
Expired activity
Please go to the PowerPak
homepage and select a course.
Hepatitis B: Shortening the Time to Seroprotection in At-Risk Adults
Introduction
Hepatitis B could be considered the "forgotten hepatitis." While much focus has been placed on the current hepatitis C epidemic, hepatitis B is often overlooked and misunderstood, with many missed opportunities to prevent serious liver damage due to chronic hepatitis B virus (HBV) infection.1 Vaccination is highly effective in preventing people from contracting the infection.2 However, many high-risk candidates for the vaccine are not identified and many others do not receive the vaccine—or do not adhere to the full vaccination series to confer adequate protection from the virus. Pharmacists are an important part of the National Viral Hepatitis Action Plan's goal to decrease the number of new HBV infections.3 Many pharmacists administer hepatitis B vaccines, and pharmacists also play an essential role in educating patients and other healthcare providers about the benefits of vaccination, vaccine selection, and administration procedures.4 Questions may arise about what to do if a patient does not complete the series, which vaccines to use for which patients, and whether vaccine types are interchangeable. This program will address these key questions while providing a thorough overview of hepatitis B screening and prevention to enable pharmacists to identify at-risk patients and administer appropriate preventive strategies.
National and Global Impact of Hepatitis B
Worldwide, an estimated 2 billion individuals have been infected with hepatitis B virus (HBV). The World Health Organization (WHO) reports that 257 million persons currently live with chronic, lifelong HBV infection.5,6 On a global basis, HBV is significantly more prevalent than hepatitis B or HIV, as shown in Figure 1.7
| Figure 1. Worldwide Burden of Hepatitis B Viral Infection |
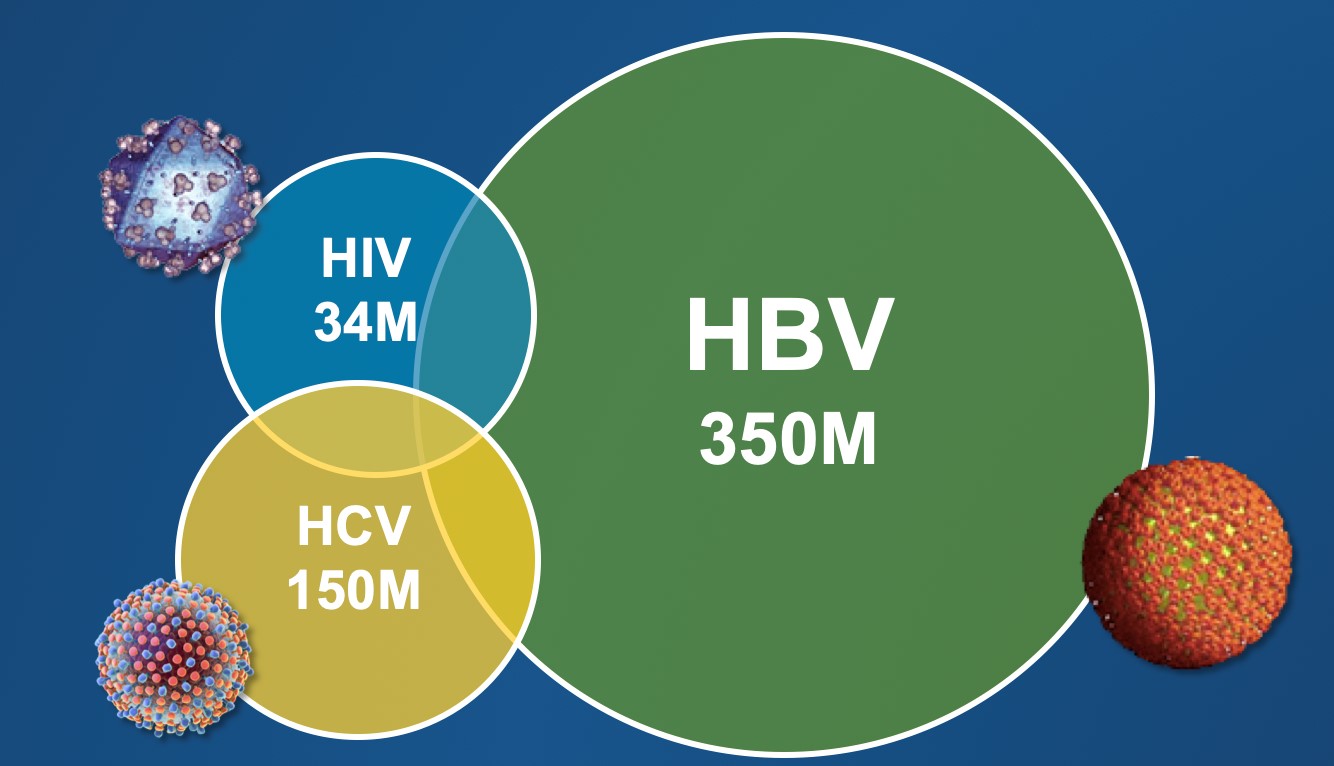 |
| Data adapted from: Matthews P, et al. J Clin Virology. 2014;61:20-33. |
While the prevalence of HBV infection is greatest in African and Asian countries (Figure 2), the impact in this country is still significant.8 Between 850,000 and 2.2 million people in the United States have chronic HBV infection, but only about a third of them are diagnosed and of those, only a third are on treatment.2 Among the overarching goals of the National Viral Hepatitis Action Plan is to increase the proportion of people with chronic HBV who are aware of their infection from 30% to 60%.3
New HBV infections in the U.S. have spiked in recent years. Surveillance data from the Centers for Disease Control and Prevention (CDC) showed nearly 22,000 newly diagnosed cases of acute HBV infection in the U.S. in 2015, an increase of 20.7% from the previous year.9 Acute infection rates tend to be highest among adults aged 30 to 39.10 Much of this new transmission can be attributed to misuse of prescription opioids and intravenous heroin use among persons who inject drugs. In the 7 years from 2006 to 2013, the rate of acute HBV infections increased by 114% in the Appalachian region (Kentucky, Tennessee, and West Virginia) where opioid abuse is prevalent.11
| Figure 2. Global Distribution of Hepatitis B Infection |
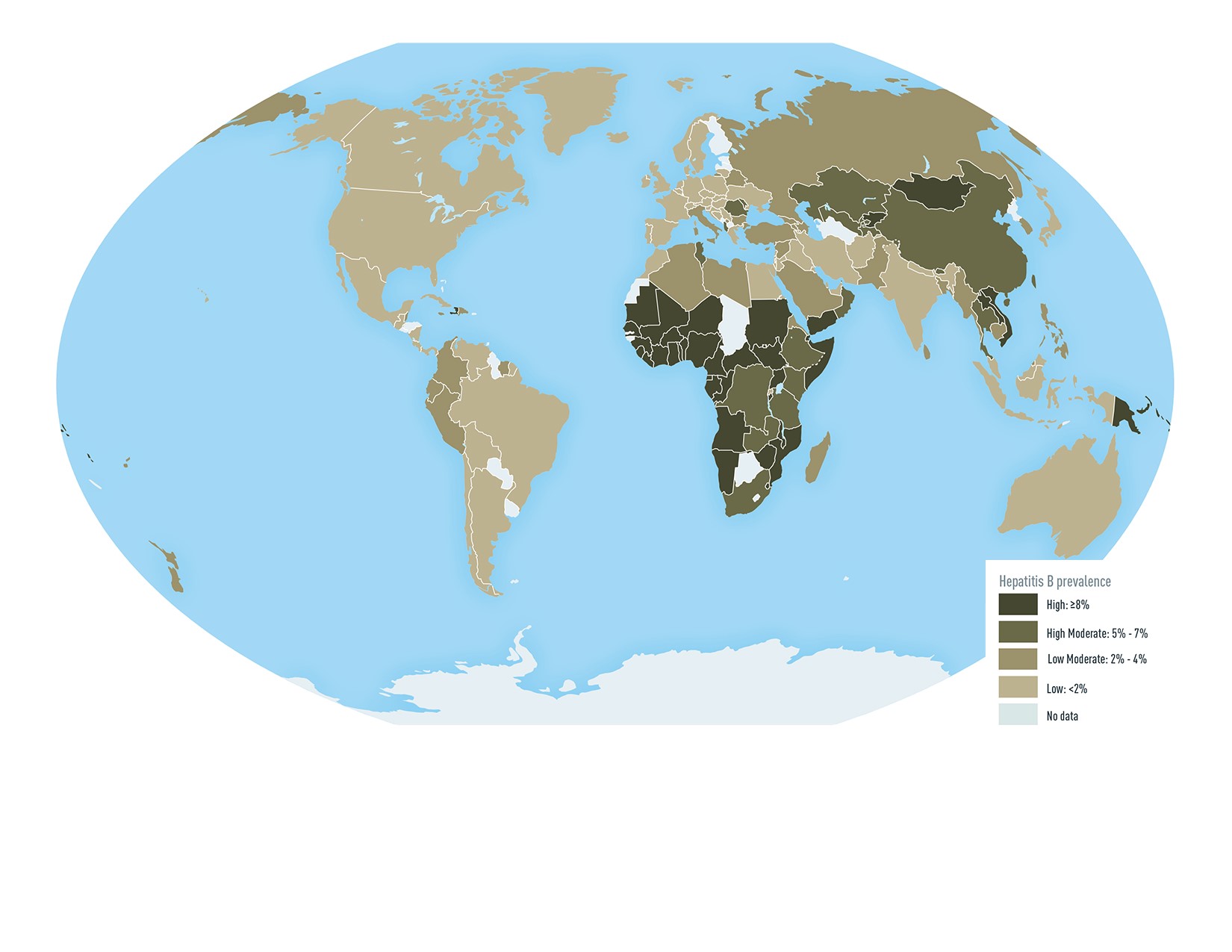 |
| Source: Centers for Disease Control and Prevention (CDC). Chapter 4. Travel-related infectious diseases. In: Yellow Book. Updated July 1, 2019 |
