
Expired activity
Please go to the PowerPak
homepage and select a course.
Pharmacists' Role in the Comprehensive Care of Acute Coronary Syndrome
INTRODUCTION
Acute coronary syndrome (ACS), including unstable angina (UA) and myocardial infarction (MI), is the most common cause of death due to coronary heart disease (CHD), which itself is the leading cause of death in the United States (US). (1) There are numerous guidelines and recommendations for managing patients with ACS. Pharmacists need to be familiar with the most current guidelines and evolving clinical perspectives on the roles of standard and newer therapies and their risks and benefits. Increasing their knowledge will improve their ability to prepare management plans that optimize patient adherence to therapy and improve outcomes with antithrombotic therapies while reducing unnecessary hospitalizations and adverse events. This monograph will address key practice concerns for pharmacists relative to ACS and help them develop effective patient education strategies.
Acute Coronary Syndrome Overview
The cause of an ACS is primarily the rupture of an atherosclerotic plaque with subsequent platelet adherence, activation, and aggregation, and the activation of the clotting cascade. Ultimately, a clot forms composed of fibrin (end product of the coagulation cascade) and platelets. National guidelines recommend strategies for ACS patient care for ST-segment elevation (STE), non-ST-segment elevation (NSTE) ACS, and for percutaneous coronary intervention (PCI), including PCI in the setting of ACS. (2, 3, 4) These practice guidelines are based on a review of available clinical evidence, have graded recommendations based on evidence and expert opinion, and are updated periodically. These guidelines form the cornerstone for quality care of the ACS patient.
Patients with ACS typically experience chest pain similar to patients with chronic stable angina, but the symptoms are often more severe and prolonged or refractory despite medical interventions. Like patients with chronic stable angina, those experiencing ACS are at risk for complications such as MI, heart failure (HF), ventricular arrhythmias, and death. The spectrum of ACS includes ST-segment-elevation myocardial infarction (STEMI), non-ST-segment-elevation myocardial infarction (NSTEMI), and unstable angina (UA). (2,3)
Epidemiology
Increasing age is directly related to the prevalence of both coronary artery disease (CAD) and CAD-related events such as MI. The American Heart Association (AHA) estimates that every 40 seconds an American will experience a MI, and over 1 million patients leave the hospital annually with a primary or secondary diagnosis of an ACS. (1) Myocardial infarction accounts for more than 70% of these hospitalizations, the majority of which represent the first occurrence of a coronary event. (1) Over the last two decades, the proportion of all patients with MI experiencing a NSTEMI and STEMI was 67% and 33%, respectively. This reflects a decline of 62% for STEMI over that time period (47% in 1999, 22.9% in 2008, p<0.001) while the age- and sex-adjusted incidence of NSTEMI was largely unchanged over the same period. (5) Many patients who experience a MI experience symptoms prompting emergent care, however, an estimated 170,000 Americans will suffer a MI with minimal or no symptoms (e.g., “silent MI”) that may go undetected, placing them at high risk for major adverse cardiovascular events (MACE). (1)
Patients who experience ACS are at high risk for complication including death, development of HF, cardiogenic shock, and ventricular arrhythmias, all of which contribute to the mortality seen with this disease. Current 1- and 5-year mortality rates for MI are estimated at 18-23% and 36-47% for males and females, respectively. The short-term risks for complications are increased in patients who experience a STEMI versus NSTEMI, whereas patients with NSTEMI typically have greater long-term risks. (1) Fortunately, declines in STEMI prevalence and overall severity of MI coupled with therapeutic advances have contributed to a reduction in complications associated with ACS globally. For example, the incidence of HF following MI has declined more than 40% over the last two decades and the risk of death has similarly declined. (1) The improvement in the rates of mortality and MACE can be attributed to the increased use of PCI and optimal medical therapy. Hence the use of evidence-based therapies to treat ACS is paramount to improve outcomes. (1)
In addition to the significant clinical burden on individual patients, ACS places a significant financial burden on the healthcare system. In the last 2 decades, hospital length of stay (LOS) for ACS has dropped by 20% with the mean LOS being 5.5 days. (5) Despite this decrease, the frequent use of revascularization therapies (e.g. PCI and coronary artery bypass grafting [CABG]) has led to an increased cost per patient, resulting in a 10% increase in patients with MI treated with PCI and approximately a 20% increase in those treated with CABG surgery between 2001 and 2011. (6) In the United States (US), the mean cost of treating patients hospitalized for UA is estimated at $7,916 (median cost, $7,841) while the average cost of a hospitalization for MI is $24,695 (median cost, $26,749). (7) The economic cost of ACS provides further stimulus to ensure evidence-based therapies are optimized to prevent recurrent events and additional utilization of healthcare resources.
Pathophysiology
The central paradigm regarding the pathophysiology of an ACS event is the rupture of an atherosclerotic plaque in the coronary vasculature with subsequent thrombus formation at the site of injury. The acute pathologic thrombus leads to an abrupt reduction or cessation of blood flow distal to the site leading to ischemia and potentially death of myocytes and infarction. (8) Plaques that are at the root of an ACS event differ from those that produce demand driven angina. The vulnerable plaque at the heart of an ACS event tends to be smaller (<70% of the luminal diameter), have a thin fibrous cap, a large cholesterol necrotic core, and evidence of inflammation. (9) Importantly, patients with non-obstructive plaques may not experience angina symptoms and are often unaware they have atherosclerotic plaques until the ACS event occurs. Inflammatory processes are typically involved in transforming plaques into the typical “vulnerable plaque” prone to rupture. (10) However, a thinning fibrous cap by itself does not usually produce plaque rupture; there is typically a connection to physiological or psychological stress which enhances the likelihood of an acute event. (11, 12) A majority of ACS events happen in the early morning and may be tied to the circadian rhythm activation of the sympathetic nervous system and catecholamine release that produces an increase in heart rate and blood pressure, placing physical stress on the vulnerable plaque.
Once plaque rupture has taken place, plaque contents are exposed to the blood leading to activation of pro-thrombotic mechanisms including platelets and the coagulation cascade. As these are arterial thrombi, platelets are a dominant feature in thrombus formation, although the coagulation cascade does play a role. (13) Upon plaque rupture, circulating platelets are initially attracted and adhere to the area of injury. Platelets may then be activated by numerous substances (thromboxane A2, adenosine diphosphate (ADP), epinephrine, and serotonin) causing a change in the platelet’s shape, recruitment of more platelets to the site of injury, and expression of active GP IIb/IIIa receptors. Platelets link together with these receptors and a fibrinogen molecule, a process known as platelet aggregation. The overall process of platelet adhesion, activation, and aggregation produce a platelet plug in the area of atherosclerotic plaque rupture. (13) The formation of a platelet plug is typically not enough to occlude blood flow for any significant amount of time, it must be stabilized by a fibrin meshwork which is the end product of the coagulation cascade. Initiation of the clotting cascade begins with the interaction and activation of factor VII and tissue factor. Tissue factor is found in endothelial cells, as well as on macrophages at the site of the ruptured fibrous cap. Importantly, the activated platelet provides the necessary scaffold for the assembly of the tenase and prothrombinase complex. This intertwining of platelets and the coagulation cascade limits thrombus formation to the site of injury. (13)
Formation of a partially or completely occlusive thrombus abruptly reduces myocardial blood flow and oxygen supply. This abrupt blockage produces ischemia and, if untreated, potentially infarction which results in myocyte necrosis and cell death. (9, 12) Therefore, early recognition and prompt initiation of treatment is crucial to limit myocardial cell damage and optimize outcomes. Various complications (arrhythmias, ventricular remodeling, stroke) are possible in patients with ACS, particularly those with MI, which can manifest hours to weeks after the index event and depend on the nature and extent of ischemia and/or infarction. (14) Ventricular remodeling is typically the result of chronic hyperactivity of either or both the sympathetic nervous system (SNS) and renin-angiotensin aldosterone system (RAAS). (15) Structural and subsequent mechanical changes to the heart as a result of activation of these are the targets of pharmacotherapy agents that blunt this chronic activation.
CASE 1
A 61-year-old Caucasian woman presents to the Emergency Department (ED) with substernal chest pain. The patient states she was reading a book when she started getting a stabbing chest pain that spread to her jaw. She continued to sit quietly for about 30 minutes but the pain never subsided. She ranks the pain an 8 out of 10. The ED orders an ECG and draws blood for cardiac markers.
CASE 1 QUESTIONS
- How is chest pain characterized in patients who experience chronic stable angina?
- How is chest pain characterized in patients who experience ACS?
- Is this patient’s presentation consistent with ACS?
- How are the results of the ECG and blood draw for cardiac markers relevant for determining the most optimal treatment approach for the patient?
PAUSE AND REFLECT: Assess this case based on the activity content thus far, then listen to faculty commentary.
|
Treatment Approaches in ACS
Treatment Approach for Patients with ACS
Overall treatment decisions for patients with ACS are made based on the initial and ongoing risk stratification. Rapid identification and delineation of ACS subtype (STEMI, NSTE-ACS) is imperative to triage the patient to the most appropriate management strategy and also play a role in the selection of various pharmacotherapy options. When ACS is suspected, the patient should be referred to a site that can perform an initial evaluation including 12-lead electrocardiogram (ECG) and assessment of a cardiac troponin level (cTn) so that timely management can take place. (2,3) Patients with ischemic symptoms in conjunction with high-risk features (persistent chest pain, severe dyspnea, syncope or presyncope, or palpitations) should activate the Emergency Medical Services (EMS) system (e.g., call 9-1-1) and seek transport via ambulance. This approach ensures EMS personnel who are equipped to treat cardiac arrest manage the patient as soon as possible, especially if reperfusion therapy is indicated.
