
Expired activity
Please go to the PowerPak
homepage and select a course.
Metastatic Gastric and Esophagogastric Junction Adenocarcinoma: A Primer for Oncology, Managed Care, and Specialty Pharmacists
EPIDEMIOLOGY AND PREVALENCE OF GASTRIC CANCER
Gastric cancer is the fourth most common cause of cancer-related death in the world. Most patients present with advanced disease, making long-term survival and cure difficult to achieve. The rates of gastric cancer are highest in eastern Asia (South Korea, Mongolia, Japan, and China), eastern Europe, and South America. Two-thirds of gastric cancers occur in developing countries.1-4
In the United States (U.S.), gastric cancer is the 15th most common cancer and it is often an aggressive form of the disease. As with gastric cancer around the world, most cases in the U.S. are typically diagnosed at an advanced stage, which leads to poor patient outcomes.4
The survival rates of gastric cancer vary depending on the stage of disease at diagnosis. Estimated survival rates based on people diagnosed with gastric cancer between 2009 and 2015 are published by the National Cancer Institute (Table 1).1
| Table 1: Estimated Survival Rates of Gastric Cancer in the United States1 |
| Extent of disease at diagnosis |
Cases by stage |
5-year relative survival |
| Localized: confined to the primary site |
28% |
68.8% |
| Regional: spread to regional lymph nodes |
26% |
31% |
| Distant: cancer has metastasized |
36% |
5.3% |
| Unknown: unstaged |
10% |
23% |
Risk factors for recurrent disease vary according to stage (disease extent), histologic grade, and status of resection margins.4 Even among patients who undergo gastrectomy for curative-intent gastric cancer, relapse rates remain high. After completion of local therapy, a majority of gastric cancers (70%-80%) relapse within 2 years and almost all (90%) recur within 5 years. It is estimated that at least 60% of patients will develop recurrent gastric cancer after curative resection.1-4
Esophagogastric junction (EGJ) adenocarcinoma is a type of cancer that begins near the gastroesophageal junction—the place where the esophagus connects to the stomach. In the curative-intent setting, treatment of EGJ adenocarcinoma is ambiguous and debatable, straddling the lines of esophageal and gastric cancers. In the advanced/metastatic setting, EGJ adenocarcinoma is often treated like gastric cancer, but a majority of statistical information regarding EGJ adenocarcinoma is collectively reported with esophageal cancer.
TREATMENT OF GASTRIC AND EGJ ADENOCARCINOMA
Most patients with gastric cancer will receive systemic treatment in the advanced, relapsed, recurrent, and metastatic settings.1-4 The standard work-up for upper gastrointestinal (GI) cancer includes upper GI endoscopy with biopsy, pathology, history and physical, complete blood count, metabolic panel and liver function labs, and imaging. Additionally, biomarker testing is very important in the evaluation of advanced, unresectable, and/or metastatic disease. At a minimum, biomarker testing should include human epidermal growth factor receptor 2 (HER2) status, microsatellite instability (MSI) status, and programmed death-ligand 1 (PD-L1) expression. These markers may have implications for treatment in the advanced/metastatic setting.4
Figure 1 lists the primary agents used in the systemic treatment of advanced/metastatic gastric and EGJ adenocarcinoma. The backbone of upper GI cancer treatments mainly consists of fluoropyrimidines (infusional 5-fluorouracil [5FU] or capecitabine) and a platinum analog (typically cisplatin or oxaliplatin) or a taxane (paclitaxel or docetaxel).4 Additions to the traditional chemotherapy backbone include biologic agents, specifically ramucirumab, which is an anti-vascular endothelial growth factor (VEGF) therapy, or trastuzumab, which is an anti-HER2 therapy for HER2-over-expressing tumors. Monotherapy options include an oral antimetabolite chemotherapy, trifluridine/tipiracil, or immunotherapy with pembrolizumab.
| Figure 1. Treatment Options for Advanced/Metastatic Gastric and Esophagogastric Junction Adenocarcinoma4 |
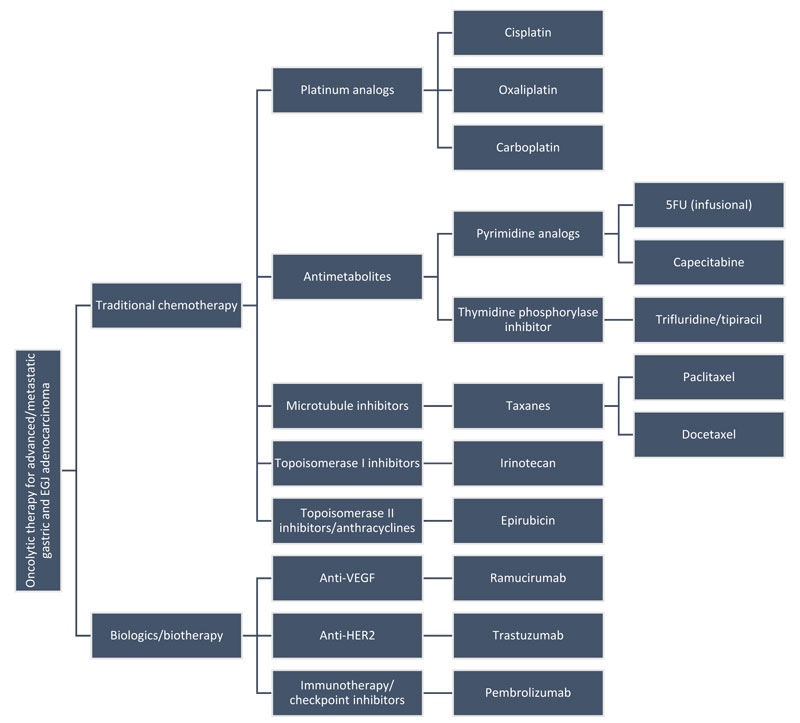 |
| 5FU, 5-fluorouracil; EGJ, esophagogastric junction; HER2, human epidermal growth factor receptor 2; VEGF, vascular endothelial growth factor. |
There are several options for first-line treatment of gastric or EGJ adenocarcinoma. Before deciding on a regimen, it is important to know the patient’s tumor molecular profile and biomarker status, performance status (PS), and organ function.4
Current options for treatment of metastatic gastric or EGJ adenocarcinoma are best supportive care (BSC) plus or minus systemic therapy. The National Comprehensive Cancer Network (NCCN) continuously advocates and encourages patients and providers to participate in clinical trials when eligible and states that “the best management of any patient with cancer is a clinical trial.”4 The choice to add systemic treatment will be made on the basis of discussions with the patient, baseline PS, access to care, organ function, and patient and provider preferences. Any patient with an Eastern Cooperative Oncology Group (ECOG) PS of 3 or higher or a Karnofsky Performance Status (KPS) less than 60% will likely not be able to tolerate systemic treatment and, for these patients, oncolytic therapy may be more harmful than helpful. In these cases, BSC alone should be strongly considered. For patients with an ECOG PS of 2 or lower or a KPS of 60% or higher, consider systemic treatment.4
At a minimum, molecular work-up should include HER2 status, deficient mismatch repair (dMMR)/MSI-high (MSI-H) status, and PD-L1 status of the tumor. An estimated 12% to 23% of gastric cancer patients over-express HER2, which is also known as “HER2-positive” status.4 According to therapies approved by the U.S. Food and Drug Administration (FDA), HER2 status is the most influential factor when selecting first-line treatment. Based on the results of the ToGA trial, a patient with HER2-positive gastric or EGJ adenocarcinoma is eligible to add trastuzumab to first-line chemotherapy.5
First-line treatment for metastatic disease: 2-drug and 3-drug regimens
Once the decision to treat with chemotherapy is made, the choice of agents/regimens largely involves deciding between 2-drug and 3-drug regimens. A 2-drug chemotherapy regimen is preferred in this setting due to a lower toxicity profile than that observed with 3-drug regimens.4 A 3-drug regimen should be reserved only for patients who are medically fit, have good PS, and have suitable access to care.4 A 3-drug chemotherapy regimen adds benefit in terms of overall survival (OS), progression-free survival (PFS), and response rate, but it does so at the cost of added toxicity in an already delicate patient population.4 Agents commonly used in 3-drug chemotherapy regimens include epirubicin, cisplatin, oxaliplatin, 5FU, capecitabine, and docetaxel. Specifically, the combinations of epirubicin, cisplatin, and 5FU (ECF) or ECF modifications (epirubicin, cisplatin, and capecitabine [ECX]) and docetaxel, cisplatin, and 5FU (DCF) and DCF modifications (docetaxel, oxaliplatin, and 5FU [DOF]) are widely recognized regimens in the setting of advanced/metastatic gastric and EGJ cancers.
