1 RAs. Short-acting agents demonstrate strong effects on gastric emptying and are associated with strong postprandial glucose effects.18 Long-acting GLP-1 RAs include liraglutide, dulaglutide, exenatide XR, and semaglutide. Because these agents are longer-acting, they produce more consistent activation of GLP-1 receptors.18 Longer-acting GLP-1 RAs are associated with less robust effects on postprandial glucose and greater effects on fasting glucose. Table 3 provides a summary of key dosing and administration information for currently marketed GLP-1 RAs.19-25
| Table 3. Key Characteristics of Currently Available GLP-1 RAs19-25 |
| |
Short-acting |
Long-acting |
| |
Exenatide |
Lixisenatide |
Liraglutide |
Exenatide XR |
Dulaglutide |
Semaglutide
(injectable) |
Semaglutide
(oral) |
| Recommended dosing |
• Initiate at 5 mcg twice daily
• Increase to 10 mcg twice daily after 1 month according to clinical response |
• Initiate at 10 mcg once daily for 14 days, then increase to 20 mcg daily |
• Initiate at 0.6 mg per day for 1 week, then increase to 1.2 mg
• May increase to 1.8 mg (after at least 1 week of 1.2-mg dose) for additional glycemic control |
• Administer 2 mg once weekly |
• Initiate at 0.75 mg once weekly
• May increase to 1.5 mg for additional glycemic control |
• Initiate at 0.25 mg once weekly, then, after 4 weeks, increase to 0.5 mg once weekly
• May increase to 1 mg (after at least 4 weeks of 0.5-mg dose) for additional glycemic control |
• Initiate at 3 mg once daily for 30 days, then 7 mg once daily
• May increase to 14 mg once daily (after at least 30 days on 7-mg dose) for additional glycemic control |
| Indication(s) |
• Adjunct to diet and exercise to improve glycemic control in T2D |
• Adjunct to diet and exercise to improve glycemic control in T2D |
• Adjunct to diet and exercise to improve glycemic control in T2D
• To reduce the risk of MACE in adults with T2D and established CVD |
• Adjunct to diet and exercise to improve glycemic control in T2D |
• Adjunct to diet and exercise to improve glycemic control in T2D |
• Adjunct to diet and exercise to improve glycemic control in T2D
• To reduce the risk of MACE in adults with T2D and established CVD |
• Adjunct to diet and exercise to improve glycemic control in T2D |
| Administration frequency |
Twice daily |
Once daily |
Once daily |
Once weekly |
Once weekly |
Once weekly |
Once daily |
| Administration timing |
Take within 60 minutes before meals |
Take within 60 minutes before morning meal |
Take at the same time each day |
Take on the same day each week |
Take on the same day each week |
Take on the same day each week |
Take at least 30 minutes before breakfast |
| Pen availability |
Multi-use pen |
Multi-use pen |
Multi-use pen |
Single-use pen |
Single-use pen |
Multi-use pen |
N/A |
| CVD, cardiovascular disease; GLP-1 RAs, glucagon-like peptide-1 receptor agonists; MACE, major adverse cardiovascular events; N/A, not applicable; T2D, type 2 diabetes mellitus; XR, extended release. |
General safety and tolerability considerations of GLP-1 RAs
The most common side effects associated with GLP-1 RA use are nausea, diarrhea, and headache. These side effects tend to be most prominent at the initiation of therapy and improve with continued use in many patients. These side effects can usually be reduced by initiating the medication at a low dose and titrating slowly. In addition, nausea may be reduced by eating smaller portions.
The risk of hypoglycemia with GLP-1 RAs is low when used as monotherapy.7 However, the risk of hypoglycemia increases when GLP-1 RAs are administered concomitantly with insulin or insulin secretagogues. The manufacturers of GLP1-RAs typically recommend lowering doses of insulin and insulin secretagogues at the initiation of GLP-1 RA treatment to reduce the risk of hypoglycemia.19-25 The GLP-1 RA and insulin secretagogue/insulin doses can subsequently be titrated on the basis of individualized needs to achieve the desired level of glycemic control.