Treatment of ACS patients is targeted at improving outcomes in both short-and long-term outcomes. Short-term outcomes include: (a) early restoration of blood flow to the infarct-related artery to prevent infarct expansion (in the case of MI) or prevent complete occlusion and MI (in UA); (b) prevention of death and other MI complications; (c) prevention of coronary artery reocclusion; and (d) relief of ischemic chest discomfort. The control of CAD risk factors, prevention of additional MACE, including reinfarction, stroke, and HF, and improvement in quality of life are typical long-term outcomes for ACS patients.
The initial step in managing ACS includes rapid diagnostic triage to determine an appropriate management strategy (Figure 1).
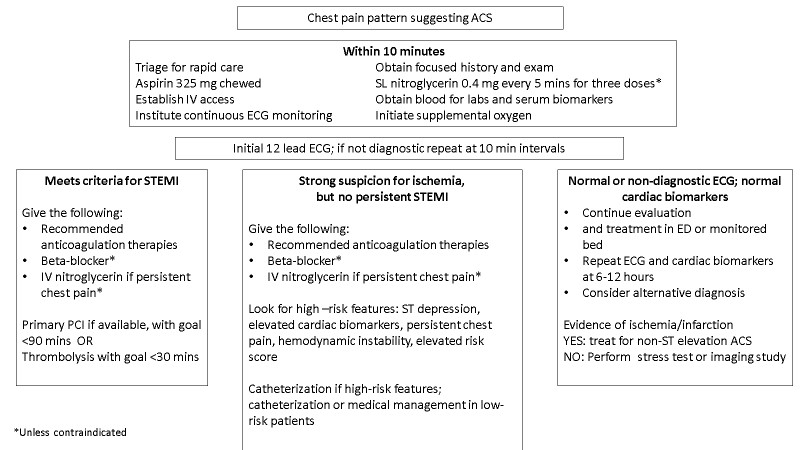 |
ACS, acute coronary syndrome; ECG, electrocardiogram; STEMI, ST-elevation myocardial infarction
Figure 1. General approach to triaging ACS in the emergency department. Adapted from: Reeder GS, Awtry E, Mahler S. Initial evaluation and management of suspected acute coronary syndrome (myocardial infarction, unstable angina) in the emergency department. UpToDate. June 2019. Available at https://www.uptodate.com/contents/initial-evaluation-and-management-of-suspected-acute-coronary-syndrome-myocardial-infarction-unstable-angina-in-the-emergency-department?search=acute%20coronary%20syndrome&source=search_result&selectedTitle=2~150&usage_type=default&display_rank=2. |
Patients with ST segment elevation on the initial ECG are uniformly high risk and should be emergently referred to the cardiac catheterization lab for primary PCI in order to re-establish blood flow to the myocardium. Patients with non-ST segment ACS are a more heterogeneous population as it relates to risk. As such, additional risk stratification is needed to determine the best approach, which is usually an early invasive approach (e.g., PCI) for intermediate- and high-risk patients or a more conservative, ischemia-guided management plan without planned PCI for those with either the lowest risk for coronary event or contraindications to the invasive procedure itself. General treatment measures regardless of treatment strategy for intermediate- and high-risk patients include admission to the hospital, oxygen administration (if oxygen saturation is <90%), bed rest with continuous multi-lead ST-segment monitoring for arrhythmias and ischemia, frequent measurement of vital signs, ischemic pain relief, and prompt initiation of antithrombotic therapy. (2,3)
From a pharmacotherapy perspective, available options can be grouped into one of three general categories. First, a range of antithrombotic agents is available to treat the acute pathologic thrombus. Second, as the rapid reduction in blood flow results in myocardial ischemia, several management options specifically target the reduction of myocardial ischemia. Lastly, other options seek to reduce or halt the progression of atherosclerosis, as well as prevent complications of myocardial ischemia/infarction. Table 1 lists the various pharmacotherapeutic options for both STEMI and NSTEMI that can be considered.
| Table 1 |
|
Target of Intervention
|
Pharmacotherapy Options
|
|
Acute Pathologic Thrombus
|
• Antiplatelet therapy
– Aspirin
– Thienopyridines
– Glycoprotein IIb/IIIa inhibitors
– Cangrelor
• Antithrombotic therapy
– Unfractionated heparin
– Low molecular weight heparin
– Factor Xa inhibitor
– Direct thrombin inhibitor
|
|
Acute Myocardial Ischemia
|
• Beta-blockers
• Nitrates
• Oxygen
• Morphine
• Calcium channel blockers
|
|
Secondary Prevention of Recurrent Events/Progression of atherosclerotic vascular disease
|
• Lipid lowering therapy
• RAAS inhibition
- Angiotensin converting enzyme inhibitors
- Aldosterone antagonists
• Risk factor modification (blood pressure [BP], diabetes mellitus [DM], diet, exercise)
|
The timing of the interventions in Table 1 may vary. Historically, early supportive care for all ACS patients followed the mnemonic MONA (Morphine,Oxygen,Nitroglycerin,Aspirin). Many of these can be administered even prior to hospital arrival and seek to help stabilize the patient. However, in recent years, recommendations for the routine use of some of these therapies (e.g., morphine, oxygen) has dissipated due to potentially harmful effects. (14) The use of opiates in particular has come under significant scrutiny due to the potential for slowing the gut absorption of thienopyridines, antiplatelet agents that are central to improve outcomes in patients. An updated mnemonic THROMBINS2 (Thienopyridine,Heparin,Renin-angiotensin-aldosterone system,Oxygen,Morphine,b-blocker,Intervention [e.g., PCI],Nitroglycerin,Statin/Salicylate [e.g., aspirin]) has emerged as a reminder for early interventions to consider in patients with ACS. (16)
Nitroglycerin
Nitrates, including nitroglycerin (NTG), are effective anti-ischemic medications and are routinely recommended as part of the initial management of patients with ACS. (2,3) Nitrates primarily cause venodilation leading to reduced preload and myocardial oxygen demand. However, some dilation of the coronary arteries may occur and increased coronary blood flow may be seen as well. Despite their routine use, nitrates have never been demonstrated to reduce MACE. (3) Despite a lack of evidence on hard outcomes, nitroglycerin is effective in relieving angina symptoms and is often utilized in patients with ACS with ongoing angina who are not hypotensive. (2,3) Initially, sublingual nitroglycerin should be administered every five minutes for up to three doses as needed for chest pain. For patients with persistent angina despite sublingual nitroglycerin, intravenous nitroglycerin should be considered, particularly in patients with uncontrolled hypertension (HTN) or evidence of HF on presentation. Intravenous nitroglycerin can be continued until symptoms have resolved and the patient has stabilized and can be transitioned to an appropriate oral regimen.
Morphine
Historically, morphine was used routinely in ACS due to its potent analgesic and anxiolytic effects that also cause venodilation and increase vagal tone which reduces heart rate. (2,3) Its clinical effects are similar to nitroglycerin though, randomized clinical trials have not been conducted to determine the optimal dose nor to evaluate the safety and efficacy of IV morphine in patients with ACS. Recent observational studies have called into question the safety of routinely using IV morphine to treat ACS. These studies have observed a higher rate of in-hospital death, longer hospital stays and larger infarct size in patients receiving morphine. (17) As previously alluded to, a potential mechanism for these observations is the presence of a drug-drug interaction with P2Y12 inhibitors. Prolonged time to peak concentrations and decreased total drug exposure leading to less platelet inhibition are likely the result of morphine slowing gastric emptying along with nausea and vomiting in some patients. (18) Given these observations, the use of IV morphine is recommended only in patients refractory to treatment with other anti-ischemic medications (Class IIb recommendation). (3)
Oxygen
Although routine oxygen is often administered to patients with ACS, it should be reserved for a minority of patients, particularly those with oxygen saturation less than 90%. Emerging data suggests that routine use of oxygen may adversely affect patients with ACS by increasing coronary vascular resistance and reducing coronary blood flow. (2,3)
Beta-blockers (β-blockers)
Beta-blockers are a cornerstone in the management of all ACS patients given their anti-ischemic effects (reduced heart rate, contractility and myocardial oxygen demand) as well as their documented ability to reduce the risk of MACE. (2,3) They should be initiated as soon as possible in all ACS patients provided there are no contraindications. Beta-blockers reduce the risk of reinfarction and post-infarction angina in patients with MI. (19,20)
Beta-blockers have been shown to improve survival in patients with MI, although this benefit has been questioned in recent years as studies demonstrating a mortality benefit were conducted prior to the modern era (pre-reperfusion) of treatment for ACS. One meta-analysis of 60 trials (N=102,003) evaluating beta-blockers in MI found a modest mortality benefit in studies conducted during the pre-reperfusion era, but no benefit was observed in studies completed during the reperfusion or modern era. (19) Although the mortality benefit of beta-blockers in the modern era of ACS management is uncertain, since they reduce the risk of MI, angina, and arrhythmias, in the absence of contraindications, current guidelines recommend the initiation of oral beta-blockers within the first 24 hours of presentation and continuation of therapy for at least three years. (2, 3, 21) Adverse effects with beta-blockers include HF, hypotension, bradycardia, and cardiogenic shock. (22) Therefore, in patients with evidence of or risk of developing these complications, beta-blocker therapy should be withheld and initiation reassessed later during hospitalization. (2, 3)
Calcium channel blockers
Calcium channel blockers (CCBs) are typically reserved for patients who are unable to take beta-blockers and need an alternative agent to provide acute anti-ischemic effects. (2,3) Although CCBs are effective as anti-ischemic agents (arterial vasodilation, decreased blood pressure, reduced heart rate and myocardial oxygen demand), the lack of consistent benefit in clinical trials and the robust data supporting beta-blockers have narrowed the indications for CCBs in patients with ACS. (2,3) Current guidelines recommend non-dihydropyridine (DHP) CCBs (e.g., diltiazem, verapamil) to treat angina symptoms in patients with ACS who have a contraindication, intolerance, or are refractory to beta-blockers in the absence of left ventricular dysfunction, risk factors for cardiogenic shock, and atrioventricular conduction defects. (2,3)
Management strategies in STEMI
The paradigm of immediate reperfusion during STEMI is responsible for the dramatic decrease in MI related mortality over the past 3 decades in the US . (23) Options for reperfusion include fibrinolytics or mechanical intervention via PCI with or without stenting, both with the aim of restoring blood flow to the infarct related artery. The selection of which reperfusion strategy to use is dependent on timing of presentation and the availability of primary PCI. Regardless of strategy used though, a systematic approach to reduce delays in reperfusion are critical and include prehospital assessment of the initial ECG by EMS, early anti-ischemic medication administration, and transport to a hospital with PCI capable facilities.