"Diagnosed" is a key word when it comes to describing HBV. According to the CDC, as many as 91% of HBV cases go unreported or undiagnosed (Figure 3),5 and many of the individuals who are infected with HBV are simply unaware that they have this infection.12 HBV infection often remains relatively silent until signs of severe chronic disease appear, such as cirrhosis or end-stage liver disease.
Not everyone who contracts HBV develops a chronic infection. Some cases resolve on their own, but in other cases the person remains an asymptomatic carrier, or a vector for spreading the infection.13 The risk for chronic infection is extremely high in infants—as approximately 90% of those exposed become chronically infected. By comparison, only 2% to 6% of adults who are infected will go on to develop chronic HBV.12 Among those who do develop chronic HBV, a high proportion will develop serious complications including cirrhosis, hepatocellular carcinoma, and/or end-stage liver disease. In untreated individuals with predominantly HBeAg positive chronic hepatitis B, the incidence of cirrhosis ranges from 2 to 5.4 per 100 person-years, with a 5-year cumulative incidence of cirrhosis of 8% to 20%.14
HBV infection accounts for approximately 45% of cases of hepatocellular carcinoma and 30% of all cirrhosis cases.15
Hepatocellular carcinoma and cirrhosis are costly to treat and usually terminal. About 25% of individuals with chronic HBV infection die prematurely from cirrhosis or liver cancer. HBV is associated with about 5,000 deaths annually in the U.S. and nearly 900,000 deaths worldwide.6
These statistics underscore the need for identifying at-risk individuals and vaccinating. Pharmacists can take a proactive role in encouraging high-risk patients to be tested and initiating vaccination where permitted.
What is Hepatitis B?
The hepatitis B virus is an enveloped deoxyribonucleic acid (DNA) virus that infects the liver, triggering hepatocellular necrosis and inflammation.15 HBV is transmitted via exposure to blood, semen, or other body fluids from an infected person.6
HBV is highly infectious—as much as 50 to 100 times more infectious than the human immunodeficiency virus (HIV).6 The virus can survive on environmental surfaces outside of the body for at least 7 days.6 The stages of HBV infection are outlined in Table 1.16 After exposure, there is an incubation period, after which the patient may develop an acute infection. The acute infection resolves on its own in most adults with normal immune status. Acute infection is usually asymptomatic but can range widely, from subclinical disease to fulminant hepatic hepatitis leading to chronic HBV. When symptomatic, the patient with acute HBV may experience fever, fatigue, nausea, and vomiting. These symptoms are usually self-limited and resolve spontaneously without treatment.15 Anorexia, dark urine, and clay-colored stool are symptoms that often prompt people to seek medical advice. In adults, the period of latency (time from acute to chronic infection) may be prolonged for many years. During that time the person can unknowingly transmit the virus to others.17 Those who recover fully will develop lifelong immunity.18 However, if the infection does not resolve, the person may either be a silent carrier or go on to develop chronic HBV with a high risk for serious liver damage.