GLP-1 RAs have been associated with the development of pancreatitis. Causality has not been established, but these agents should be used cautiously in patients with a history of pancreatitis. Preclinical studies in rodents have also shown a relationship between GLP-1 RAs and the development of thyroid c-cell tumors, including medullary thyroid carcinoma (MTC). As such, these agents are generally contraindicated in patients with a personal or family history of MTC and in patients with multiple endocrine neoplasia syndrome type 2 (MEN2).19-25 Table 4 provides a summary of key warnings and precautions listed in the labeling of each GLP-1 RA product that should be taken into account when considering use in a patient with T2D.19-25
| Table 4. Select Warnings and Precautions for Currently Available GLP-1 RAs19-25 |
| Warning/precaution |
Agent |
| Exenatide |
Lixisenatide |
Liraglutide |
Exenatide XR |
Dulaglutide |
Semaglutide
(injectable) |
Semaglutide
(oral) |
| Pancreatitis |
X |
X |
X |
X |
X |
X |
X |
| Hypoglycemia (when used in combination with SU or insulin) |
X |
X |
X |
X |
X |
X |
X |
| Renal impairment/AKI |
X |
X |
X |
X |
X |
X |
X |
| Severe GI disease |
X |
|
|
X |
X |
|
|
| Hypersensitivity reactions |
X |
X |
X |
X |
X |
X |
X |
| Immunogenicity (anti-drug antibody production) |
|
X |
|
X |
|
|
|
| Thyroid c-cell tumors |
|
|
X |
X |
X |
X |
X |
| Injection-site reactions |
|
|
|
X |
|
|
|
| Acute gallbladder disease |
|
|
X |
X |
|
|
|
| Diabetic retinopathy complications |
|
|
|
|
|
X |
X |
| AKI, acute kidney injury; GI, gastrointestinal; GLP-1 RAs, glucagon-like peptide-1 receptor agonists; SU, sulfonylurea; XR, extended release. |
Recently approved GLP-1 RA products
Several new GLP-1 RA products have been introduced to the market in recent years. The following section provides a review of the most recent GLP-1 RA products approved in the U.S.: oral semaglutide and the fixed-ratio GLP-1 RA/basal insulin combination products.
Oral semaglutide
Oral semaglutide received approval from the U.S. Food and Drug Administration (FDA) in September 2019 for use as an adjunct to diet and exercise to improve glycemic control in adults with T2D.25 The product is available in 3-, 7-, and 14-mg tablet strengths. The manufacturer recommends initiating oral semaglutide at 3 mg once daily; after 30 days, the dose may be increased to 7 mg once daily. For patients requiring additional glycemic lowering, the dose can be further up-titrated to 14 mg once daily after taking the 7 mg dose for at least 30 days. Notably, the manufacturer has filed with the FDA for a second indication to reduce MACE in adults with T2D and established cardiovascular disease.26 According to a manufacturer press release, the FDA review for the MACE indication is expected to be completed in the first quarter of 2020.26
Oral semaglutide is co-formulated with the absorption enhancer sodium N-(8-[2-hydroxylbenzoyl] amino) caprylate – or “SNAC.”27 Co-formulation with SNAC helps facilitate semaglutide absorption in the stomach by increasing the local pH, which, in turn, leads to increased drug solubility and protection against proteolytic degradation.28 Oral administration does not appear to diminish the glucose-lowering or weight-lowering efficacy of semaglutide,29 with oral semaglutide comparing favorably when studied against the SGLT-2 inhibitor empagliflozin.30 In terms of cardiovascular safety, oral semaglutide was shown to be noninferior to placebo in the PIONEER 6 trial.13
As the first orally administered GLP-1 RA, oral semaglutide provides an option for patients unwilling or unable to self-inject. It should be noted, however, that oral semaglutide does require care upon administration to ensure proper absorption. Patients taking oral semaglutide should be instructed to ingest the tablet at least 30 minutes before the first food, beverage, or other oral medications of the day with no more than 4 ounces of plain water only.25 The prescribing information notes that waiting less than 30 minutes or taking with food, beverages other than plain water, or other oral medications will lessen the effect of the product. Conversely, waiting more than 30 minutes to eat may increase drug absorption. Oral semaglutide tablets should also not be crushed or chewed.25
Basal insulin–GLP-1 RA fixed-ratio combination injectables
Two fixed-ratio combination (FRC) products containing a basal insulin and a GLP-1 RA are also available as options for patients being managed on combination injectable therapy (Table 5).14,15 These products provide an option for patients who could benefit from use of both medication classes with a single daily injection, which has adherence benefits for some patients. Another potential advantage of this combination is mitigation of insulin-associated weight gain when used in combination with a GLP-1 RA.