Primary PCI improves survival, establishes consistent revascularization to the infarct related artery, significantly reduces the risk of stroke and intracranial hemorrhage, and reduces reinfarction and recurrent ischemia when compared to fibrinolysis. (2, 24, 25) In addition, more rapid performance of primary PCI can result in superior clinical outcomes for patients with STEMI. (2, 24, 25) Early reperfusion with primary PCI is preferred by guidelines for patients presenting with STEMI, with the goal of reperfusion within 90 minutes from time of first medical contact. (2) Only 39% of all hospitals in the US can perform PCI, which leaves fibrinolysis as the only other reperfusion strategy for many patients. (26) Current recommendations for patients presenting with STEMI to a hospital unable to perform PCI are to transfer them to a PCI-capable hospital to achieve reperfusion within 120 minutes of the first medical contact. (2) Patients with STEMI undergoing primary PCI also require adjunctive antiplatelet and anticoagulant therapy which is discussed in greater detail later in this monograph.
When primary PCI for patients with STEMI is not possible within the desired time frame, fibrinolysis becomes the preferred reperfusion strategy. Fibrinolytics prevent 30 early deaths per 1000 patients treated within 6 hours of symptom onset. While an exact time frame is debatable based on the current literature, recent guidelines state that fibrinolysis is indicated and should be administered when PCI cannot be performed within 120 minutes. (2) If fibrinolysis is the preferred strategy for reperfusion, therapy should be given within 30 minutes of hospital arrival provided no contraindications are present. (2) Fibrinolytic therapy is associated with a slight but statistically significant risk for stroke, largely attributed to intracranial hemorrhage (ICH), which occurs in 0.9-1.0% of patients. (27) Significant predictors for ICH include advanced age, lower total body weight, female sex, pre-existing cerebrovascular disease, and systolic and diastolic HTN at time of presentation. (27) Relative contraindications to fibrinolytic therapy should be mitigated where possible (e.g., giving antihypertensive medications to reduce blood pressure to <185/110 mm Hg) to reduce the risk for major bleeding, including ICH, prior to administration. Patients at high risk for major bleeding (including a history of ICH) presenting with an absolute contraindication should not receive fibrinolytic therapy and should be transferred to a hospital capable of performing PCI. Fibrin-specific agents (alteplase, reteplase, or tenecteplase) are recommended over a non-fibrin-specific agent (e.g., streptokinase) because of greater reperfusion success and less systemic bleeding with fibrin specific agents. (2) As with primary PCI, antiplatelet therapy and parenteral anticoagulation should be given concomitantly in patients treated with fibrinolytic therapy to improve vessel patency and to prevent reocclusion and will be subsequently discussed below. (2)
Management strategies in NSTE-ACS
As discussed previously, patients presenting with NSTE-ACS are more heterogeneous in terms of risk, and the preferred management strategy may vary. (3) In addition, patients presenting with NSTE-ACS typically have a partially occluded coronary artery (as opposed to a total occlusion which is often seen in STEMI) and performing PCI is not as urgent or critical. In NSTE-ACS, patients may be managed with an early-invasive approach, or an ischemia-guided approach (i.e. medical management). (3) With an early invasive approach, the patient has a diagnostic angiography performed early in the hospital course, typically within the first 24 hours in order to determine the best management approach which often can be revascularization with PCI. An early invasive strategy improves cardiovascular outcomes in patients presenting with NSTE-ACS with the greatest benefits achieved in those patients with the highest risk for MACE. Risk stratification is, therefore, essential in NSTE-ACS to determine which patients will derive the most benefit from an early invasive approach. Most recent practice guidelines recommend an early invasive strategy in those with an elevated risk for death or MI (as determined by validated risk scores), those with refractory angina, acute HF, other symptoms of cardiogenic shock, or arrhythmias. (3) Examples of validated risk scales can be found in Table 2. In contrast, patients at the lowest risk are referred to an ischemia-guided approach, or “medical management,” where antiplatelet and anticoagulant medications are administered and PCI is not initially planned. The patient is evaluated for signs and symptoms of recurrent ischemia or hemodynamic instability and taken for coronary angiography and possible PCI only if recurrent symptoms develop. This strategy is appropriate for those with Thrombolysis In Myocardial Infarction (TIMI) risk scores of 0-1, Global Registry of Acute Coronary Events (GRACE) scores <109, for those with serious comorbidities or contraindications to angiography/PCI (e.g., renal failure), or when the risks of the procedure outweigh the benefits of revascularization. (3)
| Table 2 |
TIMI Risk Score (NSTE-ACS)(28)
Each component worth 1 point |
GRACE Risk Score(29)
Points for each component vary based on value |
| Age ≥65 y |
Age |
| ≥3 CAD risk factorsa |
Killip class |
| Known CADb |
Systolic BP |
| Aspirin use within 7 days |
Heart rate |
| ≥2 angina episodes within 24 h |
Serum creatinine |
| Transient STE or ST depression |
Cardiac arrest on admission |
| Elevated biomarkers (e.g., cTn) |
Elevated biomarkers (e.g., cTn) |
| |
ST deviationc |
| Calculate point total and determine risk for major adverse cardiac events |
Low risk: 0-2 points
Intermediate risk: 3-4 points
High risk: ≥5 points |
Low risk: <109 points
Intermediate risk: 109-140 points
High risk: >140 points |
aRisk factors include family history of coronary artery disease, hypertension, hypercholesterolemia, diabetes, and current smoker
bPrior coronary stenosis ≥50%
cIncludes transient ST-segment elevation ≥1 mm, ST-segment depression ≥1 mm, new T wave inversions ≥1 mm, pseudo-normalization of previously inverted T waves, new Q waves, new R wave > S wave in lead V1, new left bundle branch block
TIMI=thrombolysis in myocardial infarction; STEMI=ST-segment elevation myocardial infarction; NSTE-ACS=non-ST-segment elevation acute coronary syndrome; GRACE =global registry of acute coronary events; BP=blood pressure; STE=ST-segment elevation; CAD=coronary artery disease; ST=ST-segment; cTn=cardiac troponin |
CASE 2
A 62-year-old Caucasian woman presents to the ED with ST segment elevation myocardial infarction x 5 hours. She has a past medical history of hypertension, peptic ulcer disease (PUD), and hyperlipidemia. The hospital can initiate PCI therapy in the interventional lab in 130 minutes. Which reperfusion strategy should be selected for this patient?
CASE 2 QUESTIONS
- Which reperfusion strategy would be the most appropriate for the patient?
- Should this patient receive a β-blocker within the first 24 hours? If so, should it be given intravenously or by mouth?
- When would it be appropriate to initiate an ACE inhibitor in this patient?
PAUSE AND REFLECT: Assess case based on content thus far, then listen to faculty commentary.
|
Antithrombotic Therapy in ACS
Antithrombotic Therapy for ACS Patients
Given that pathologic thrombus formation is central to the pathophysiology of ACS, timely and appropriate antithrombotic therapy is an important component of optimal pharmacotherapy. A combination of antiplatelet and anticoagulant strategies is often used in the acute setting, and while most patients historically have continued on long-term antiplatelet therapy only, evidence for use of long-term anticoagulant therapy after ACS is emerging for some high-risk groups. There are several challenges to using antithrombotic therapy in patients with ACS, one being that not all agents have been studied across the spectrum of ACS and its different management strategies. While some agents may have data in the setting of NSTE-ACS, they may not have data in STEMI. For patients with NSTE-ACS, data are different for patients being managed with an ischemia-driven approach compared to those receiving PCI. (3) Some agents may have data in the setting of primary PCI in STEMI, but not with the use of fibrinolytics in STEMI. (2) Additionally, dosing strategies to optimize outcomes may vary depending on the patient population and management strategy. Therefore, it is imperative that pharmacists know the evidence regarding appropriate antithrombotic drug use, dose, and duration based on the patient’s diagnosis and management strategy to optimize patient outcomes and prevent adverse events.
Intravenous Antiplatelet Agents
Glycoprotein (GP) IIb/IIIa inhibitors are potent antiplatelet agents that have been available for over 2 decades and that have a role in preventing MACE in patients with ACS and/or undergoing PCI. Abciximab, a chimeric human-murine monoclonal antibody Fab fragment which blocks the GP IIb/IIIa receptor-fibrinogen binding, was the first agent available for clinical use. Despite strong clinical evidence for abciximab in reducing MACE in several patient populations, the drug is no longer commercially available. Eptifibatide and tirofiban are commonly referred to as “small molecule” GP IIb/IIIa inhibitors, as they are peptide and nonpeptide inhibitors of the GP IIb/IIIa receptor, respectively, and have a much smaller molecular weight compared to abciximab. These agents have reversible binding of the GP IIb/IIIa receptor.