| Table 1. Trajectory of HBV Infection |
| Exposure |
| Exposure |
Mean incubation period 90 days (60–150 days) from exposure to onset of jaundice |
| Acute infection |
Self-limited
Asymptomatic
Symptomatic |
- About 95% of primary infections in adults with normal immune status
- Immunosuppressed adults
- 30%–50% of adults
|
| Infection Resolves |
| Patient is immune |
| Chronic HBV |
Asymptomatic
Symptomatic |
Patient is a carrier Inflammation, cirrhosis, hepatocellular carcinoma |
| Adapted from: Immunization Action Coalition. Ask the Experts. Hepatitis B. |
Whether or not a person develops chronic infection is dependent on a combination of host, viral, and environmental factors. Groups at higher risk for developing chronic HBV include19,20:
- Infants
- Older males
- Persons with diabetes
- Immunocompromised persons (e.g., coinfection with HIV)
Screening Recommendations and At-Risk Populations in the US
Modes of HBV transmission include sexual contact, sharing needles, syringes, or other equipment for injecting drugs, occupational exposure among healthcare workers, and vertical transmission from mother to infant during birth. Risk factors for transmission of HBV include:9
- Needle-sharing when using injectable drugs
- Sexual contact with infected individuals
- Contact with blood or open sores of infected persons
- Healthcare workers exposed to blood or contaminated body fluids
- Needle sticks
- Diabetes
- Hemodialysis treatment
- Travel to countries with high or intermediate HBV prevalence
| Figure 4. Distribution of Foreign-Born Individuals in the U.S. Living With Chronic HBV Infection |
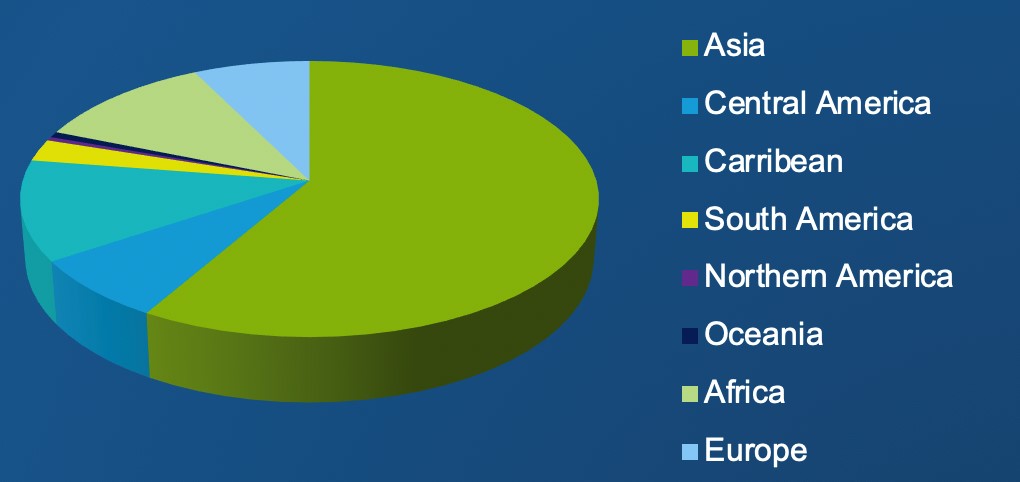 |
| Source: Kowdley KV, Wang CC, Welch S, et al. Prevalence of chronic hepatitis B among foreign-born persons living in the United States by country of origin. Hepatology. 2012;56(2):422-433. |
The National Viral Hepatitis Action Plan was established to focus on reducing the rates of new hepatitis B and C infections, including a goal of decreasing the number of new HBV infections by at least 60% by the year 2020 (Table 2).3 This requires improved surveillance at many levels, including implementation of routine screening in at-risk populations. The CDC has issued recommendations for routine screening in certain high-risk populations, which includes people born in regions where HBV is endemic at high or intermediate levels (HBsAg prevalence ≥2%) (Table 3).18 Among people born in the U.S., routine screening is recommended for those who were not vaccinated as infants and those whose parents were born in regions with high HBV endemicity (HBsAg prevalence ≥8%).20
| Table 2. National Goals for Eradication of HBV Infection |
| Organization |
Goals |
Interventions |
| Centers for Disease Control and Prevention (CDC) |
By 2020:
- Reduce new infections by 60%
- Reduce HBV-related deaths by 20%
- Reduce HBV health disparities
- Coordinate, monitor, and report
|
- Increase awareness by 66%
- Universal HBV vaccination
- Prevent mother-to-child transmission
- Improve access to care
- Implement culturally-competent prevention and care services
|
| National Academies of Sciences, Engineering, and Medicine |
By 2030:
- Reduce HBV-related HCC by 30%
- Reduce HBV-related cirrhosis by 45%
- Reduce HBV-related deaths by 50%
|
- Diagnose 90% of chronic HBV patients
- Link 90% of diagnosed patients to care
- Treat 80% of eligible patients
- Expand access to vaccination
- Increase HBV testing
- Antiviral prophylaxis of HBsAg mothers
|
| Source: National Academies of Sciences, Engineering, and Medicine. Eliminating the Public Health Problem of Hepatitis B and C in the United States: Phase One Report. Washington, DC: The National Academies Press; 2016 |
| Table 3. CDC Recommendations for Routine Testing and Follow-up for Chronic HBV Infection |
| Population |
Testing |
Vaccination/Follow-up |
| Persons born in regions of high and intermediate HBV endemicity (HBsAg prevalence ≥2%) |
Test for HBsAg, regardless of vaccination status in their country of origin, including:
- immigrants
- refugees
- asylum seekers
- internationally adopted children
|
If HBsAg-positive, refer for medical management. If negative, assess for on-going risk for hepatitis B and vaccinate if indicated. |
| U.S.-born persons not vaccinated as infants whose parents were born in regions with high HBV endemicity ≥8%) |
Test for HBsAg regardless of maternal HBsAg status if not vaccinated as infants in the U.S. |
If HBsAg-positive, refer for medical management. If negative, assess for on-going risk for hepatitis B and vaccinate if indicated. |
| Injection-drug users |
Test for HBsAg, as well as for anti-HBc or anti-HBs to identify susceptible persons. |
First vaccine dose should be given at the same visit as testing. Susceptible persons should complete a 3-dose or 2-dose hepatitis B vaccine series to prevent infection from ongoing exposure. |
| Men who have sex with men |
Test for HBsAg, as well as for anti-HBc or anti-HBs to identify susceptible persons. |
First vaccine dose should be given at the same visit as testing.