The approach to treatment is an additional consideration when choosing between 2-drug and 3-drug chemotherapy regimens. Once metastatic disease is present, a patient is not eligible for surgical resection and the intent of treatment is to prolong survival and preserve/improve quality of life (QOL). Considering those treatment goals, choosing a 2-drug regimen allows preservation of QOL because of the reduced toxicity profile. In general, a 3-drug regimen will provide a more robust OS benefit compared with a 2-drug regimen. However, chemotherapy is limited by long-term toxicities and cancer most often develops resistance mechanisms to each line of treatment.4 Utilizing 3 powerful and robust (and likely toxic) chemotherapy agents upfront in the first-line setting leaves fewer options for subsequent lines of therapy.
For first-line treatment with a 2-drug regimen, the options include combinations of a fluoropyrimidine, a platinum-based compound, and a taxane: combinations can consist of a fluoropyrimidine plus a platinum or a platinum plus a taxane. The NCCN prefers a fluoropyrimidine-plus-platinum combination, with the fluoropyrimidine being either infusional 5FU or capecitabine and the platinum being either cisplatin or oxaliplatin (Table 2).4
| Table 2. First-Line 2-Drug Regimens for Advanced/Metastatic Gastric and Esophagogastric Junction Adenocarcinoma4 |
| |
Cisplatin |
Oxaliplatin |
| Infusional 5FU |
Cisplatin + 5FU (FP) |
Oxaliplatin + 5FU (FOLFOX) |
| Capecitabine |
Cisplatin + capecitabine (XP) |
Oxaliplatin + capecitabine (XELOX or CapeOx) |
| 5FU, 5-fluorouracil. |
Historically, 5FU and cisplatin have been the quintessential pair, but infusional 5FU or capecitabine with oxaliplatin (as FOLFOX or CapeOx) may be a better-tolerated pair. Other 2-drug combinations include cisplatin plus paclitaxel or docetaxel, paclitaxel plus carboplatin, and 5FU plus irinotecan (FOLFIRI). A fluoropyrimidine plus oxaliplatin or cisplatin remains the preferred 2-drug regimen in the first-line metastatic/unresectable setting.4
Additions to the chemotherapy backbone
Trastuzumab for HER2-positive metastatic gastric or EGJ adenocarcinoma is the only recommended and FDA-approved biotherapy agent that can be added to the chemotherapy backbone in the first-line advanced/metastatic setting.4 The use of trastuzumab is based on the ToGA trial, which was a landmark trial for the treatment of metastatic HER2-positive upper GI cancer. It was the first randomized, prospective, multicenter, phase III trial to evaluate safety and efficacy of trastuzumab in patients with HER2-positive gastric and EGJ adenocarcinoma. This trial established a new standard of care for HER2-positive gastric/EGJ adenocarcinoma.5 Patients were randomized 1:1 to receive chemotherapy for 6 cycles with or without trastuzumab. The chemotherapy consisted of cisplatin plus a fluoropyrimidine every 3 weeks (Figure 2).5
| Figure 2. Randomization of the ToGA Trial5 |
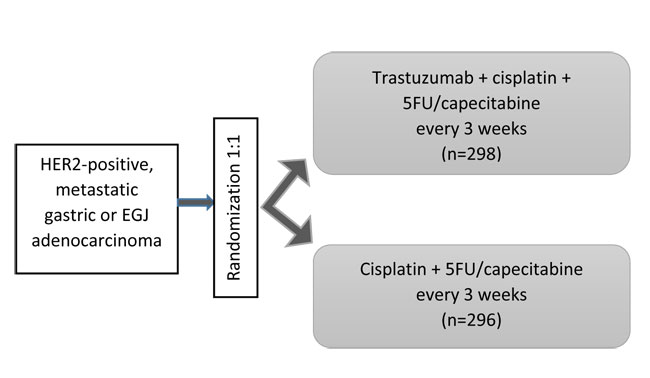 |
5FU: 800 mg/m2/day continuous IV infusion on days 1-5.
Cisplatin: 80 mg/m2 IV on day 1 for a total of 6 cycles.
Capecitabine: 2000 mg/m2/day in 2 divided doses on days 1-14 of a 21-day cycle.
Trastuzumab: 8 mg/kg IV loading dose on day 1 of cycle 1, followed by 6 mg/kg (maintenance dose) IV on day 1 of cycles 2 and beyond.
5FU, 5-fluorouracil; EGJ, esophagogastric junction; HER2, human epidermal growth factor receptor 2; IV, intravenously. |
The addition of trastuzumab did not significantly increase toxicities.4 As a result of the ToGA trial, trastuzumab plus cisplatin and 5FU became the NCCN-preferred and Category 1 recommendation for first-line metastatic HER2-over-expressing/positive adenocarcinoma (Table 3).4,5
| Table 3. Survival and Response Rates of the ToGA Trial5 |
| |
Trastuzumab + cisplatin/fluoropyrimidine |
|
Cisplatin/fluoropyrimidine |
| Median OS |
13.8 months |
p=0.0046 |
11.1 months |
| Median PFS |
6.7 months |
p=0.0002 |
5.5 months |
| Best overall response |
139 (47%) |
p=0.0017 |
100 (35%) |
| Complete response |
16 (5%) |
p=0.0599 |
7 (2%) |
| Partial response |
123 (42%) |
p=0.0145 |
93 (32%) |
| Stable disease |
93 (32%) |
-- |
101 (35%) |
| Progressive disease |
35 (12%) |
-- |
53 (18%) |
| OS, overall survival; PFS, progression-free survival. |
Although the ToGA trial used cisplatin as the platinum agent of choice, the NCCN allows some flexibility when adding trastuzumab to first-line chemotherapy4,6: the NCCN states that trastuzumab may be combined with other systemic chemotherapies. (It may not be combined with an anthracycline-containing regimen, however, as this can increase the risk of cardiomyopathy.) The combination of trastuzumab plus other chemotherapy is a Category 2B recommendation.4
Treatment of metastatic disease: second-line treatment and beyond
A majority of the recent practice changes and new FDA-approved therapies for upper GI cancer have largely been in the settings of second-line treatment and beyond. The choice for therapy beyond the first-line setting largely depends on the patient’s PS and his or her previous therapies. In addition to traditional chemotherapy (both combination therapy and monotherapy), ramucirumab with or without paclitaxel, trifluridine/tipiracil, and pembrolizumab are newer treatment options in the second-line and beyond settings.
Ramucirumab
Ramucirumab is a human monoclonal antibody (mAB) vascular endothelial growth factor receptor 2 (VEGFR2) antagonist. Blocking VEGFR2 prevents the VEGF ligands from binding to the receptor, which reduces tumor vascularity and growth, essentially “choking-off” the tumor’s blood and nutrition supplies.7
Ramucirumab was first approved by the FDA in April 2014 as monotherapy for treatment of gastric and EGJ adenocarcinoma.7 The phase III trial supporting this indication was the REGARD trial, the results of which were published by Fuchs and colleagues in October 2013 (Table 4).8 This was a phase III, international, multi-center, randomized, placebo-controlled trial of ramucirumab monotherapy for previously treated advanced gastric or EGJ adenocarcinoma. Patients who progressed after first-line chemotherapy consisting of a platinum plus a fluoropyrimidine with or without an anthracycline were randomized to ramucirumab 8 mg/kg intravenously (IV) every 2 weeks or placebo (Figure 3).8
| Table 4. Survival and Response Rates of the REGARD Trial8 |
| |
Ramucirumab |
|
Placebo |
| Median OS |
5.2 months |
HR (95% CI) = 0.776
(0.603-0.998); p=0.047 |
3.8 months |
| Median PFS |
2.1 months |
HR (95% CI) = 0.483
(0.376-0.620); p<0.0001 |
1.3 months |
| Best overall response |
|
|
|
| Complete response |
1 (< 1%) |
-- |
0 |
| Partial response |
7 (3%) |
-- |
3 (3%) |
| Stable disease |
108 (45%) |
-- |
24 (21%) |
| Progressive disease |
78 (33%) |
-- |
63 (54%) |
| CI, confidence interval; HR, hazard ratio; OS, overall survival; PFS, progression-free survival. |
| Figure 3. Randomization of the REGARD Trial8 |
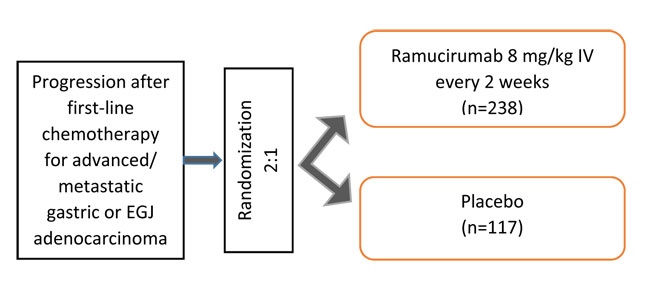 |
Note: crossover was NOT allowed.
EGJ, esophagogastric junction; IV, intravenously. |
Toxicities of any grade were reported in 94% of patients in the ramucirumab arm and in 88% of patients in the placebo arm. Hypertension was more common in the ramucirumab arm than the placebo arm (16% vs. 8%). However, similar rates of other toxicities, including fatigue, venous thromboembolism, arterial thromboembolism, bleeding/hemorrhage, proteinuria, GI perforation, fistula formation, and infusion-related reactions, were seen in both arms.8
Almost 1 year after the REGARD trial was published, in September 2014, the results of the phase III RAINBOW trial were published by Wilke and colleagues (Table 5).9 This trial was similar in design to the REGARD trial, except that ramucirumab was combined with and compared to chemotherapy with paclitaxel. Patients who progressed after first-line chemotherapy consisting of a platinum plus a fluoropyrimidine with or without an anthracycline were randomized 1:1 to ramucirumab plus paclitaxel or placebo plus paclitaxel (Figure 4).9
| Table 5. Survival and Response Rates of the RAINBOW Trial9 |
| |
Ramucirumab + paclitaxel |
|
Placebo + paclitaxel |
| Median OS |
9.6 months |
HR (95% CI) = 0.807
(0.678-0.962); p=0.017 |
7.4 months |
| Median PFS |
4.4 months |
HR (95% CI) = 0.635
(0.536-0.752);
p<0.0001 |
2.9 months |
| Best overall response |
|
|
|
| Complete response |
2 (< 1%) |
-- |
1 |
| Partial response |
90 (27%) |
-- |
53 (16%) |
| Stable disease |
172 (52%) |
-- |
159 (47%) |
| Progressive disease |
43 (13%) |
-- |
83 (25%) |
| CI, confidence interval; HR, hazard ratio; OS, overall survival; PFS, progression-free survival. |
| Figure 4. Randomization of the RAINBOW Trial9 |
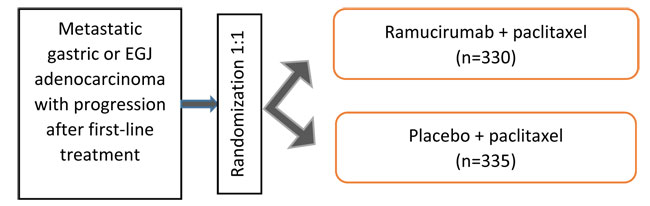 |
Note: crossover was NOT allowed.
Paclitaxel: 80 mg/m2 IV on days 1, 8, and 15 of a 28-day cycle.
Placebo: IV on days 1 and 15 of a 28-day cycle.
Ramucirumab: 8 mg/kg IV on days 1 and 15 of a 28-day cycle.
EGJ, esophagogastric junction; IV, intravenously. |
As expected, the toxicity profile in the RAINBOW trial was more significant than in the REGARD trial (Table 6).9 Hypertension, neutropenia, leukopenia, and fatigue were more common in the ramucirumab-plus-paclitaxel arm.
| Table 6. Adverse Events Noted in the RAINBOW Trial9 |
| Grade ≥ 3 adverse events |
Ramucirumab + paclitaxel |
Placebo + paclitaxel |
| Neutropenia |
133 (41%) |
62 (19%) |
| Febrile neutropenia |
10 (3%) |
8 (2%) |
| Leucopenia |
57 (17%) |
22 (7%) |
| Hypertension |
46 (14%) |
8 (2%) |
| Fatigue |
39 (12%) |
18 (5%) |
| Anemia |
30 (9%) |
34 (10%) |
| Abdominal pain |
20 (6%) |
11 (3%) |
On the basis of the RAINBOW trial, the ramucirumab indication was updated in November 2014 to include combination therapy with ramucirumab plus paclitaxel for advanced gastric or EGJ adenocarcinoma after prior systemic therapy. This combination regimen is currently the only NCCN-preferred and Category 1 doublet therapy for second-line treatment of advanced disease.9 Of note, the RAINFALL trial, a phase III, double-blind, randomized, placebo-controlled trial of ramucirumab plus cisplatin and 5FU versus placebo plus cisplatin and 5FU in the first-line metastatic setting yielded no OS benefit. Therefore, the place in therapy for ramucirumab remains in the second-line metastatic setting.
Ramucirumab is dosed at 8 mg/kg of actual body weight and administered IV every 2 weeks over 60 minutes. The manufacturer recommends premedication with a histamine-1 antagonist (e.g., diphenhydramine) to reduce infusion-related hypersensitivity reactions with ramucirumab.7
Other second-line options
Other options for second-line treatment of gastric and EGJ adenocarcinoma include chemotherapy (e.g., FOLFIRI or monotherapy with paclitaxel, docetaxel, or irinotecan). There are many ongoing clinical trials trying to incorporate immunotherapy (i.e., checkpoint inhibitors) with chemotherapy in the second-line setting. However, to date, there have been no FDA approvals or NCCN guideline changes related to this research.4 The exception is within the minority population of MSI-H metastatic gastric cancer.
Pembrolizumab can be used in the second-line metastatic setting for patients who have MSI-H status. The current FDA approval for pembrolizumab includes any MSI-H metastatic solid tumor. The significance and impact of MSI-H in gastric cancer is still being explored. The overall incidence of MSI-H status in gastric cancer varies widely from 5% to 30%, depending on the study population (i.e., Asian versus western populations).12,13 The Cancer Genome Atlas data estimate the incidence of MSI-H in all-stage gastric cancer to be approximately 22%.14
Third-line treatment options
Currently, third-line therapy includes trifluridine/tipiracil or pembrolizumab. Chemotherapy is still an option, as well.4
Trifluridine/tipiracil. Trifluridine/tipiracil is an oral, anti-metabolite chemotherapy: more specifically, it is a fluoropyrimidine and thymidine phosphorylase inhibitor combination that was first approved by the FDA for refractory metastatic colorectal cancer in 2015.15 Recently, in February 2019, trifluridine/tipiracil expanded its indications to include advanced, refractory gastric/EGJ adenocarcinoma on the basis of data from the phase III TAGS trial (Table 7).16 The TAGS trial, published by Shitara and colleagues in October 2018, was a phase III, placebo-controlled, double-blind trial of trifluridine/tipiracil plus BSC versus placebo plus BSC in patients with heavily pre-treated metastatic gastric and EGJ adenocarcinoma (Figure 5).16
| Table 7. Survival and Response Rates of the TAGS Trial16 |
| |
Trifluridine/tipiracil + BSC |
|
Placebo + BSC |
| Median OS |
5.7 months (4.8-6.2) |
HR (95% CI) = 0.69
(0.56-0.85);
1-sided p=0.00029,
2-sided p=0.00058 |
3.6 months (3.1-4.1) |
| Median PFS |
2 months (1.0-2.3) |
HR = 5.7 (95% CI: 0.47-0.70);
2-sided p<0.001 |
1.8 months (1.7-1.9) |
| Tumor response |
|
|
|
| Objective response |
4% |
P=0.28 |
2% |
| Disease control |
44% |
P<0.001 |
14% |
| Median time to deterioration of ECOG PS score to ≥ 2 |
4.3 months |
HR = 0.69 (95% CI: 0.56-0.85)
2-sided p=0.00053 |
2.3 months |
| BSC, best supportive care; CI, confidence interval; ECOG PS, Eastern Cooperative Oncology Group Performance Status; HR, hazard ratio; OS, overall survival; PFS, progression-free survival. |
| Figure 5. Randomization of the TAGS Trial16 |
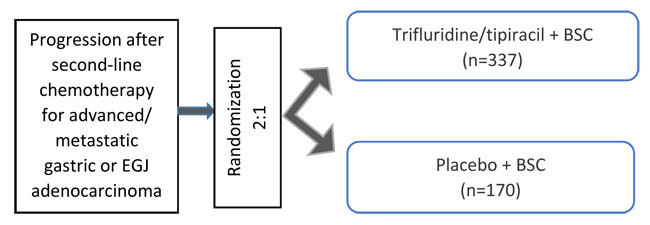 |
Trifluridine/tipiracil: 35 mg/m2 by mouth twice daily on days 1-5 and 8-12 of a 28-day cycle.
BSC, best supportive care; EGJ, esophagogastric junction. |
| Table 8. Adverse Events Noted in the TAGS Trial16 |
| Grade ≥ 3 adverse events |
Trifluridine/tipiracil + BSC (n=335) |
Placebo + BSC (n=168) |
| Any treatment-related ADR |
176 (53%) |
22 (13%) |
| Neutropenia |
114 (34%) |
0 |
| Febrile neutropenia |
6 (2%) |
0 |
| Anemia |
64 (19%) |
13 (8%) |
| Leucopenia |
31 (9%) |
0 |
| Fatigue |
23 (7%) |
10 (6%) |
| Thrombocytopenia |
11 (3%) |
0 |
| Nausea |
10 (3%) |
5 (3%) |
| ADR, adverse drug reaction; BSC, best supportive care. |
On the basis of the improved survival data and acceptable safety profile (Table 8), trifluridine/tipiracil was approved by the FDA as single-agent treatment for metastatic gastric or EGJ adenocarcinoma previously treated with at least 2 prior lines of chemotherapy, including a fluoropyrimidine AND a platinum AND either a taxane OR irinotecan, and, if appropriate, HER2-targeted therapy.15
Because of the robust trial design—a phase III, randomized trial with statistically and clinically significant outcomes— trifluridine/tipiracil became the only NCCN-preferred and Category 1 regimen for third-line or subsequent therapy.4
Pembrolizumab. Pembrolizumab is the most studied immunotherapy agent for gastric and EGJ adenocarcinoma. It is an immune checkpoint inhibitor: specifically, a mAb blocking the programmed cell death protein (PD)-1 receptor. The result is an increased immune response that will hopefully stimulate the patient’s innate immune system to eliminate or “treat” the cancer. Currently, immunotherapy exists in 2 key scenarios in the treatment of gastric and EGJ adenocarcinoma11:
- dMMR/MSI-H: The use of pembrolizumab in dMMR/MSI-H gastroesophageal cancer is based on the phase II, open-label KEYNOTE-01617 trial, which evaluated the activity of pembrolizumab in any dMMR/MSI-H solid tumor. The results led to the FDA approval of pembrolizumab use in any dMMR/MSI-H solid tumor that has progressed following prior treatment.11
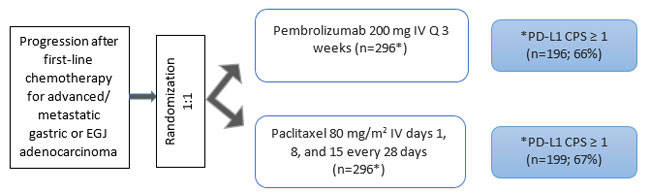
- PD-L1 positive: Because dMMR/MSI-H gastroesophageal cancer is uncommon, the use of pembrolizumab in gastroesophageal cancer patients relies on having a PD-L1-positive tumor. The phase IB KEYNOTE-012,18 phase II KEYNOTE-059,19 and phase III KEYNOTE-06120 trials are of importance in this patient population (Figure 6).
Among various cancer types, PD-L1 positivity may be calculated and reported by different scoring systems. In gastric and EGJ adenocarcinoma, it is defined by a combined positive score (CPS) of 1% or higher. (To read more about how the scores are calculated and reported, please see the pembrolizumab prescribing information.11) The CPS score/PD-L1 positivity is usually reported on the patient’s tumor pathology report.
| Figure 6. Trial Designs Evaluating Pembrolizumab in PD-L1 Positive Cancer18-20 |
Phase IB KEYNOTE-01218
 |
KEYNOTE-059, cohort 119
 |
| Of the 259 patients enrolled in cohort 1, 57.1% were PD-L1 positive and 42.1% were PD-L1 negative. |
KEYNOTE-059, cohort 219
 |
Cohort 2 received pembrolizumab plus chemotherapy for first-line metastatic gastric and EGJ adenocarcinoma. Patients could be PD-L1 positive or negative in this cohort. Overall, 64% of patients in cohort 2 had a CPS ≥ 1.
*Chemotherapy consisted of cisplatin 80 mg/m2 IV on day 1 plus 5FU 800 mg/m2/day via continuous infusion on days 1-5 of every 21-day cycle. In Japan, patients received capecitabine (1000 mg/m2 by mouth twice daily on days 1-14) in place of infusional 5FU. |
KEYNOTE-059, cohort 319
 |
| Cohort 3 only included PD-L1-positive patients receiving first-line therapy for metastatic gastric and EGJ adenocarcinoma. |
KEYNOTE-06120
 |
| 5FU, 5-fluorouracil; ADR, adverse drug reaction; CPS, combined positive score; CR, complete response; EGJ, esophagogastric junction; IV, intravenously; ORR, objective response rate; PD-L1, programmed death-ligand 1; PR, partial response. |
The KEYNOTE-059 was a multicenter, open-label, non-randomized, 3-cohort, phase II study of pembrolizumab for previously treated and first-line advanced or metastatic gastric or EGJ adenocarcinoma. Cohort 1 evaluated pembrolizumab in patients who had received 2 or more previous therapies; the results of this cohort were published in May 2018. Cohorts 2 and 3 evaluated pembrolizumab in the first-line advanced/metastatic setting. The results of these cohorts were recently published in July 2019. An important consideration for this study is that patients did not need to be PD-L1 positive to enroll in this protocol.19
When the authors divided patients by PD-L1 status, PD-L1 positivity resulted in an objective response rate (ORR) of 15.5% with a median duration of response of 16.3 months; PD-L1-negative patients had an ORR of 6.4% and a median duration of response of 6.9 months. Median OS of the population was 5.6 months: 5.8 months in PD-L1-positive patients and 4.9 months in PD-L1-negative patients.
The total population median PFS was 6.6 months and median OS was 13.8 months. When stratified for PD-L1/CPS of 1 or higher, the median OS was 11.1 months. Patients who were PD-L1 negative had a median OS of 19.8 months. The median PFS was 3.3 months and the median OS was 20.7 months in this cohort of patients.
The KEYNOTE-061 trial was a phase III, randomized, open-label, multicenter study comparing pembrolizumab and paclitaxel for second-line treatment of gastric or EGJ adenocarcinoma. The trial originally enrolled patients regardless of CPS status, but it changed to only enroll patients with CPS of 1 or higher after the first 489 patients were enrolled. According to the results of KEYNOTE-061, pembrolizumab did not extend OS or PFS compared to paclitaxel monotherapy. However, it did have a more favorable adverse drug reaction profile (Table 9).20
| Table 9. Survival, Response Rates, and Adverse Events Noted in the KEYNOTE-061 Trial20 |
| |
Pembrolizumab (CPS ≥ 1)
(n=196) |
Paclitaxel (CPS ≥ 1)
(n=199) |
Median OS
(HR 0.82, 95% CI: 0.66-1.03, 1-sided p = 0.0421) |
9.1 months |
8.3 months |
Median PFS
(HR 1.27, 95% CI: 1.03-1.57) |
1.5 months |
4.1 months |
| 1-year OS |
90% |
94% |
| Overall response rate |
16% |
14% |
| Duration of response |
18 months |
5.2 months |
| Grade ≥ 3 ADRs |
42 (14%) |
96 (35%) |
Fatigue
|
7 (2%) |
13 (5%) |
Anemia
|
7 (2%) |
12 (4%) |
Decreased appetite
|
2 (<1%) |
0 |
| Decreased neutrophil count |
0 |
28 (10%) |
| ADR, adverse drug reaction; CI, confidence interval; CPS, combined positive score; HR, hazard ratio; OS, overall survival; PFS, progression-free survival. |
In June 2019, the results of the KEYNOTE-062 trial were presented as an abstract (LBA4007) by the American Society of Clinical Oncologists. This was a phase III randomized trial of pembrolizumab with or without chemotherapy versus chemotherapy alone as first-line treatment of metastatic, HER2-negative, PD-L1-positive (defined as CPS ≥ 1) gastric or EGJ adenocarcinoma (Figure 9).21
| Figure 9. Randomization of the KEYNOTE-062 Trial21 |
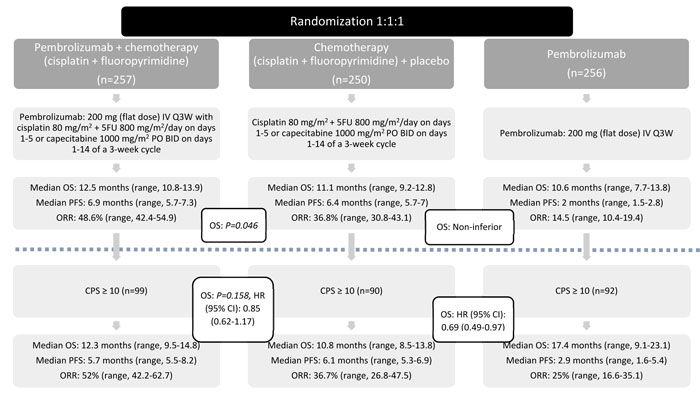 |
| 5FU, 5-fluorouracil; BID, twice daily; CI, confidence interval; CPS, combined positive score; HR, hazard ratio; IV, intravenously; Q3W, every 3 weeks; PO, by mouth; ORR, overall response rate; OS, overall survival; PFS, progression-free survival. |
While the results of KEYNOTE-062 were somewhat lackluster, they do suggest that there is a clinically meaningful benefit to pembrolizumab over chemotherapy in patients with a CPS of 10 or higher. However, adding pembrolizumab to chemotherapy did not improve OS or PFS, regardless of CPS status. There may be a role for first-line, single-agent pembrolizumab in patients with a CPS of 10 or higher. Additionally, because of its improved toxicity profile, it may be useful for patients who may not be able to tolerate first-line traditional chemotherapy. It is important to remember that this stratification for CPS was somewhat of an afterthought. Approximately one-third of patients in each treatment arm had a CPS of 10 or more, and this study was not designed nor powered properly to detect a difference for this sub-population. This topic will continue to be explored as these data mature and more trials are conducted.21
The role of immunotherapy
So far, immunotherapy has not been the “blockbuster” treatment for gastric and EGJ adenocarcinoma that it has proved to be for other oncologic disease states. Many immunotherapy-containing trials are currently underway.
Pembrolizumab’s current indication is as single-agent treatment for advanced/metastatic gastric or EGJ adenocarcinoma whose tumors express PD-L1 (CPS ≥ 1) with disease progression during or after 2 or more prior lines of therapy including prior fluoropyrimidine-and-platinum-containing chemotherapy, and if appropriate, HER2-targeted therapy.11 However, if a patient has metastatic gastric/EGJ adenocarcinoma that is MSI-H, pembrolizumab can be used in the second-line metastatic setting, since pembrolizumab’s indication includes any MSI-H solid tumor.11
Putting together the primary literature
Staying up to date with primary oncologic literature can be overwhelming. Figure 10 provides a simplified decision-making algorithm for available treatments for gastric and EGJ adenocarcinoma according to patient factors and preferences.4
| Figure 10. Treatment Decision-Making Algorithm for Gastric and Esophagogastric Junction Adenocarcinoma4 |
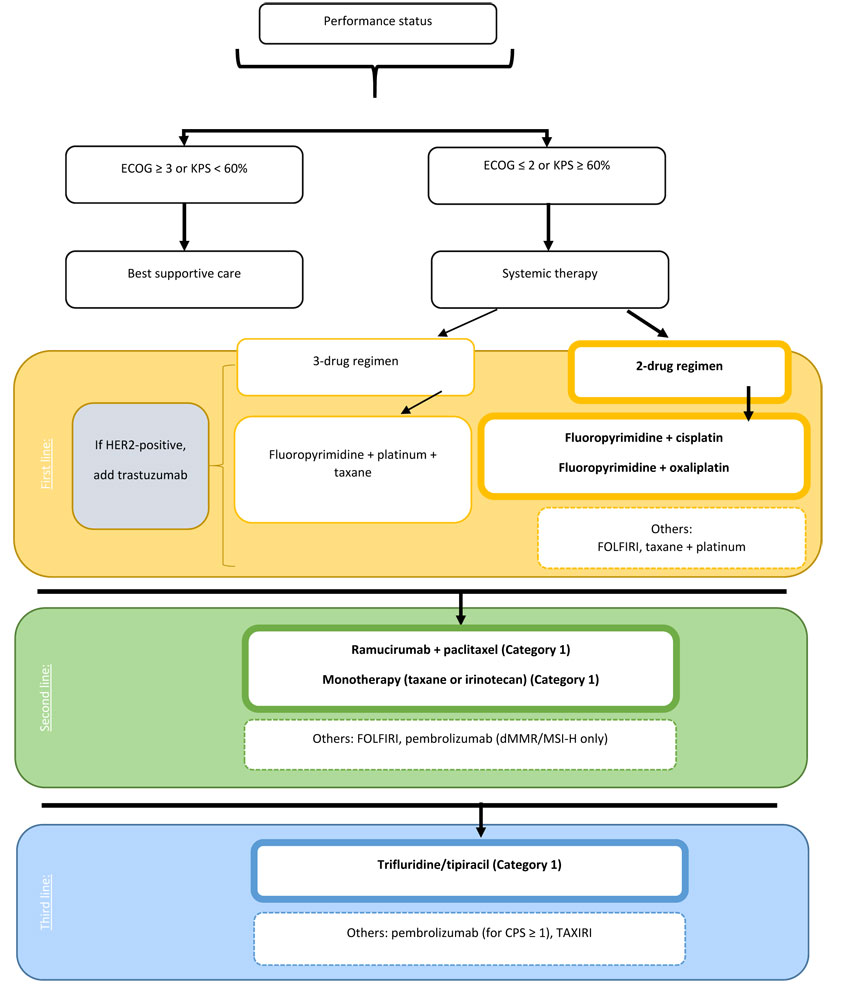 |
Note: Bolded items are “preferred” by the NCCN.
CPS, combined positive score; dMMR/MSI-H, deficient mismatch repair/microsatellite instability-high; ECOG, Eastern Cooperative Oncology Group; FOLFIRI, irinotecan + leucovorin + 5-fluorouracil; HER2, human epidermal growth factor receptor 2; KPS, Karnofsky Performance Status; NCCN, National Comprehensive Cancer Network; taxane, docetaxel or paclitaxel; TAXIRI, irinotecan + paclitaxel or docetaxel. |
When making treatment decisions, follow these steps:
- Stratify by PS. If PS allows for systemic treatment, continue with choosing a treatment.
- For first-line treatment, a 2-drug chemotherapy cocktail is preferred: infusional 5FU or capecitabine plus a platinum-based compound (cisplatin or oxaliplatin). Other chemotherapy options include FOLFIRI or a platinum plus a taxane. Add trastuzumab if the tumor over-expresses HER2.
- For second-line treatment, ramucirumab plus paclitaxel is preferred (Category 1). Other chemotherapy options include FOLFIRI or a single-agent taxane.
- For third-line treatment, trifluridine/tipiracil is preferred (Category 1). Other options include immunotherapy with pembrolizumab or chemotherapy with a taxane, platinum, or irinotecan, if not used earlier in treatment.
TREATMENT CONSIDERATIONS AND BARRIERS WITH NEWER THERAPIES
Patients with advanced/metastatic gastric and EGJ adenocarcinoma are particularly fragile and require attention to detail. Choosing a treatment requires several considerations, including drug acquisition, adherence, and formulation, as well as adverse events and dose adjustments.
Adherence, formulation, and drug acquisitionconsiderations
Therapy with trifluridine/tipiracil is appealing because patients do not have to travel for intravenous infusions, get a needle stick for therapy administration, or carry an ambulatory intravenous pump, but there are other barriers to overcome when using this medication.
Trifluridine/tipiracil is dosed at 35 mg/m2 of body surface area (BSA) per dose (based on the trifluridine component; maximum of 80 mg per dose). It is administered by mouth twice daily on days 1 through 5 and 8 through 12 of a 28-day cycle. Trifluridine/tipiracil tablets are available in 2 strengths: 15 mg trifluridine/6.14 mg tipiracil and 20 mg trifluridine/8.19 mg tipiracil; these tablets are different colors.15 The availability of 2 tablet strengths allows for a more accurate BSA-based dose, but prescribing more than 1 tablet strength is often confusing to patients and leads to more than 1 prescription copay.
Preferably, trifluridine/tipiracil tablets should stay in their original container: they can be stored outside the original bottle, but, if so, they must be discarded after 30 days. Also, because trifluridine/tipiracil is chemotherapy, caution should be taken when handling this medication. Anyone who handles or comes in contact with this medication should use appropriate precautions for receiving, handling, administration, and disposal. Single-use gloves should be worn during receiving, unpacking, and placing in storage. The National Institute for Occupational Safety and Health recommends wearing single-use gloves for administration of intact tablets or capsules.15,22 With that in mind, it is best to advise patients to keep their trifluridine/tipiracil tablets in the original bottle, not to combine the tablets into containers holding other medications, and not to let anyone else handle their medication.
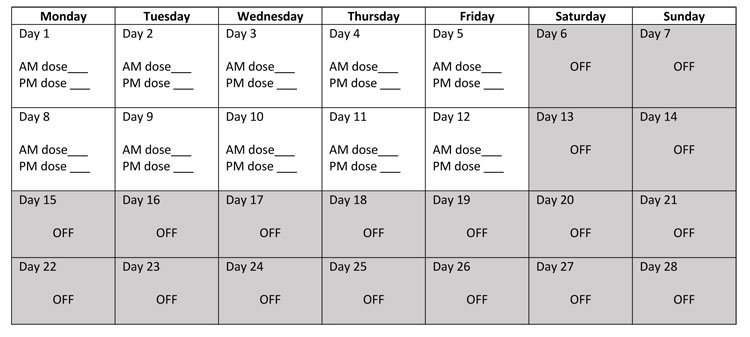
The trifluridine/tipiracil dosing scheme can be very confusing. Since it is taken only on certain days of a 28-day cycle, the administration can become very confusing, especially if patients start the regimen mid-week. Advise patients to keep a calendar and mark the doses as they take them: this is a very effective way to help track when doses are given, when they are due, and when “off” days are scheduled. An additional counseling tip is to advise patients to start the 28-day cycles on a Monday. This way, days 1 through 5 and 8 through 12 are Monday through Friday, which most patients find works well with their other daily and weekly activities. Figure 11 provides a sample dosing calendar that can be shared with patients.
| Figure 11. Sample Dosing Calendar for a 28-day Cycle of Trifluridine/Tipiracil |
 |
The trifluridine/tipiracil tablet formulation itself presents an additional challenge, particularly in the gastric and EGJ cancer population. The tablets should be taken with food and swallowed whole.15 At this time, there is no data to support breaking or crushing tablets or administering via a feeding tube. Many patients may have difficulty swallowing, pain with swallowing, or refractory reflux, and taking up to 4 tablets by mouth, with food, twice a day can be a significant compliance barrier for these patients. Additionally, if a patient has undergone a previous gastrectomy, a majority or all of their stomach may be missing. This leads to a question of the pharmacokinetic absorptive properties of this oral therapy in a patient without a stomach; in the same way, the question of how food affects absorption of oral medications is a consideration for many therapies.
Drug acquisition can be a substantial barrier to the use of trifluridine/tipiracil. It is only dispensed from specialty pharmacies, so the prescribing team must often investigate which specialty pharmacy is contracted with the patient’s insurance provider. Many specialty pharmacies will accept prescriptions via fax or e-prescribing, which eases some burden related to drug acquisition and prescribing, but the process of getting the drug to the patient can still be lengthy: the time needed to identify the pharmacy, send the prescription, create the patient profile, complete prior authorization, and contact the patient for delivery usually takes at least 1 week. Since many oncology patients are anxious to start new treatment after recent disease progression, the workflow must be explained and realistic expectations about time to drug delivery must be set and this information must be effectively communicated to the patient.15
Cost can be another barrier to drug acquisition. Trifluridine/tipiracil is prescription chemotherapy and, as such, is usually billed through the patient’s prescription insurance plan. The average wholesale price varies according to tablet strength and quantity (packages of 20, 40, or 60), and the costs of these different bottle/package sizes and strengths vary from $4000 to nearly $16,000.23 For a patient on the maximum dose of trifluridine/tipiracil—80 mg by mouth twice daily—80 tablets would be prescribed for a single 28-day cycle. The cost of the 20-mg tablets in a 60-tablet pack plus a 20-tablet pack would be close to $20,000. While many insurance providers cover trifluridine/tipiracil because it is FDA approved and listed in NCCN compendia, patients without private insurance (e.g., those with Medicare) are often faced with prohibitive medication costs. Some cost-savings options for patients without private insurance include copay assistance, coupon cards, and patient-assistance programs. Unfortunately, patients with Medicare are often excluded from these programs: these patients may be able to access support through non-profit organizations. Simply, many steps and many delays are usually involved in overcoming these cost barriers, and, in the end, the medication may still be too expensive for patients to afford. Additionally, these steps can consume precious time of the prescriber/prescribing team. More resources for both patients and prescribers regarding cost, including information about available cost-assistance programs, can be found on the Lonsurf website.15
Adverse events and disease-related concerns
The adverse event profile and the disease state itself present barriers to the use of certain medications in gastric and EGJ adenocarcinoma.
Nausea and vomiting
Trifluridine/tipiracil is associated with a moderate emetic potential15, 24 and, therefore, it is recommended that patients be premedicated with antiemetic therapy to prevent nausea and vomiting. Most gastric and EGJ cancer patients have some degree of symptoms from their primary disease: reflux, persistent nausea, early satiety, or difficulty swallowing. For these patients, taking oral chemotherapy that is associated with a moderate emetic potential can present challenges, not only in tolerating the actual tablets but with treating refractory or persistent nausea.
Thromboembolism
A risk of thromboembolism is associated with anti-VEGF therapy with ramucirumab. Patients with active cancer are coagulopathic by nature and already at an increased risk of a thrombotic event. While not a contraindication to use, initiating ramucirumab therapy in a patient with a blood clot requires a discussion of risk versus benefit with all members of the healthcare team. Thromboembolism, either venous or arterial, is a potentially fatal complication, so initiating or continuing a patient on ramucirumab should be carefully considered.7
GI bleeding
Patients whose gastric or EGJ adenocarcinoma has not been surgically removed (i.e., “primary intact”) are at high risk of bleeding, specifically a major GI bleed. Ramucirumab carries a black box warning for hemorrhage. Caution should be exercised when initiating or continuing ramucirumab in patients whose primary upper GI cancer is still intact and in patients with a history of an upper GI bleed. Ramucirumab should be discontinued in a patient with a severe or life-threatening bleed. Discontinue frequent non-steroidal anti-inflammatory drug use and/or high-dose corticosteroids, as these can cause further gastric upset and contribute to this complication.7
GI obstructions and/or perforations
GI perforations and obstructions are also of interest in patients with abdominal disease–primarily peritoneal carcinomatosis and/or omental disease spread. Peritoneal disease is a common metastasis in gastric cancer: the cancer is often caked on the inside of the abdomen and the lining of the abdomen, sitting on top of the bowels; this caked-on cancer pushes down on the bowels and can strangulate the bowels, leading to several complications. All antiangiogenic therapy, as well as ramucirumab, is associated with GI perforation and, if metastatic peritoneal cancer is intertwined and strangulating the bowels, it could theoretically increase the risk of intestinal obstruction, perforation, or fistula. The data to support this are largely extrapolated from the gynecologic oncology patient population. While not a contraindication, to use, prescribers should heavily weigh risk versus benefit of ramucirumab in a patient with an active or recent history of bowel obstruction.7
Autoimmune and transplant considerations
For a patient who is a candidate for pembrolizumab, a thorough investigation of the patient’s medication list and past medical history is crucial. Pharmacists are key in helping to identify any immunosuppressive therapy or anti-rejection medications used for the treatment of various autoimmune disorders or previous transplants. Patients who have undergone organ or bone marrow transplant can be at risk for potentially fatal organ rejection or graft-versus-host-disease from immunotherapy. For patients with autoimmune disorders, pembrolizumab has the potential to aggravate or exacerbate dormant or active autoimmune disease. Significant relapses of autoimmune disease complicated by severe symptom burden have been seen with immunotherapy, including pembrolizumab.11
Pharmacists must have a vigilant and detailed eye for medications and their doses for several drug categories, including corticosteroids (oral, topical, and rectal formulations), calcineurin inhibitors, mTOR kinase inhibitors, tumor necrosis factor blocking agents, Janus-associated kinase inhibitors, selective T-cell co-stimulation blockers, interleukin inhibitors, oral methotrexate, and other immunosuppressant and disease-modifying therapies, that patients may be taking.
Weight changes and nutritional deficiencies
Many of the therapies for gastric and EGJ adenocarcinoma use some form of weight-based dosing (e.g., mg/kg or BSA). Because of the anatomic location of disease and disease spread, as well as the aggressive nature of advanced gastric or EGJ adenocarcinoma, patients are often losing weight, both muscle and fat, because of their inability to eat, lack of appetite, early satiety, or physical limitations of their GI tract. The resulting malnourishment not only affects the actual weight of the patient but their nutritional composition, as well, which can impact dosing.
Dose adjustments based on changes in weight
All doses of chemotherapy, ramucirumab, and trifluridine/tipiracil used in the treatment of advanced upper GI cancer are calculated using weight. Traditional chemotherapy and trifluridine/tipiracil are dosed using BSA, which is calculated using height and weight15; ramucirumab dosing is determined by calculating the number of milligrams of drug per kilogram of body weight.7 Patients who are consistently losing weight will continually need their doses adjusted. For example, with trifluridine/tipiracil, the dose calculated when the patient is seen and the prescription is written could differ significantly by the time the patient is due to start the second cycle of therapy, warranting a new prescription be written.
Changes in protein binding
Changes in weight can also cause nutritional and metabolic deficiencies. Serum albumin is one such metabolic component that is specific to drug distribution. As patients continue to lose weight, at times becoming cachexic, albumin levels will also decrease. Certain medications are highly bound to serum albumin, and, when there is less albumin to bind medication, the result is more “free” or “active” drug in plasma that is able to distribute into tissues and organs. Trifluridine/tipiracil is highly bound to human serum albumin.15 If a patient has low serum albumin concentrations, the medication will have an increased volume of distribution into tissue, raising the concern for increased toxicity.
CONCLUSION
Treatment of metastatic gastric and EGJ adenocarcinoma is a complex process that involves multiple factors. There are numerous ways that pharmacists can contribute to the cancer treatment decision-making process, including weighing the projected efficacy of treatment with the adverse event profile; considering patient-specific factors related to PS; and assessing organ function, cost, feasibility of treatment administration, and anatomic location(s) of metastatic disease spread.
REFERENCES
- National Cancer Institute. Surveillance, Epidemiology, and End Results (SEER) Program. Cancer facts: Stomach cancer. https://seer.cancer.gov/statfacts/html/stomach.html. Accessed October 7, 2019.
- Crew KD, Neugut AI. Epidemiology of gastric cancer. World J Gastroenterol. 2006;12(3):354-62.
- Sitarz R, Skierucha M, Mielko J, et al. Gastric cancer: epidemiology, prevention, classification, and treatment. Cancer Manag Res. 2018;10:239-48.
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Gastric Cancer. Version 2.2019. https://www.nccn.org/professionals/physician_gls/pdf/gastric_blocks.pdf. Published June 4, 2019. Accessed August 5, 2019.
- Bang YJ, Van Cutsem E, Feyereislova A, et al; ToGA Trial Investigators. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet. 2010; 376(9742):687-97.
- Soularue E, Cohen R, Tournigand C, et al; for GERCOR. Efficacy and safety of trastuzumab in combination with oxaliplatin and fluorouracil-based chemotherapy for patients with HER2-positive metastatic gastric and gastro-oesophageal junction adenocarcinoma patients: a retrospective study. Bull Cancer. 2015;102(4):324-31.
- CYRAMZA [package insert]. Indianapolis, IN: Eli Lilly and Company; 2019.
- Fuchs CS, Tomasek J, Yong CJ, et al; REGARD Trial Investigators. Ramucirumab monotherapy for previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (REGARD): an international, randomised, multicentre, placebo-controlled, phase 3 trial. Lancet. 2014;383(9911):31-9.
- Wilke H, Muro K, Van Cutsem E, et al; RAINBOW Study Group. Ramucirumab plus paclitaxel versus placebo plus paclitaxel in patients with previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (RAINBOW): a double-blind, randomised phase 3 trial. Lancet Oncol. 2014;15(11):1224-35.
- Fuchs CS, Shitara K, Di Bartolomeo M, et al; RAINFALL Study Group. Ramucirumab with cisplatin and fluoropyrimidine as first-line therapy in patients with metastatic gastric or junctional adenocarcinoma (RAINFALL): a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Oncol. 2019;20(3):420-35.
- KEYTRUDA [package insert]. Whitehouse Station, NJ: Merck & Co., Inc; 2019.
- Kim JY, Shin NR, Kim A, et al. Microsatellite instability status in gastric cancer: a reappraisal of its clinical significance and relationship with mucin phenotypes. Korean J Pathol. 2013;47(1):28-35.
- Ratti M, Lampis A, Hahne JC, et al. Microsatellite instability in gastric cancer: molecular bases, clinical perspectives, and new treatment approaches. Cell Mol Life Sci. 2018;75(22):4151-62.
- The Cancer Genome Atlas Research Network. Comprehensive molecular characterization of gastric adenocarcinoma. Nature. 2014;513(7517):202-9.
- LONSURF [package insert]. Princeton, NJ: Taiho Pharmaceutical Co.; 2019.
- Shitara K, Doi T, Dvorkin M, et al. Trifluridine/tipiracil versus placebo in patients with heavily pretreated metastatic gastric cancer (TAGS): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2018;19(11):1437-48.
- Le DT, Uram JN, Wang H, et al. PD-1 blockade in tumors with mismatch-repair deficiency. N Engl J Med. 2015;372(26):2509-20.
- Fuchs CS, Doi T, Jang RW, et al. Safety and efficacy of pembrolizumab monotherapy in patients with previously treated advanced gastric and gastroesophageal junction cancer: phase 2 clinical KEYNOTE-059 trial. JAMA Oncol. 2018;4(5):e180013.
- Muro K, Chung HC, Shankaran V, et al. Pembrolizumab for patients with PD-L1-positive advanced gastric cancer (KEYNOTE-012): a multicentre, open-label, phase 1b trial. Lancet Oncol. 2016;17(6):717-26.
- Shitara K, Özgüroğlu M, Bang YJ, et al; KEYNTOE-061 investigators. Pembrolizumab versus paclitaxel for previously treated, advanced gastric or gastro-oesophageal junction cancer (KEYNOTE-061): a randomised, open-label, controlled, phase 3 trial. Lancet. 2018;392(10142):123-33.
- Tabernero J, Van Cutsem E, Bang, YJ, et al. Pembrolizumab with or without chemotherapy versus chemotherapy for advanced gastric or gastroesophageal junction (G/GEJ) adenocarcinoma: the phase III KEYNOTE-062 study. J Clin Oncol. 2019;37(18_suppl):abstract LBA4007.
- Centers for Disease Control and Prevention. NIOSH list of antineoplastic and other hazardous drugs in healthcare settings, 2016. https://www.cdc.gov/niosh/docs/2016-161/. Accessed August 14, 2019.
- Active ingredient: Trifluridine/tipiracil. RED BOOK Online. Micromedex Healthcare Series [database online]. Greenwood Village, CO: Truven Health Analytics; 2015. https://www.micromedexsolutions.com/micromedex2/librarian/CS/473DB9/ND_PR/evidencexpert/ND_P/evidencexpert/DUPLICATIONSHIELDSYNC/8661C0/ND_PG/evidencexpert/ND_B/evidencexpert/ND_AppProduct/evidencexpert/ND_T/evidencexpert/PFActionId/redbook.ShowProductSearchResults?SearchTerm=LONSURF&searchType=redbookProductName&searchTermId=44148&searchContent=REDBOOK&searchFilterAD=filterADActive&searchFilterRepackager=filterExcludeRepackager&searchPattern=%5Elonsurf. Accessed August 20, 2019.
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Antiemesis. Version 1.2019. https://www.nccn.org/professionals/physician_gls/pdf/antiemesis.pdf. Published February 28, 2019. Accessed September 11, 2019.
Back Top