Although GP IIb/IIIa inhibitors have demonstrated a significant reduction in MACE in several trials, the majority of these trials were conducted before dual antiplatelet therapy (DAPT) became standard of care and before the more potent P2Y12 inhibitors, prasugrel and ticagrelor, were available. Contemporary trials of GP IIb/IIIa inhibitors suggest that there may still be a benefit in ACS patients receiving DAPT with clopidogrel who present with an elevated troponin. (30) However, the ability of GP IIb/IIIa inhibitors to reduce MACE in patients receiving prasugrel or ticagrelor remains unknown. Trials comparing a strategy of GP IIb/IIIa inhibitors plus heparin to bivalirudin alone in patients with ACS undergoing PCI demonstrated no difference in MACE, but significantly less major bleeding with bivalirudin alone. (31,32) While these trials have many limitations, the routine use of GP IIb/IIIa inhibitors has declined significantly over the last decade. Patients with NSTE-ACS undergoing an ischemia-driven approach do not derive benefit from GP IIb/IIIa inhibitors and these agents should not be used in these patients. (3) Patients with STEMI receiving reperfusion with fibrinolytics have significant increases in major bleeding and ICH when GP IIb/IIIa inhibitors are used concomitantly and they should be avoided in these patients as well. (2) Despite reduced use, guidelines still support the use of GP IIb/IIIa inhibitors in PCI for NSTE-ACS patients with elevated cTn (e.g., suffering MI), or in STEMI patients who have not been preloaded with a P2Y12 inhibitor and are not being treated with bivalirudin. Guidelines also state that it is reasonable to use a GP IIb/IIIa inhibitor in patients who are preloaded with clopidogrel. (2,3,27) Glycoprotein IIb/IIIa inhibitors should always be given with unfractionated heparin (UFH) or a low molecular weight heparin (LMWH) that should be discontinued immediately following the PCI procedure to reduce risk of major bleeding. In addition to bleeding, GP IIb/IIIa inhibitors can also cause significant thrombocytopenia in about 1% of patients receiving abciximab and 0.5% with eptifibatide and tirofiban. (33)
Cangrelor is an intravenously administered P2Y12 inhibitor and the only other IV antiplatelet option other than GP IIb/IIIa inhibitors. Similar to ticagrelor, cangrelor is a reversible inhibitor of the P2Y12 receptor. Despite currently recommended loading doses, oral P2Y12 inhibitors take a minimum of 1 to 2 hours to obtain maximum platelet inhibition, and 3 to 7 days for platelet recovery after discontinuation. (34) Cangrelor has a rapid onset and offset, achieving maximum platelet inhibition within approximately 2 minutes of an IV bolus dose, with restoration of normal platelet reactivity within 1 to 2 hours of cessation of the infusion. Cangrelor has an elimination half-life of less than 9 minutes and is eliminated by ATPases in the blood making it an attractive agent to use in patients with either hepatic or renal dysfunction. (34) The fast return to normal platelet function may provide safety advantages for cangrelor over other P2Y12 inhibitors in the context of bleeding or transition to CABG surgery.
Where cangrelor fits into the treatment of ACS patients is not well defined. Current scientific evidence suggests that cangrelor at 48 hours after PCI provides a significant reduction in MACE with an increase in minor bleeding, but not major bleeding, compared to an oral strategy involving clopidogrel initiated in the catheterization laboratory during PCI (i.e. not pre-loaded). (35) The utility of cangrelor in patients pre-loaded with clopidogrel though is unknown, as is how it might compare to faster acting and more potent prasugrel and ticagrelor. As such, the clinical uptake of cangrelor has been limited but at minimum provides a reasonable option for use in patients with significant renal dysfunction since abciximab has become unavailable. An important clinical consideration with cangrelor is that it may interfere with binding of the active metabolites of clopidogrel and prasugrel to the site of action on platelets. Studies have demonstrated that when clopidogrel is given with cangrelor, the ability of the thienopyridines to irreversibly inhibit platelet function was reduced. (36,37) The postulated mechanism is that cangrelor directly prevents binding of the short-lived, but irreversible active metabolites of clopidogrel and prasugrel. Therefore, it is important that if cangrelor is used, the loading dose of clopidogrel or prasugrel not be given until the cangrelor infusion has been discontinued. This interaction does not exist with ticagrelor.
Injectable Anticoagulants
As discussed previously, anti-platelets are a cornerstone for both the acute and long term management of patients with ACS. However, inhibition of the coagulation cascade does have a role in the management of these patients. (2,3) Currently available injectable anticoagulants inhibit the production of thrombin by inhibiting factor Xa, inhibiting thrombin itself, or a combination of these. While the use of oral anticoagulants may be common for other thromboembolic disease states, all of the current evidence in the acute management of ACS is with injectable agents.
Unfractionated heparin has been widely used in the management of patients with ACS for several decades. UFH binds to the endogenous anticoagulant antithrombin (AT) via a unique pentasaccharide sequence, increasing its affinity for clotting factor inhibition by 1000-fold. (38) These UFH-AT complexes can then inhibit clotting factors IXa, Xa, XIa, XIIa, and thrombin, with most of the impact provided through inhibition of factor Xa and thrombin. Despite being used for many years in ACS, the anticoagulant effect of UFH is highly variable for a variety of reasons necessitating routine monitoring of the anticoagulant effect and dose adjustment. (38) Monitoring of the anticoagulant effect can be done with the activated partial thromboplastin time (aPTT) or heparin levels (measure of anti-factor Xa activity). In either case, the anticoagulant effect should be measured every 6 hours until two consecutive readings are within the therapeutic range, as determined by the individual institutional protocols, then every 24 hours for the duration of UFH therapy. Platelet counts should also be monitored daily or every other day to monitor for the occurrence of heparin induced thrombocytopenia (HIT). (38) Unfractionated heparin can be used across the spectrum of ACS and regardless of the management strategy. (2,3) The recommended dose of UFH is an IV bolus of 60 units/kg (initial maximum total dose of 4000 units) and an initial infusion rate of 12 units/kg/hour (initial maximum 1000 units/hour). In a meta-analysis of six trials (N=1,353) comparing the use of heparin plus aspirin to aspirin alone in patients with NSTE-ACS, the risk of death or MI was reduced by 33% in heparin-treated patients. (39) Because of the long-standing experience and use of UFH in patients with ACS, it has been the standard-of-care comparison in clinical trials.
Similar to UFH, LMWHs must first bind to AT to provide their anticoagulant activity. Low molecular weight heparins are created through chemical or enzymatic depolymerization of UFH molecules. (38) Compared to UFH, LMWHs provide a predicable anticoagulant dose response with no need for routine therapeutic monitoring. While most patients receiving a LMWH do not require therapeutic monitoring, an anti-Xa (or LMWH) level may be desired in certain patient populations such as pregnancy, obesity (>190 kg), and patients with severe renal insufficiency (e.g., creatinine clearance [CrCl] less 30 mL/min). (38) There is also a lower incidence of HIT with the use of LMWH (<2%) compared to UFH (2-5%). Even though the risk of HIT is lower with LMWH, monitoring platelet counts is still warranted. (40) While other LMWHs are available, enoxaparin is the most widely studied agent in patients with ACS, and is the only LMWH recommended in the American College of Cardiology/American Heart Association (ACC/AHA) guidelines. (2,3) Data supporting the use of enoxaparin exist in patients with NSTE-ACS and STEMI regardless of the management or reperfusion strategy used. Unfortunately, the dosing of enoxaparin varies across these different settings, requiring careful attention to ensure the right dose is used in the right patient to maximize efficacy and safety. In patients with NSTE-ACS undergoing an ischemia-driven approach, use of subcutaneous (SQ) enoxaparin at 1 mg/kg every 12 hours for up to three days is recommended. In ACS patients who undergo PCI, a supplemental dose of 0.3 mg/kg intravenously (IV) should be given if the patient has received less than 2 doses, or has received their last dose 8-12 hours ago. (3,41) Patients with a CrCl <30 mL/min should receive enoxaparin 1 mg/kg every 24 hours SQ instead of every 12 hours. For STEMI patients receiving reperfusion with fibrinolytics, enoxaparin should be dosed at 30 mg IV bolus followed immediately by 1 mg/kg subcutaneously every 12 hours. Patients ≥ 75 years (no bolus, 0.75 mg/kg every 12 hours) and those with a CrCl <30 mL/min (dosing interval once daily) should receive adjusted doses to minimize the risk of bleeding. Patients undergoing primary PCI for STEMI can receive a single IV dose of 0.5 mg/kg of enoxaparin.
Fondaparinux is a synthetic molecule comprising only the five saccharides needed to bind to and potentiate the activity of AT. (38) Fondaparinux only inhibits factor Xa and has no activity against thrombin. Similar to LMWH, fondaparinux also provides a predictable anticoagulant dose response and no need for therapeutic monitoring. (38) Although off-label, fondaparinux has been extensively studied and is dosed as 2.5 mg subcutaneously once daily in ACS. Fondaparinux is contraindicated in patients with a CrCl <30 mL/min due to the significant degree of renal elimination. Several large trials have evaluated the use of fondaparinux in ACS patients. (42,43) The trial in NSTE-ACS patients compared fondaparinux with enoxaparin, showing similar efficacy results with significantly less major bleeding in patients receiving fondaparinux. (42) The trial utilizing fondaparinux in STEMI evaluated patients receiving reperfusion with either fibrinolytics or primary PCI. In this trial, fondaparinux was compared to UFH. (93) Again, similar efficacy results were achieved with a lower risk of bleeding in the fondaparinux groups. An important finding in both trials was that there was a significant increase in catheter-related thrombosis if they received fondaparinux compared to enoxaparin. (93) Due to this concern, supplemental doses of IV UFH must be given if a patient receiving fondaparinux requires PCI. (3) These results typically relegate fondaparinux to managing patients who are not undergoing PCI for their ACS event.
Bivalirudin is an intravenously administered direct thrombin inhibitor that has only been evaluated in patients experiencing ACS who are also undergoing PCI and is therefore limited to those patient populations. (2,3,38) In a NSTE-ACS trial, patients were randomized to a heparin derivative (UFH or enoxaparin) with a GP IIb/IIIa inhibitor, bivalirudin with a GP IIb/IIIa inhibitor, or bivalirudin alone. (44) There was no difference in efficacy or safety in patients receiving a heparin with a GP IIb/IIIa inhibitor compared to bivalirudin with a GPII/IIIa inhibitor. As a result, due to the lack of benefit and increased cost associated with the combination of bivalirudin and a GP IIb/IIIa inhibitor, this regimen is not recommended in patients with NSTE-ACS undergoing PCI. Patients receiving bivalirudin alone demonstrated similar efficacy, but significantly less major bleeding compared to a heparin with a GP IIb/IIIa inhibitor. Similar to the study in NSTE-ACS, bivalirudin alone demonstrated similar efficacy with significantly less major bleeding compared to UFH with a GP IIb/IIIa in patients undergoing primary PCI for STEMI. (45) Additional investigations in recent years suggest that bivalirudin does not offer efficacy or safety benefits over UFH alone in the setting of primary PCI for STEMI, particularly as vascular access to perform PCI has moved from a predominantly femoral arterial approach associated with higher rates of bleeding to radial artery approach associated with less bleeding. (46, 47, 48) While the role of bivalirudin in these patients is recommended in the guidelines, many clinicians have reverted back to using primarily UFH due to cost.
Oral Antiplatelet Therapy
Aspirin
Aspirin has been a cornerstone in the treatment of ACS for several decades. Aspirin exerts its antiplatelet effect by acetylating a hydroxyl group of serine 530 on the cyclooxygenase (COX)-1 enzyme on platelets, and thereby preventing the conversion of arachidonic acid into thromboxane A2. (49) Thromboxane A2 produces platelet activation as well as vasoconstriction. While unbound aspirin has a half-life of only about 15-20 minutes, the irreversible binding of aspirin to the platelet COX-1 enzyme inhibits thromboxane A2-induced platelet activation for the life of the platelet (7-10 days).
Aspirin is recommended for all patients with ACS provided there are no contraindications. The initial dose of aspirin should be 162-325 mg (non-enteric coated) given as soon as possible. Patients undergoing PCI for NSTE-ACS or STEMI already receiving chronic aspirin doses of 81 mg daily should be given an additional dose of 81-325 mg before the procedure. (2,3) Subsequently, daily doses of aspirin should be 81 mg daily and continued indefinitely. Clinical trials have demonstrated that higher daily doses of aspirin do not provide additional clinical benefit, but do increase the risk of bleeding. (50) Contraindications to aspirin include a hypersensitivity to aspirin and major GI intolerance. In these rare cases, clopidogrel with a loading dose followed by a maintenance dose should be used as an alternative. (2,3) The main adverse effects of aspirin include dyspepsia and GI bleeding, and the use of low-dose and/or enteric-coated aspirin can reduce the risk of these. Although most surgical procedures can be conducted with patients on aspirin, it should be discontinued approximately 5 days before the procedure if requested.
P2Y12 inhibitors-general
Single antiplatelet therapy (SAPT) with aspirin for the management of ACS evolved in the early 2000’s to a combined approach with an oral P2Y12 inhibitor as part of DAPT. There are currently three orally administered P2Y12 inhibitors (clopidogrel, prasugrel, and ticagrelor) available on the U.S. market. Clopidogrel and prasugrel are thienopyridines and prodrugs that are metabolized to their active forms. Once activated, they bind to the P2Y12 receptor preventing the receptor’s ability to be activated by adenosine diphosphate and subsequent platelet activation and aggregation. (49) Ticagrelor is not a thienopyridine nor a prodrug. Ticagrelor does not form an irreversible bond with the P2Y12 receptor like clopidogrel or prasugrel, but instead bind reversibly in a different location. With ticagrelor, adenosine diphosphate is allowed to bind to the P2Y12 receptor, but the signal is blocked and does not lead to platelet activation and aggregation. Bleeding risk in patients treated with a P2Y12 inhibitors undergoing major surgery is of concern. DAPT regimens containing any of the available P2Y12 receptor antagonists increases the risk of bleeding. (51,52) Consequently, clopidogrel and ticagrelor should be held for at least 5 days and prasugrel should be held for 7 days prior to elective surgery (e.g., CABG surgery). (2.3)
P2Y12 inhibitors-Clopidogrel
The activation of clopidogrel to its active moiety requires two cytochrome P450(CYP) enzymatic steps. (49) While multiple CYP enzymes take part in this conversion, CYP2C19 is responsible for a majority of this conversion. Importantly, it is now understood there is underlying genetic variability with this enzyme. Patients with loss of functional alleles (*2 or *3) have a reduced ability to convert clopidogrel to its active form and have less platelet inhibition compared to patients with wild-type CYP2C19 (*1). Approximately 40% of patients receiving clopidogrel fail to achieve an optimal antiplatelet effect, with these patients having a higher risk of MACE compared to full responders. (53) Although we now have a better understanding of the genetic polymorphisms of CYP2C19 and how they contribute to the inadequate response to clopidogrel, CYP2C19 status only explains 12-15% of the variability in anti-platelet effect seen with clopidogrel. (53) Supporting the complexity behind the antiplatelet response to clopidogrel, clinical trials have not demonstrated improved CV outcomes in patients receiving genetic or platelet function testing. (2,3) Since proton pump inhibitors are known inhibitors of CYP2C19, there is also concern that the use of clopidogrel increases the risk for MACE in patients receiving these agents. While the clopidogrel labeling information lists omeprazole and esomeprazole as being contraindicated, clinical evidence supporting this interaction is inconsistent. (53) Despite these potential limitations, the clinical trial evidence of the use of clopidogrel in ACS is robust. The CURE trial (Clopidogrel in Unstable Angina to Prevent Recurrent Events) compared aspirin alone to clopidogrel given as a 300 mg loading dose, followed by 75 mg daily for up to 12 months plus aspirin. (54) Patients receiving DAPT demonstrated a significant reduction in CV death, MI, and stroke compared to aspirin alone. This trial not only demonstrated the efficacy of clopidogrel, but also established DAPT as the standard of care for patients presenting with ACS. Subsequent trials demonstrated the value of a 600 mg clopidogrel loading dose providing a more rapid onset of antiplatelet activity. (55) A 600 mg loading dose for clopidogrel should definitely be used in patients undergoing PCI for NSTE-ACS and STEMI. Finally, clopidogrel is the only P2Y12 inhibitor to be evaluated in large clinical trials in patients with STEMI receiving reperfusion with fibrinolytic therapy. Two trials have demonstrated the efficacy and safety of clopidogrel as part of DAPT in these patients. (56, 57) Due to the increased concern of ICH in patients receiving fibrinolytics, only a 300-mg loading dose of clopidogrel is used, and patients ≥75 years do not receive any loading dose.
P2Y12 inhibitors-Prasugrel
Although prasugrel must also be converted to an active compound, the stepwise process is not subject to variability and hence is more consistent and efficient than clopidigrel. (58) As such, prasugrel (dosed as a 60 mg load, followed by a 10 mg daily maintenance dose) compared to clopidogrel provides a more rapid and complete anti-platelet effect. A major clinical trial comparing prasugrel to clopidogrel as part of DAPT with aspirin in patients undergoing PCI for NSTE-ACS or STEMI there was a significant reduction in CV death, MI, or stroke with prasugrel compared to clopidogrel. (59) The benefit was observed both in the first few days of the trial, as well as over the longer term. The increase in efficacy did not come without risks though, and an increase in non-CABG major bleeding and fatal bleeding was observed with prasugrel. Patients with a history of stroke or transient ischemic attack were at greater risk for harm from prasugrel, and therefore, these patients have an absolute contraindication to receiving prasugrel. In addition, prasugrel patients ≥75 years and those weighing <60 kg experienced more bleeding, but the overall net clinical benefit was neutral. Prasugrel is typically avoided in patients ≥75 years while in patients weighing <60 kg, a 5-mg maintenance dose is recommended instead of the typical 10-mg dose to minimize the risk of bleeding. Prasugrel has been compared to clopidogrel in patients undergoing an ischemia-driven approach. (60) Although there was no increased risk of bleeding with prasugrel in this trial, there was also no difference in efficacy and hence is not guideline recommended. (3) Prasugrel has also not been evaluated in patients with STEMI receiving reperfusion therapy with fibrinolytics.
P2Y12 inhibitors-Ticagrelor
Compared to clopidogrel, ticagrelor provides faster and more potent inhibition of platelets similar to prasugrel. (61) Unlike clopidogrel and prasugrel which are cleared from the plasma quickly, ticagrelor is metabolized by CYP3A4. Practitioners therefore must be aware of significant drug-drug interactions. Ticagrelor is contraindicated in patients receiving strong CYP3A4 inhibitors such as azole antifungals and protease inhibitors, as well as strong inducers of this enzyme such as carbamazepine, phenytoin, rifamycins, and St. John’s Wort. Patients on ticagrelor should not receive doses of simvastatin or lovastatin higher than 40 mg daily. Due to competition for P-glycoprotein, ticagrelor can increase digoxin concentrations by 30-50%. (61)
Ticagrelor (dosed as a 180 mg loading dose, then 90 mg twice daily) has been compared to clopidogrel as part of DAPT with aspirin in patients undergoing PCI (NSTE-ACS or STEMI) or undergoing an ischemia-driven approach for NSTE-ACS in a large clinical trial (n=18,624). (62) Significant reductions in CV death, MI, or stroke were observed with ticagrelor compared to clopidogrel. Ticagrelor provided a benefit over clopidogrel both in the early phase of the trial, as well as out to 1 year. This is a similar scenario seen with prasugrel whereas the benefit of ticagrelor was not simply due to more potent antiplatelet therapy early, but also sustained potent antiplatelet therapy over time leading to both short-term and long-term benefits. Distinct from prasugrel, ticagrelor demonstrated a significant benefit in patients receiving an ischemia-driven approach compared to those receiving PCI. Also unique to ticagrelor, there was a significant reduction (21%) in CV mortality with the use ticagrelor compared to clopidogrel. (62) When ticagrelor is used as part of DAPT for ACS, the dose of aspirin (ASA) should not exceed 100 mg daily. In the trial, higher doses of aspirin attenuated the benefit of ticagrelor compared to clopidogrel, and only patients receiving low-dose aspirin (daily dose of 100 mg or less) received benefit. (63) Similar to prasugrel though, increased efficacy was accompanied by an increased risk of non-CABG major bleeding. While ticagrelor has been found to be noninferior to clopidogrel for major bleeding risk in patients with STEMI receiving reperfusion with fibrinolytics, clopidogrel is the only P2Y12 inhibitor with specific recommendations as an adjunct to fibrinolytic therapy in patients with STEMI. (64) Additional considerations that practitioners should be aware of with ticagrelor are the unique adverse effects other than bleeding. Ticagrelor patients experienced more dyspnea (13.8%) compared to those receiving clopidogrel (7.8%) in clinical trials. (62) While the occurrence can be initially alarming, patients should be educated that the symptoms are typically mild to moderate, require no specific therapy or work up, and usually dissipate within 2-4 weeks. Use of ticagrelor was also associated with an increase in asymptomatic ventricular pauses, increases in uric acid, and small increases in serum creatinine.
Switching antiplatelet agents
As P2Y12 inhibitors have been integrated into clinical practice, clinicians are often faced with scenarios that switch patients from one agent to a different agent. In some scenarios an escalation of therapy is needed from clopidogrel to a more potent P2Y12 inhibitor such as ticagrelor or prasugrel. Causes for escalation may include a heightened risk for coronary event or stent thrombosis, development of drug interaction, intolerance or nonadherence to a particular agent, identification of a genetic polymorphism to clopidogrel or confirmation of inadequate platelet inhibition. In reverse, patients may need or undergo de-escalation from a more potent P2Y12 inhibitor to clopidogrel. Causes of de-escalation of P2Y12 inhibitor may include bleeding, a new indication for concomitant use with an oral anticoagulant, or in cases of nonadherence because of the cost of prolonged therapy. Data on the safety and efficacy on switching agents are limited and primarily based on pharmacodynamic studies. Clinical decisions based on the reason for switching (i.e. escalation versus de-escalation) and the timing from index event (i.e. acute/early phase within the first 30 days versus later) must be weighed. International consensus recommendations for de-escalating therapy highlight the need to balance ischemic risk and bleeding risk in individual patients when considering a loading dose of the new P2Y12 for different clinical situations. (65) De-escalation from ticagrelor to other P2Y12 inhibitors should not require a loading dose. (65) Escalations in therapy should be accompanied by a loading dose of the new agent regardless of time of last P2Y12 inhibitor dose, followed by maintenance therapy 24 hours after last P2Y12 inhibitor dose. (65) If clinically feasible, any switch should occur 24 hours after the last dose of the previous P2Y12 inhibitor. (65)
CASE 3
J.W. is a 65-year-old Latino man who presents to the ED with chest tightness and shortness of breath. He gives a history of similar symptoms the prior day that lasted 20 minutes. He was given aspirin 325 mg, intranasal oxygen, IV metoprolol tartrate, and started on an IV NTG infusion, which was increased to 80 mcg/minute; at that time, his BP was 110/60 mmHg, and his heart rate was 88. His ECG revealed segment depression in the anterior leads. His shortness of breath was relieved, but he still complained of chest tightness. His past medical history includes hypertension for which he takes hydrochlorothiazide 25 mg daily. He has smoked a pack of cigarettes per day for the past 30 years. Laboratory values include Na, 135 mEq/L; K, 4.0 mEq/L; Cl, 100 mEq/L; CO2, 20 mEq/L; BUN, 15 mg/dL; SrCr, 1.3 mg/dL; glucose, 100 mg/dL; Mg, 2 mEq/L; and troponin-I, 0.5 ng/mL (normal, <2). Based on his symptoms and ECG, the diagnosis is presumed unstable angina.
CASE 3 QUESTIONS
- Is this patient a candidate for an intravenous antiplatelet agent such as a GP IIb/IIIa inhibitor or cangrelor?
- What options are there for acute anticoagulation for this patient for ACS?
- What P2Y12 receptor antagonist would you recommend for this patient, and for what duration?
PAUSE AND REFLECT: Assess case based on content thus far, then listen to faculty commentary.
|
Secondary Prevention in ACS
Secondary prevention of ischemic events
While the initial management of patients with ACS is important to stabilize the patient and improve outcomes, equally important is the use of evidence-based therapies to effectively prevent the progression of atherosclerosis and recurrent ischemic events. As patients now have established atherosclerotic cardiovascular disease (ASCVD) after an ACS event, effective secondary prevention strategies typically include anti-ischemic, antiplatelet, lipid-lowering, and antihypertensive therapies. (2,3,21) These interventions should be initiated prior to hospital discharge and patients should be educated about the benefits of these interventions. A systematic process should be in place to ensure patients leave the hospital on DAPT, a beta-blocker, an angiotensin converting enzyme (ACE) inhibitor or angiotensin receptor blocker (ARB), and statin therapy unless a contraindication exists. (2,3) In addition, short-acting NTG should be prescribed as needed for any subsequent episode of acute angina for patients not taking phosphodiesterase-5 inhibitors. Select patients may also benefit from an aldosterone antagonist. Aggressive risk factor modification strategies should always be the cornerstone of any secondary prevention strategy. Patients should understand the importance and benefits of increased physical activity, dietary modification, weight loss, blood pressure modification and smoking cessation, which should be, initiated, and continued indefinitely. (66) Proton pump inhibitors provide a protective benefit in patients at highest risk for GI bleeding from DAPT and may be considered for select patients (e.g., history of GI bleeding, triple therapy with DAPT and an oral anticoagulant with or without a history of GI bleeding). (3) All patients should refrain from chronic use of nonsteroidal anti-inflammatory drugs with high degree of cyclo-oxygenase-2 selectivity as they are associated with increased cerebrovascular and cardiovascular events. (2,3)
Cholesterol management-Statins
Landmark clinical trials have unequivocally demonstrated the value of statins in secondary prevention following MI and provide an approximate 1% reduction in risk of ASCVD event per 1% reduction in low-density lipoprotein cholesterol (LDL-C) over time. (67) Furthermore, there is a benefit of high-intensity statins initiated 1–10 days after ACS presentation. As such, a high-intensity statin should be initiated during the index hospitalization once the patient has been stabilized and continued indefinitely. If patients are taking low- or moderate-intensity statin therapy at time of ACS presentation, they should be moved to a high-intensity statin. Patients ≥75 years are an exception as a moderate-intensity statin may be needed to reduce the risk of adverse effects. (67)
Cholesterol management-Other cholesterol-lowering therapies
Some non-statin therapies have been shown to lower the risk of MACE in patients with ACS already on statin therapy. The IMPproved Reduction of Outcomes: Vytorin Efficacy International Trial (IMPROVE-IT) study compared the combination of simvastatin and ezetimibe, a non-statin, to moderate-dose simvastatin in patients with recent (within 10 days) ACS and an LDL-C level between 50-100 mg/dL. (68) At seven years, there was a modest reduction (6.4% relative risk reduction) in the rate of MACE in the simvastatin/ezetimibe group compared to simvastatin alone. More recently the proprotein convertase subtilisin-kexin type 9 (PCSK9) inhibitors has also been shown to lower the risk of MACE in patients with ACS. Trials have demonstrated the addition of a PCSK9 to a statin in ACS patients leads to further LDL-C reduction by approximately 60% and the risk of MACE at four years by 15% compared to high-intensity statin therapy alone. (69)
ACE inhibitors or ARBs
A large body of scientific evidence supports the use of angiotensin converting enzyme (ACE) inhibitors post-MI. ACE inhibitors reduce mortality, reinfarction rates, and HF through prevention of adverse cardiac remodeling. (2,3,70,71) Early administration (within 48 hours of presentation) of ACE inhibitors is associated with the strongest benefit. These agents provide the greatest benefit in patients with left ventricular dysfunction (LVEF ≤40%) or in those who developed HF symptoms in the early phase of ACS. (70) Because they have been shown to have comparable benefit to ACE inhibitors in patients with MI, an angiotensin II receptor blocker (ARB) may be prescribed for those who cannot tolerate an ACE inhibitor. (72)
Aldosterone Antagonists
Adding an aldosterone antagonist (eplerenone or spironolactone) in addition to an ACE inhibitor and beta-blocker has been demonstrated to lead to additional improvements in morbidity and mortality. (2,3) Patients should have LVEF ≤40% and either HF symptoms or DM, adequate renal function and a normal serum potassium in order to be considered for an aldosterone antagonist. (2,3,73) The mechanism of benefit is likely further reductions in myocardial remodeling beyond what can be achieved with an ACE inhibitor and beta-blocker.
Antithrombotic therapy-Duration of Dual Antiplatelet Therapy (DAPT)
Dual antiplatelet therapy as a treatment paradigm involves both the rapid initiation of a P2Y12 agent with ASA in the acute management of ACS, but also historically involved continuing DAPT for a 12-month duration. This recommendation was based on initial studies with clopidogrel, and subsequent trials with newer agents, prasugrel and ticagrelor, that demonstrated a 12-month time frame reduced the risk of recurrent ischemic events. Furthermore, patients who stopped DAPT prematurely have been shown to have a significantly increased risk of recurrent cardiac events. As such, ACS guidelines have traditionally recommended a 12-month duration for DAPT for any ACS patient. (2,3,74) In the past several years, multiple trials have investigated whether the 12-month duration for DAPT can be either shortened, or lengthened depending on the specific patient. The ACC/AHA have recently published guidelines incorporating this new evidence and provide patient specific recommendations related to dosing, initiation, and duration of DAPT after ACS, including situations when therapy should be discontinued. (2,3,74) A shorter duration of DAPT may be considered in patients with a lower ischemic risk who may have a high bleeding risk. Conversely, longer durations of DAPT may be reasonable in patients at higher ischemic risk if bleeding risk is not unacceptably high. Two separate randomized controlled trials support this general approach.
The DAPT trial was a randomized comparison of the standard 12-month duration or DAPT compared to a 30-month duration in patients who had PCI with intracoronary stenting for either stable ischemic heart disease (SIHD) or ACS. Most patients (65%) enrolled in this study were administered clopidogrel while a minority were treated with prasugrel (35%); ticagrelor was not used. Overall, continuing DAPT out to 30 months did result in reductions of MACE, in particular the risk of recurrent MI and stent thrombosis, compared to the standard 12-month duration. One of the most important results from the DAPT trial is the development of the DAPT score, which allows for individual risk prediction of the balance of recurrent ischemic and bleeding events when DAPT is continued beyond 12 months. Details of the DAPT score can be found in Table 3. A risk score of two or more suggests that prolonging therapy is favorable and would reduce ischemic events with perhaps only a modest increase in bleeding risk. Conversely, for those with a DAPT less than two, the risk for bleeding is anticipated to be greater than an ischemic benefit and the P2Y12 inhibitor should be discontinued. It is important to realize that the DAPT score was developed from a study comparing standard DAPT (12 months) to an extended duration of 30 months of therapy in patients who had PCI with intracoronary stenting for either SIHD or ACS and is not appropriate for determining DAPT durations shorter than 12 months. (74,75)
| Table 3. Factors used to calculate DAPT score and predict ischemic and bleeding events. (74,75) |
|
Points
|
+2
|
+1
|
-1
|
-2
|
|
Clinical variables
|
CHF or LVEF ≤30%
Saphenous vein graft PCI
|
Current tobacco user
Diabetes mellitus
NSTEMI or STEMI at presentation
Prior MI or PCI
Stent diameter less than 3 mm
Paclitaxel-eluting stent
|
Age 65 to 74
|
Age ≥75 years
|
| Risk factors ordered from left to right include those with highest ischemic risk and highest point accrual to those with the highest bleeding risk and negative point accrual. A score of ≥2 favors prolonged DAPT; a score of <2 is of unfavorable risk/benefit. Total score ranges from -2 to 10. |
Continued use of DAPT with ticagrelor beyond 12 months after ACS can be considered. One trial (Pegasus TIMI-54) compared standard-dose ticagrelor to a reduced dose of 60 mg twice daily in combination with low-dose aspirin to aspirin alone in patients who had suffered an MI one to three years prior. (76) This study demonstrated continued DAPT with either dose of ticagrelor decreased the composite of CV death, MI, or stroke compared to aspirin alone. While major bleeding was increased in patients treated with ticagrelor compared to aspirin alone, there were fewer bleeds in the low-dose ticagrelor group compared to the standard dose. It is important to note that the lower dose of ticagrelor (60 mg twice daily) has not been studied in the first 12 months after ACS; therefore, only the 90 mg twice daily is appropriate for the first year after index event. Regardless, this second trial supports the concept that some patients may likely benefit from longer durations of DAPT. Several sub-analyses have been presented adding further information which can help determine who may be an appropriate candidate for longer duration DAPT with ticagrelor. One analysis found that the benefits of restarting DAPT in the Pegasus TIMI-54 trial were present regardless of whether the patient received PCI or not as part of their treatment strategy for their qualifying MI event. (77) Another important sub-analysis assessed whether clinical characteristics predicting bleeding (anemia at baseline, prior hospitalization of bleeding) and thrombosis (recent P2Y12 use within 1 year, MI <2 years prior, chronic kidney disease, multiple prior MIs) could identify subgroups of patients who derive benefit with extended DAPT using ticagrelor. (78) In patients who had no risk factors for bleeding but 2 or more ischemic risk factors, the benefit of extended DAPT was substantial with a minimal increased risk of bleeding. (78)
Additional guidance on DAPT in ACS includes that for patients with STEMI treated with fibrinolysis, the minimum recommended duration of DAPT is 14 days. (2, 74) Every patient receiving DAPT should understand the benefit as well as risks associated with the therapy and the importance of maintaining adherence with therapy for the appropriately duration of therapy.
Antithrombotic therapy-Management of DAPT in Patients with Atrial Fibrillation
The management of patients who have atrial fibrillation and then undergo PCI plus stent implantation has challenged clinicians for a number of years. Overall, it is estimated that 1 in 5 patients with atrial fibrillation will undergo PCI or have an ACS event. As such, this scenario is one that clinicians will commonly face. Dual antiplatelet therapy is essential, of course, for preventing platelet mediated coronary events, especially stent thrombosis. But, in patients with atrial fibrillation, therapeutic anticoagulation is superior to DAPT for the prevention of stroke. Initially, the approach to these patients was to prescribe both DAPT plus an oral anticoagulant, triple therapy. However, the use of triple therapy substantially increases the risk of bleeding. Hence, there have been significant research efforts to identify an antithrombotic approach that will maintain efficacy for the prevention of both coronary events and stroke, while reducing the risk of bleeding. (79) We now have multiple randomized controlled trials that support an alternative approach to the management of these patients. (80, 81, 82) In each of these trials, the use of a dual antithrombotic approach (oral anticoagulation with a direct oral anticoagulant [DOAC] plus single antiplatelet therapy with clopidogrel) significantly reduced the risk of bleeding compared to triple therapy while maintaining efficacy in the prevention of coronary and cerebrovascular events. This approach calls for the removal of aspirin from the chronic antithrombotic regimen. The challenging question that remains is when should the ASA be removed from the patient? In a patient at a low risk of thrombotic events (elective PCI without high risk features for thrombosis and/or high risk of bleeding), early omission of ASA and treatment with just an oral anticoagulant plus clopidogrel makes sense. However, in patients undergoing complex, multivessel, or high-risk PCI or in those presenting with ACS, triple therapy should probably be used for a minimum of 1 month and then re-evaluated as to whether ASA can be dropped from the regimen at that time. (79) Importantly, none of the trials evaluating a dual therapy approach for atrial fibrillation patients undergoing PCI used either ticagrelor or prasugrel. As such, clopidogrel should still remain the preferred P2Y12 antagonist for these patients.
Medication Adherence, Transitions of Care and Shared Decision Making
As important as ensuring that patients are prescribed appropriate pharmacotherapy during and after an ACS event, equally important is whether patients can be adherent to their prescribed pharmacotherapy regimen. Despite evidence to support mortality reduction with secondary prevention strategies, typically less than 50% of patients remain adherent at 1 year after an ACS event. (83) Because nonadherence with secondary prevention medications following ACS leads to poor CV outcomes, it is paramount that patients receive thorough medication counseling (including counseling prior to hospital discharge) and be monitored for medication persistence. (2,3,84) Counseling should include assessments of health literacy level, barriers to adherence, access to medications, and understanding of instructions. (84) Additionally, patients and their caregivers should be provided written and verbal instructions about the purpose of each medication, changes to previous medication regimen, optimal time to take each medication, new allergies or medication intolerances, need for timely prescription fill after discharge, anticipated duration of therapy, consequences of nonadherence, common and/or serious adverse reactions that may develop, and drug–drug and drug–food interactions. (84) Early follow up (within 6 weeks) after discharge has been associated with improved medication adherence and, for this reason, post-discharge follow up is often scheduled within 1-2 weeks. (85)
The transition from an acute care setting to home is recognized as a challenging time for patients. (86,87) As many of these important interventions are being implemented in this high-risk period, patients may be challenged to adhere to secondary prevention therapies. This is especially true for patients with ACS who may be required to start multiple new medications at the same time they are being asked to make lifestyle changes (e.g., diet, exercise, smoking). (86,87) Pharmacists, whether in the acute care setting, ambulatory care setting or potentially the community setting, can play critical roles in providing patient education. In addition, they are uniquely suited to meet with patients to assess for potential reasons for nonadherence (cost, side effects, pill burden), and identify solutions to address nonadherence especially to life-saving medications. Lastly, they can serve in important roles within a transitions of care program to help patients smoothly and efficiently move from hospital to home. (88)
An important tool that pharmacists have at their disposal to help increase patient adherence to life saving interventions is shared decision making. Shared decision making is a process that increases the likelihood of patients receiving the care they need in a manner consistent with the best available research evidence and their values and preferences. (89) When prescribed therapy better aligns with patients’ preferences and values, adherence is more likely to happen. Essential components to a shared decision-making approach include:
- Define and explain the problem to the patient
- Present all potential options to the patients
- For each option, discuss the pros/cons and risks/benefits of each
- Identify key patient values and preferences
- Discuss with the patient their ability to care for themselves
- Provide knowledge to the patient if needed
- Check for understanding and clarify any issues at the end of the discussion
- Jointly make a decision with the patient or defer the decision to a later time
- Arrange for follow up
A key aspect to this process is presenting information at an appropriate level and in a manner that is understandable to the patient, which requires considering the patient’s underlying health literacy. For many patients, a pictograph may be the best way to communicate the pros/cons and risks/benefits for each potential option. One example can be found on page 331 of the Lin and Fagerlin article linked in the resource list.
Several reports in the literature have documented that using a shared decision-making approach in ACS/PCI helps increase patient knowledge about their overall risk, increases their engagement in their health, and can potentially improve outcomes and reduce health care resources. (90, 91, 92)
CASE 4
Recall our patient from Case #3, J.W. is a 65-year-old Latino man presents to the ED with chest tightness and shortness of breath. Patient has a past medical history of hypertension, hyperlipidemia, atrial fibrillation, and COPD. He has smoked a pack of cigarettes per day for the past 30 years. Laboratory values include Na, 135 mEq/L; K, 4.0 mEq/L; Cl, 100 mEq/L; CO2, 20 mEq/L; BUN, 15 mg/dL; SrCr, 1.3 mg/dL; glucose, 100 mg/dL; Mg, 2 mEq/L; and troponin-I, 0.5 ng/mL (normal, <2). Based on his symptoms and ECG, the diagnosis is presumed unstable angina.
CASE 4 QUESTIONS
- What secondary prevention options should be initiated for this patient to reduce the risk of further ischemic events?
- What should this patient’s chronic antithrombotic regimen consist of to manage the patient’s ACS event and also his atrial fibrillation? Does your answer change if the patient undergoes PCI plus stent placement as part of their ACS treatment?
- Assume the patient does not have atrial fibrillation, and needs DAPT therapy post ACS. How long should DAPT be continued in this patient?
- Which P2Y12 inhibitor would you recommend for this patient as part of DAPT? Does your answer change if atrial fibrillation is present or not? How could shared decision making be used to help select a P2Y12 inhibitor for the patient?
PAUSE AND REFLECT: Assess case based on content thus far, then listen to faculty commentary.
|
SUMMARY
For the majority of patients, the pathophysiology of ACS involves an acute disruption of an atherosclerotic plaque followed by platelet activation and aggregation and subsequent intracoronary thrombus formation. Myocardial ischemia ensues due to an acute imbalance between myocardial oxygen supply and demand and may lead to MI depending on the severity and duration of thrombotic occlusion. Therefore, the acute pharmacotherapeutic management of ACS is focused on antiplatelet, anticoagulation, and anti-ischemic therapies. Appropriate selection of these agents depends upon patient presentation (e.g., STEMI or NSTE-ACS), the decision for reperfusion (e.g., PCI, fibrinolysis, or no reperfusion), and individual considerations for efficacy and safety associated with individual agents (e.g., pharmacokinetic alterations, drug-drug interactions, contraindications). High-intensity statins should be initiated early and continued indefinitely for all patients with ACS without contraindications to lower LDL-C and stabilize atherosclerotic plaques. Long-term use of DAPT lowers the risk of MACE after ACS and maintains stent patency in patients who had intracoronary stent implantation during PCI. Although 12 months of DAPT is still the general recommendation, evolving evidence suggests that some patients may benefit from either shorter or longer durations of DAPT therapy. Neurohormonal blocking drugs such as β-blockers and inhibitors of the RAAS system are also associated with lower risk of MACE and should be initiated prior to hospital discharge in appropriate patients. The pharmacist plays an important role in the patient care process for ACS, collecting and analyzing clinical information, collaborating in the development and implementation of the care plan, and evaluating therapeutic outcomes. In addition, pharmacists are critical to helping patients adhere to life-saving medications.
Resources
Lin GA, Fagerlin A. Shared Decision Making: State of the Science. Circulation: Cardiovascular Quality and Outcomes. 2014;7:328-334. Available at https://www.ahajournals.org/doi/pdf/10.1161/CIRCOUTCOMES.113.000322.
REFERENCES
- Benjamin EJ, Virani SS, Callaway CW, et al. Heart disease and stroke statistics-2018 update: a report from the American Heart Association. 2018;137:e67-e492.
- O'Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines.J Am Coll Cardiol.2013;61:e78-140.
- Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines.J Am Coll Cardiol.2014;64:e139-e228.
- Levine GN, Bates ER, Blankenship JC, et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography andJ Am Coll Cardiol.2011;58:e44–122.
- Tickoo S, Bhardwaj A, Fonarow GC, Liang L, Bhatt DL, Cannon CP. Relation between hospital length of stay and quality of care in patients with acute coronary syndromes (from the American Heart Association's Get With the Guidelines—coronary artery disease data set).Am J Cardiol.2016;117:201-205.
- Sugiyama T, Hasegawa K, Kobayashi Y, Takahashi O, Fukui T, Tsugawa Y. Differential time trends of outcomes and costs of care for acute myocardial infarction hospitalizations by ST elevation and type of intervention in the United States, 2001-2011.J Am Heart Assoc.2015;4:e001445.
- Nicholson G, Gandra SR, Halbert RJ, Richhariya A, Nordyke RJ. Patient-level costs of major cardiovascular conditions: a review of the international literature.Clinicoecon Outcomes Res.2016;8:495-506.
- Ford TJ, Berry C, De Bruyne B, et al. Physiological predictors of acute coronary syndromes: emerging insights from the plaque to the vulnerable patient.JACC Cardiovasc Interv.2017;10:2539-2547.
- Crea F, Liuzzo G. Pathogenesis of acute coronary syndromes.J Am Coll Cardiol.2013;61:1-11.
- Libby P. Mechanisms of acute coronary syndromes and their implications for therapy.N Engl J Med.2013;368:2004-2013.
- Crea F, Libby P. Acute coronary syndromes: the way forward from mechanisms to precision treatment. 2017;136:1155-1166.
- Fuster V, Kovacic JC. Acute coronary syndromes: pathology, diagnosis, genetics, prevention, and treatment.Circ Res.2014;114:1847-1851.
- Furie B, Furie BC. Mechanisms of thrombus formation. N Engl J Med 2008;359:938-49.
- Reed GW, Rossi JE, Cannon CP. Acute myocardial infarction. 2017;389:197-210.
- Gabriel-Costa D. The pathophysiology of myocardial infarction-induced heart failure. 2018;25:277-284.
- Kline KP, Conti CR, Winchester DE. Historical perspective and contemporary management of acute coronary syndromes: from MONA to THROMBINS2.Postgrad Med.2015;127:855-862.
- McCarthy CP, Bhambhani V, Pomerantsev E, Wasfy JH. In-hospital outcomes in invasively managed acute myocardial infarction patients who receive morphine.J Interv Cardiol.2018;31:150-158.
- Kubica J, Kubica A, Jilma B, et al. Impact of morphine on antiplatelet effects of oral P2Y12 receptor inhibitors.Int J Cardiol.2016;215:201-208.
- Bangalore S, Makani H, Radford M, et al. Clinical outcomes with beta-blockers for myocardial infarction: a meta-analysis of randomized trials.Am J Med.2014;127:939-953.
- Freemantle N, Cleland J, Young P, Mason J, Harrison J. Beta blockade after myocardial infarction: systematic review and meta regression analysis. 1999;318:1730-1737.
- Smith SC, Jr., Benjamin EJ, Bonow RO, et al. AHA/ACCF secondary prevention and risk reduction therapy for patients with coronary and other atherosclerotic vascular disease: 2011 update: a guideline from the American Heart Association and American College of Cardiology Foundation endorsed by the World Heart Federation and the Preventive Cardiovascular Nurses Association.J Am Coll Cardiol.2011;58:2432-2446.
- Chen ZM, Pan HC, Chen YP, et al. Early intravenous then oral metoprolol in 45,852 patients with acute myocardial infarction: randomised placebo-controlled trial. 2005;366:1622-1632.
- Bagai A, Dangas GD, Stone GW, Granger CB. Reperfusion strategies in acute coronary syndromes.Circ Res.2014;114:1918-1928.
- Bagai A, Jollis JG, Dauerman HL, et al. Emergency department bypass for ST-Segment-elevation myocardial infarction patients identified with a prehospital electrocardiogram: a report from the American Heart Association Mission: Lifeline program. 2013;128:352-359.
- Ting HH, Krumholz HM, Bradley EH, et al. Implementation and integration of prehospital ECGs into systems of care for acute coronary syndrome: a scientific statement from the American Heart Association Interdisciplinary Council on Quality of Care and Outcomes Research, Emergency Cardiovascular Care Committee, Council on Cardiovascular Nursing, and Council on Clinical Cardiology. 2008;118:1066-1079.
- Langabeer JR, Henry TD, Kereiakes DJ, et al. Growth in percutaneous coronary intervention capacity relative to population and disease prevalence.J Am Heart Assoc.2013;2:e000370.
- Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC).Eur Heart J.2018;39:119-177.
- Antman EM, Cohen M, Bernink PJ, et al. The TIMI risk score for unstable angina/non-ST elevation MI: A method for prognostication and therapeutic decision making. 2000;284:835-842.
- Granger CB, Goldberg RJ, Dabbous O, et al. Predictors of hospital mortality in the global registry of acute coronary events.Arch Intern Med.2003;163:2345-2353.
- Kastrati A, Mehilli J, Neumann FJ, et al. Abciximab in patients with acute coronary syndromes undergoing percutaneous coronary intervention after clopidogrel pretreatment: the ISAR-REACT 2 randomized trial. 2006;295:1531-1538.
- Stone GW, McLaurin BT, Cox DA, et al. Bivalirudin for patients with acute coronary syndromes.N Engl J Med.2006;355:2203-2216.
- Stone GW, Witzenbichler B, Guagliumi G, et al. Bivalirudin during primary PCI in acute myocardial infarction.N Engl J Med.2008;358:2218-2230.
- Dobesh PP, Latham KA. Advancing the battle against acute ischemic syndromes: a focus on the GP IIb-IIIa inhibitors. 1998;18:663-685.
- Akers WS, Oh JJ, Oestreich JH, Ferraris S, Wethington M, Steinhubl SR. Pharmacokinetics and pharmacodynamics of a bolus and infusion of cangrelor: a direct, parenteral P2Y12 receptor antagonist.J Clin Pharmacol.2010;50:27-35.
- Bhatt DL, Stone GW, Mahaffey KW, et al. Effect of platelet inhibition with cangrelor during PCI on ischemic events.N Engl J Med.2013;368:1303-1313.
- Steinhubl SR, Oh JJ, Oestreich JH, Ferraris S, Charnigo R, Akers WS. Transitioning patients from cangrelor to clopidogrel: pharmacodynamic evidence of a competitive effect.Thromb Res.2008;121:527-534.
- Dovlatova NL, Jakubowski JA, Sugidachi A, Heptinstall S. The reversible P2Y antagonist cangrelor influences the ability of the active metabolites of clopidogrel and prasugrel to produce irreversible inhibition of platelet function.J Thromb Haemost.2008;6:1153-1159.
- Garcia DA, Baglin TP, Weitz JI, Samama MM. Parenteral anticoagulants: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. 2012;141:e24S-e43S.
- