
Expired activity
Please go to the PowerPak
homepage and select a course.
Understanding the Treatment Paradigm for Age-Related Macular Degeneration
Introduction
Neovascular age-related macular degeneration (nAMD) is a leading cause of vision loss among older people in the United States.1 Its treatment has been revolutionized by anti–vascular endothelial growth factor (VEGF) therapy, but achieving optimal outcomes for individual patients depends on timely initiation of effective therapy and careful follow-up with ongoing treatment to control disease activity. Individualization of treatment plans is a key theme for achieving good outcomes. In real-world settings, however, there are challenges to meeting these needs.
Collaboration between payers and providers is critical for enabling selection of the most appropriate treatment for patients with nAMD and improving overall visual outcomes (see Commentary: Collaboration Through Discussion and Education). It is important that retina specialists understand the issues payers face in their efforts to balance cost, quality, and access on a population-wide basis. At the same time, there is a need for payers to understand the issues confronting retina specialists as they try to preserve vision and quality of life of patients with nAMD. Payers must also understand the current landscape of nAMD treatment and the evidence on which it is based so that best clinical practices are incorporated into payer models for covering care.
Background: Prevalence, Treatment, and Health Care Spending
Dr Wong: According to a report in 2010, Medicare spent one-sixth of its part B medication budget on anti-VEGF treatment for nAMD.2 What is the burden of nAMD in terms of its prevalence or number of affected people?
Dr Heier: Age-related macular degeneration (AMD) is a chronic and potentially progressive disease, of which nAMD is a late, advanced form. Although approximately only 20% of people with AMD develop neovascular disease, 90% of the severe vision loss attributed to AMD is due to nAMD.1
A report published in 2004 estimated that AMD affected 14 million people in the United States, of which 1.75 million had an advanced, sight-threatening form of AMD in at least 1 eye, and more than 7 million had features of AMD that put them at increased risk of developing advanced disease in 1 or both eyes.3 On the basis of the expected growth of the aging population, the study projected that in 2020, nearly 3 million people in the United States would have advanced AMD.
AMD typically does not develop until after age 50, but its prevalence and the prevalence of nAMD increase with age.4 A recent analysis pooling data from several population-based studies determined that nAMD prevalence increased steadily from 0.14% in people aged < 55 years to 8.5% in people aged ≥ 85 years.4
Dr Clark: Researchers using data from the phase 3 trials of ranibizumab for nAMD estimated that using the anti-VEGF agent could reduce the number of cases of legal blindness by approximately 75% and the number of cases of visual impairment by approximately 35%.5
Before anti-VEGF therapy, the only treatment available for nAMD was photodynamic therapy, but it only slowed the rate of vision loss. Results from clinical trials investigating anti-VEGF therapy showed that for the first time, we could stabilize vision for most patients and even improve vision for a significant minority of patients when they were treated with ranibizumab on a monthly basis or with aflibercept monthly or every other month.6-8
Clinical Trials vs Real-World Outcomes
Dr Wong: What do the US Food and Drug Administration (FDA) registration trials show about the efficacy of anti-VEGF treatment for nAMD?
Dr Heier: The primary end point in the registration trials looked at the proportion of patients with stable vision, defined as losing < 15 letters on an ETDRS (Early Treatment Diabetic Retinopathy Study) eye chart from their baseline visual acuity (VA).6-11 Key secondary efficacy end points looked at the proportion of patients with a clinically relevant improvement in vision, defined as gaining ≥ 15 letters from baseline VA, change from baseline VA, change in retinal thickness, and absence of fluid. Results from the registration trials for aflibercept and ranibizumab and from CATT (Comparison of Age-Related Macular Degeneration Treatments Trials), which investigated ranibizumab and bevacizumab, showed that after 1 year, > 90% of patients maintained stable vision, defined as a loss of < 15 ETDRS letters. It is important to realize, however, that these outcomes were achieved in highly selected populations of patients who were managed for a finite duration, followed closely at monthly visits, and received regular treatment. We know from other studies and from clinical experience that in the real world, many patients do not maintain the initial benefit of anti-VEGF therapy (Figure 1).12-16 For example, in the SEVEN-UP (Seven-Year Observational Update of Macular Degeneration Patients Post-MARINA/ANCHOR and HORIZON Trials) study that included participants from the ranibizumab registration trials, 37% of eyes were legally blind at 7 years.12
| Figure 1. Mean change in ETDRS letter score12 |
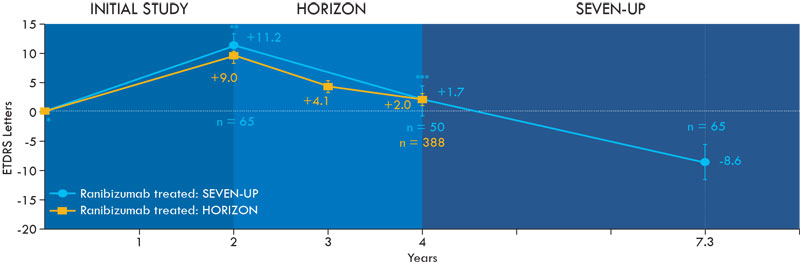 |
Abbreviations: ETDRS, Early Treatment Diabetic Retinopathy Study; SEVEN-UP, Seven-Year Observational Update of Macular Degeneration Patients Post-MARINA/ANCHOR and HORIZON Trials.
Note: ± indicates standard error of the mean.
* P < .005 vs SEVEN-UP Year 7.3
** P < .0001 vs SEVEN-UP Year 7.3
** P < .001 vs SEVEN-UP Year 7.3
Permissions request submitted. |
Dr Owens: What accounts for the discrepancy?
Dr Clark: There are several contributing factors. First, as is typical of FDA registration trials, enrolled patients are not fully representative of those seen in the real-world setting. Registration trials enroll a highly selective patient population because these trials use strict inclusion/exclusion criteria. The cohort of patients encountered in clinical practice is more heterogeneous and might include patients with more complex disease features. Consequently, the response to treatment might be different for patients seen in the real world compared with that in clinical trial participants.
Dr Heier: Not only were patients in the registration trials and in CATT more ideal with respect to their clinical characteristics, they also received more ideal follow-up and treatment. Patients in the clinical trials had close monthly follow-up and regular treatment with injections given monthly or every other month, depending on the medication. Monthly treatment is generally highly effective for keeping the macula dry and preserving vision, but it can be impractical and a burden for many patients with nAMD, considering their advanced age, likelihood of having comorbidities, dependence on a caregiver for transportation, and the need for some to travel long distances to see a retina specialist.
The data are pretty clear that patients need to receive approximately 6 injections per year to achieve the vision gains seen in the registration trials after 1 year and maintain the benefit in the second year.17,18 Compared with the clinical trial participants, real-world patients are not receiving this level of treatment.15 In SEVEN-UP, patients followed for up to 7 years were getting just 2 to 3 injections annually.12 A study of real-world ranibizumab therapy in treatment-naïve eyes found the median number of injections received in the first, second, and third years was 5, 4, and 4, respectively.15
Obstacles to Optimizing Outcomes
Dr Wong: Although a monthly injection scheme provides the most opportunity for a patient to retain maximum vision, it is easy to appreciate how patients might not be able to maintain ongoing treatment because of logistic issues that limit their ability to return for monthly visits. We also need to ask if economics is a factor. Do you think high copays play a role?
Dr Heier: For some patients, carrying a commercial plan that has a high deductible or lacking a supplemental Medicare coverage plan might limit treatment frequency and choice of the anti-VEGF agent. Although the copay for bevacizumab might just be $15, it could be $400 for aflibercept or ranibizumab. Manufacturer patient-assistance programs and grant money that is available through independent foundations can help reduce the cost burden. But because bevacizumab costs less than ranibizumab and aflibercept, in my experience, some commercial insurers have step-therapy policies that mandate treatment for nAMD be initiated with the off-label use of bevacizumab. According to these policies, coverage for treatment with an FDA-approved drug—ranibizumab or aflibercept—is not allowed without documentation that the patient has a contraindication to bevacizumab or had a trial with bevacizumab and either failed to respond or showed intolerance. Beginning in January 2019, Medicare Advantage plans will also be allowed to implement step therapy for physician-administered and other part B drugs.19
Dr Wong: It is interesting to see step-therapy mandates requiring treatment initiation with bevacizumab, essentially a drug with an off-label use and one requiring compounding for an ophthalmic preparation. When claims for bevacizumab treatment of nAMD began being submitted, many of my colleagues were questioning its use because of these 2 aspects. However, at that time, neither ranibizumab nor aflibercept was approved or available. With the approval of ranibizumab, many health plan managers considered a definitive step therapy using bevacizumab first. Some decided not to adopt step therapy beginning with bevacizumab because bevacizumab was off-label and required compounding, the latter of which might be performed in a nonsterile environment and, therefore, raised concerns of contamination risk. Although off-label use is a noncovered service on most benefit plans, managers still elected to continue coverage for bevacizumab to assure that patients received appropriate care at the lowest cost. Evidence from the literature on the efficacy and safety of bevacizumab is what helped to clear the barrier relating to off-label use.10,11
What concerns do retina specialists have with step therapy for nAMD? Are there data to show that the 3 anti-VEGF drugs differ in efficacy, or are there clinical situations in which there is a preference for using a particular anti-VEGF agent?
Dr Clark: Step therapy beginning with bevacizumab would be reasonable if bevacizumab had an FDA-approved indication for the treatment of nAMD,20 and if it showed similar efficacy and safety compared with ranibizumab or aflibercept in multiple randomized clinical trials with confirmatory results. Because these criteria are not met, establishing bevacizumab as primary therapy for all patients with nAMD is problematic. Although CATT gave us useful information for guiding treatment decisions, it was neither a registration trial nor a confirmatory pivotal trial.10,11 In addition, CATT was not powered to evaluate the safety of bevacizumab as treatment for nAMD—a critical measure in the process of FDA approval for a medication. Also, because bevacizumab is not available to retina specialists in single-dose vials, as are ranibizumab and aflibercept, there remains uncertainty regarding the sterility and bioavailability of bevacizumab when delivered in syringes prepared by compounding pharmacies. Finally, recent reports of intravitreal silicone oil droplets after bevacizumab injections create uncertainty for clinicians and their patients.21,22
Although it is true that the 2-year VA outcomes in CATT were similar for bevacizumab and ranibizumab when comparing the groups treated with the same dosing regimen—bevacizumab monthly vs ranibizumab monthly or bevacizumab as needed vs ranibizumab as needed—patients receiving bevacizumab as needed had the least gain in VA; the bevacizumab as-needed group also had the greatest lesion growth and the greatest likelihood of having macular fluid (Table).11 This is an important point because dosing less than once a month probably reflects how patients are treated in the real world.12,15 CATT is the only trial that provides data on as-needed treatment with bevacizumab, and its results indicate that this approach compromises outcomes.
| Table. Outcomes in CATT for Patients Maintained on the Same Dosing Regimen for 2 Years11 |
|
Treatment
|
VA Gain, Letters |
Fluid on OCT, % |
Mean Change in Lesion Area From Baseline, mm2 |
| Monthly |
|
|
|
| Ranibizumab |
8.8 |
51.5 |
-0.4 |
| Bevacizumab |
7.8 |
67.4 |
1.6 |
| As needed |
|
|
|
| Ranibizumab |
6.7 |
75.0 |
1.9 |
| Bevacizumab |
5.4 |
84.5 |
3.0 |
| P value |
|
|
|
| Drug |
.21 |
.0003 |
.006 |
| Regimen |
.046 |
< .0001 |
.0003 |
| Abbreviations: CATT, Comparison of Age-Related Macular Degeneration Treatments Trials; OCT, optical coherence tomography; VA, visual acuity. |
Dr Heier: Step therapy for nAMD is concerning because it can interfere with the ability to optimize outcomes for individuals according to their unique clinical characteristics and other circumstances. Because bevacizumab needs to be compounded, there are inherent safety concerns with its use.
I use all 3 anti-VEGF medications to treat nAMD, and I start most patients on bevacizumab. I think bevacizumab can be very appropriate as first-line therapy because it is a very good drug that in many patients is as efficacious as the FDA-approved medications. In my experience, however, it is not more efficacious for every patient than the on-label alternatives.
There are situations in which I would prefer to use aflibercept, either because it can reduce treatment burden or because it has potential benefit in certain hard-to-treat patients. For example, there are cases in which time is of the essence in getting a treatment response. Data from the aflibercept registration trials—VIEW 1 and VIEW 2—provide evidence that it has a more potent and more persistent macular drying effect than does ranibizumab.8 An integrated analysis of data from the VIEW trials showed that the percentage of patients achieving dry status was higher in the groups receiving aflibercept 2 mg every 4 weeks or 2 mg every 8 weeks than in the group receiving ranibizumab 0.5 mg every 4 weeks (72.4% and 67.7% vs 62%, respectively). In addition, a post hoc analysis considering patients with early persistent retinal fluid found that the mean best-corrected VA gain from baseline to week 52 was greater in eyes treated with aflibercept 2 mg every 4 weeks than in those treated with ranibizumab 0.5 mg every 4 weeks or aflibercept 2 mg every 8 weeks.23 Patients receiving aflibercept 2 mg every 4 weeks also had the lowest percentage of eyes losing 5 or more letters compared with those receiving ranibizumab or aflibercept 2 mg every 8 weeks (6.5% vs 16.6% and 16.2%, respectively). A step-therapy approach can delay timely use of a more appropriate treatment for a given patient.
Dr Owens: Is there a way to identify the “given” patients for whom aflibercept might be needed so that the step-therapy process could be made more efficient?
Dr Heier: It would be difficult to propose specific criteria for identifying such patients. Rather, these situations reflect the art of practicing medicine and applying clinical judgment.
Dr Wong: Do you see other issues requiring step therapy?
Dr Heier: Step therapy also interferes with patient choice. I inform patients about the efficacy, safety, and cost of the available medications. Some patients prefer to start treatment with bevacizumab because it is the less-expensive drug. Others feel more comfortable being treated with an FDA-approved drug, despite the fact that it might be more expensive, but they might not be allowed to receive the treatment they desire because of their insurance policy.
Dr Wong: I agree that in the area of specialty drugs, physician and patient choice should play a large role. Unfortunately, we live in a world in which economics comes into play. Even if a patient wants the higher-cost drug and authorization is not an issue, he or she might have a fairly significant out-of-pocket cost that might limit access.
Dr Owens: Are you finding that payers are putting a limit on the number of injections patients can receive each year?
Dr Clark: Not currently, which is good for many patients. In the past, there were some problems with insurers refusing to pay for aflibercept administered more often than once every 8 weeks after the initial 3 loading doses, but the issue seems to have been resolved when the original labeling was revised. The labeling now states, “Some patients may need every-4-week (monthly) dosing after the first 12 weeks.”24
Dr Wong: This has been a very informative discussion, and I hope my colleagues are gaining an appreciation of some of the nuances of treating patients with nAMD. Are there other issues that you are encountering that might be impeding your ability to optimize patient outcomes?
Dr Heier: Some insurers have denied payments for anti-VEGF injections given more frequently than every 28 days. Considering practical issues that affect appointment scheduling, it is important to be able to treat patients before 28 days. Trials had a window around the allowable reinjection time, so treating a little sooner than every 28 days can be considered safe. In MARINA (Minimally Classic/Occult Trial of the Anti-VEGF Antibody Ranibizumab in the Treatment of Neovascular Age-Related Macular Degeneration), for example, retreatment was allowed within 23 days.6
Dr Clark: As another issue, the requirement for prior authorization can delay essential treatment for some patients. Data from clinical trials showing that vision outcomes with anti-VEGF therapy are best when patients are treated when vision is still good and/or the lesion is small support the importance of early treatment.25-27 Furthermore, we know that some patients’ conditions can deteriorate quickly in a very short time. Ideally, therefore, we should be able to initiate treatment on the same day we make the diagnosis of nAMD rather than having to ask a patient to return when we have received authorization for treatment. Getting to the clinic can be a difficult burden for many patients. Same-day treatment can further patient satisfaction because a second trip is avoided and treatment needs are immediately addressed.
Update on the Treat-and-Extend Dosing Scheme to Reduce Treatment Burden and Improve Vision
Dr Wong: Considering all the burdens and the cost of maintaining monthly treatment, is there a treatment strategy that can optimize patient outcomes while balancing costs and convenience?
Dr Heier: Recognition that monthly injections presented a burden and might also be overtreatment for some patients prompted interest in alternative treatment strategies. Initial studies evaluated as-needed approaches, in which patients were treated monthly to achieve disease control—only if they had evidence of recurrent disease activity—and then evaluated at return visits.28-32 Results from studies investigating as-needed treatment clearly showed that it did not provide the same benefit as fixed monthly injections unless patients continued to be followed rigorously with monthly visits.
With an as-needed approach, patients develop disease reactivation time and again, and the exposure to multiple recurrences likely increases the risk for permanent loss of vision.32 Treat-and-extend (TAE) is a strategy for administering anti-VEGF injections that aims to maximize outcomes for patients by maintaining disease control while minimizing the costs and inconvenience of frequent, regular follow-up.
Treat-and-extend is customized to the patient, and, in contrast to an as-needed approach, is designed to limit patient exposure to recurrent disease activity. In TAE, treatment is initiated on a fixed monthly schedule that continues until macular fluid resolves or is stabilized at an improved level. Then, the treatment interval is extended in a stepwise manner as long as there is no active disease. The interval between treatments is usually increased by 2-week increments up to a maximum of 8 to 12 weeks. Patients are evaluated at each visit by clinical examination and imaging with optical coherence tomography (OCT) that can identify macular fluid as a subclinical sign of recurrent activity, before there is a significant decrease in vision that might be irreversible.
For example, once disease activity is controlled with monthly injections, a patient will return after 6 weeks for assessment and treatment. If the nAMD is quiet, the patient will be asked to return again after 8 weeks. If the retina is still dry, the treatment interval can be extended to 10 weeks. If at any follow-up visit there is fluid present on OCT, the interval between visits would be shortened, and the patient would be kept on the more frequent schedule for follow-up and treatment indefinitely or at least for a period of time before trying to extend treatment again.
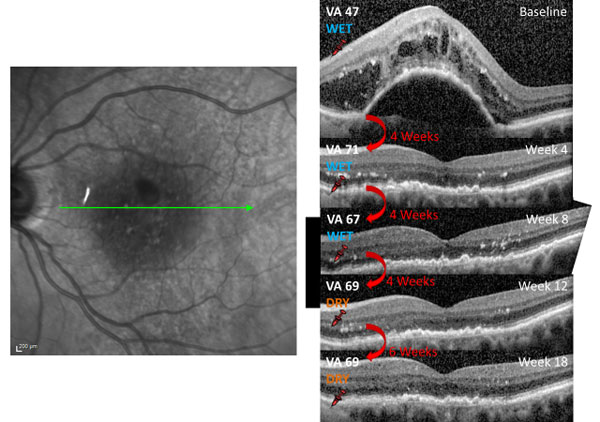
Dr Clark: I was an investigator in the TREX-AMD (Treat and Extend Protocol in Patients With Wet Age-Related Macular Degeneration) study, which was a randomized trial of TAE with ranibizumab vs a monthly dosing regimen for patients with nAMD.33 The OCT images and VA data collected at follow-up visits from 1 of the participating patients who was treated by Dr Charles Wykoff provide an excellent illustration of how TAE works (Figure 2).
| Figure 2. Optical coherence tomography scans and visual acuity changes of a patient receiving a treat-and-extend regimen of ranibizumab |
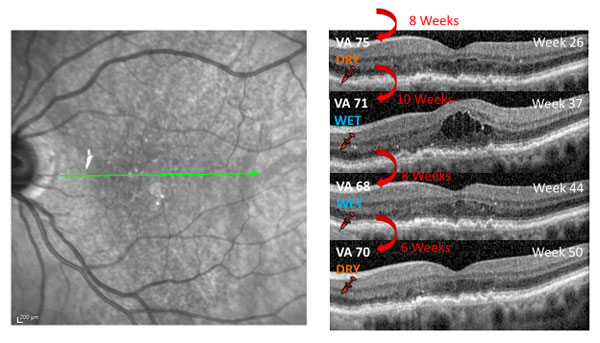 |
Abbreviation: VA, visual acuity.
Images courtesy of Charles C. Wykoff, MD, PhD |
The initial anti-VEGF injection resulted in dramatic, almost complete resolution of fluid that was accompanied by a 24-letter gain in VA. For this patient, the level of functional improvement brought the vision to a level that was good enough to drive a car. At 12 weeks after starting monthly treatment and having achieved durable disease control, the injection interval was extended to 6 weeks and then extended successfully 2 more times. However, when the patient returned at 10 weeks postinjection, there was recurrence of intraretinal fluid, with a 4-letter decrease in VA. The patient was treated and instructed to return after just 8 weeks. Because there was still fluid on the OCT, and VA had further decreased, the interval between treatments was shortened to 6 weeks. At the next visit, the macula was dry, and the patient’s VA had improved by 2 letters.
Dr Heier: You can see from the images in this case that the success of TAE requires the use of OCT at each follow-up visit and intensive review of the images by the retina specialist to identify evidence of subclinical recurrence that cannot be appreciated by clinical examination or VA testing. Although there is cost associated with the required imaging and assessment, because TAE can reduce the frequency of anti-VEGF injections, it can be cost saving. For example, the ability to manage a patient with injections every 6 weeks instead of every 4 weeks reduces the number of injections given per year by 3, which translates to an annual savings of > $6000 for a health plan when a patient is being treated with 1 of the on-label medications. The savings might exceed the costs for reimbursing the diagnostic testing and its interpretation.
Dr Wong: Is TAE considered standard of care for managing nAMD?
Dr Heier: It has not been endorsed by any practice guidelines. According to recent survey results, however, most retina specialists in the United States are using TAE to manage patients with nAMD.34
|
Commentary: Collaboration Through Discussion and Education
W. Lloyd Clark, MD
Anti–vascular endothelial growth factor therapy has been a revolutionary advancement in the treatment of neovascular age-related macular degeneration. With ranibizumab, aflibercept, and off-label bevacizumab, retina specialists have 3 options for achieving the goal of eliminating exudation to maximize vision gains with a durable result. Initial clinical trials showed these outcomes could be achieved with fixed monthly dosing. More recent research supports the use of treat-and-extend therapy, showing that with careful monitoring, this approach can produce similar outcomes to those seen with monthly injections, with reduced treatment burden and costs for patients and payers.1,2 Ongoing information exchange between retina specialists and payers enables collaboration and success in reaching our common goal of optimizing treatment delivery for neovascular age-related macular degeneration and maximizing the number of patients who can avoid devastating vision loss from this disease.
References
- Haga A, Kawaji T, Ideta R, Inomata Y, Tanihara H. Treat-and-extend versus every-other-month regimens with aflibercept in age-related macular degeneration. Acta Ophthalmol. 2018;96(3):e393-e398.
- Lanzetta P, Loewenstein A; Vision Academy Steering Committee. Fundamental principles of an anti-VEGF treatment regimen: optimal application of intravitreal anti-vascular endothelial growth factor therapy of macular diseases. Graefes Arch Clin Exp Ophthalmol. 2017;255(7):1259-1273.
|
Dr Clark: Although TAE is widely used, there is limited published level 1 evidence that supports it. Several published studies, anecdotal reports, and a wealth of personal knowledge indicate that outcomes for patients managed by TAE with careful follow-up can be similar to those achieved with fixed monthly injections. Authors of a systematic review and meta-analysis that included 4 studies using ranibizumab concluded that the evidence suggested TAE is comparable to monthly dosing and superior to as-needed dosing for both efficacy and safety.35 There are also promising data for aflibercept.17,36 There are little data on TAE using bevacizumab.37,38 In LUCAS (Lucentis Compared to Avastin Study), in which patients were randomized to a TAE protocol with ranibizumab or bevacizumab, functional and anatomic outcomes after 1 year were similar in the 2 groups, but the mean number of injections was significantly greater with bevacizumab than with ranibizumab.37
Dr Heier: In my personal experience, there is a durability advantage for using aflibercept for TAE. For this reason, I might be able to maintain patients using a longer interval between treatments than I would with bevacizumab. Treat-and-extend with bevacizumab every 5 weeks or with aflibercept every 6 to 8 weeks might provide the same outcome, assuming that both regimens keep the retina dry. The reduced treatment burden that comes with the longer interval between treatments can be important to some patients and can result in better treatment adherence.
Dr Owens: Treat-and-extend seems to be a good economic proposition. I think it is important that payers become aware that there is good objective evidence showing that by doing the OCT-guided TAE approach, patients can receive fewer injections without jeopardizing their outcomes.
Take-Home Points
AMD is a leading cause of severe vision loss among adults.
- Neovascular AMD accounts for 90% of AMD-related severe vision loss
Visual acuity can be maintained for up to 2 years in > 90% of patients with nAMD who are treated with regular monthly injections of aflibercept, bevacizumab, or ranibizumab.
- Early treatment improves outcomes
- Outcomes in patients treated with anti-VEGF agents in the real world do not match those achieved by clinical trial participants receiving fixed monthly injections
Off-label use of compounded bevacizumab can be effective treatment for many patients.
Evidence from comparative clinical trials suggests that compared with ranibizumab, aflibercept might have a stronger and more persistent drying effect.
As-needed treatment with injections given for recurrent nAMD activity is not as effective as fixed monthly treatment for maintaining early VA gains unless patients receive monthly follow-up.
Treat-and-extend anti-VEGF regimens for nAMD can provide outcomes comparable to those seen with fixed monthly injections, but with fewer visits and fewer anti-VEGF injections.
Open dialogue between payers and providers can keep payers apprised of the latest standards of care and help provide optimal and cost-effective health care services to patients with nAMD.
|
Commentary: Collaboration Through Discussion and Education
Winston Wong, PharmD
This discussion is an excellent example of how payers and providers can collaborate to deliver optimal health care services. The role of payers is to manage the common health needs of the insured population. Hence, it is imperative that they stay relatively up-to-date on the current standards of care for the most common diseases and medical conditions. It is impossible, however, for payers to be knowledgeable of the latest standards and best practices for every disease, especially specialty diseases such as neovascular age-related macular degeneration. Open dialogues and educational programs that involve both payers and providers go a long way to keep payers well informed and might help payers facilitate the delivery of optimal and cost-effective health care services.
|
References
- Retina/Vitreous Preferred Practice Pattern® Panel. Preferred Practice Pattern®. Age-Related Macular Degeneration. San Francisco, CA: American Academy of Ophthalmology; 2015.
- Office of Inspector General. Medicare Payments for Drugs Used to Treat Wet Age-Related Macular Degeneration. Washington, DC: Department of Health and Human Services; 2012.
- Friedman DS, O’Colmain BJ, Muñoz B, et al; Eye Diseases Prevalence Research Group. Prevalence of age-related macular degeneration in the United States. Arch Ophthalmol. 2004;122(4):564-572.
- Lambert NG, ElShelmani H, Singh MK, et al. Risk factors and biomarkers of age-related macular degeneration. Prog Retin Eye Res. 2016;54:64-102.
- Bressler NM, Doan QV, Varma R, et al. Estimated cases of legal blindness and visual impairment avoided using ranibizumab for choroidal neovascularization: non-Hispanic white population in the United States with age-related macular degeneration. Arch Ophthalmol. 2011;129(6):709-717.
- Rosenfeld PJ, Brown DM, Heier JS, et al; MARINA Study Group. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1419-1431.
- Brown DM, Michels M, Kaiser PK, Heier JS, Sy JP, Ianchulev T; ANCHOR Study Group. Ranibizumab versus verteporfin photodynamic therapy for neovascular age-related macular degeneration: two-year results of the ANCHOR study. Ophthalmology. 2009;116(1):57-65.e5.
- Heier JS, Brown DM, Chong V, et al; VIEW 1 and VIEW 2 Study Groups. Intravitreal aflibercept (VEGF Trap-eye) in wet age-related macular degeneration. Ophthalmology. 2012;119(12):2537-2548.
- Brown DM, Kaiser PK, Michels M, et al; ANCHOR Study Group. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1432-1444.
- Martin DF, Maguire MG, Ying GS, Grunwald JE, Fine SL, Jaffe GL; CATT Research Group. Ranibizumab and bevacizumab for neovascular age-related macular degeneration. N Engl J Med. 2011;364(20):1897-1908.
- Martin DF, Maguire MG, Fine SL, et al; Comparison of Age- Related Macular Degeneration Treatments Trials (CATT) Research Group. Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: two-year results. Ophthalmology. 2012;119(7):1388-1398.
- Rofagha S, Bhisitkul RB, Boyer DS, Sadda SR, Zhang K; SEVEN-UP Study Group. Seven-year outcomes in ranibizumab-treated patients in ANCHOR, MARINA, and HORIZON: a multicenter cohort study (SEVEN-UP). Ophthalmology. 2013;120(11):2292-2299.
- Singer MA, Awh CC, Sadda S, et al. HORIZON: an open-label extension trial of ranibizumab for choroidal neovascularization secondary to age-related macular degeneration. Ophthalmology. 2012;119(6):1175-1183.
- Maguire MG, Martin DF, Ying GS, et al; Comparison of Age-Related Macular Degeneration Treatments Trials (CATT) Research Group. Five-year outcomes with anti-vascular endothelial growth factor treatment of neovascular age-related macular degeneration: the Comparison of Age-Related Macular Degeneration Treatments Trials. Ophthalmology. 2016;123(8):1751-1761.
- Writing Committee for the UK Age-Related Macular Degeneration EMR Users Group. The neovascular age-related macular degeneration database: multicenter study of 92 976 ranibizumab injections: report 1: visual acuity. Ophthalmology. 2014;121(5):1092-1101.
- Chong V. Ranibizumab for the treatment of wet AMD: a summary of real-world studies. Eye (Lond). 2016;30(2):270-286.
- DeCroos FC, Reed D, Adam MK, et al. Treat-and-extend therapy using aflibercept for neovascular age-related macular degeneration: a prospective clinical trial. Am J Ophthalmol. 2017;180:142-150.
- Rayess N, Houston SK 3rd, Gupta OP, Ho AC, Regillo CD. Treatment outcomes after 3 years in neovascular age-related macular degeneration using a treat-and-extend regimen. Am J Ophthalmol. 2015;159(1):3-8.e1.
- Centers for Medicare & Medicaid Services. Medicare advantage prior authorization and step therapy for part B drugs. https://www.cms.gov/newsroom/fact-sheets/medicare-advantage-prior-authorization-and-step-therapy-part-b-drugs. Published August 7, 2018. Accessed October 19, 2018.
- Avastin [package insert]. South San Francisco, CA: Genentech, Inc; 2018.
- Khurana RN, Chang LK, Porco TC. Incidence of presumed silicone oil droplets in the vitreous cavity after intravitreal bevacizumab injection with insulin syringes. JAMA Ophthalmol. 2017;135(7):800-803.
- Avery RL, Castellarin AA, Dhoot DS, et al. Large silicone droplets after intravitreal bevacizumab (Avastin). Retin Cases Brief Rep. 2019;13(2):130-134.
- Jaffe GJ, Kaiser PK, Thompson D, et al. Differential response to anti-VEGF regimens in age-related macular degeneration patients with early persistent retinal fluid. Ophthalmology. 2016;123(9):1856-1864.
- Eylea [package insert]. Tarrytown, NY: Regeneron Pharmaceuticals, Inc; 2018.
- Boyer DS, Antoszyk AN, Awh CC, Bhisitkul RB, Shapiro H, Acharya NR; MARINA Study Group. Subgroup analysis of the MARINA study of ranibizumab in neovascular age-related macular degeneration. Ophthalmology. 2007;114(2):246-252.
- Kaiser PK, Brown DM, Zhang K, et al. Ranibizumab for predominantly classic neovascular age-related macular degeneration: subgroup analysis of first-year ANCHOR results. Am J Ophthalmol. 2007;144(6):850-857.
- Regillo CD, Busbee BG, Ho AC, Ding B, Haskova Z. Baseline predictors of 12-month treatment response to ranibizumab in patients with wet age-related macular degeneration. Am J Ophthalmol. 2015;160(5):1014-1023.e2.
- Fung AE, Lalwani GA, Rosenfeld PJ, et al. An optical coherence tomography-guided, variable dosing regimen with intravitreal ranibizumab (Lucentis) for neovascular age-related macular degeneration. Am J Ophthalmol. 2007;143(4):566-583.
- Lalwani GA, Rosenfeld PJ, Fung AE, et al. A variable-dosing regimen with intravitreal ranibizumab for neovascular age-related macular degeneration: year 2 of the PrONTO Study. Am J Ophthalmol. 2009;148(1):43-58.e1.
- Busbee BG, Ho AC, Brown DM, et al; HARBOR Study Group. Twelve-month efficacy and safety of 0.5 mg or 2.0 mg ranibizumab in patients with subfoveal neovascular age-related macular degeneration. Ophthalmology. 2013;120(5):1046-1056.
- Boyer DS, Heier JS, Brown DM, Francom SF, Ianchulev T, Rubio RG. A phase IIIb study to evaluate the safety of ranibizumab in subjects with neovascular age-related macular degeneration. Ophthalmology. 2009;116(9):1731-1739.
- Lanzetta P, Loewenstein A; Vision Academy Steering Committee. Fundamental principles of an anti-VEGF treatment regimen: optimal application of intravitreal anti-vascular endothelial growth factor therapy of macular diseases. Graefes Arch Clin Exp Ophthalmol. 2017;255(7):1259-1273.
- Wykoff CC, Ou WC, Croft DE, et al; TREX-AMD Study Group. Neovascular age-related macular degeneration management in the third year: final results from the TREX-AMD randomised trial. Br J Ophthalmol. 2018;102(4):460-464.
- Rezaei KA, Stone TW, eds. 2014 Global Trends in Retina Survey. Chicago, IL: American Society of Retina Specialists; 2014.
- Okada M, Kandasamy R, Chong EW, McGuiness M, Guymer RH. The treat-and-extend injection regimen versus alternate dosing strategies in age-related macular degeneration: a systematic review and meta-analysis. Am J Ophthalmol. 2018;192:184-197.
- Haga A, Kawaji T, Ideta R, Inomata Y, Tanihara H. Treat-and-extend versus every-other-month regimens with aflibercept in age-related macular degeneration. Acta Ophthalmol. 2018;96(3):e393-e398.
- Berg K, Hadzalic E, Gjertsen I, et al. Ranibizumab or bevacizumab for neovascular age-related macular degeneration according to the Lucentis Compared to Avastin Study treat-and-extend protocol: two-year results. Ophthalmology. 2016;123(1):51-59.
- Mrejen S, Jung JJ, Chen C, et al. Long-term visual outcomes for a treat and extend anti-vascular endothelial growth factor regimen in eyes with neovascular age-related macular degeneration. J Clin Med. 2015;4(7):1380-1402.
Back Top