| Table 5. Fixed-Ratio Basal Insulin Plus GLP-1 RA Combination Products14,15 |
| Product |
Product availability |
Units per pen |
Dose range per injection (pens only) |
Recommended pen storage at room temperature (days) |
| Generic name |
| Insulin glargine/lixisenatide |
Prefilled pen |
300 units
(insulin glargine) |
15-60 units
(insulin glargine) |
28 |
| Insulin degludec/liraglutide |
Prefilled pen |
300 units
(insulin degludec) |
10-50 units
(insulin degludec) |
21 |
| GLP-1 RA, glucagon-like peptide-1 receptor agonist. |
These products have dosing limitations that must be considered and may limit their use in some patients with T2D. The number of units of basal insulin that can be administered with these products is limited by the GLP-1 RA component. Specifically, the insulin glargine/lixisenatide FRC product can provide a maximum of 60 units per injection of basal insulin, and the insulin degludec/liraglutide product can deliver a maximum of 50 units per injection of basal insulin.14,15 Both products carry risks of adverse events that can occur with their component parts. Agent-specific information is summarized below.
Insulin glargine (U-100)/lixisenatide: Insulin glargine/lixisenatide is indicated as an adjunct to diet and exercise to improve glycemic control in adults with T2D.14 The recommended starting dose depends on the background therapy the patient is taking at the time of drug initiation. Of note, the dose is based on the basal insulin component in units. The recommended starting doses are as follows:
- For patients naïve to basal insulin or to a GLP-1 RA, currently on less than 30 units of basal insulin, or on a GLP-1 RA: Start at 15 units subcutaneously once daily within 60 minutes of the first meal of the day.
- For patients inadequately controlled on 30 to 60 units of basal insulin: Start at 30 units subcutaneously once daily within 60 minutes of the first meal of the day.
Insulin degludec (U-100)/liraglutide: Similarly, the insulin degludec/liraglutide FRC product is indicated as an adjunct to diet and exercise to improve glycemic control in adults with T2D.15 The dose of this product is also based on the insulin component in units, and the recommended starting dose is dependent on the patient’s background therapy at the time of drug initiation. The following summarizes the manufacturer’s recommended starting doses for the product:
- For patients naïve to basal insulin or a GLP-1 RA: Start at 10 units subcutaneously once daily without regard to meals.
- For patients currently on basal insulin or a GLP-1 RA: Start at 16 units subcutaneously once daily without regard to meals.
For additional product-specific information on agents from the GLP-1 RA class, please refer to the companion lesson titled: “An Overview of GLP-1 RAs: What Every Pharmacist Should Know.”
PUTTING IT ALL TOGETHER: CASE REVIEW AND DISCUSSION
Case scenario
JM is a 65-year-old man with T2D of 8 years duration. JM is presenting to the pharmacotherapy clinic today following a referral from his primary care provider (PCP). JM’s PCP has requested a medication evaluation, inclusive of a review of his current diabetes care. Upon further discussion with JM, it is determined that he is not opposed to self-injection, but he notes that he experienced frequent hypoglycemic events in the past when he was taking a sulfonylurea and he prefers to take glucose-lowering medications with a low risk of hypoglycemia. JM volunteers that his brother recently died following a myocardial infarction and he is eager to implement changes to minimize his risk of a cardiovascular event following his revascularization procedure in early 2019.
Past medical history:
- T2D
- Hypertension
- Hypercholesterolemia
- History of coronary artery bypass graft (CABG) in January of 2019
- Peripheral vascular disease
- Obesity
Current medications:
- Metformin ER 1000 mg by mouth twice daily
- Linagliptin 5 mg by mouth once daily
- Rosuvastatin 20 mg by mouth once daily
- Lisinopril 20 mg by mouth once daily
- Amlodipine 10 mg by mouth once daily
- ASA (aspirin) 81 mg by mouth once daily
- Multivitamin by mouth once daily
Social history:
- Lives with his wife of 36 years
- Works full time as a software engineer
- Reports no history of tobacco use
- Reports consuming alcohol infrequently; when he does drink, he consumes 1-2 alcoholic beverages
- In terms of lifestyle, JM reports that he “could eat better” and that he engages in limited physical activity (estimated at 30 minutes per week of light walking)
Laboratory and vital findings:
- Weight: 232 pounds (body mass index [BMI] = 34 kg/m2 )
- Blood pressure: 128/84 mmHg (average of 3 seated blood pressure readings)
- Blood glucose: 116 mg/dL (fasting)
- Point-of-care A1C: 7.1%
- Serum creatinine: 1.5 mg/dL
- eGFR: 50 mL/min/1.73 m2
- Sodium: 139 mEq/L
- Potassium: 4.9 mEq/L
- UACR: 60 mg/g (microalbuminuria)
- Low-density lipoprotein cholesterol (LDL-C): 88 mg/dL
- High-density lipoprotein cholesterol (HDL-C): 40 mg/dL
- Triglycerides: 148 mg/dL
Case discussion
JM provided some important information that will be helpful when determining a treatment plan to minimize his cardiovascular risk. First, he appears to be motivated to minimize his risk factors following his CABG in January and the unfortunate passing of his brother. Second, JM is willing to take injectable medications as long as they do not increase his risk for hypoglycemia. Overall, JM appears to be in good metabolic control. His blood pressure and lipids are reasonably controlled, and he is receiving antiplatelet therapy with ASA 81 mg daily. JM self-reports that his lifestyle could be improved in terms of both diet and physical activity, and interventions aimed at achieving weight loss would be beneficial. In terms of his glucose control, JM’s fasting blood glucose is within the recommended general ADA target range of 80 to 130 mg/dL, with a slightly elevated A1C of 7.1%. Of importance, JM has an eGFR of 50 mL/min/1.73 m2 with evidence of microalbuminuria.
So, what interventions could be recommended for JM to mitigate his cardiovascular risk? According to 2020 ADA guidance (Figure 2), and in consideration of JM’s established ASCVD, the addition of a GLP-1 RA with evidence of cardiovascular benefit to JM’s regimen could be considered.7 In line with JM’s priorities for care, this approach could reduce his risk for a future cardiovascular event, promote weight loss, and would be considered to have a low risk for contributing to hypoglycemic events. As outlined in Table 2, several of the injectable GLP-1 RAs have proven superior to placebo for reducing MACE in patients with T2D.8-12 It should also not be forgotten that oral semaglutide is now an option for patients who are not good candidates for injectable glucose-lowering therapy. Also noted in Table 2, several GLP-1 RAs have demonstrated favorable effects on secondary kidney outcomes.8-12 Specifically, the addition of a GLP-1 RA may also confer the added benefit of slowing the progression of albuminuria.31
Potential case recommendations and considerations
It should be acknowledged that there are multiple factors that must be considered when devising a treatment plan for any patient, including evaluation of the patient’s preferences and priorities. In the case of JM, the following treatment plan was agreed upon through the process of shared decision-making and in consideration of current clinical guidance:
- JM was referred to a diabetes educator for diabetes self-management education and support
JM is motivated to make changes to both his lifestyle and medication regimen to decrease his cardiovascular risk. This makes now an ideal time to refer him to a diabetes educator to reinforce his previous diabetes education and formulate a plan to improve his diet and increase his physical activity.
- Injectable semaglutide was started at 0.25 mg once weekly
Even though JM’s A1C is fairly well controlled (7.1%), he has established ASCVD. According to the 2020 ADA Standards of Medical Care in Diabetes, his revascularization procedure in January 2019 is a clinical trigger to consider the addition of a glucose-lowering agent with evidence of cardiovascular benefit. The pros and cons of each available GLP-1 RA were discussed with JM to determine which agent would best meet his goals. JM expressed a preference for once-weekly injection, and, clinically, an agent with demonstrated cardiovascular risk reduction and efficacy for weight loss are indicated. In consideration of JM’s desire for a once-weekly product and a desire to add an agent with proven cardiovascular benefit and notable weight loss, injectable semaglutide was selected and initiated.
- JM’s background metformin was continued
As stressed in the ADA Standards of Care, metformin remains the recommended first-line pharmacologic therapy in patients with T2D and should be continued with the addition of other glucose-lowering therapies in those who can tolerate and do not have a contraindication to metformin therapy.
- JM’s linagliptin prescription was discontinued
Because JM is initiating injectable semaglutide, it was decided to discontinue his DPP-4 inhibitor. Current guidelines do not recommend combination therapy with GLP-1 RAs and DPP-4 inhibitors, and the ADA/EASD consensus report specifically recommends discontinuation of DPP-4 inhibitors when initiating GLP-1 RA therapy.5,6
- JM was scheduled for a phone follow-up in 1 week
JM was provided with a demonstration of appropriate injection technique and use of the semaglutide injection device. He was also counseled on what to expect with the new medication, including the possibility of experiencing gastrointestinal side effects with GLP-1 RA therapy and how to minimize them. JM was encouraged to call the clinic with any questions or concerns. He was additionally scheduled for a phone call 1 week later to follow up on his progress.
CONCLUSION
The expanding selection of glucose-lowering agents and the ever-increasing understanding of the impact of these agents on cardiovascular and renal outcomes provides an opportunity for pharmacy professionals to make a notable impact on patient care. Pharmacists are well suited to advocate for optimal patient care by recommending appropriate agents on the basis of patient-specific considerations and providing appropriate education to people living with T2D. Familiarizing oneself with newly available medications and pertinent counseling information is a critical step toward helping patients effectively utilize their medications to best meet their individualized treatment goals. As additional research becomes available, recommendations related to the use of glucose-lowering agents to optimize glycemic, cardiovascular, and renal outcomes will undoubtedly continue to evolve and inform patient-centered diabetes care.
REFERENCES
- Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2017: Estimates of Diabetes and Its Burden in the United States. https://www.cdc.gov/diabetes/pdfs/data/statistics/national-diabetes-statistics-report.pdf. Published 2017. Accessed December 20, 2019.
- DeFronzo RA. Lilly lecture 1987. The triumvirate: beta-cell, muscle, liver. A collusion responsible for NIDDM. Diabetes. 1988;37(6):667-87.
- DeFronzo RA, Triplitt CL, Abdul-Ghani M, Cersosimo E. Novel agents for the treatment of type 2 diabetes. Diabetes Spectr. 2014;27(2):100-12.
- Das SR, Everett BM, Birtcher KK, et al. 2018 ACC expert consensus decision pathway on novel therapies for cardiovascular risk reduction in patients with type 2 diabetes and atherosclerotic cardiovascular disease: a report of the American College of Cardiology Task Force on Expert Consensus Decision Pathways. J Am Coll Cardiol. 2018;72(24):3200-23.
- Davies MJ, D’Alessio DA, Fradkin J, et al. Management of hyperglycemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2018;41(12):2669-701.
- Buse JB, Wexler DJ, Tsapas A, et al. 2019 update to: Management of hyperglycemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care.
- American Diabetes Association. Standards of Care in Diabetes – 2020. Diabetes Care. 2020;43(Suppl. 1):S1-212.
- Pfeffer MA, Claggett B, Diaz R, et al; ELIXA Investigators. Lixisenatide in patients with type 2 diabetes and acute coronary syndrome. N Engl J Med. 2015;373(23):2247-57.
- Marso SP, Daniels GH, Brown-Frandsen K, et al; LEADER Steering Committee; LEADER Trial Investigators. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2016;375(4):311-22.
- Marso SP, Bain SC, Consoli A, et al; SUSTAIN-6 Investigators. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375(19):1834-44.
- Holman RR, Bethel MA, Mentz RJ, et al; EXSCEL Study Group. Effects of once-weekly exenatide on cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2017;377(13):1228-39.
- Gerstein HC, Colhoun HM, Dagenais GR, et al; REWIND Investigators. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): a double-blind, randomized placebo-controlled trial. Lancet. 2019;394(10193):121-30.
- Husain M, Birkenfeld AL, Donsmark M, et al; PIONEER 6 Investigators. Oral semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2019;381(9):841-51.
- Insulin glargine and lixisenatide (Soliqua®) injection [package insert]. Bridgewater, NJ: Sanofi-aventis U.S.;2019.
- Insulin degludec and liraglutide (Xultophy®) injection [package insert]. Plainsboro, NJ: Novo Nordisk, Inc.;2019.
- Neumiller JJ. Incretin pharmacology: a review of the incretin effect and current incretin-based therapies. Cardiovasc Hematol Agents Med Chem. 2012;10(4):276-88.
- Ahrén B. GLP-1 for type 2 diabetes. Exp Cell Res. 2011;317(9):1239-45.
- Meier JJ. GLP-1 receptor agonists for individualized treatment of type 2 diabetes mellitus. Nat Rev Endocrinol. 2012;8(12):728-42.
- Exenatide (Byetta®) injection [package insert]. Wilmington, DE: AstraZeneca Pharmaceuticals LP;2018.
- Lixisenatide (Adlyxin®) injection [package insert]. Bridgewater, NJ: Sanofi-aventis U.S., LLC.;2019.
- Liraglutide (Victoza®) injection [package insert]. Plainsboro, NJ: Novo Nordisk, Inc.;2019.
- Exenatide extended-release (Bydureon®) injectable suspension [package insert]. Wilmington, DE: AstraZeneca Pharmaceuticals LP;2019.
- Dulaglutide (Trulicity®) injection [package insert]. Indianapolis, IN: Eli Lilly and Company.;2019.
- Semaglutide (Ozempic®) injection [package insert]. Plainsboro, NJ: Novo Nordisk, Inc.;2019.
- Semaglutide (Rybelsus®) tablets [package insert]. Plainsboro, NJ: Novo Nordisk, Inc.;2019.
- Rybelsus® (semaglutide tablets), the first GLP-1 in a tablet approved in the US [press release]. Bagsvaerd, Denmark: Novo Nordisk; September 20, 2019. https://www.novonordisk.com/bin/getPDF.2172050.pdf. Accessed December 20, 2019.
- Buckley ST, Bækdal TA, Vegge A, et al. Transcellular stomach absorption of a derivatized glucagon-like peptide-1 receptor agonist. Sci Transl Med; 2018;10(467).
- Davies M, Pieber TR, Hartoft-Nielsen ML, et al. Effect of oral semaglutide compared with placebo and subcutaneous semaglutide on glycemic control in patients with type 2 diabetes: a randomized clinical trial. JAMA. 2017;318(15):1460-70.
- Pratley R, Amod A, Hoff ST, et al; PIONEER 4 Investigators. Oral semaglutide versus subcutaneous liraglutide and placebo in type 2 diabetes (PIONEER 4): a randomized, double-blind, phase 3a trial. Lancet. 2019;394(10192):39-50.
- Rodbard HW, Rosenstock J, Canani LH, et al; PIONEER 2 Investigators. Oral semaglutide versus empagliflozin in patients with type 2 diabetes uncontrolled on metformin: the PIONEER 2 trial. Diabetes Care. 2019;42(12):2272-81.
- Gerstein HC, Colhoun HM, Dagenais GR, et al; REWIND Investigators. Dulaglutide and renal outcomes in type 2 diabetes: an exploratory analysis of the REWIND randomised, placebo-controlled trial. Lancet. 2019;394(10193):131-8.
Back Top