
Expired activity
Please go to the PowerPak
homepage and select a course.
New Guidelines and Strategies to Manage CVD Residual Risk: Beyond Statin Therapy
What’s New in the 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol
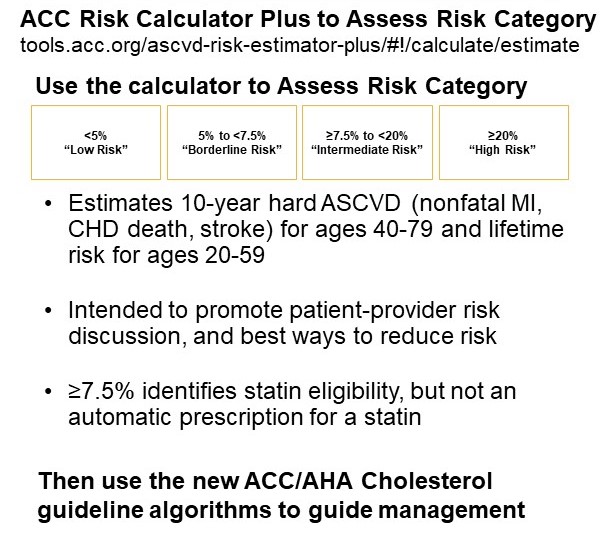
In November, 2018, the American Heart Association, American College of Cardiology, and ten other professional societies released the Guideline on the Management of Blood Cholesterol.1 There are important updates in this guideline starting with risk assessment. While the concept of estimating risk in primary and secondary prevention is not different from the previous guidelines in the clinical setting where one should use a risk assessor or a risk calculator, there are several new categories and changes that more accurately assess risk. The risk calculator mentioned in the Guideline has been recently improved and updated by the ACC and is shown here in Figure 1, ACC Risk Calculator Plus to Assess Risk Category (http://tools.acc.org/ascvd-risk-estimator-plus/#!/calculate/estimate/).2
Figure 1
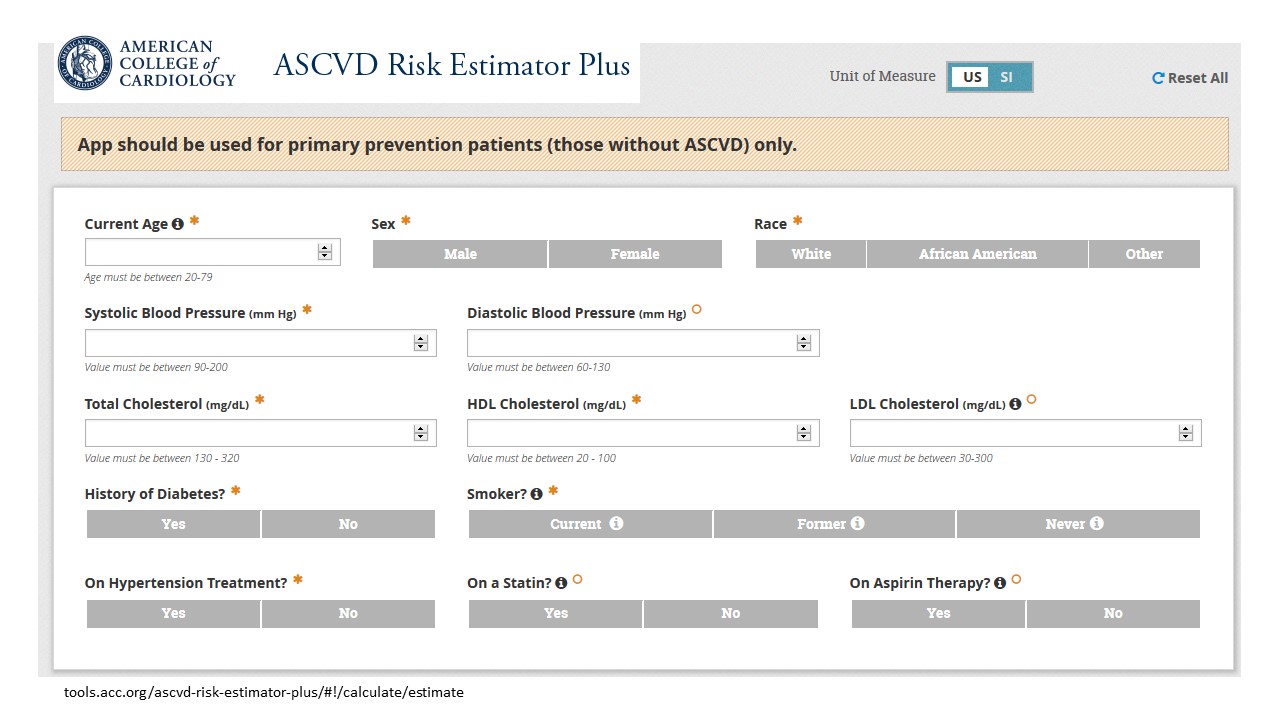
In Figure 1, you see the 13 fields used, including age, sex, race, lipids, blood pressure (whether you’re treated or not), diabetes, smoking, and current therapy. It will estimate a 10-year risk of an atherosclerotic cardiovascular disease (ASCVD) event, a combination of nonfatal myocardial infarction (MI), coronary heart disease (CHD), death or stroke for patients age 40 through 79. With this risk calculator, one can also calculate a lifetime risk, and there is emphasis in the new guidelines on lifetime risk of being untreated and having a high cholesterol for ages between 20 and 39. Unless the patient has an LDL-C>190 mg/dL or diabetes, there is no automatic risk factor requiring a statin prescription, but instead, the Guideline recommends a “Risk Discussion”. There’s more emphasis in the new guideline than previous versions of the guidelines to promote the patient’s involvement in the decision-making process. That involves discussing individual risk status with patients, going over their risk factors and what their 10-year estimated risk is, and have them be part of that thought process in deciding how to manage their risk. Figure 2 shows the four 10-year risk categories, Low, Borderline, Intermediate, and High, which is a ten year risk of an event that exceeds 20%. Intermediate Risk (≥7.5% to <20%) identifies statin eligibility, but as stated before, not an automatic prescription for a statin. Another thing that’s new in the guidelines is that there are now high risk patients can be further subdivided once exceeding a 20% 10-year risk. There are people who have unstable ASCVD with additional uncontrolled risk factors that might put them into an even higher risk category.
Figure 2
Another nice aspect of the guidelines is that there’s a set of recommendations that are called the Top 10 Take-Home Messages. They are also available as slides for free if you’re involved in educating about the new guidelines (https://healthmetrics.heart.org/wp-content/uploads/2018/11/2018-Guideline-on-the-Management-of-Blood-Cholesterol-Executive-Summary-Slide-Set.pdf).
Take-Home Message 1 (Figure 3). For all individuals, we should be emphasizing a heart-healthy lifestyle across the life course, such as diet and exercise. It’s abundantly clear that a healthy lifestyle reduces the risk of heart disease.
Figure 3
Take-Home Message 2 (Figure 4). For patients with clinically diagnosed ASCVD, we should be reducing LDL cholesterol with high-intensity statin therapy, or at least maximally tolerated statin therapy if the patient cannot actually tolerate high-intensity statin therapy.
Figure 4
Take-Home Message 3 (Figure 5). There’s a concession about targets not included in the previous guidelines. I’ve been a clinician through almost every set of guidelines, starting back in the 1980s. The previous set didn’t really focus on lowering LDL to say a target, per se, but now there’s a concession where the more you reduce LDL-C on a statin, the greater will be the subsequent risk reductions.
Figure 5
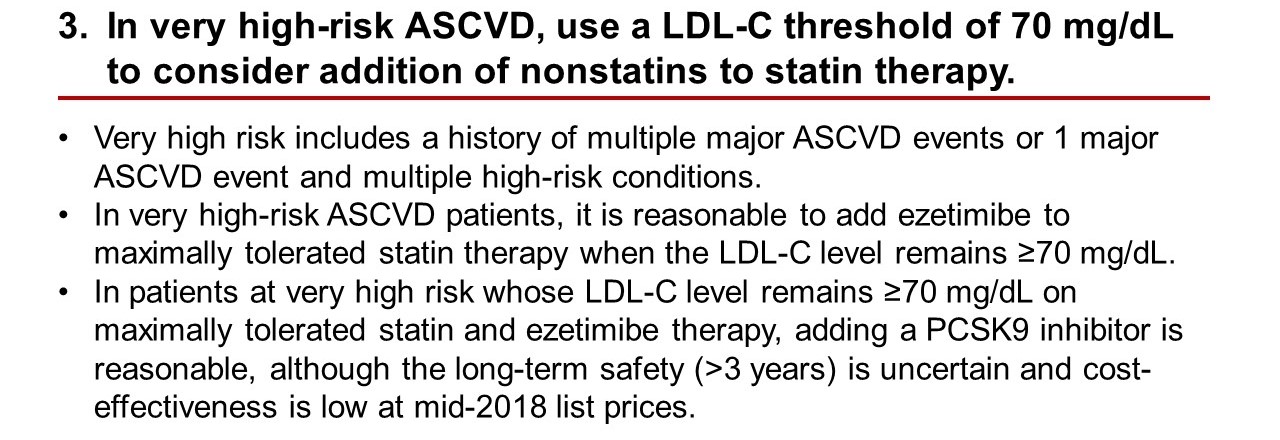
So, there’s a bit of going back to what many of us probably thought beforehand, and the Guideline now recommends maximally tolerated statin therapy should provide an LDL cholesterol reduction target of at least 50%. Now, if you are in the very high risk ASCVD category, the guidelines won’t say that there’s a target for your LDL cholesterol, but if you don’t get below 70 mg/dL, which is now called a threshold, one might want to intensify therapy beyond what the statin therapy alone is doing for you.
Who are these people with very high risk? They have multiple major ASCVD events or they’ve had one ASCVD event and have other multiple high-risk conditions, like they continue to smoke, or they have poorly controlled diabetes. So, if they are very high risk and their LDL remains above 70 mg/dl on maximally tolerated statin therapy, it’s now a recommendation to add ezetimibe. And if adding ezetimibe doesn’t add enough reduction with maximally tolerated statin therapy to below the threshold of 70 mg/dL, then you can now consider adding, a PCSK9 inhibitor. The recognition of additional risk reduction with ezetimibe and the PCSK9 inhibitors is one of the major changes in the guidelines. Although, they do add a caveat, that the long-term safety of greater than three years is uncertain, and the cost effectiveness – at least at mid-2018 list prices – makes it an uncertain option as well. However, we do see periodically that the companies who make the PCSK9 inhibitors continue discussions about a further reduction in pricing, in trying to achieve a more cost-effective price.
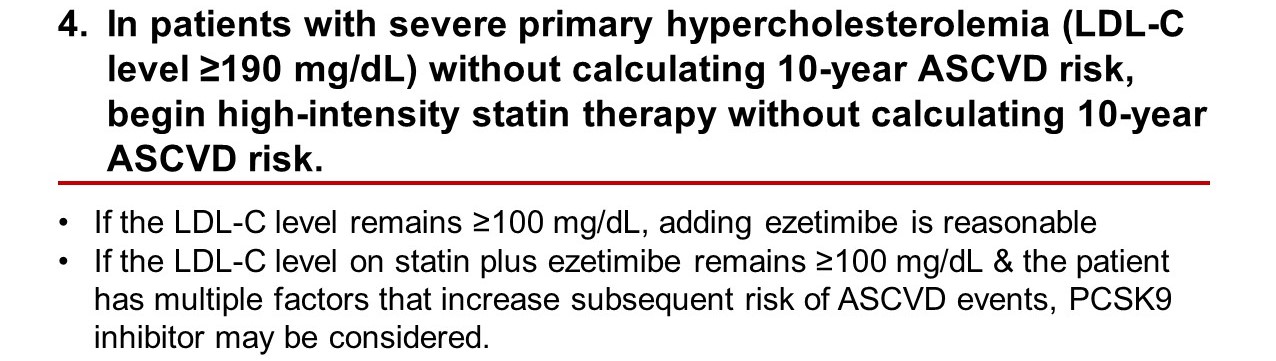
Take-Home Message 4 (Figure 6). These are patients with primary hypercholesterolemia, and an LDL level of ≥190 mg/dL. You can begin high-intensity statin therapy without the need to calculate a 10-year ASCVD risk. Many of these patients probably have heterozygous familial hypercholesterolemia (FH). If after starting high-intensity statin therapy the LDL-C remains above 100 mg/dL, then you can consider ezetimibe, and with the addition of ezetimibe, if LCL-C still remains above 100 mg/dL, then again you can consider the PCSK9 inhibitors with the same caveats about long-term safety and cost effectiveness.
Figure 6
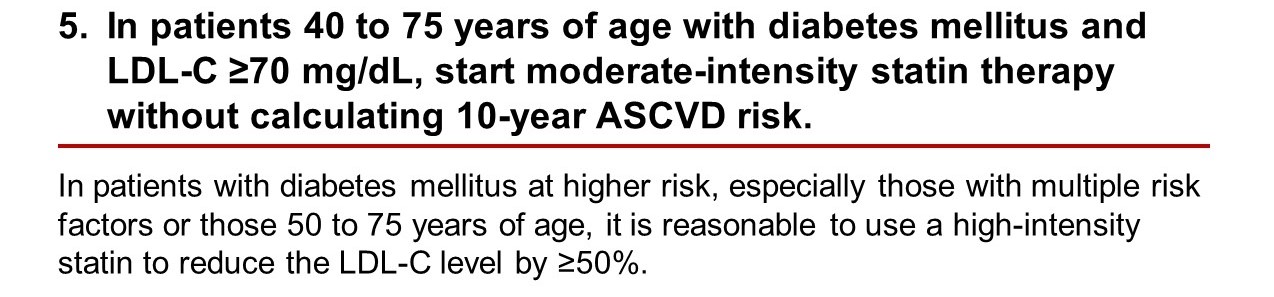
Take-Home Message 5 (Figure 7). In a patient who is 40-75 years of age, who also has diabetes and their LDL is greater than 70 mg/dL, then you can at least start moderate-intensity statin therapy and then evaluate for the presence of additional multiple risk factors, one of which might be that they are at the upper end of that age range – say greater than the age of 50 – then it might be reasonable to use high-intensity statin therapy instead of moderate-intensity statin therapy.
Figure 7
Take-Home Message 6 (Figure 8). Again, we’re in a primary prevention setting of ASCVD events for patients who are age 40-75, then you should be having a clinician/patient discussion about their individual ASCVD risk.
Figure 8
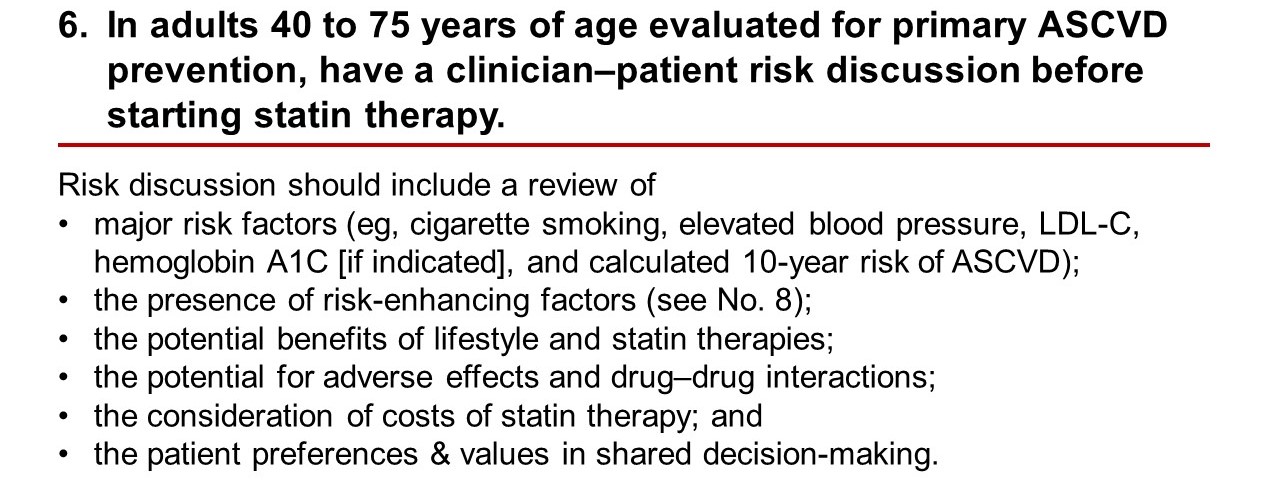
The things that you could consider in that discussion would be their individualized risk factors and their willingness to modify lifestyle, for example, to quit smoking. Other risk-enhancing factors that may be present – those are on Take-Home Message 8. The benefits of lifestyle versus the benefits of statin therapy or both are important to discuss with your patients. This includes the potential for statin-related adverse effects, drug interactions, the cost of statin therapy, and their particular values in the shared decision-making process.
Take-Home Message 7 (Figure 9). Again, if the patient is in the primary prevention setting, 40-75 years, LDL-C is ≥ 70 mg/dL, and they have a 10-year risk ≥7.5%, that puts them into consideration for moderate intensity statin therapy, assuming that the discussion from the previous figure led to a shared decision that the patient is willing to go on statin therapy.
Figure 9
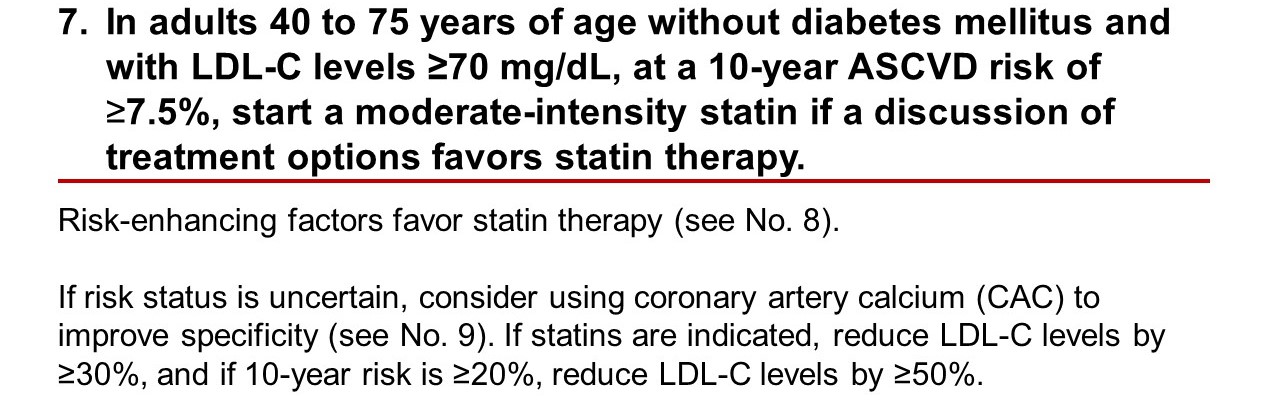
If you are unsure, if the patient is unsure, there’s a new recommendation about using a coronary artery calcium score, or a CAC, to help you in your decision-making process. And this might be one of those additional risk factors assessment tools to consider that was not included in the previous guidelines. You would – if you start moderate-intensity statin therapy – expect to reduce LDL-C by at least 30%. If the decision is to go to high-intensity statin therapy or if the 10-year risk is greater than 20%, then you want to reduce the LDL levels by 50% or more with high-intensity statin therapy.
Take-Home Message 8 (Figure 10). This is the Intermediate Risk category, with an estimated 10-year risk of 7.5 to 19.%. The figure shows the major risk-enhancing factors that you should consider, such as a premature family history of ASCVD, or LDL-C levels that are in the higher end of that range, up to 190 mg/dL, say greater than 160 mg/dL.
Figure 10
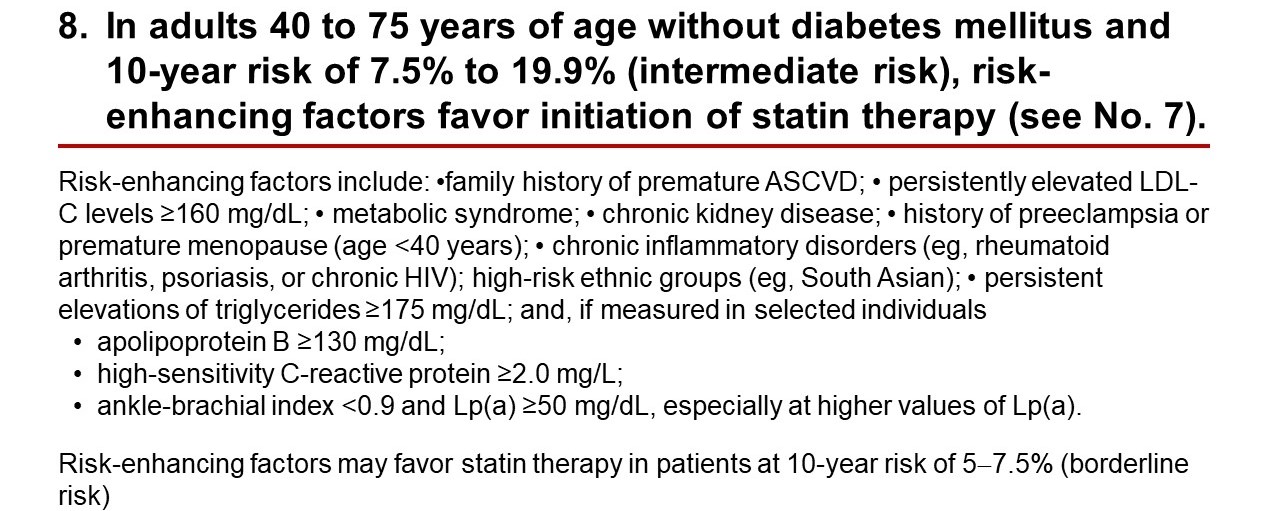
Other factors include presence of metabolic syndrome, chronic kidney disease, history of preeclampsia or premature menopause, chronic inflammatory disorders like arthritis, chronic HIV, other high-risk ethnic groups, and persistent elevations of triglycerides. Others are bullet pointed here – apolipoprotein B greater than 130, an hsCRP of greater than 2 mg/L, an ankle-brachial index of less than 0.9 or an Lp(a) of greater than 50.
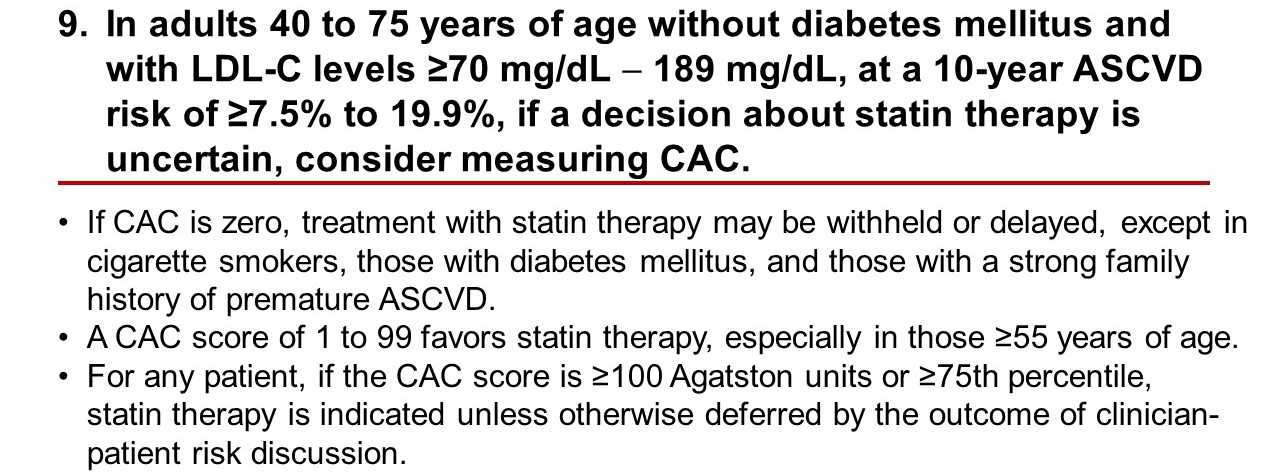
Take Home Message 9 (Figure 11). If you do get a CAC and the score is 0, then you could feel confident about withholding statin therapy or at least delaying it. A CAC score of 1 to 99 would favor statin therapy, particularly in those greater than the age of 55, and then for any patient, if the CAC score is ≥100, which is usually above the 75th percentile, then statin therapy is indicated.
Figure 11
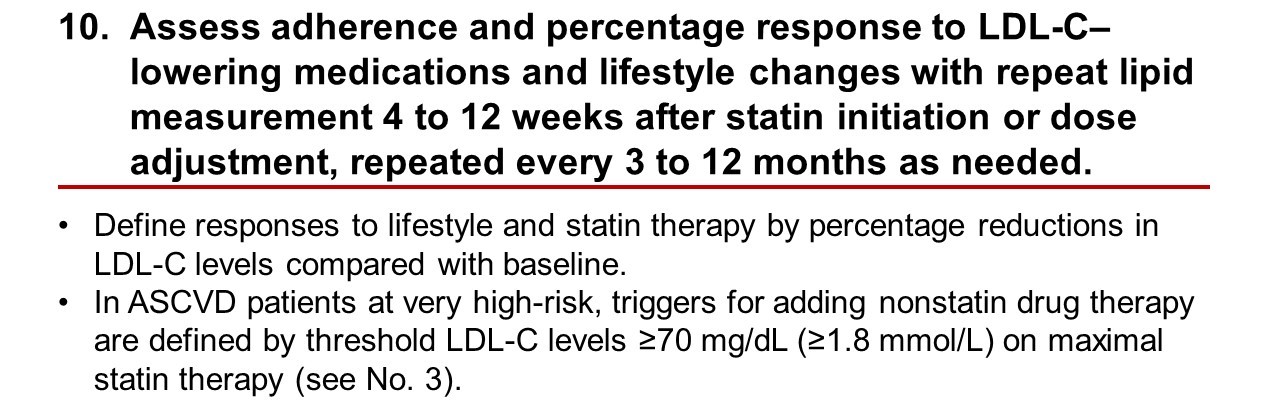
Take-Home Message 10 (Figure 12). In earlier guidelines, there was not a lot of emphasis for starting therapy and then monitoring response to therapy. This Guideline is a little more liberal in suggesting that after you start statin therapy or make a change in therapy or even a lifestyle change, then a repeat lipid panel is indicated 4-12 weeks, and then maybe every 3-12 months afterwards. It’s likely a recognition of what many clinicians were probably doing anyway, despite the previous guidelines not clearly recommending such a follow-up.
Figure 12
Figures 13 and 14 are algorithms from the Guideline. Again, you can download these from the link that was provided to you earlier, and they show the treatment options that were reviewed in the 10 Take-Home Messages. Figure 13 is the primary prevention treatment algorithm. You see the 3 different age groups. Usually you don’t do anything with the teenage and younger group unless they have FH, and then they might be a statin candidate.
Figure 13
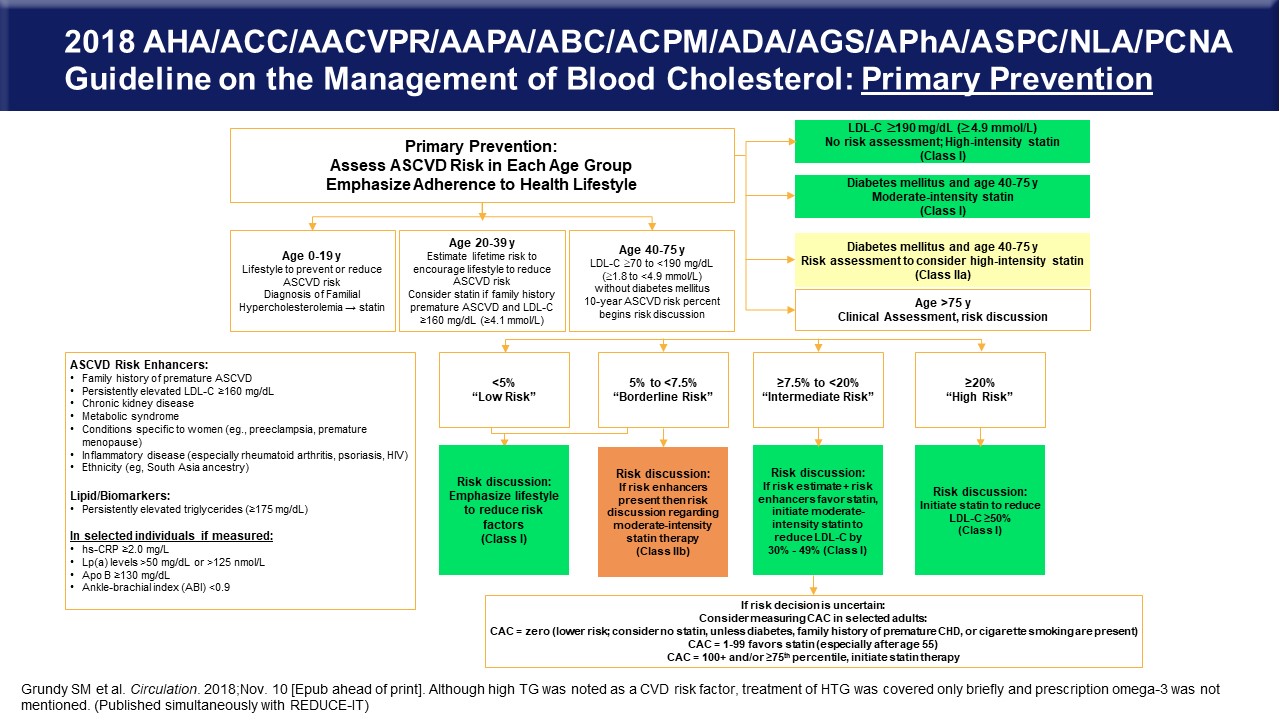
And then for the younger age group, 20-39, one would estimate the risk and maybe consider statin therapy if there’s some other features that concern you about that patient, like a premature family history of ASCVD or LDL-C is greater than 160 mg/dL. And then the usual group that’s going to be recommended for therapy is that age group of 40-75, who has an LDL-C above 70 mg/dL and below 190 mg/dL but without diabetes. The recommendation is to calculate the 10-year ASCVD risk. For those patients with an LDL-C greater than 190 mg/dL, you don’t need to do an assessment, you start high-intensity statin therapy. For patients with diabetes, you’ll start on moderate-intensity statin therapy, unless they have other risk features that would make you consider high-intensity therapy. If patients are greater than the age of 75, then they require clinical assessment and a risk discussion. That’s where, again, because of the increased sensitivity to the recommended drug therapy, the higher likelihood of drugs on board creating drug interaction situations that after your clinical assessment, you might need a risk discussion before you start statin therapy. At the bottom of the Figure are the Low, Borderline, Intermediate, and High-Risk groups with the type of risk discussion shown below them.
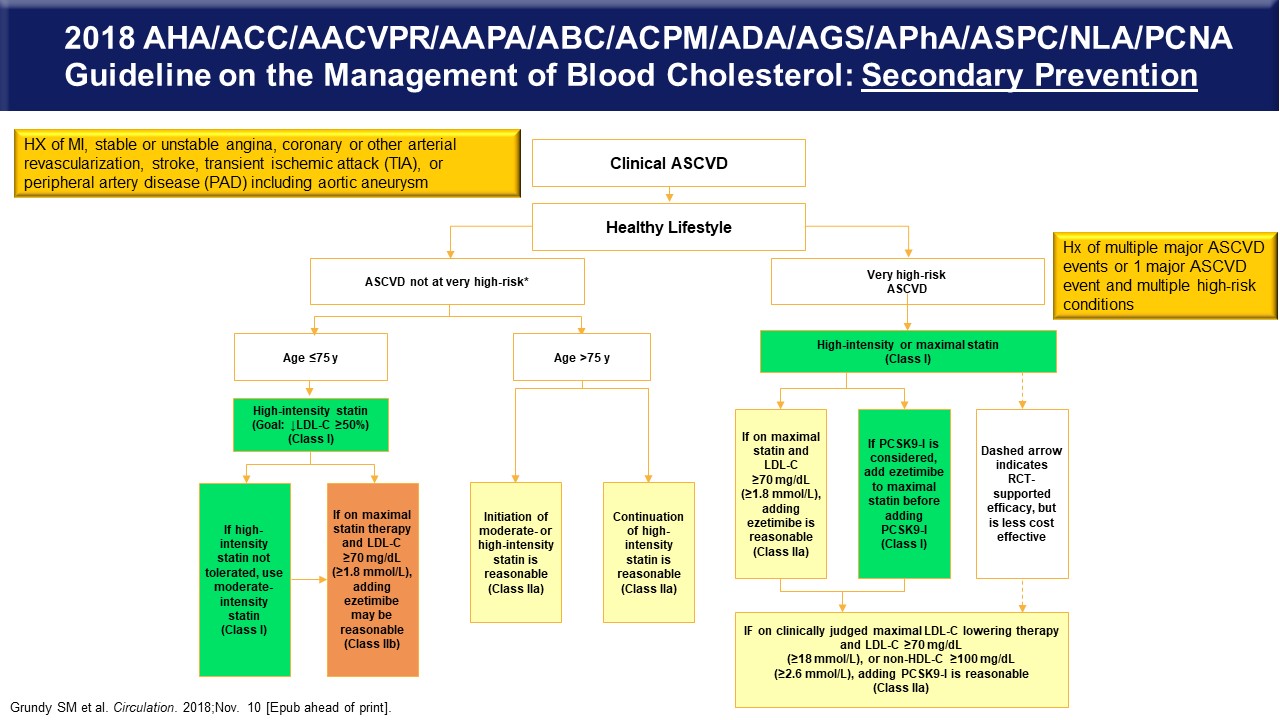
Figure 14 is the algorithm for secondary prevention, those with known ASCVD. If they’re not in the very high-risk category and their age is ≤75, then they should be taking high-intensity statin therapy. Use that threshold value of 70 mg/dL to decide if you’re going to add ezetimibe, and then after ezetimibe use and the patient is still over the threshold value of 70 mg/dL, add a PCSK9 inhibitor. Again, greater than the age of 75 with known ASCVD requires at least moderate, if not high-intensity statin therapy. The very high-risk group should be on high intensity again statin therapy, with the same thresholds of 70 mg/dL for deciding about adding ezetimibe and PCSK9 inhibitors.
Figure 14
Therapeutic Options and Evidence of Adjuncts to Statin Therapy to Reduce Risk
Figure 15 is a reminder that it has been a statin world for at least 25 years across the spectrum of primary and secondary prevention statin trials.3-9 It’s also a reminder that even in statin treated patients, (circled in red) there remains significant risk for subsequent events depending on the patient population and risk status at baseline.
Figure 15
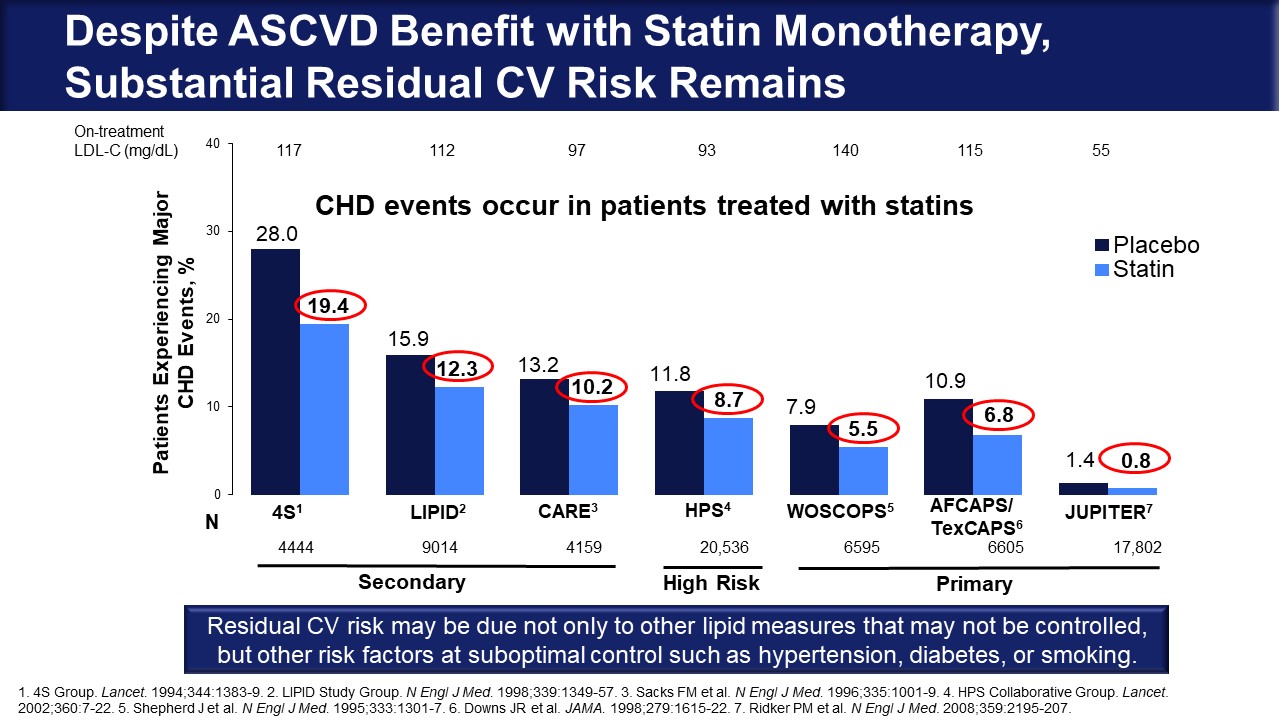
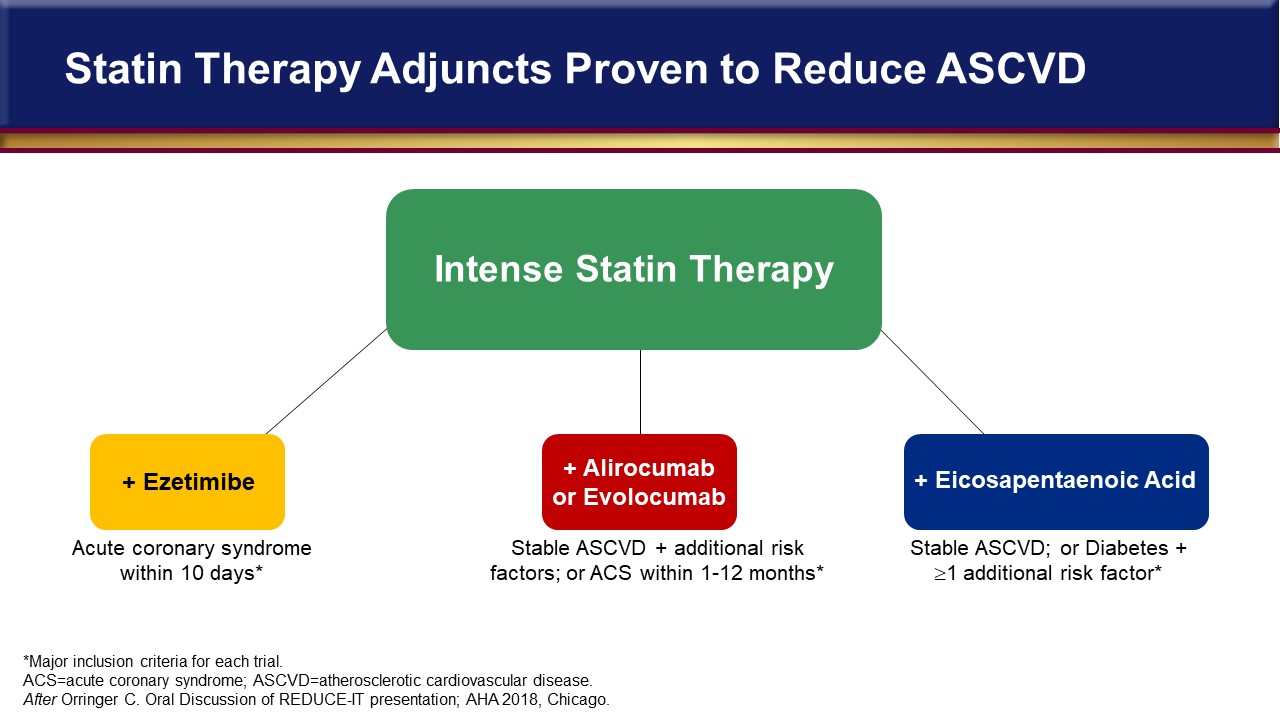
Primary prevention high-risk patients in WOSCOPS had an average LDL-C of 150, and this cohort still had 5.5% annual event rates.7 In secondary prevention, the 4S trial in patients with known ASCVD had a 20% risk of an event in the first year of the trial. These event rates are in statin-treated people and point to the need for more event reduction beyond statin therapy.3 Until recently, we haven’t had a lot of good data about lowering event rates further beyond statin therapy. Figure 16 shows statin therapy adjuncts tested to further reduce ASCVD.10 Outcome trials with ezetimibe and the two PCSK9 inhibitors are completed and published.11-13 Most recently, we have EPA data in an additional outcome trial.14
Figure 16
Let’s review some of these additional therapeutic targets for residual risk in patients who are already optimized on statin therapy by looking at some of the residual risk trials that have been in the literature in the last year and a half. And then, when appropriate, particularly when cost is an issue, we’re going to review some of the cost-effectiveness analyses of those strategies as well.
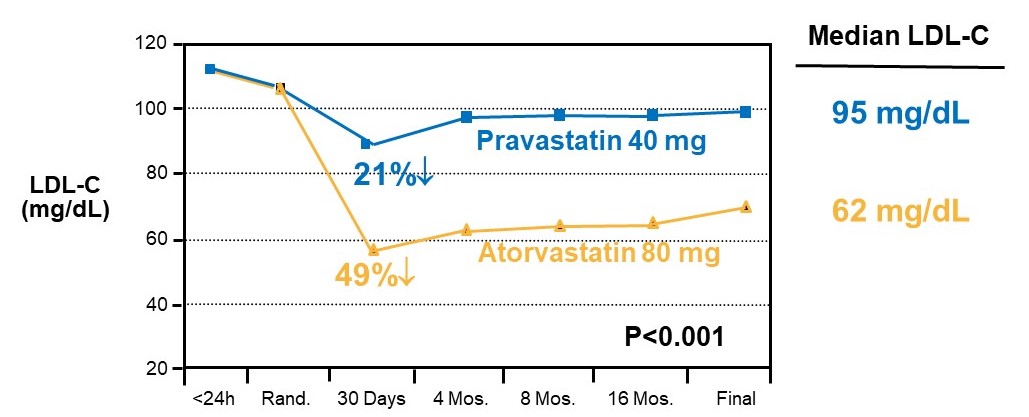
One of the first studies highlighting the concern about residual risk with well-treated statin patients was shown in the PROVE IT trial (Figure 17) which was proof of concept that a more intense statin therapy – in this case, atorvastatin 80 mg – would produce a lower rate of events associated with a lower LDL C than a moderate-intensity statin, pravastatin 40 mg.15
Figure 17
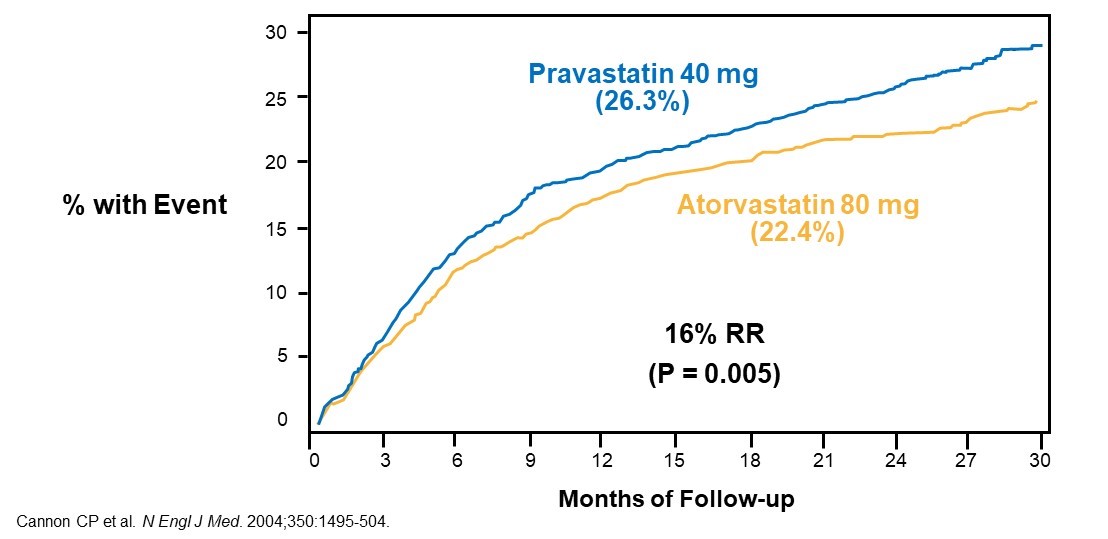
This finding started the notion “lower is better” for LDL-C reduction. Figure 18 shows PROVE-IT Kaplan-Meier curves showing lower event rates with high-intensity atorvastatin therapy, but certainly event rates do not go down to zero. This is the residual risk that cannot be accounted for by even high-intensity statin therapy producing LDL-C levels of 60 mg/dL. And that translates into – as an average two years in the trial – of around 22% repeat cardiovascular events, MI, stroke, and cardiovascular death. And so, these people retain a relatively high risk, despite our best efforts with statin therapy.
Figure 18
Therefore, what are the targets and what can we do after statin therapy? We know that the atherosclerotic process and its progression eventually leads to atherosclerotic plaque rupture and thrombosis, so intensified antithrombotic therapy might be one of the targets. There’s also the contribution of atherogenic lipoproteins that can be LDL, triglycerides and its remnants VLDL, IDL and other remnant particles from VLDL metabolism. And we also know that inflammation plays a role. We’ve long known that inflammation creates an accelerated atherosclerotic process. We see higher rates of CV events in the HIV population as well as in patients with rheumatoid arthritis, and so components of the inflammatory process have become targets for residual risk reduction as well.
Figure 19 provides a review of targets of therapy for reduction in events beyond maximally tolerated statin therapy.
Figure 19
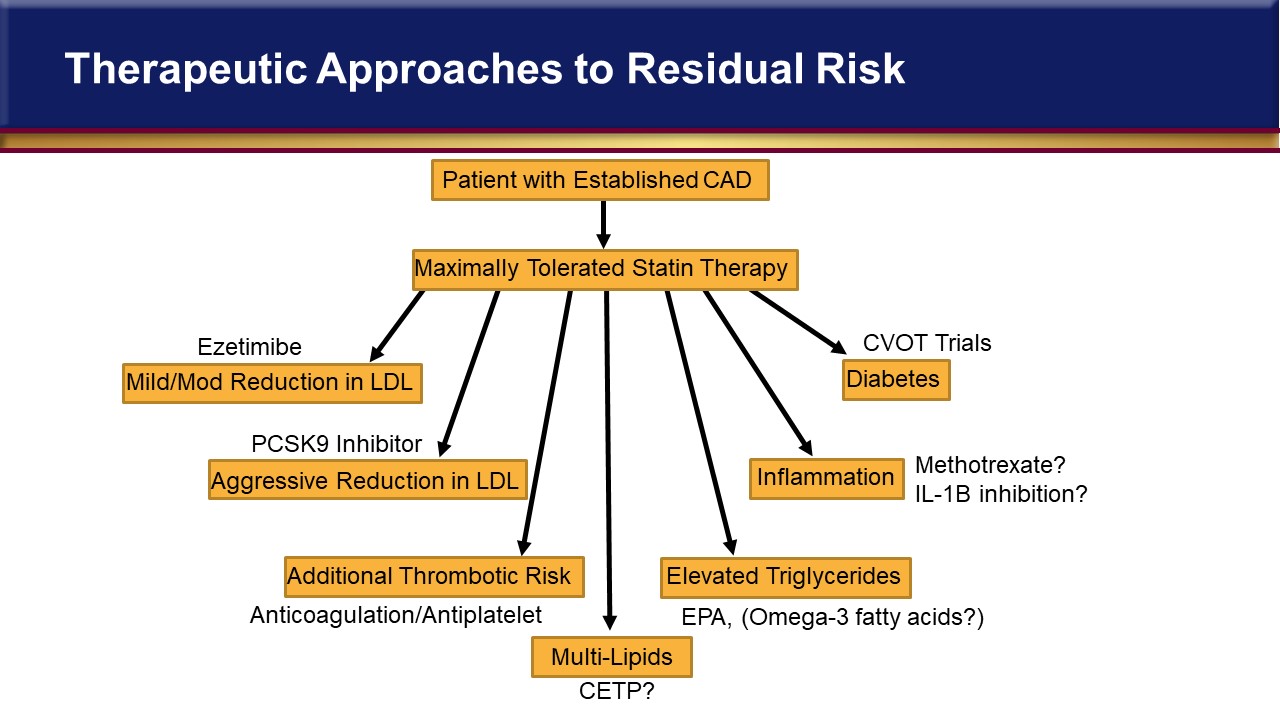
On the left, there is mild-to-moderate LDL reduction with ezetimibe. Below that are the PCSK9 inhibitors, and continuing counterclockwise, additional antithrombotic therapy with either anticoagulation or intensified antiplatelet therapy, multiple lipid targets, EPA based on the REDUCE-IT results, inflammation targets, and then the cardiovascular outcome trials with diabetes drugs that might be additional targets. Most of those trials are in patients with diabetes but some of those drugs are being studied in nondiabetic patients for risk reduction, and so that story may continue to unfold.
As a reminder, Figure 20 describes cholesterol metabolism and transport and where the targets for drug therapy are based on what we know. Dietary cholesterol is blocked by ezetimibe in inhibiting the absorption of dietary cholesterol. Statins block the hepatic cholesterol biosynthesis pathway intracellularly.
Figure 20
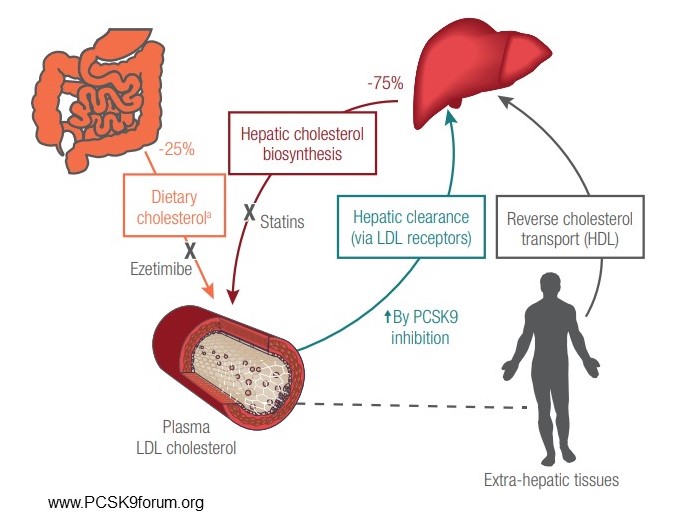
The PCSK9 inhibitors upregulate LDL receptors and increase LDL clearance through those LDL receptors in the liver. And then the concept that’s been sought for a long time of raising HDL is also shown. We know epidemiologically that high HDL seems to be associated with a lower rate of atherosclerotic disease, and so if enhancing HDL or at least its beneficial function is possible, then we might get more reverse cholesterol transport and that could reduce atherosclerotic burden as well.
Figure 21
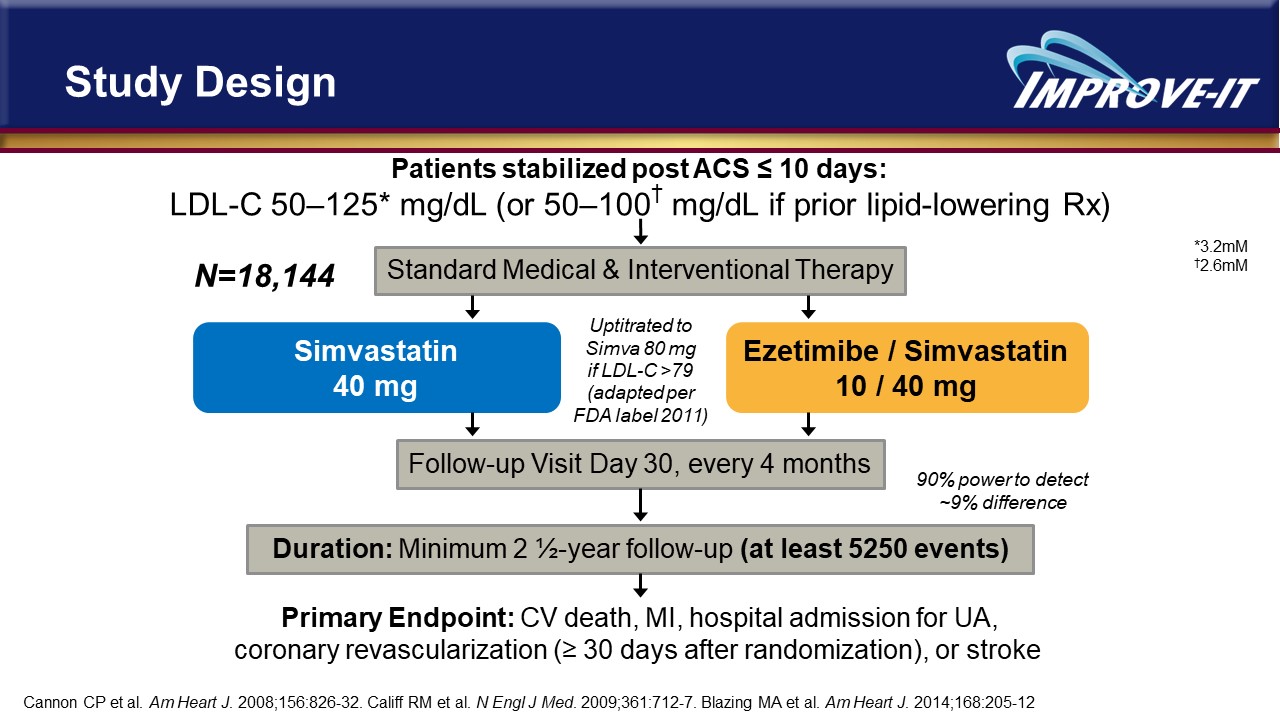
In reviewing these targets beyond statin therapy, the first report was with the use of ezetimibe in the IMPROVE IT trial that enrolled 18,144 post-ACS patients within 10 days of the ACS event. Patients were randomized to moderate-intensity statin therapy with simvastatin 40 mg or ezetimibe 10 mg with simvastatin 40 mg, and then followed for at least 5,250 events (Figure 21).11 This is what we call an event-driven trial and the statistics are all driven on having a long enough follow-up with enough events to make the results clinically and statistically meaningful. Patients were followed for cardiovascular death, MI, a hospital admission for unstable angina, a revascularization procedure, or stroke. The lipid changes are shown in Figure 22.
And as you would expect from what we’ve know with ezetimibe, the absolute reduction in LDL was a little over 16 mg/dL, translating into about a 20% reduction.
Figure 22
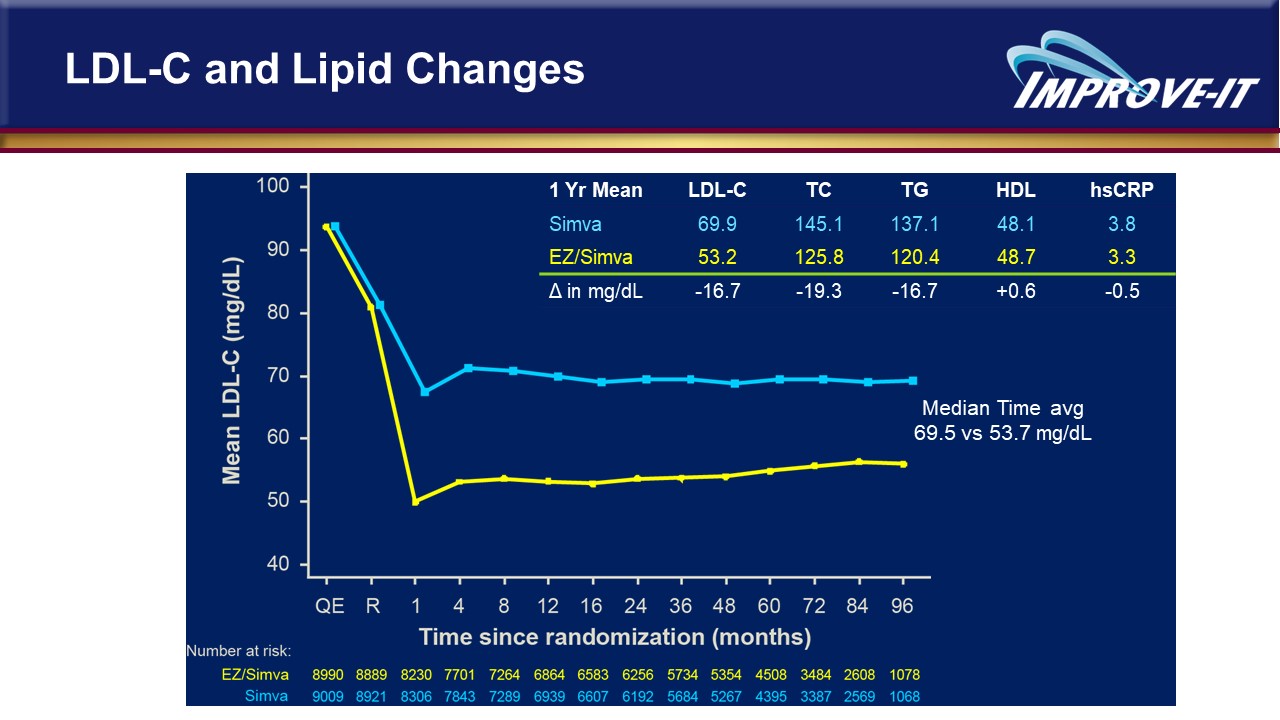
There wasn’t a lot of change in triglycerides, HDL, or hsCRP. Ezetimibe use was associated with a minor but statistically significant 6.4% relative risk reduction in cardiovascular events that took 7 years to complete (Figure 23).
Figure 23
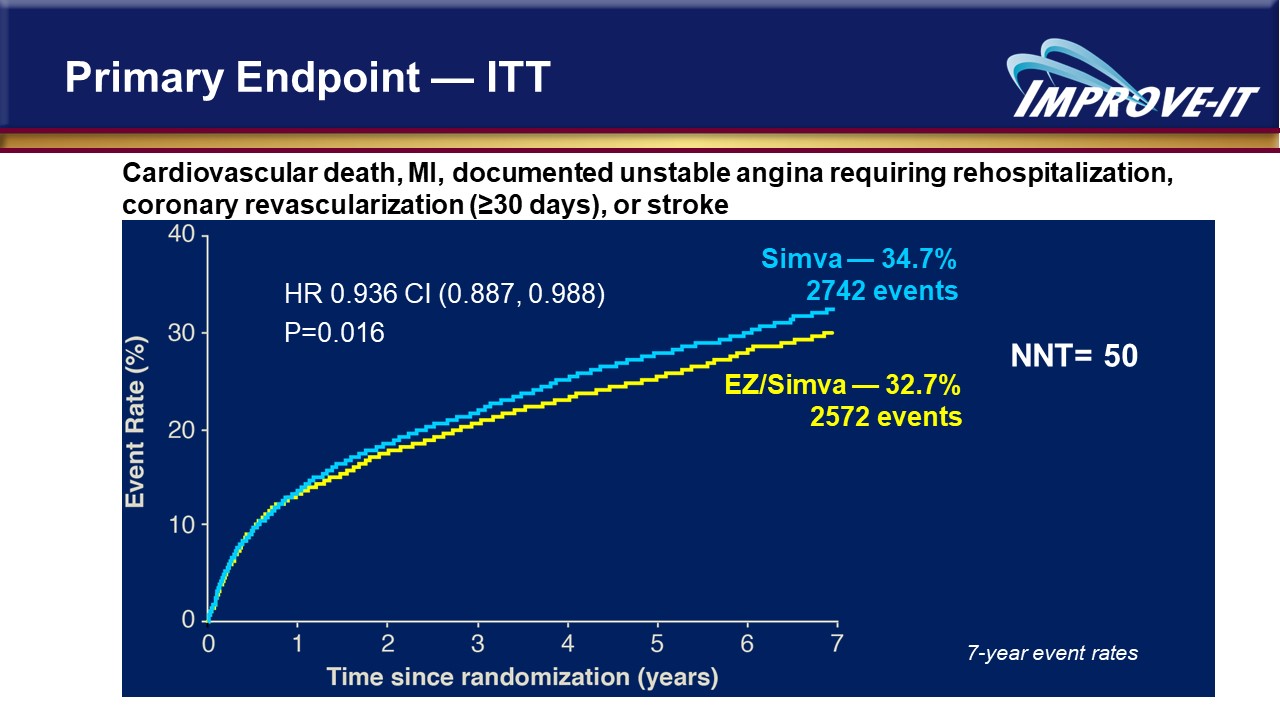
So, the fact that this is recommended before more aggressive therapy with PCSK9 inhibitors is somewhat controversial depending on where your baseline LDL-C is after statin therapy. But, nevertheless, considering ezetimibe before PCSK9 inhibitors is in the Guideline. There was an absolute risk reduction of 2%, which gives you a number needed to treat of about 50. Now, interestingly, when the sponsor for ezetimibe took this to the FDA to get an FDA indication based on this trial, the FDA did not grant them an indication. So, event reduction is not an FDA-approved indication for this drug, even though it’s recommended in the Guideline. The FDA did give it the indication for reduction of elevated total-C and LDL-C levels.
Figure 24
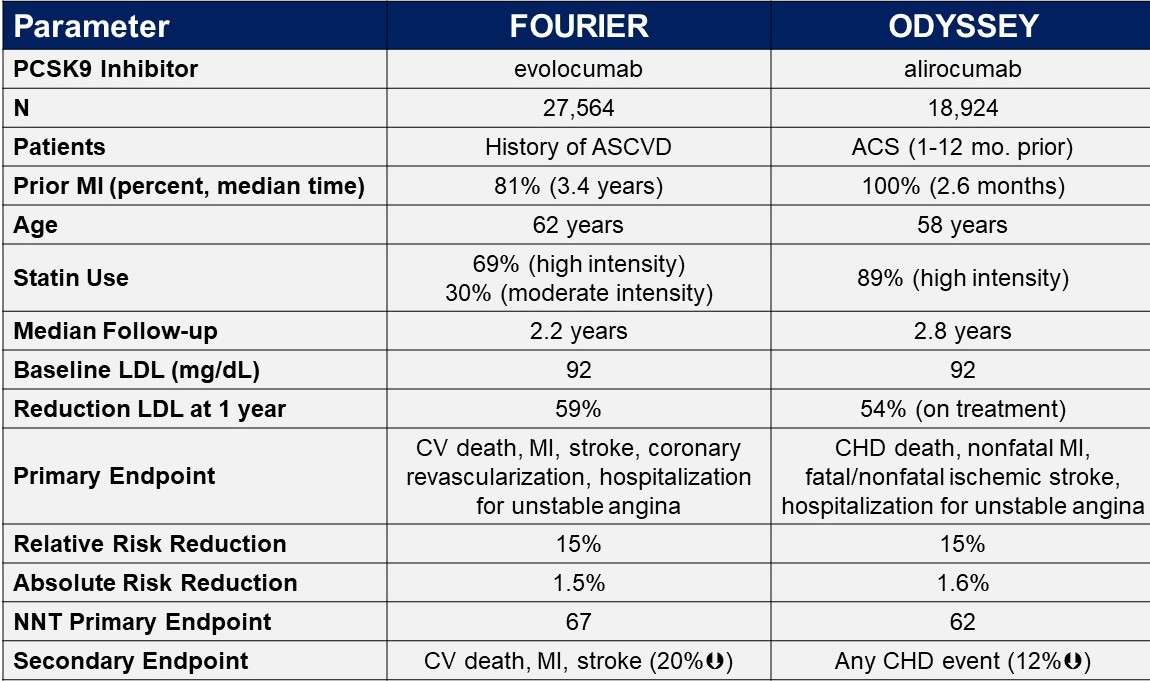
The PCSK9-inhibitor story for patients who need a more intense LDL-C lowering beyond statin therapy is an interesting one. The search for a drug that would block PCSK9 came from genetic studies showing that people who had a loss-of-function gene for the PCSK9 protein was had low LDL-C and protection against cardiovascular disease.16,17 Some of these people with loss-of-function PCSK9 had LDL-Cs of 14, 21, 30, and so a target of therapy then became PCSK9, and drugs consisting of antibodies against PCSK9 were developed. We now have two outcome trials – the one with evolocumab is FOURIER; the one with alirocumab is ODYSSEY OUTCOMES.12-13 They have some similarities and differences, shown in Figure 24. The numbers of patients in these trials are huge – 27,564 in FOURIER and 18,924 in ODYSSEY. The ODYSSEY patients were perceived to be at higher risk because they had a recent ACS that, on average, occurred 2.6 months prior to being into the trial. 81% of the FOURIER patients had a history of MI that was, on average, three years previous to randomization, so they were perceived as being a little bit more stable patient population. Ages were similar – late 50s/early 60s. There was a little more high-intensity statin therapy in the ODYSSEY trial. FOURIER was somewhat criticized for not being a very long follow up, although ODYSSEY was only six months longer. Baseline LDLs for both were in the low 90s. LDL reduction was similar between these two antibodies that both have a very similar mechanism of action. The primary endpoints are similar although FOURIER had an additional endpoint of hospitalization for unstable angina that ODYSSEY didn’t have, but despite those subtle differences, they both had a relative risk reduction of 15% with an absolute risk reduction of 1.5-1.6%, and a number needed to treat into the 60s, so I don’t think there’s a lot of difference in performance between these two drugs. Figure 25 shows the Kaplan-Meier curves and one can see the curves start splitting at about a year.
Figure 25
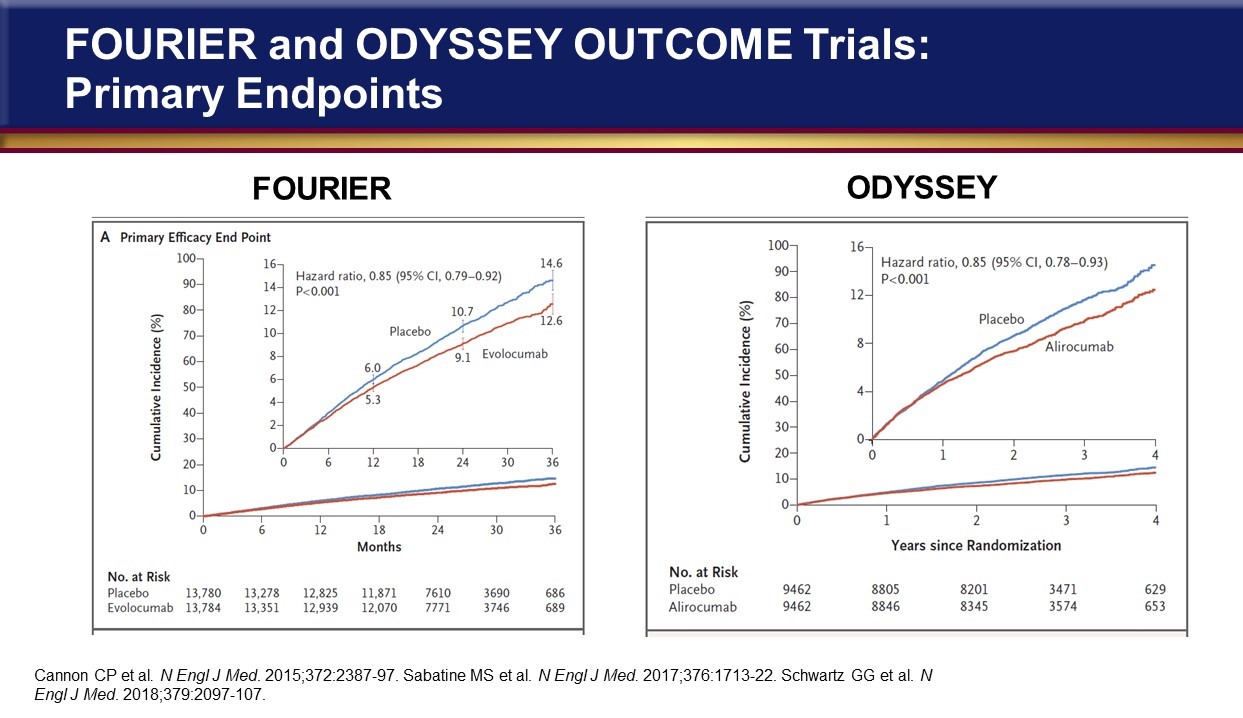
Figure 26
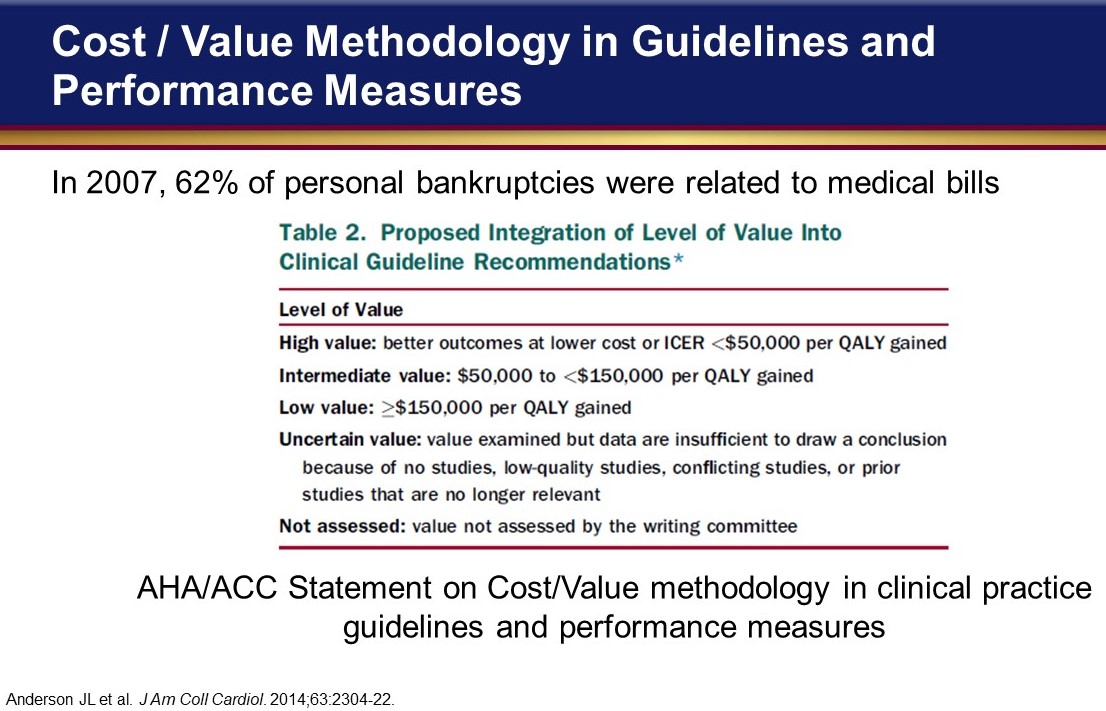
What’s concerning is their cost effectiveness and in recognition of the impact of medical bills in this country – in fact, in Figure 26, we see that well over half of personal bankruptcies were related to medical bills, and so the American Heart Association put out a statement a few years ago about the importance of evaluating cost effectiveness with cardiovascular therapies.18
Figure 27
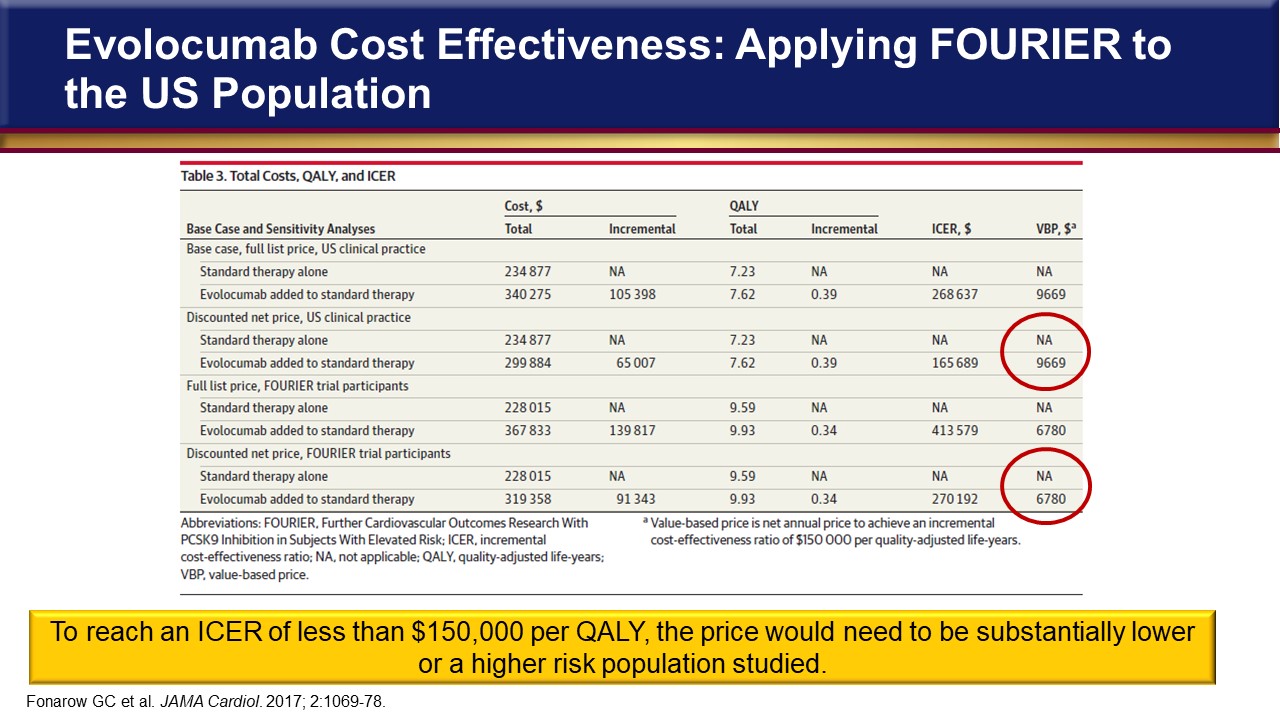
The figure shows that the term high value is when the incremental cost-effective ratio is less than $50,000 per Quality of Life Year (QALY) gained. Intermediate value is when the cost-effective ratio is between $50,000 and $150,000, and low value if it’s more than $150,000 per QALY gained. This is a yardstick measure that is used when reviewing some of the cost-effective studies from the PCSK9 inhibitor trials. There’s a lot of data in Figure 27 but the principle finding is in the last column where the circles highlight what the cost would need to be of the PCSK9 inhibitor evolocumab to produce $150,000 per QALY gained.19
Figure 28
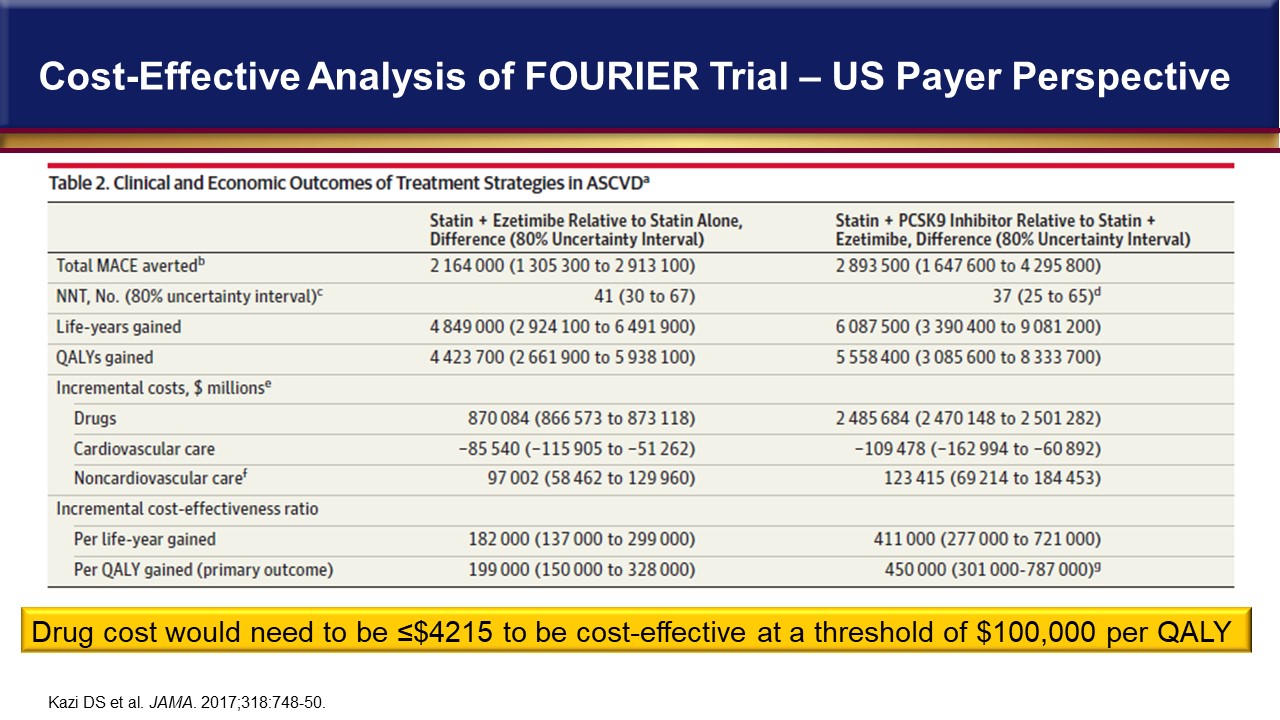
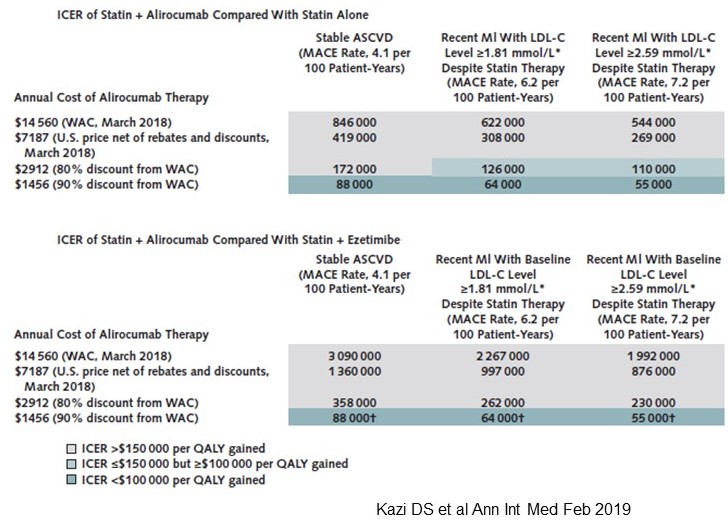
So, for the broad-based US clinical practice type of patients, the cost-effective threshold is just under $10,000, and if it was based on the FOURIER trial patient population, which was a more limited, restrictive criteria for entry into the trial, it would still have to be $6,700 and that’s just to reach that barely acceptable $150,000 cost per QALY. So obviously the cost of the drugs is going to have to be a lot lower than that. Figure 28 is from another study that used $100,000 per QALY as a threshold for cost-effectiveness and found that the cost of a PCSK9 inhibitor would need to be about $4,000 to reach that threshold.20 And then the ODYSSEY trial just had a cost-effective paper published recently and is shown in Figure 29.21 The top half of the figure is for alirocumab + statin vs statin alone, while the bottom half is for statin + alirocumab compared with statin + ezetimibe. The legend indicates that the darkest blue colored rows are for <$100,000 per QALY gained. Looking at the bottom portion for <$100,000 we can see the cost of $88,000, $64,000, $55,000 is based on a discount of 90% from the average wholesale price for different ASCVD states, respectively. So, these drugs need to be markedly lower, no more than $3,000 a year to really reach acceptable QALY dollar values. And, again, the companies continue with some price reductions and keep talking about reducing the prices further.
Figure 29
What about trials focusing on other lipid targets? Lower triglycerides with a drug and you typically raise HDL. That’s usually what we think of with fibrates and niacin. There are four fibrate trials of interest, there’s a few more, but the two that are most relevant because they involve statin therapy are the fenofibrate trials with FIELD22 and ACCORD,23 and these two trials are highlighted in Figure 30.
Figure 30
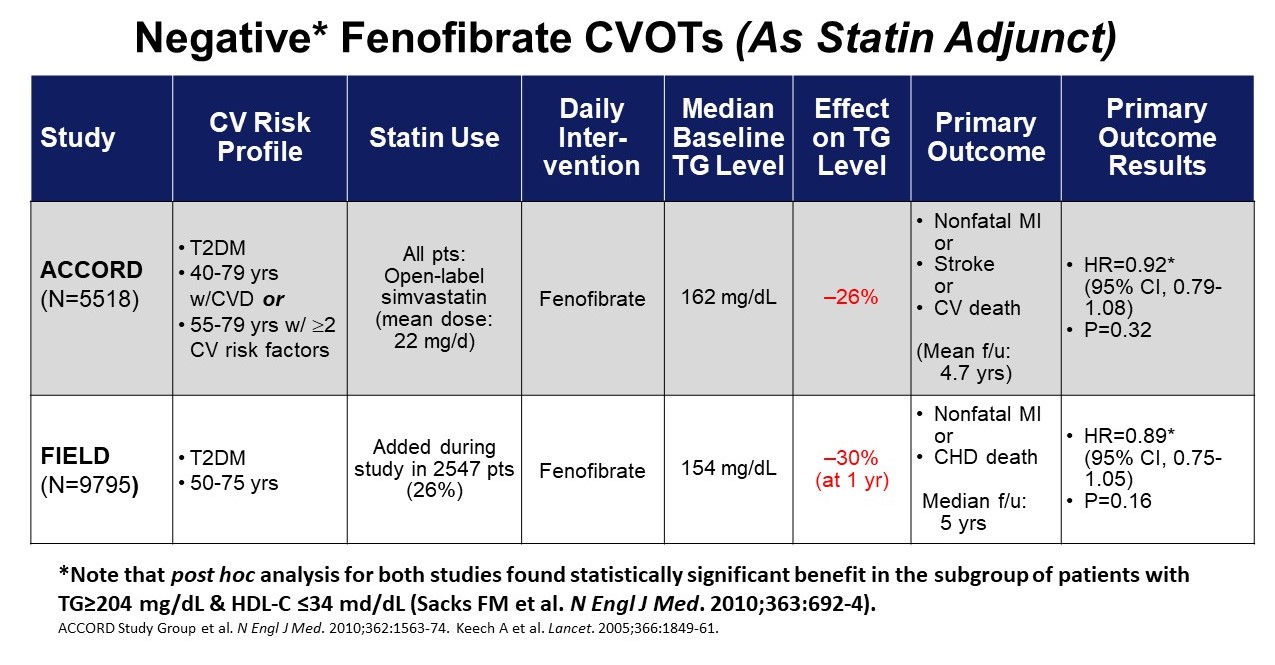
They were both done in patients with type 2 diabetes. Unfortunately, the average triglycerides in these trials wasn’t very high. So, these weren’t people who, on average, were hypertriglyceridemic at all. Nevertheless, a 30% or so reduction in triglyceride levels with fenofibrate on top of statin therapy was not associated with a significant clinical benefit. Based on these results, we really don’t consider adding fenofibrate for triglyceride reduction to reduce events.
Figure 31
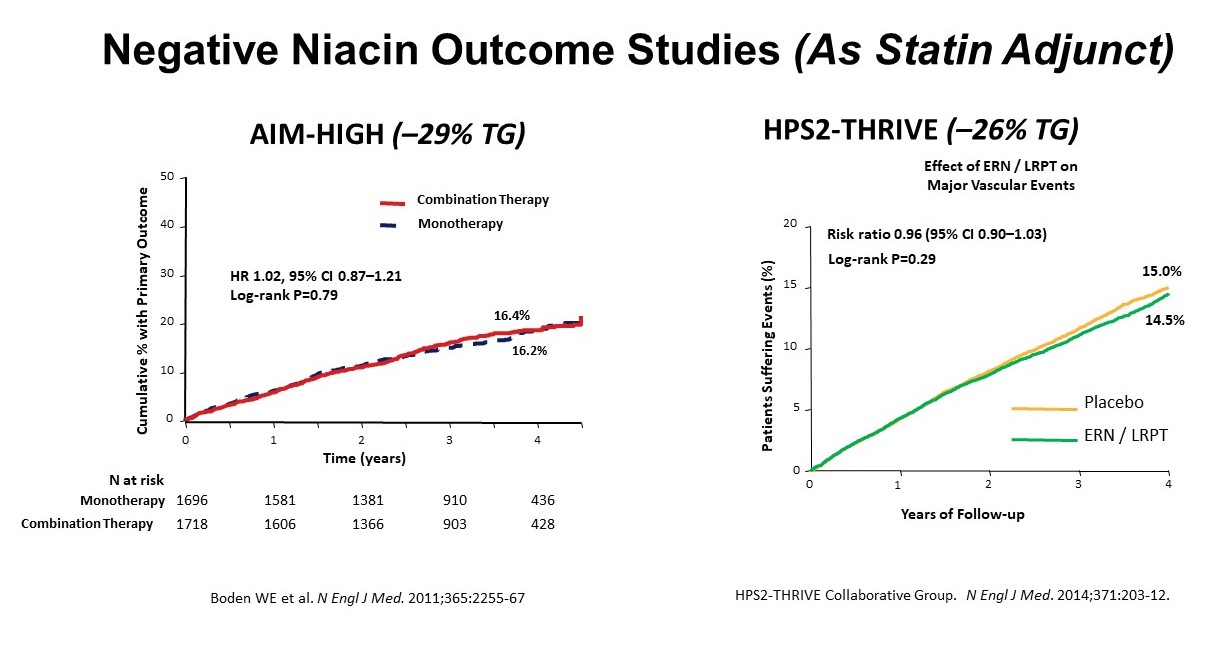
Figure 31 shows two niacin trials that were even more bleak looking. The AIM HIGH24 and the HPS2-THRIVE 25 trial with 29 and 26% reductions in triglyceride in niacin therapy, respectively, showed no benefit over the course of four years. And so, adding niacin to statin therapy is really of no benefit as well. Now, what about targeting HDL? We’ve long been targeting raising HDL, particularly with the statin/niacin trials where niacin raised HDL levels even though it did not show a benefit. The drug category that’s gotten the most attention over the last 10 years or so was the cholesteryl ester transfer protein (CETP) inhibitors. There were some earlier trials with dalcetrapib and evacetrapib that were negative. The first trial conducted was with torcetrapib, which was not only negative, it was harmful and actually killed more people than placebo in a post-MI setting, despite increases in HDL-C of 100%. So the mechanism by which these drugs raise HDL-C may not be producing a functional HDL to increase reverse cholesterol transport as expected.
Figure 32
A recent trial with anacetrapib reported out (Figures 32and 33) and it showed an HDL-C increase of 104%, so HDL-Cs doubled.26 Non-HDL-C levels went down 8% and directly measured LDL-C levels went down 41%, and yet, over the four years of the trial, there was still only a 9% reduction in cardiovascular events.
Figure 33
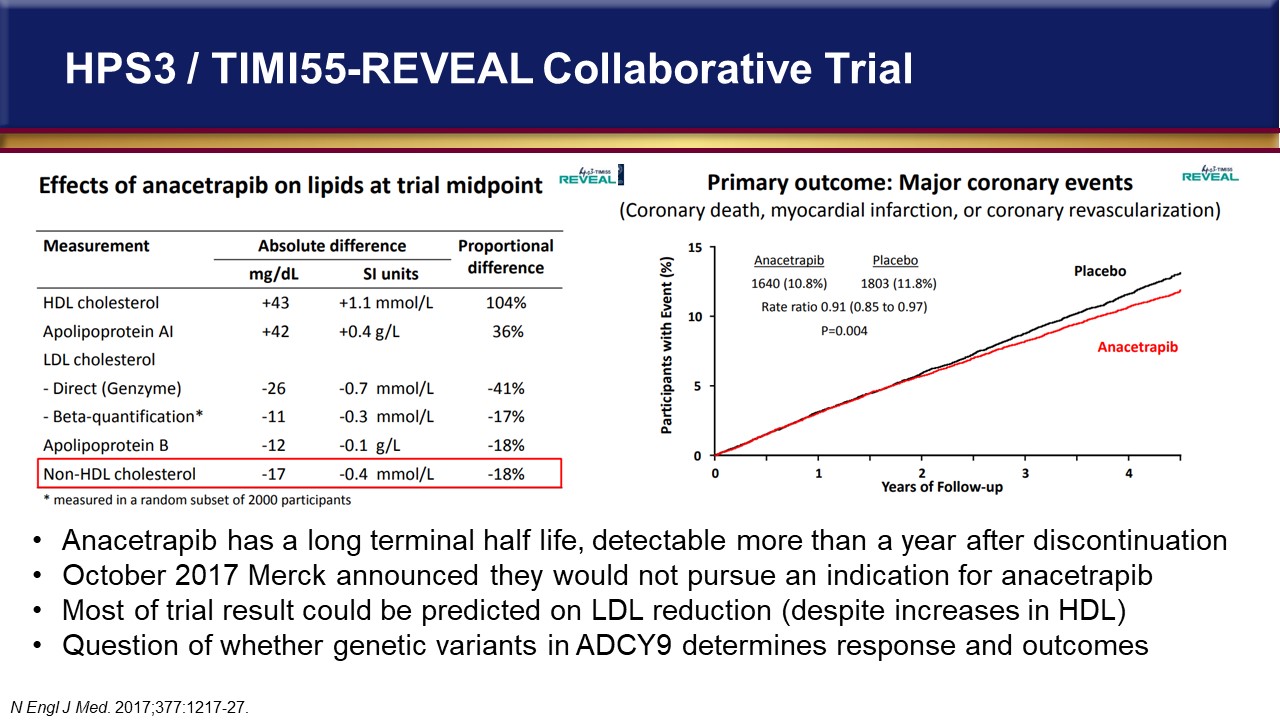
So, despite doubling HDL-C, it didn’t really alter outcomes much. In fact, most of the trial results could be predicted based on the LDL-C reduction, if you look at the relationship between LDL-C and events, despite this increase in HDL-C. In fact, within 2 or 3 months after this trial came out, Merck announced that they were not going to pursue an indication or market anacetrapib. Interestingly, in the area of pharmacogenomics, the study had an interesting finding for those who have a genetic deficit in a gene called ADCY9, which encodes for adenylate cyclase type 9 that is involved in ATP metabolism. If you were deficient in ADCY9 and got anacetrapib, you had a 40% reduction in events. So, it would have been nice from a pharmacogenetics standpoint to use a CETP inhibitor drug targeting those that were genetically deficient in this gene. Unfortunately, we won’t get that opportunity.
Figure 34
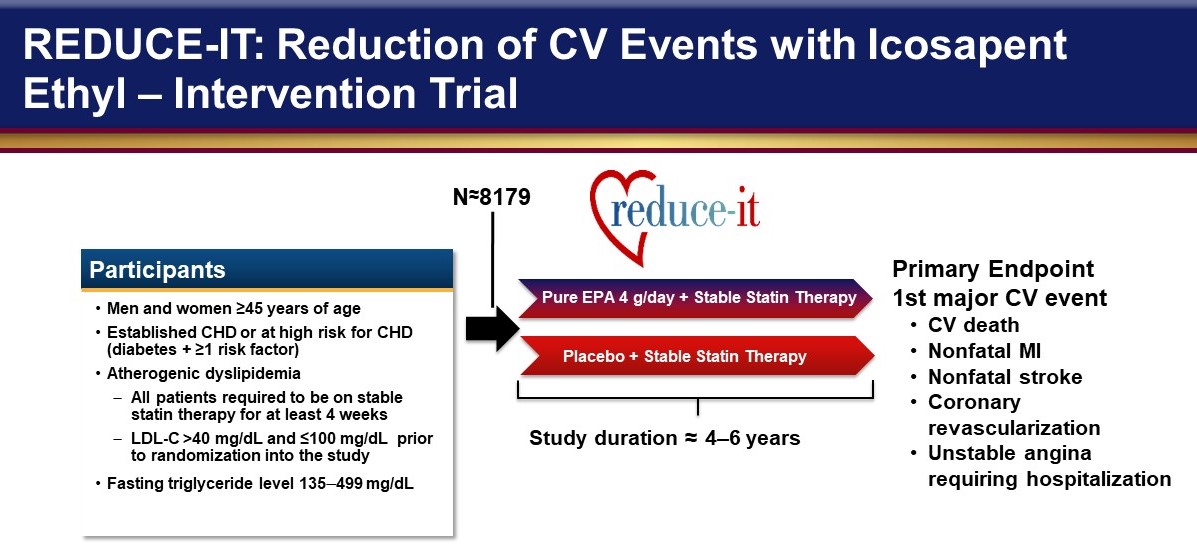
Targeting triglycerides with icosapent ethyl has recently shown great success based on the results of REDUCE-IT (Figure 34).14 It was a study of individuals that either were secondary prevention, which was about 70% of the population, or primary prevention, which they capped at 30%. So, primary prevention patients had to have a history of diabetes with additional risk factors. These were all well-controlled patients in terms that they had to be on stable statin therapy, LDL-C levels between 40 and less than 100 mg/dL, and then fasting triglyceride levels that were 135 mg/dL up to less than 500 mg/dL. Ultimately, the median triglyceride level at inclusion into this trial was about 220 mg/dL. They followed these patients for 5 years who were on statin therapy, and EPA at 4 gm/BID or placebo. The primary composite endpoint was a 5-point outcome. The key secondary endpoint, CV death, MI, and stroke, was what most of us are probably more familiar with. In both endpoints (Figure 35), there was a statistically significant reduction with the use of the EPA-only omega 3 fatty acid. So, for the primary endpoint, we can see that the absolute reduction was 4.8% and the relative risk reduction was almost 25%. The number needed to treat was 21. When you look at the triple endpoint, the absolute risk reduction was a little bit less, 3.6%, but the relative risk reduction was 26.5% and the number needed to treat was 28. This was very surprising to a lot of people in not only the lipid but cardiovascular arenas in terms of the magnitude of benefit with the pure EPA product at a 4gm/day dose since so many other omega-3 studies using different formulations and lower doses were negative trials.
Figure 35
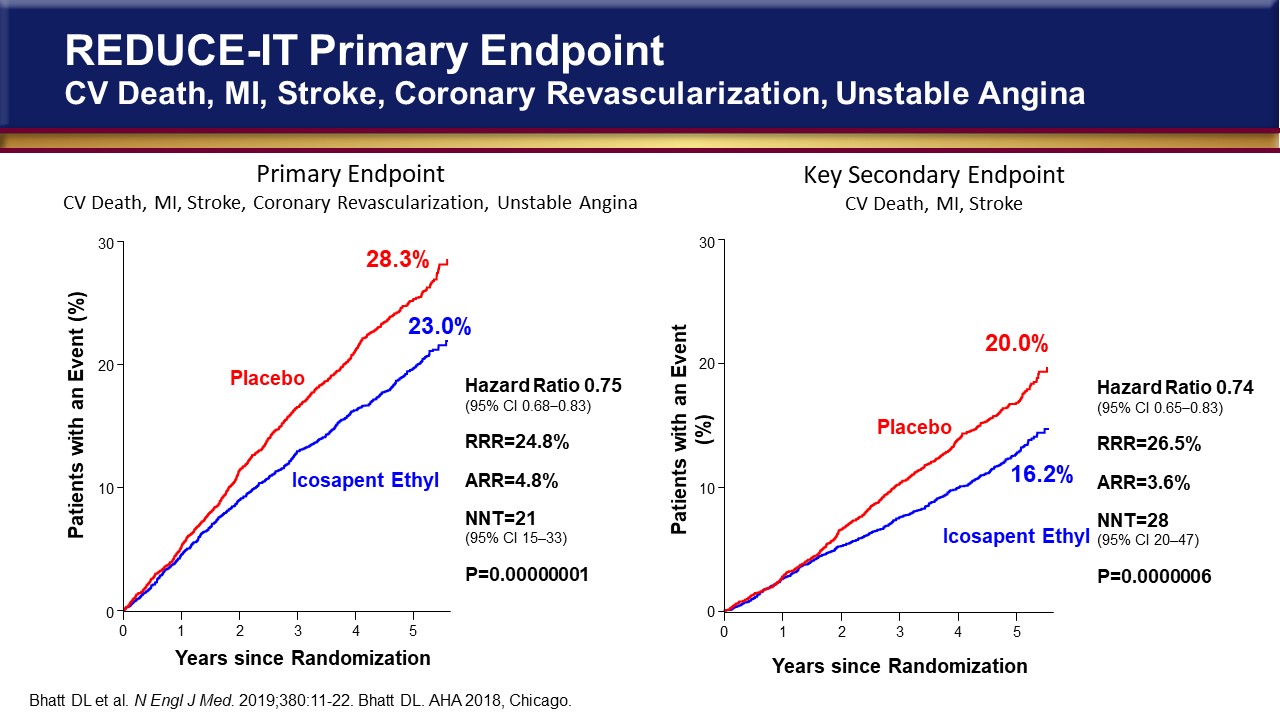
Also, the magnitude of benefit seen was much higher than other lipid-lowering trials such as IMPROVE-IT, FOURIER, and ODYSSEY, this these are remarkable results. Interestingly, the Guideline on Blood Cholesterol was published at the same time that the REDUCE-IT trial results became available, so there’s no mention of REDUCE-IT. There is however, a recommendation that hypertriglyceridemia, fasting or nonfasting triglycerides 175 to 499 mg/dL, should be addressed and treated with lifestyle factors, secondary factors such as diabetes, and medications that increase triglycerides, and in those with ASCVD risk >7.5%, to consider a persistently elevated triglyceride level as a factor favoring initiation or intensification of statin therapy.
Figure 36
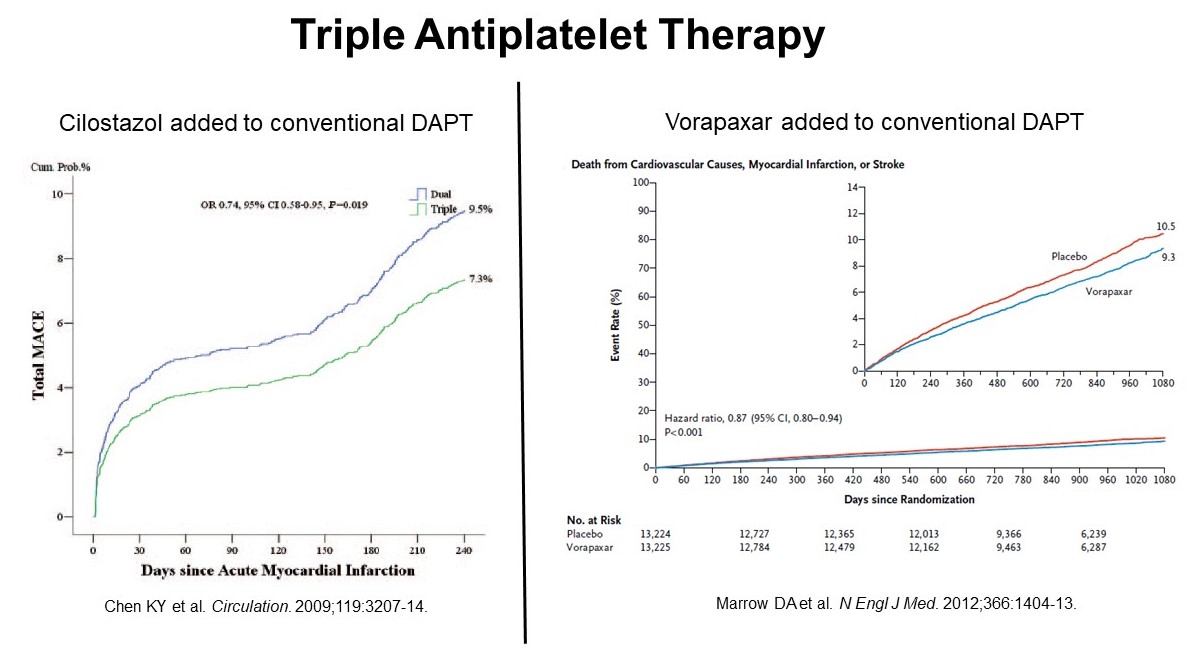
What about antithrombotic approaches? There have been trials looking at triple antiplatelet therapy to intensify our usual double antiplatelet therapy. Adding cilostazol to a P2Y12 inhibitor and aspirin actually showed benefit (Figure 36, left panel).27 Unfortunately, this is a little bit of an older trial and it was retrospective. And there are some other small studies that show similar results, but usually the benefit is offset by increased bleeding risk and so you don’t see these drugs being used in triple therapy very often, if at all. There’s a PAR-1 antagonist called vorapaxar that antagonizes the thrombin receptor on a platelet, which is perhaps the most powerful stimulant for platelet activation.28 And there was a small benefit with vorapaxar when added to the usual double antiplatelet regimen (Figure 36, right panel). Unfortunately, the bleeding risk went up and so the balance between the clinical benefit versus the negative effects of the bleeding doesn’t make this a very attractive strategy.
Figure 37
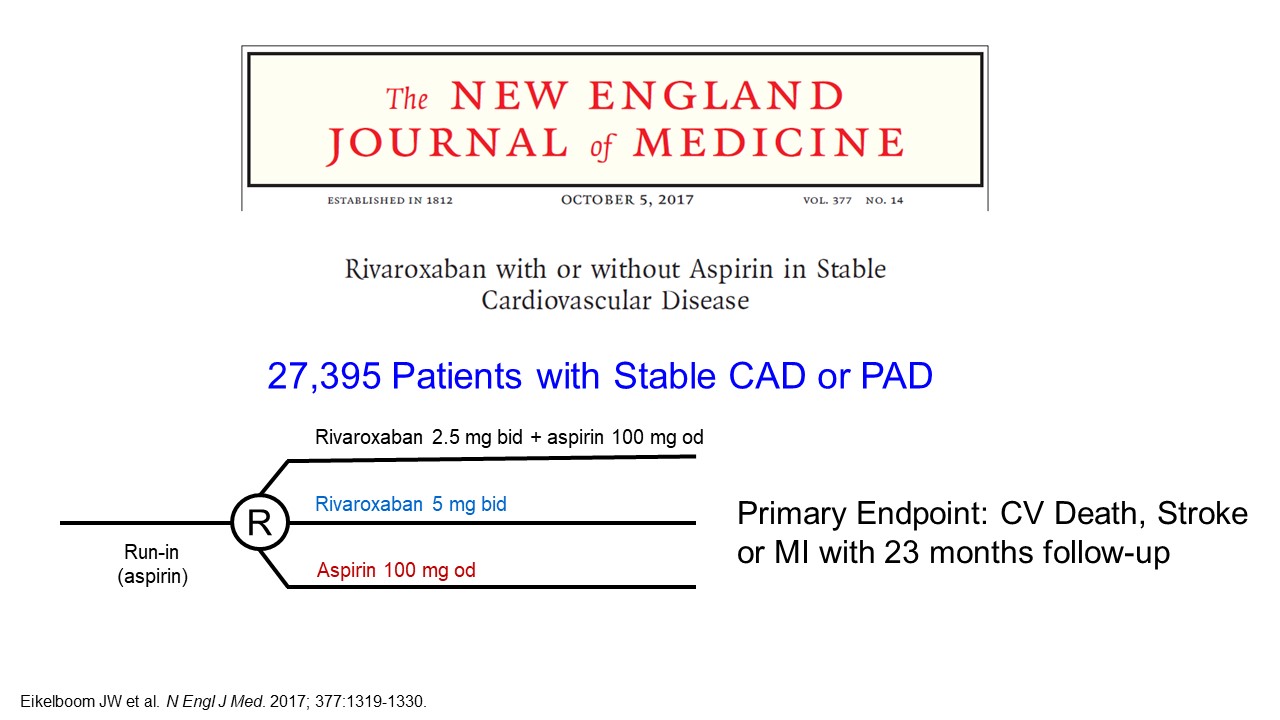
Figure 38
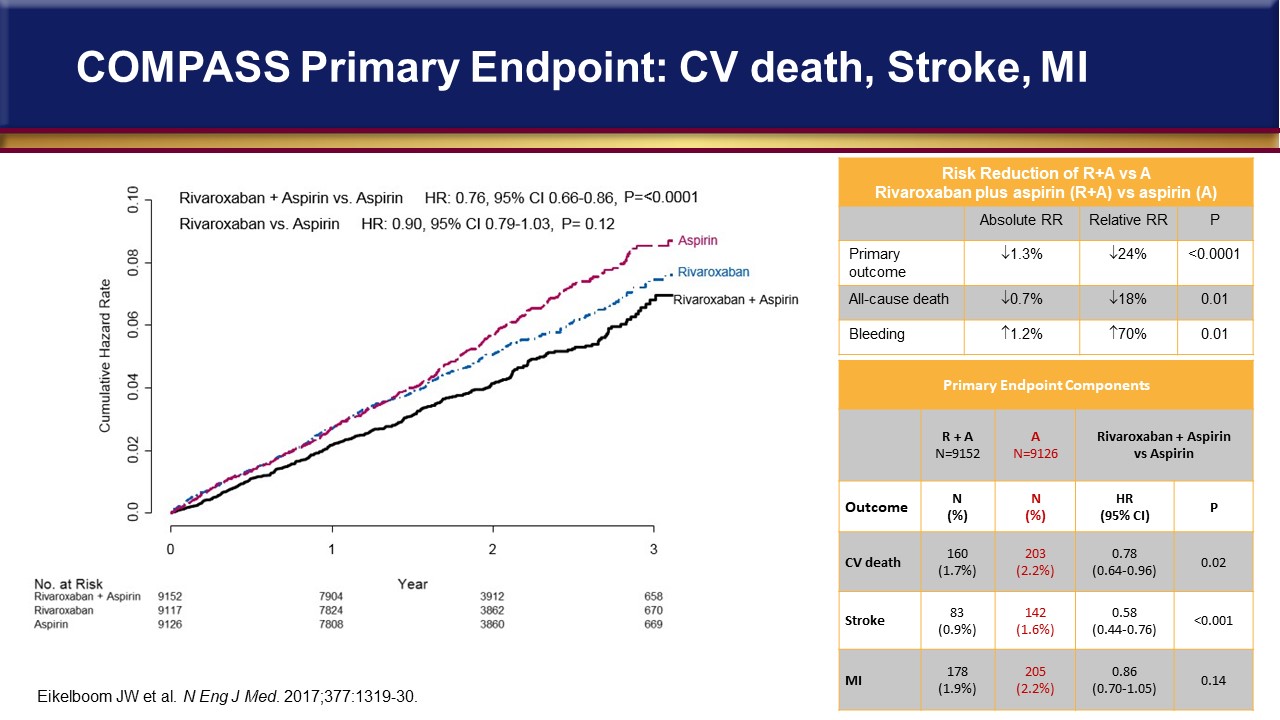
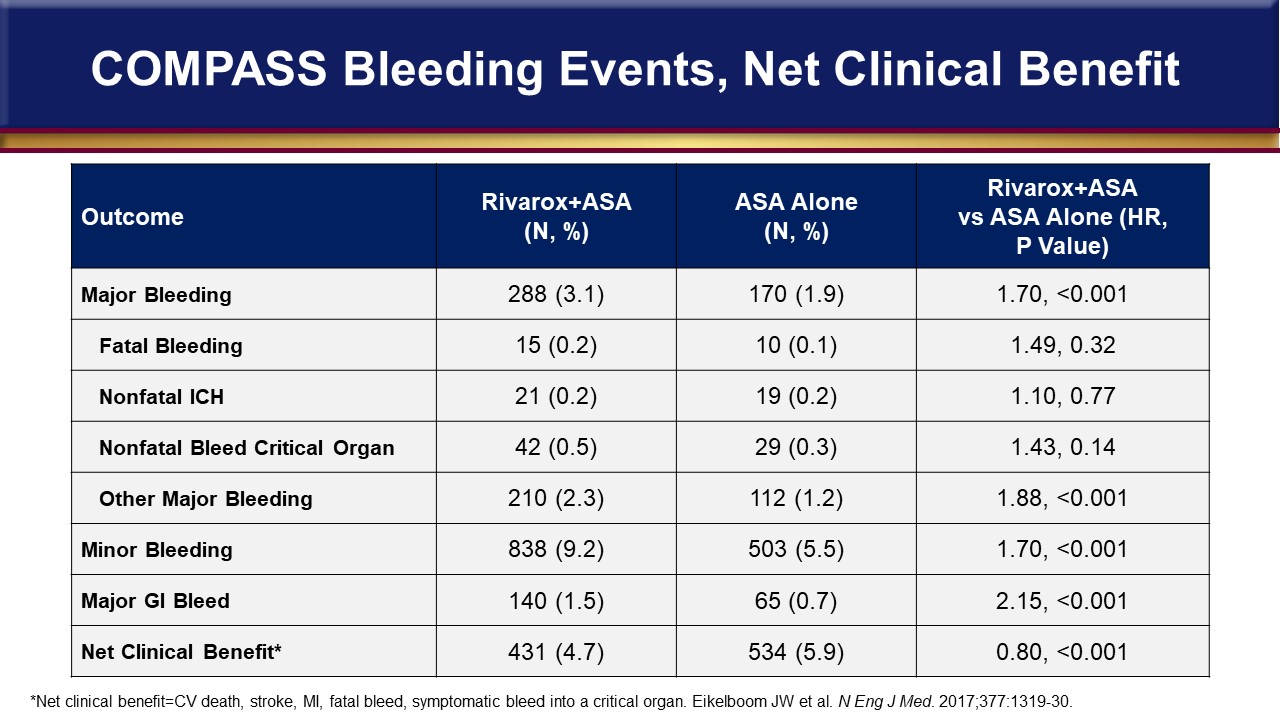
There was also the COMPASS trial with rivaroxaban (Figure 37).29 Over 27,000 patients were enrolled who had stable CAD or PAD, and there was an aspirin arm, a rivaroxaban-alone arm, and a combined arm. The reduced-dose rivaroxaban of 2.5 mg BID with aspirin was tested for reductions in CV death, stroke, or an MI, and the COMPASS trial results are shown in Figure 38. The lowest event rates were on the low-dose rivaroxaban plus aspirin. That was associated with an absolute risk reduction of 1.3%, so that gives a number needed to treat of 77. All-cause death was reduced statistically, but not very much numerically. But there was an excess of bleeding (Figure 39) with the combination compared to aspirin alone, so one has to be careful and vigilant when using the combination antiplatelet therapy with an anticoagulant, even with reduced anticoagulant doses.
Figure 39
What about inflammation? There are two trials that have been in the last year and a half or so. One is called CIRT30 with low-dose methotrexate that had no effect on inflammatory markers and, therefore, had no effect on major adverse cardiac events (Figure 40, lower panel).
Figure 40
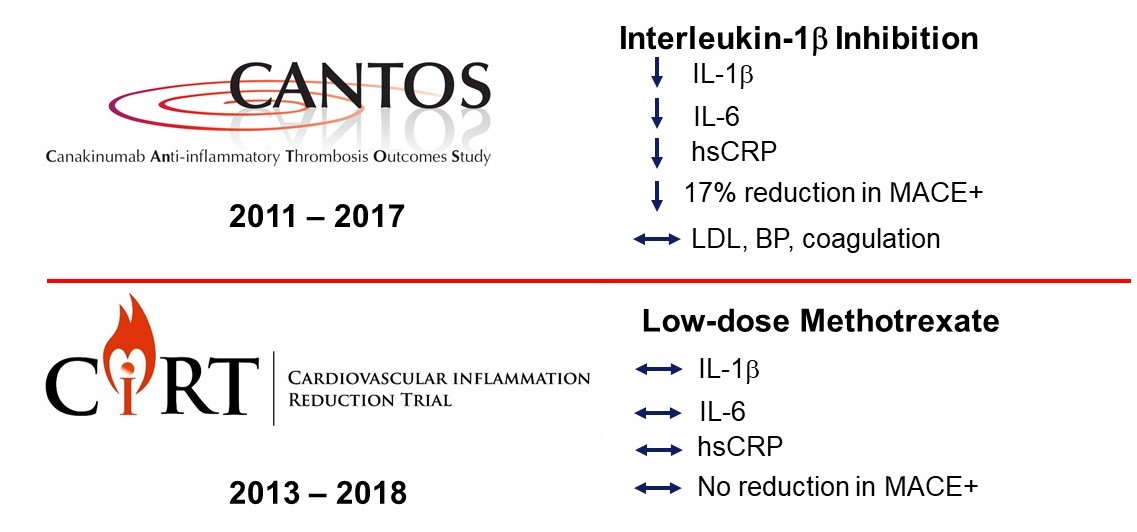
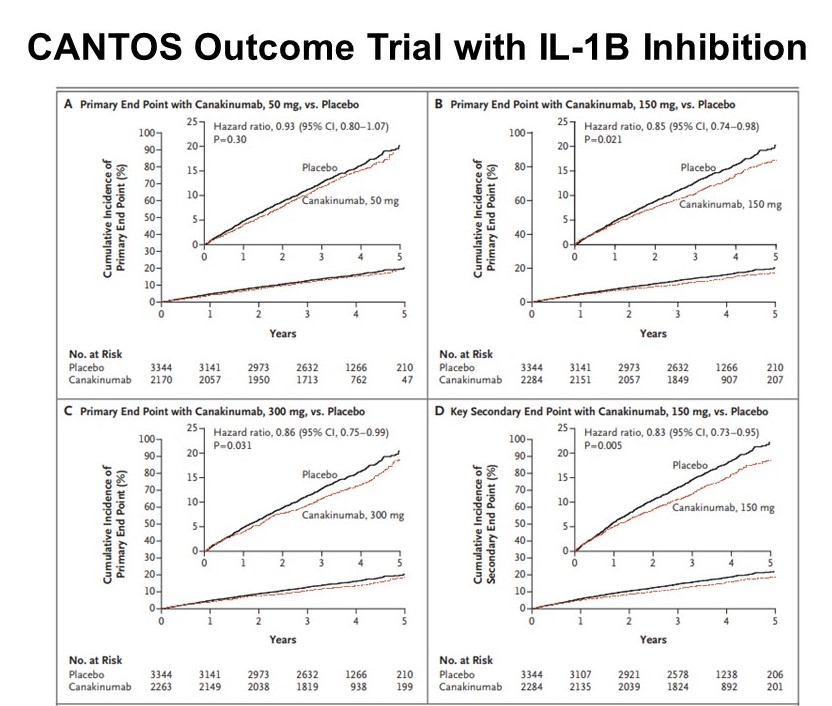
And then there’s the CANTOS31 trial with an anti-inflammatory drug that targets interleukin-1 beta called canakinumab, which is FDA-approved at a cost of about $200,000 a year for a couple of rare autoimmune diseases, Tumor Necrosis Factor (TNF) receptor Associated Periodic Syndrome (TRAPS) and Hyperimmunoglobulin D (Hyper-IgD) Syndrome (HIDS)/Mevalonate Kinase Deficiency (MKD). However, that $200,000 a year cost is based on a monthly dosing strategy. This CANTOS trial was a dose-ranging trial as well as a proof-of-concept trial where patients received one of three doses administered subcutaneously every 3 months. The primary endpoint was the typical combination of CV death, MI and stroke endpoints.31 Figure 41 shows that the 50 mg dose had no benefit, the 150 mg dose showed benefit; and the 300 mg showed a mild benefit as well, and then the 150 mg dose also showed an endpoint benefit that when adding unstable angina as a secondary endpoint. However, despite the proof of concept that inhibiting inflammatory pathways can reduce major CV events, the FDA denied approval for this indication.
Figure 41
So, from these statin adjunct trials, we can conclude the following. Targeting additional LDL-C reduction does produce a modest additional risk reduction with minimal risk and minimal additional cost if the PCSK9i cost keeps coming down. And targeting triglycerides with fibrates and niacin did not show additional risk reduction, however purified EPA added to statin therapy has shown benefits of important clinical value. An updated indication based on the results of REDUCE-IT is expected from the FDA at the end of the year or in early 2020. Targeting thrombotic targets does give some additional risk reduction, but usually with a more than offsetting risk for major and minor bleeding. Increasing HDL by the means that have been tested just isn’t effective and points to the need to better understand the role and function of HDL. Targeting inflammation does also produce a modest additional risk reduction but a viable therapeutic cost-effective solution remains elusive.
References
- Grundy SM, Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, Braun LT, de Ferranti S, Faiella-Tommasino J, Forman DE, Goldberg R, Heidenreich PA, Hlatky MA, Jones DW, Lloyd-Jones D, Lopez-Pajares N, Ndumele CE, Orringer CE, Peralta CA, Saseen JJ, Smith SC Jr, Sperling L, Virani SS, Yeboah J. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;139:e1082-e1143.
- acc.org/ascvd-risk-estimator-plus/#!/calculate/estimate. Accessed August 28, 2019.
- 4S Group. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). 1994;344:1383-9.
- LIPID Study Group. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med. 1998;339:1349-57.
- Sacks FM Pfeffer MA, Moye LA, Rouleau JL, Rutherford JD, Cole TG, Brown L, Warnica JW, Arnold JM, Wun CC, Davis BR, Braunwald E. The effect of pravastatin on coronary events after myocardial infarction in patients with average cholesterol levels. Cholesterol and Recurrent Events Trial investigators. N Engl J Med. 1996;335:1001-9.
- HPS Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet. 2002;360:7-22.
- Shepherd J, Cobbe SM, Ford I, Isles CG, Lorimer AR, MacFarlane PW, McKillop JH, Packard CJ. Prevention of coronary heart disease with pravastatin in men with hypercholesterolemia. West of Scotland Coronary Prevention Study Group. N Engl J Med. 1995;333:1301-7.
- Downs JR, Clearfield M, Weis S, Whitney E, Shapiro DR, Beere PA, Langendorfer A, Stein EA, Kruyer W, Gotto AM Jr. Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels: results of AFCAPS/TexCAPS. Air Force/Texas Coronary Atherosclerosis Prevention Study. 1998;279:1615-22.
- Ridker PM, Danielson E, Fonseca FA, Genest J, Gotto AM Jr, Kastelein JJ, Koenig W, Libby P, Lorenzatti AJ, MacFadyen JG, Nordestgaard BG, Shepherd J, Willerson JT, Glynn RJ; JUPITER Study Group. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med. 2008;359:2195-207.
- Orringer CE. Icosapent ethyl: Where will it fit into guideline-based medical therapy for high risk atherosclerotic cardiovascular disease? Trends Cardiovasc Med. 2019;pii: S1050-1738(19)30054-4.
- Cannon CP, Blazing MA, Giugliano RP, McCagg A, White JA, Theroux P, Darius H, Lewis BS, Ophuis TO, Jukema JW, De Ferrari GM, Ruzyllo W, De Lucca P, Im K, Bohula EA, Reist C, Wiviott SD, Tershakovec AM, Musliner TA, Braunwald E, Califf RM; IMPROVE-IT Investigators. Ezetimibe added to statin therapy after acute coronary syndromes. N Engl J Med. 2015;372:2387-2397.
- Sabatine MS, Giugliano RP, Keech AC, Honarpour N, Wiviott SD, Murphy SA, Kuder JF, Wang H, Liu T, Wasserman SM, Sever PS, Pedersen TR; FOURIER Steering Committee and Investigators. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. 2017;376:1713-22.
- Schwartz GG, Steg PG, Szarek M, Bhatt DL, Bittner VA, Diaz R, Edelberg JM, Goodman SG, Hanotin C, Harrington RA, Jukema JW, Lecorps G, Mahaffey KW, Moryusef A, Pordy R, Quintero K, Roe MT, Sasiela WJ, Tamby JF, Tricoci P, White HD, Zeiher AM; ODYSSEY OUTCOMES Committees and Investigators. Alirocumab and cardiovascular outcomes after acute coronary Syndrome. N Engl J Med. 2018;379:2097-107.
- Bhatt DL, Steg PG, Miller M, Brinton EA, Jacobson TA, Ketchum SB, Doyle RT Jr, Juliano RA, Jiao L, Granowitz C, Tardif JC, Ballantyne CM; REDUCE-IT Investigators. Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia. N Engl J Med. 2019;380:11-22.
- Cannon CP, Braunwald E, McCabe CH, Rader DJ, Rouleau JL, Belder R, Joyal SV, Hill KA, Pfeffer MA, Skene AM; Pravastatin or Atorvastatin Evaluation and Infection Therapy-Thrombolysis in Myocardial Infarction. Intensive versus moderate lipid lowering with statins after acute coronary syndromes. N Engl J Med. 2004;350:1495-504.
- Abifadel M., Varret M., Rabes J. P., Allard D., Ouguerram K., Devillers M., Cruaud C., Benjannet S., Wickham L., Erlich D., Derré A, Villéger L, Farnier M, Beucler I, Bruckert E, Chambaz J, Chanu B, Lecerf JM, Luc G, Moulin P, Weissenbach J, Prat A, Krempf M, Junien C, Seidah NG, Boileau C. Mutations in PCSK9 cause autosomal dominant hypercholesterolemia. Genet. 2003;34: 154–156.
- Cohen JC, Boerwinkle E, Mosley TH Jr, Hobbs HH. Sequence variations in PCSK9, low LDL, and protection against coronary heart disease. N Engl J Med. 2006; 354:1264-72.
- Anderson JL, Heidenreich PA, Barnett PG, Creager MA, Fonarow GC, Gibbons RJ, Halperin JL, Hlatky MA, Jacobs AK, Mark DB, Masoudi FA, Peterson ED, Shaw LJ. ACC/AHA statement on cost/value methodology in clinical practice guidelines and performance measures: a report of the American College of Cardiology/American Heart Association Task Force on Performance Measures and Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63:2304-22.
- Fonarow GC, Keech AC, Pedersen TR, Giugliano RP, Sever PS, Lindgren P, van Hout B, Villa G, Qian Y, Somaratne R, Sabatine MS. Cost-effectiveness of evolocumab therapy for reducing cardiovascular events in patients with atherosclerotic cardiovascular Disease. JAMA Cardiol. 2017; 2:1069-78.
- Kazi DS Penko J, Coxson PG, Moran AE, Ollendorf DA, Tice JA, Bibbins-Domingo K5. Updated cost-effectiveness analysis of PCSK9 inhibitors based on the results of the FOURIER trial. JAMA. 2017;318:748-50.
- Kazi DS, Penko J, Coxson PG, Guzman D, Wei PC, Bibbins-Domingo K. Cost-effectiveness of alirocumab: A just-in-time analysis based on the ODYSSEY outcomes trial. Ann Intern Med. 2019. Jan 1. doi: 10.7326/M18-1776. [Epub ahead of print]
- Keech A, Simes RJ, Barter P, Best J, Scott R, Taskinen MR, Forder P, Pillai A, Davis T, Glasziou P, Drury P, Kesäniemi YA, Sullivan D, Hunt D, Colman P, d'Emden M, Whiting M, Ehnholm C, Laakso M; FIELD study investigators. Effects of long-term fenofibrate therapy on cardiovascular events in 9795 people with type 2 diabetes mellitus (the FIELD study): randomised controlled trial. Lancet. 2005;366:1849-61.
- ACCORD Study Group, Ginsberg HN, Elam MB, Lovato LC, Crouse JR 3rd, Leiter LA, Linz P, Friedewald WT, Buse JB, Gerstein HC, Probstfield J, Grimm RH, Ismail-Beigi F, Bigger JT, Goff DC Jr, Cushman WC, Simons-Morton DG, Byington RP. Effects of combination lipid therapy in type 2 diabetes mellitus. N Engl J Med. 2010;362:1563-74.
- AIM-HIGH Investigators, Boden WE, Probstfield JL, Anderson T, Chaitman BR, Desvignes-Nickens P, Koprowicz K, McBride R, Teo K, Weintraub W. Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. N Engl J Med. 2011;365:2255-67
- HPS2-THRIVE Collaborative Group, Landray MJ, Haynes R, Hopewell JC, Parish S, Aung T, Tomson J, Wallendszus K, Craig M, Jiang L, Collins R, Armitage J. Effects of extended-release niacin with laropiprant in high-risk patients. N Engl J Med. 2014;371:203-12.
- HPS3/TIMI55–REVEAL Collaborative Group, Bowman L, Hopewell JC, Chen F, Wallendszus K, Stevens W, Collins R, Wiviott SD, Cannon CP, Braunwald E, Sammons E, Landray MJ. Effects of anacetrapib in patients with atherosclerotic vascular disease. N Engl J Med. 2017;377:1217-1227.
- Chen KY, Rha SW, Li YJ, Poddar KL, Jin Z, Minami Y, Wang L, Kim EJ, Park CG, Seo HS, Oh DJ, Jeong MH, Ahn YK, Hong TJ, Kim YJ, Hur SH, Seong IW, Chae JK, Cho MC, Bae JH, Choi DH, Jang YS, Chae IH, Kim CJ, Yoon JH, Chung WS, Seung KB, Park SJ; Korea Acute Myocardial Infarction Registry Investigators. Triple versus dual antiplatelet therapy in patients with acute ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. Circulation. 2009;119:3207-14.
- Morrow DA, Braunwald E, Bonaca MP, Ameriso SF, Dalby AJ, Fish MP, Fox KA, Lipka LJ, Liu X, Nicolau JC, Ophuis AJ, Paolasso E, Scirica BM, Spinar J, Theroux P, Wiviott SD, Strony J, Murphy SA; TRA 2P–TIMI 50 Steering Committee and Investigators. Vorapaxar in the secondary prevention of atherothrombotic events. N Engl J Med. 2012;366:1404-13.
- Eikelboom JW, Connolly SJ, Bosch J, Dagenais GR, Hart RG, Shestakovska O, Diaz R, Alings M, Lonn EM, Anand SS, Widimsky P, Hori M, Avezum A, Piegas LS, Branch KRH, Probstfield J, Bhatt DL, Zhu J, Liang Y, Maggioni AP, Lopez-Jaramillo P, O'Donnell M, Kakkar AK, Fox KAA, Parkhomenko AN, Ertl G, Störk S, Keltai M, Ryden L, Pogosova N, Dans AL, Lanas F, Commerford PJ, Torp-Pedersen C, Guzik TJ, Verhamme PB, Vinereanu D, Kim JH, Tonkin AM, Lewis BS, Felix C, Yusoff K, Steg PG, Metsarinne KP, Cook Bruns N, Misselwitz F, Chen E, Leong D, Yusuf S; COMPASS Investigators. Rivaroxaban with or without aspirin in stable cardiovascular disease. N Engl J Med. 2017; 377:1319-1330.
- Ridker PM, Everett BM, Pradhan A, MacFadyen JG, Solomon DH, Zaharris E, Mam V, Hasan A, Rosenberg Y, Iturriaga E, Gupta M, Tsigoulis M, Verma S, Clearfield M, Libby P, Goldhaber SZ, Seagle R, Ofori C, Saklayen M, Butman S, Singh N, Le May M, Bertrand O, Johnston J, Paynter NP, Glynn RJ; CIRT Investigators. Low-dose methotrexate for the prevention of atherosclerotic events. N Engl J Med. 2019;380:752-762.
- Ridker PM, Everett BM, Thuren T, MacFadyen JG, Chang WH, Ballantyne C, Fonseca F, Nicolau J, Koenig W, Anker SD, Kastelein JJP, Cornel JH, Pais P, Pella D, Genest J, Cifkova R, Lorenzatti A, Forster T, Kobalava Z, Vida-Simiti L, Flather M, Shimokawa H, Ogawa H, Dellborg M, Rossi PRF, Troquay RPT, Libby P, Glynn RJ; CANTOS Trial Group. Antiinflammatory therapy with canakinumab for atherosclerotic disease. N Engl J Med. 2017;377:1119-1131.
Back Top