Susceptible persons should complete a 3-dose or 2-dose hepatitis B vaccine series to prevent infection from ongoing exposure. |
| Persons needing immunosuppressive therapy, including: chemotherapy, immunosuppression related to organ transplantation, and immunosuppression for rheumatologic or gastroenterologic disorders |
Test for all markers of HBV infection (HBsAg, anti-HBc, and anti-HBs). |
Treat persons who are HBsAg-positive. Monitor closely persons who are anti-HBc positive for signs of liver disease. |
| Persons with elevated ALT/AST of unknown etiology |
Test for HBsAg along with other appropriate medical evaluation. |
Follow-up as indicated. |
| Donors of blood, plasma, organs, tissues, or semen |
Test for HBsAg, anti-HBc, and HBV-DNA as required. |
|
| Hemodialysis patients |
Test for all markers of HBV infection (HBsAg, anti-HBc, and anti-HBs). Test vaccine nonresponders monthly for HBsAg. HBsAg-positive hemodialysis patients should be cohorted. |
Vaccinate against hepatitis B to prevent transmission and revaccinate when serum anti-HBs titer falls below 10mIU/mL. |
| All pregnant women |
Test for HBsAg during each pregnancy, preferably in the first trimester. Test at the time of admission for delivery if prenatal HBsAg test result is not available or if mother was at risk for infection during pregnancy. |
If HBsAg-positive, refer for medical management. To prevent perinatal transmission, infants of HBsAg-positive mothers and unknown HBsAg status mothers should receive vaccination and postexposure immunoprophylaxis in accordance with recommendations and within 12 hours of delivery. |
| infants born to HBsAg-positive mothers |
Test for HBsAg and anti-HBs 1–2 mos after completion of a t least 3 doses of a licensed hepatitis B vaccine series (i.e., at age 9–18 months, generally at the next well-child visit to assess effectiveness of postexposure immunoprophylaxis). Testing should not be performed before age 9 months or within 1 month of the most recent vaccine dose. |
Vaccinate in accordance with recommendations. |
| Household, needle-sharing, or sex contacts of persons known to be HBsAg-positive |
Test for HBsAg, as well as anti-HBc or anti-HBs to identify susceptible persons. |
First vaccine dose should be given at the same visit as testing. Susceptible persons should complete a 3-dose or 2-dose hepatitis B vaccine series to prevent transmission from ongoing exposure. |
| Persons who are the sources of blood or body fluids resulting in an exposure (e.g., needlestick, sexual assault) that might require postexposure prophylaxis |
Test source for HBsAg. |
Vaccinate healthcare and public safety workers with reasonably anticipated occupational exposures to blood or infectious body fluids. Provide postexposure prophylaxis to exposed person if needed. |
| HIV-positive persons |
Test for HBsAg, as well as for anti-HBc or anti-HBs to identify susceptible persons. |
Vaccinate susceptible persons against hepatitis B to prevent transmission. |
| Source: Centers for Disease Control and Prevention (CDC). Recommendations for Routine Testing and Follow-up for Chronic Hepatitis B Virus (HBV) Infection. Available at: https://www.cdc.gov/hepatitis/hbv/PDFs/ChronicHepBTestingFlwUp.pdf |
While these guidelines are clearly defined for screening of at-risk populations, there are a number of real-world barriers to screening, some clinician-related and some patient-related. Clinician-related barriers to screening include lack of awareness of current screening recommendations and suboptimal screening rates in at-risk populations. For example, in a 2017 survey of 277 primary care providers in San Francisco (an area with a large Asian immigrant population), only 42% reported screening over 50% of patients who fell into at-risk categories.21 In a survey of 109 physicians in New York City, 53 % answered incorrectly that a 25-year-old patient from China should be screened for HBV.22 Similar findings have been seen in communities with other Asian immigrant populations.23,24
Patient-related barriers to screening may include lack knowledge of HBV transmission, risk factors, and health consequences; a "disconnect" between knowledge of HBV causing serious liver disease and the importance of screening; language barriers; lower socioeconomic status; low level of education; cultural beliefs/values, and stigma about HBV infection, which may occur particularly among East Asians. Many foreign-born adults are difficult to reach with screening/treatment programs, particularly if they are uninsured or are undocumented immigrants.24
Interpretation of Serology
Interpretation of serology is a critical part of the hepatitis B screening and treatment process. It is essential for pharmacists to interpret serology to determine what patients are eligible for immunization. The hepatitis B panel consists of three parts:25
- HBsAg (hepatitis B surface antigen). Positive/reactive result means that the person has active infection and can spread the virus. This could indicate either an acute or a chronic infection.
- Total Anti-HBs or HBsAb (hepatitis surface antibody). Positive/reactive result means that the person is immune to HBV, either due to recovery from a past infection or receiving the vaccine. The individual cannot transmit the virus to others
- Anti-HBc or HBcAb (hepatitis core antibody). Positive/reactive result indicates past or current HBV infection. Unlike the surface antibody, presence of the core antibody does not confer protection against HBV. Interpretation of this serology is based on findings of the previous two parts. Positive core antibody in the presence of both negative surface antigen and surface antibody can occur through a number of different circumstances, detailed under the asterisk* in Table 4.26
Additionally the hepatitis e antigen (HBeAg) is a marker of an actively replicating HBV virus infection. People with positive HBeAg have active replication in their liver cells, more virus circulating in their blood, and thus are more infectious, with a higher likelihood of transmitting HBV to others.25
| Table 4. Interpretation of Serologic Test Results for Hepatitis B Virus Infection |
| CLINICAL STATE |
HBsAg
(Surface Antigen) |
TOTAL ANTI-HBs
(Surface Antibody) |
TOTAL ANTI-HBc
(Core
Antibody) |
RECOMMENDED
ACTION
(CDC and American
College of Physicians) |
| Chronic infection |
Positive |
Negative |
Positive |
Link to hepatitis B-directed care |
| Acute |
Positive |
Negative |
Positive (IgM anti-HBc) |
Link to hepatitis B-directed care |
| Resolved infection |
Negative |
Positive |
Positive |
Counseling, reassurance |
| Immune (immunization) |
Negative |
Positive |
Negative |
Reassurance |
Susceptible (never
infected and no
evidence of
immunization) |
Negative |
Negative |
Negative |
Vaccinate |
| Isolated core antibody |
Negative |
Negative |
Positive |
Depends on situation* |
Source: Abara WE, et al. Hepatitis B vaccination, screening, and linkage to care: best practice advice from the American College of Physicians and the Centers for Disease Control and Prevention. Ann Intern Med. 2017;167(11):794-804.
Abbreviation Key: HBsAg hepatitis B surface antigen; anti-HBs, antibody to hepatitis B surface antigen; hepatitis B-directed care, physical exam and laboratory anti-HBc, antibody to hepatitis B core antigen ALT, evaluation for liver transaminase HBV DNA, and hepatitis B e antigen
*Can be a result of:
- False positive, repeat testing required
- Past infection, no action needed
- Occult HBV infection, needs to be known if patient ever becomes immunosuppressed or given chemotherapy or treated with antiviral therapy for hepatitis C virus infection. Consider monitoring HBV DNA
- Passive transfer to infant born to HBsAg-positive mother; no specific action needed
|
Vaccines for the Prevention of HBV Infection
HBV Vaccine Background
Our ability to identify and prevent HBV all started with the work of late Barry Blumberg, MD, a National Institutes of Health scientist. Blumberg was awarded the 1965 Nobel Prize in Medicine for discovering the hepatitis B virus. His eureka moment came with the discovery of a surface antigen (later identified to be HBV) in a blood sample of an aboriginal Australian with "yellow jaundice." Blumberg was also involved in developing an HBV screening test and the first HBV vaccine.27
The early 1981 HBV vaccine was derived from plasma, but in 1986 this was discontinued in favor of a genetically engineered (DNA recombinant) HBV vaccine. The recombinant HBV vaccines introduced in the 1980s contain aluminum adjuvants, which are commonly utilized in non-live vaccines (including hepatitis A and B, Haemophilusinfluenzae type b, and pneumococcal vaccines) to boost immune response to the vaccine.28 In 2017, a newer HBV vaccine with a novel non-aluminum adjuvant—cytoside phosphoguanine (CpG) 1018—was approved by the FDA.29 The three available vaccines are described below and summarized in Table 5.29-31 Because there are clinically meaningful differences in the dosage of the three HBV vaccines, they are identified by their brand names for clarity.
| Table 5 |
Vaccine
(Manufacturer) |
Recombivax HB
(Merck) |
Engerix-B
(GlaxoSmithKline) |
Heplisav-B
(Dynavax) |
| Contents |
Single antigen, recombinant hepatitis B surface antigen (HBsAg) produced in yeast cells |
Single antigen, recombinant hepatitis B surface antigen (HBsAg) produced in yeast cells |
Single antigen, recombinant hepatitis B surface antigen (HBsAg) produced in yeast cells |
| Adjuvant |
Aluminum adjuvant |
Aluminum adjuvant |
CpG 1018, binds to toll-like receptor 9 to stimulate directed immune response |
| How supplied |
- 0.5-mL (5 mcg) prefilled syringes (pediatric)
- 1-mL (10 mcg) single-dose vials and prefilled syringes (adult);
- 1-mL (40 mcg) single-dose vials (dialysis)
|
- 0.5-mL (10 mcg) prefilled syringes
- 1-mL (20 mcg) single-dose vials and prefilled syringes
|
- Single-dose vial,
0.5 mL
- Single-dose syringe, 0.5 mL
|
| Dosage schedule |
- Birth–19 yrs:
3-dose series (5mcg) at 0, 1, and 6 months;
- Adolescents (age 11 – 15 yrs): Either 3-dose series (5mcg) at 0, 1, and 6 months; or 2-dose series (10mcg) at 0 and 4 to 6 months.
- Adults age ≥20: 3-dose series (10mcg) at 0, 1, and 6 months
- Adults on hemodialysis: 3-dose series (40mcg) at 0, 1, and 6 months.
|
- Birth – 19 yrs:
3-dose series (10mcg) at 0, 1, and 6 months;
- Adults ≥ age 20:
3-dose series (20mcg) at 0, 1, and 6 months;
- Adults on hemodialysis: 4-dose series (40mcg each) at 0, 1, 2, and 6 months.
|
- Adults age ≥18:
First dose (0.5 mL), second dose 1 month later
- Not studied in hemodialysis or pediatric population
|
Traditional recombinant vaccines (aluminum adjuvant)
Recombivax HB
Recombivax HB is a recombinant vaccine for HBV initially approved in 1986. The vaccine is available in 0.5-mL (5 mcg) prefilled syringes (pediatric formulation); 1-mL (10 mcg) single-dose vials and prefilled syringes (adult formulation); and 1-mL (40 mcg) single-dose vials (dialysis formulation). The dosage schedule requires a 2- or 3-injection series as shown below:31
- Birth through 19 years: 3-dose series (5ug) at 0, 1, and 6 months
- Adolescents (age 11 through 15 years): Either a 3-dose series (5ug) at 0, 1, and 6 months; or 2-dose series (10ug) at 0 and 4 to 6 months.
- Adults age 20 and older: 3-dose series (10ug) at 0, 1, and 6 months
- Adults on hemodialysis: 3-dose series (40ug) at 0, 1, and 6 months.
Engerix-B
Engerix-B is a recombinant vaccine for HBV initially approved in 1989. The vaccine is available in 0.5-mL (10 mcg) prefilled syringes and 1-mL (20 mcg) single-dose vials and prefilled syringes. The dosage schedule requires a 3- or 4-injection series as shown below:30
- Birth through 19 years: 3-dose series (10ug) at 0, 1, and 6 months
- Adults age 20 and older: 3-dose series (20ug) at 0, 1, and 6 months
- Adults on hemodialysis: 4-dose series (40ug each) at 0, 1, 2, and 6 months.
Non-aluminum adjuvant, 2-dose vaccine
Heplisav-B
Heplisav-B is a single-antigen HBV vaccine approved by the FDA in November 2017. This vaccine differs from the two formulations listed above (Recombivax and Engerix) because it utilizes a non-aluminum adjuvant not contained in any other U.S. vaccines to date.32 Other key differences between Heplisav-B and the older recombinant vaccines are its dosage schedule (with a standard 2-dose series instead of 3) and the age range (approved for adults only), as shown below:29
- Supplied as single-dose vial or prefilled syringe. A single dose is 0.5 mL.
- Dosage schedule, adults age 18 or older: 2 (two) doses (0.5 mL each) administered one month apart.
The adjuvant, CpG 1018, is thought to work by activating dendritic cells and promoting T-helper (Th1) cell differentiation. This activation appears to produce higher, sustained antibody responses, by generating large numbers of anti-HBsAg-secreting plasmacytes and HBsAg-specific memory cells.33 Relative to the other HBV vaccines, Heplisav-B has been shown to stimulates improved seroprotection. FDA approval of hepatitis B vaccine recombinant–adjuvanted was based on data from three pivotal Phase 3 trials involving nearly 10,000 adults.29 In the largest phase 3 trial (N=6,665), Heplisav-B had a statistically significant higher rate of protection relative to the active comparator, Engerix-B (95.4% vs 81.3% for Engerix-B).29
| Table 5. Available Hepatitis B Vaccines |
 |
| Source: Kowdley KV, Wang CC, Welch S, et al. Prevalence of chronic hepatitis B among foreign-born persons living in the United States by country of origin. Hepatology. 2012;56(2):422-433. |
Special Considerations for HBV vaccines
Interchangeability
With three HBV vaccines available and some differences in the dosage forms and dosage schedules, an area of potential confusion is the interchangeability of the vaccines. In particular, interchangeability may be a problem when the patient returns for a second dose and there is no record of which vaccine he or she initially received, or the pharmacy does not have the appropriate stock on hand (See Case Presentation 1). Ideally, when feasible, the same manufacturer’s vaccine should be used to complete a full HBV vaccine series. However, if the prior manufacturer is unknown or that vaccine is unavailable, the patient should complete the series of 3 doses using the longest recommended dosing interval, with the assumption that an traditional recombinant vaccine (Recombivax or Engerix) was used. According to the Advisory Committee on Immunization Practices:34
- Dose 1 and Dose 2 should be separated by at least 4 weeks. Dose 2 and Dose 3 should be separated by at least 8 weeks. Dose 1 and Dose 3 should be separated by at least 16 weeks.
- Any doses separated by a shorter interval would need to be repeated.
With the 2-dose hepatitis B vaccine (Heplisav-B), any series that contains 2 doses of this vaccine, separated by at least 4 weeks, is considered appropriate.34
Safety and tolerability
Contraindications to the HBV vaccine include severe allergic reaction, such as anaphylaxis, after a previous dose of any hepatitis B vaccine or to any component of the vaccine, including yeast.29-31 The most common adverse reactions reported for the vaccines are injection site pain or soreness and systemic reactions including fatigue (11% to 17%) and headache (8% to 17%).
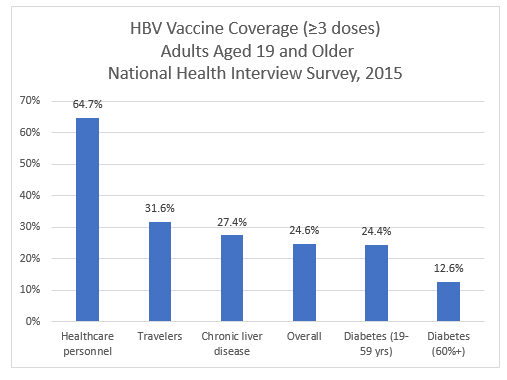
Vaccination for persons with diabetes
Because of the immunocompromised status in people with diabetes, CDC guidelines recommend HBV vaccination for all unvaccinated adults with diabetes younger than age 60. The CDC emphasizes the importance of HBV vaccination as soon as possible after a diagnosis of diabetes.35 Despite the fact that this recommendation has been heavily promoted since 2011, it is estimated that fewer than 30% of adults with diabetes have been immunized against hepatitis B.35
Reduced seroprotection
Approximately 5% to 15% of people who receive the traditional vaccines are nonresponders.5,6 The seroprotection rate (anti-HBs ≥10 mIU/mL) for traditional vaccines ranges from 70.5% to 90.2%, depending on the patient population immunized. Younger adults tend to have high seroprotection rates, between 90% and 100%. However, the proportion of adults who achieve seroprotection from the 3-dose vaccines begins to drop off notably after age 40 and is less than 75% by age 60.36,37 Other factors associated with decreased response rates in adults include male gender, obesity, history of smoking, and concomitant illnesses, including diabetes.38
Delayed seroprotection
With standard 3-dose HBV vaccines, between 45% and 70% of persons age 40 and younger do not achieve seroprotection until after they have received the third vaccine dose, at 6 months. Because of this, these individuals remain at risk for contracting HBV infection until they have completed the series.16 This delay in achieving seroprotection may be particularly important for certain individuals at risk for exposure to HBV, including healthcare workers, injection-drug users, and people traveling to an HBV-endemic area.32 For these patients, the 2-dose vaccine would be preferred.
Pregnancy
Although the available vaccines have not been specifically studied in pregnant women, CDC guidelines for vaccination of pregnant women (updated August 2016) recommend vaccination in women who are at risk for HBV, as follows:39
- "Pregnancy is not a contraindication to vaccination. Limited data suggest that developing fetuses are not at risk for adverse events when hepatitis B vaccine is administered to pregnant women. Available vaccines contain noninfectious HBsAg and should cause no risk of infection to the fetus."
- "Pregnant women who are identified as being at risk for HBV infection during pregnancy(e.g., having more than one sex partner during the previous 6 months, been evaluated or treated for an STD, recent or current injection drug use, or having had an HBsAg-positive sex partner) should be vaccinated."39
- The newer two-dose hepatitis B vaccine has not been studied in pregnant women and there are insufficient data to recommend use in pregnant women. Animal data demonstrated no fetal risk. A pregnancy registry is available for pregnant women exposed to Heplisav-B.29
Coinfection with HIV or HCV
In the U.S., about 10% of all people living with HIV also have HBV infection.9 HIV, HCV, and HBV share common pathways of transmission, including injection drug use, sexual intercourse, and mother-to-child transmission. Viral coinfection has been associated with reduced survival rates, increased risk of progression to liver disease, and increased risk of hepatotoxicity associated with antiretroviral therapy.40 Case Presentation 1 discusses HBV vaccination in a patient with HIV coinfection.
Postvaccination testing
Postvaccination testing for antibody to hepatitis B surface antigen (anti-HBs) is recommended for certain groups 1 to 2 months after the last dose of vaccine. This includes people with HIV or HCV coinfection.18 In addition, the CDC recommends postvaccination testing for healthcare providers who have a high risk of occupational exposure to blood or body fluids (e.g., those with direct patient contact, at risk of needlestick or sharps injury, and laboratory workers who draw, test or handle blood specimens).41 Healthcare workers who are low risk for contact with HBV-infected fluids need not have postvaccination testing, but should be tested if they are exposed postvaccination.41
The Pharmacist's Role in HBV Prevention
Pharmacists currently deliver approximately 28% of adult vaccinations.4Because the HBV vaccines are administered in a series, receiving vaccination from a pharmacist can enhance the convenience for patients to promote completion of the full series. Pharmacies that track their patients will be better able to help them adhere to the schedule and complete the series.
Challenges: Initiating the vaccination series
Encouraging adults to initiate the HBV vaccination series is a considerable challenge. This is due in part to healthcare access barriers in at-risk individuals as well as limited formal programs to encourage adult immunization, although these have increased in recent years.3 A 2014 analysis found that vaccination levels for HBV were low (only about 25%) among adults age 19 and older.42 A 2011 study showed that only 34.7% of adults in high-risk groups for HBV had ever received the vaccine.43 Vaccination rates are also low among people with diabetes—at least 75% of people with a diagnosis of diabetes had not been vaccinated as of 2015.35 It is important for pharmacists to discuss HBV vaccination with patients who have diabetes.
Nonadherence to conventional 3-dose vaccine series
Even after the individual has taken the first steps to receive a first dose of the HBV vaccine, adherence to subsequent doses drops off sharply, especially if the 3-dose vaccine is used. In the Vaccine Safety Datalink, a large retrospective study involving more than 88,000 adult HBV vaccine recipients, only 54% had received all 3 doses within 1 year and only 64% of those vaccinated received all 3 doses of the vaccine.44
High-risk populations do not necessarily fare better, although there is more at stake. In a study involving an STD clinic population of men who have sex with men, only 43% of patients received all 3 doses of HBV vaccine, even when it was administered on an accelerated schedule (0, 1, and 4 months rather than the recommended 6 month dosing period).45 People at high risk for HBV are often living in circumstances that make it difficult to adhere to the regimen—they may be using illicit drugs or other substances, living in poverty, or facing significant health and/or life challenges including comorbid HIV or HCV infection.40,46,47 In a CDC-funded study of 14 health departments across the country that implemented pilot vaccination programs between 2012 and 2015, nearly 48,000 doses of HBV vaccine were administered. However:48
- Among persons receiving dose 1, only 40% received dose 2
- Among those receiving doses 1 and 2, only 22% received dose 3
- STD clinics had the lowest adherence to the 3-dose schedule, at just 17%
Low adherence to the 3-series schedule has been observed even among healthcare professionals, who have higher risk associated with their jobs and also more information about the severity of the infection.49 Risks for healthcare workers for contracting HBV should not be underestimated. Healthcare workers who had needle sticks involving HBV-infected blood have a 37% to 62% of developing serologic HBV infection and a 22% to 31% risk for developing clinical hepatitis if the blood was positive for both HBsAg and hepatitis Be antigen.50
To address the problem of nonadherence to the HBV vaccine series, the CDC's Advisory Committee on Immunization Practices recommended the use of Heplisav-B for prevention of prevention of HBV in persons age 18 and over. In a February 2018, statement, the advisory committee noted, "The benefits of protection with 2 doses administered over 1 month make HepB-CpG an important option for prevention of HBV."34 Heplisav B has not been studied in patients undergoing dialysis, immunocompromised patients, or pediatric patients; therefore recommendations cannot be made in these patient populations.29
Patient counseling
Pharmacists who administer the HBV vaccine should be prepared to counsel patients about the importance of completing the series in order to confer protection against the virus. Patients should be advised that all the available HBV vaccines are derived from non-infectious, purified HBsAg and cannot cause a hepatitis B infection.29-31 Patients should be advised to report any potential adverse events to their healthcare provider and should be given appropriate Vaccine Information Statements prior to vaccination. These are available from the CDC website at www.cdc.gov/vaccines, Pharmacists should coordinate with patient and provider to report adverse events to the Vaccine Adverse Event Reporting System (VAERS; www.vaers.hhs.gov).51
Conclusion
Vaccination is highly effective in preventing people from contracting HBV. However, many high-risk candidates for the vaccine are not identified and many others do not receive the vaccine. Pharmacists are an important part of the National Viral Hepatitis Action Plan's goal to decrease the number of new HBV infections. Many pharmacists administer hepatitis B vaccines, and pharmacists also play an essential role in educating patients and other healthcare providers about the benefits of vaccination, vaccine selection, and administration procedures.4 Pharmacists must be aware of which vaccines are recommended for individual patients, whether vaccine types are interchangeable, how to encourage patients to adhere to the full vaccination series.
Case 1. Patient With HIV Coinfection
The patient, a 40-year-old male, tells you that his physician has advised him to be immunized for hepatitis B virus, based on recent lab results. He was told he could do this at community pharmacy. The patient has a history of well controlled HIV with a high CD4 count with no other comorbidities. He wants to know if he can start this vaccine series today. Which of the available vaccine formulations are appropriate for this patient? What follow-up steps would you recommend after he has completed the vaccine series?
Answer: All patients with HIV who do not have documented immunity or exposure to hepatitis B should receive vaccination. Historically, HIV-positive patients have had a reduced response to the recombinant hepatitis B vaccines. Factors associated with poor response include low CD4+ T cell counts, detectable HIV viral load, hepatitis C coinfection, and poor overall health status. Studies showed that in HIV-negative individuals, 2 doses of Heplisav-B was superior to three doses of Engerix-B in seroprotection rates. HIV treatment guidelines state that a 2-dose series of Heplisav-B can be offered to HIV-positive patients. However, it is important to counsel your patient that the safety and efficacy of Heplisav-B has not been studied in HIV-positive patients. It is recommended that patients with HIV be tested for immunity to hepatitis B (defined as concentration of anti-HBs 10mIU/mL or higher) after a period of 1 to 2 months following completion of the hepatitis B vaccine series.
Case Presentation 2. Nonadherence to Hepatitis B Vaccine Series, Interchanging Vaccine Formulas
A patient in your pharmacy tells you that she started a hepatitis B vaccine series 4 months ago at your pharmacy but she forgot to follow up after one month for the next injection. She wants to know if she can receive a second vaccination today. You check her records and see that she received an injection of Recombivax-HB 1mL (10 mcg) 123 days ago. You check your stock, but unfortunately Recombivax-HB is currently unavailable from your supplier. In stock, you currently have 2 doses of Engerix-B 1mL (20 mcg) and 4 doses of Heplisav-B 0.5mL (20 mcg). What should you tell your patient about continuing the vaccine series? Does she need to start over since 4 months have passed? What options can you provide based on the vaccines you currently have available? When should the patient return for a third dose of hepatitis B vaccine?
Answer: The full vaccination series does not need to be repeated, despite the second dose being about 3 months late. Although it would be preferable to continue with the same manufacturer, in this case a different manufacturer can be substituted. This patient has two options:
- She can continue with dose 2 of the 3-dose hepatitis B vaccine series today, substituting with Engerix-B 1.0 mL. She would then receive another dose of Engerix-B in 8 weeks. For the 3-dose recombinant vaccine schedule, the minimum time between the second and third dose should be 8 weeks and between the first and third dose should be 16 weeks.
(Note: 1mL of Recombivax HB contains 10 mcg of recombinant hepatitis B surface antigen protein, while 1.0 mL of Engerix-B contains 20ug recombinant hepatitis B surface antigen protein. However the adult dose for each vaccine is 1mL and is not based on the amount of hepatitis B surface antigen protein).
- The patient can receive one dose of Heplisav-B 0.5mL today and a repeat dose of Heplisav-B 0.5 mL in 4 weeks.
|
References
- Cohen C, Holmberg SD, McMahon BJ, et al. Is chronic hepatitis B being undertreated in the United States? J Viral Hepat. 2011;18(6):377-383.
- Committee on a National Strategy for the Elimination of Hepatitis B, Board on Population H, Public Health P, et al. In: Buckley GJ, Strom BL, eds. Eliminating the Public Health Problem of Hepatitis B and C in the United States: Phase One Report. Washington (DC): National Academies Press (US); 2016.
- U.S. Department of Health & Human Services. National Viral Hepatitis Action Plan 2017-2020. Available at: https://www.hhs.gov/hepatitis/viral-hepatitis-action-plan/index.html.
- Bach AT, Goad JA. The role of community pharmacy-based vaccination in the USA: current practice and future directions. Integr Pharm Res Pract. 2015;4:67-77.
- National Notifiable Diseases Surveillance System. CDC Hepatitis Statistics 2017. Available at: https://www.cdc.gov/hepatitis/statistics/2017surveillance/index.htm#ref05.
- World Health Organization (WHO). Hepatitis B Fact Sheet. Updated 18 July 2019. https://www.who.int/en/news-room/fact-sheets/detail/hepatitis-b.
- Matthews PC, Geretti AM, Goulder PJ, et al. Epidemiology and impact of HIV coinfection with hepatitis B and hepatitis C viruses in Sub-Saharan Africa. J Clin Virol. 2014;61(1):20-33.
- Centers for Disease Control and Prevention (CDC). Chapter 4. Travel-related infectious diseases. In: Yellow Book. Updated July 1, 2019. Available at: https://wwwnc.cdc.gov/travel/yellowbook/2020/travel-related-infectious-diseases/hepatitis-b.
- Centers for Disease Control and Prevention. Viral Hepatitis Surveillance – United States, 2015. https://www.cdc.gov/hiv/pdf/library/factsheets/hiv-viral-hepatitis.pdf.
- Ghomraoui FA, Alfaqeeh FA, Algadheeb AS, et al. Medical students' awareness of and compliance with the hepatitis B vaccine in a tertiary care academic hospital: An epidemiological study. J Infect Public Health. 2016;9(1):60-65.
- Centers for Disease Control and Prevention (CDC). Viral hepatitis and young persons who inject drugs. Available at: https://www.cdc.gov/hepatitis/featuredtopics/youngpwid.htm.
- Roberts H, Kruszon-Moran D, Ly KN, et al. Prevalence of chronic hepatitis B virus (HBV) infection in U.S. households: National Health and Nutrition Examination Survey (NHANES), 1988-2012. Hepatology. 2016;63(2):388-397.
- Sharma SK, Saini N, Chwla Y. Hepatitis B virus: inactive carriers. Virol J. 2005;2:82.
- Fattovich G. Natural history of hepatitis B. J Hepatol. 2003;39 Suppl 1:S50-58.
- World Health Organization (WHO). Guidelines for the prevention and treatment of persons with chronic hepatitis B infection. March 2015. Available at: http://apps.who.int/iris/bitstream/10665/154590/1/9789241549059_eng.pdf?ua=1&ua=1.
- Mast EE, Weinbaum CM, Fiore AE, et al. A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the United States: recommendations of the Advisory Committee on Immunization Practices (ACIP) Part II: immunization of adults. MMWR Recomm Rep. 2006;55(Rr-16):1-33; quiz CE31-34.
- Post SE, Sodhi NK, Peng CH, et al. A simulation shows that early treatment of chronic hepatitis B infection can cut deaths and be cost-effective. Health Aff (Millwood). 2011;30(2):340-348.
- Centers for Disease Control and Prevention (CDC). Recommendations for Routine Testing and Follow-up for Chronic Hepatitis B Virus (HBV) Infection. Available at: https://www.cdc.gov/hepatitis/hbv/PDFs/ChronicHepBTestingFlwUp.pdf.
- Lee MH, Yang HI, Liu J, et al. Prediction models of long-term cirrhosis and hepatocellular carcinoma risk in chronic hepatitis B patients: risk scores integrating host and virus profiles. Hepatology. 2013;58(2):546-554.
- Weinbaum CM, Williams I, Mast EE, et al. Recommendations for identification and public health management of persons with chronic hepatitis B virus infection. MMWR Recomm Rep. 2008;57(Rr-8):1-20.
- Mukhtar NA, Kathpalia P, Hilton JF, et al. Provider, Patient, and Practice Factors Shape Hepatitis B Prevention and Management by Primary Care Providers. J Clin Gastroenterol. 2017;51(7):626-631.
- Fitzgerald S, Chao J, Feferman Y, et al. Hepatitis B and Hepatocellular Carcinoma Screening Practices in Chinese and African Immigrant-Rich Neighborhoods in New York City. J Racial Ethn Health Disparities. 2016.
- Xiong M, Nguyen RH, Strayer L, et al. Knowledge and behaviors toward hepatitis B and the hepatitis B vaccine in the Laotian community in Minnesota. J Immigr Minor Health. 2013;15(4):771-778.
- Strong C, Lee S, Tanaka M, et al. Ethnic differences in prevalence and barriers of HBV screening and vaccination among Asian Americans. J Community Health. 2012;37(5):1071-1080.
- Hepatitis B Foundation. Hepatitis B Blood Tests. Updated 2019. Available at: https://www.hepb.org/prevention-and-diagnosis/diagnosis/hbv-blood-tests/.
- Abara WE, Qaseem A, Schillie S, et al. Hepatitis B Vaccination, Screening, and Linkage to Care: Best Practice Advice From the American College of Physicians and the Centers for Disease Control and Prevention. Ann Intern Med. 2017;167(11):794-804.
- Segelken HR. Baruch Blumberg, Who Discovered and Tackled Hepatitis B, Dies at 85. New York Times. April 6, 2011. Available at: https://www.nytimes.com/2011/04/07/health/07blumberg.html.
- Vaccine Education Center. Children’s Hospital of Philadelphia. Vaccine Ingredients - Aluminum. Reviewed March 22, 2018. Available at: https://www.chop.edu/centers-programs/vaccine-education-center/vaccine-ingredients/aluminum.
- Heplisav-B [Hepatitis B Vaccine (Recombinant) Adjuvanted]. Package Insert. Berkeley, CA: Dynavax. Revised 03/2018.
- Engerix-B [Hepatitis B Vaccine (Recombinant)] injectable suspension. Package insert. Research Triangle Park, NC, GlaxoSmithKline. Revised 08/2019.
- Recombivax HB Hepatitis B Vaccine (Recombinant). Package insert. Whitehouse Station, NJ: Merck; Revised 12/2018.
- P&T Product Profiler. Heplisav-B. Hepatitis B Vaccine (Recombinant) Adjuvanted. March 2018;43(3):1-33.
- Food & Drug Administration. FDA Briefing Document Heplisav-B (Hepatitis B Vaccine Recombinant and 1018 ISS Adjuvant. July 28, 2017. Available at: https://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/BloodVaccinesandOtherBiologics/VaccinesandRelatedBiologicalProductsAdvisoryCommittee/UCM568492.pdf.
- Schillie S, Harris A, Link-Gelles R, et al. Recommendations of the Advisory Committee on Immunization Practices for Use of a Hepatitis B Vaccine with a Novel Adjuvant. MMWR Morb Mortal Wkly Rep. 2018;67(15):455-458.
- Centers for Disease Control & Prevention. Diabetes and hepatitis B vaccination: information for diabetes educators. Available at: https://www.cdc.gov/diabetes/pubs/pdf/HepB_vaccination.pdf.
- Halperin SA, Dobson S, McNeil S, et al. Comparison of the safety and immunogenicity of hepatitis B virus surface antigen co-administered with an immunostimulatory phosphorothioate oligonucleotide and a licensed hepatitis B vaccine in healthy young adults. Vaccine. 2006;24(1):20-26.
- Jackson S, Lentino J, Kopp J, et al. Immunogenicity of a two-dose investigational hepatitis B vaccine, HBsAg-1018, using a toll-like receptor 9 agonist adjuvant compared with a licensed hepatitis B vaccine in adults. Vaccine. 2018;36(5):668-674.
- Yang S, Tian G, Cui Y, et al. Factors influencing immunologic response to hepatitis B vaccine in adults. Sci Rep. 2016;6:27251.
- Centers for Disease Control and Prevention (CDC). Pregnancy and vaccination. Guidelines for vaccinating pregnant women. Updated August 2016. Available at: https://www.cdc.gov/vaccines/pregnancy/hcp-toolkit/guidelines.html.
- Huy BV, Vernavong K, Kinh NV. HBV and HCV Coinfection among HIV/AIDS Patients in the National Hospital of Tropical Diseases, Vietnam. AIDS Res Treat. 2014;2014:581021.
- Centers for Disease Control and Prevention. CDC Guidance for Evaluating Health-Care Personnel for Hepatitis B Virus Protection and for Administering Postexposure Management. Morbid Mortal Wkly Rep. 2013;62(10):1-19. Available at: www.cdc.gov/mmwr/pdf/rr/rr6210.pdf.
- LeFevre ML, Force USPST. Screening for hepatitis B virus infection in nonpregnant adolescents and adults: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;161(1):58-66.
- Annunziata K, Rak A, Del Buono H, et al. Vaccination rates among the general adult population and high-risk groups in the United States. PLoS One. 2012;7(11):e50553.
- Nelson JC, Bittner RC, Bounds L, et al. Compliance with multiple-dose vaccine schedules among older children, adolescents, and adults: results from a vaccine safety datalink study. Am J Public Health. 2009;99 Suppl 2:S389-397.
- Gunn RA, Lee MA, Murray PJ, et al. Hepatitis B vaccination of men who have sex with men attending an urban STD clinic: impact of an ongoing vaccination program, 1998-2003. Sex Transm Dis. 2007;34(9):663-668.
- da Silva LN, da Silva Franca DD, Del-Rio NHA, et al. Low prevalence, low immunization and low adherence to full hepatitis B vaccine scheme and high-risk behaviors among crack cocaine users in central Brazil. J Infect Public Health. 2017;10(1):76-83.
- Mavilia MG, Wu GY. HBV-HCV Coinfection: Viral Interactions, Management, and Viral Reactivation. J Clin Transl Hepatol. 2018;6(3):296-305.
- Bridges CB, Watson TL, Nelson NP, et al. Challenges with hepatitis B vaccination of high risk adults - A pilot program. Vaccine. 2019;37(35):5111-5120.
- Williams WW, Lu PJ, O’Halloran A, et al. Surveillance of Vaccination Coverage Among Adult Populations – United States, 2015. Morbid Mortal Wkly Rep. 2017;66(11)1-28. Available at: https://www.cdc.gov/mmwr/volumes/66/ss/ss6611a1.htm.
- Updated U.S. Public Health Service Guidelines for the Management of Occupational Exposures to HBV, HCV, and HIV and Recommendations for Postexposure Prophylaxis. MMWR Recomm Rep. 2001;50 (RR11);1-42.
- VAERS. Vaccine Adverse Reporting System. Available at: www.vaers.hss.gov.
Back Top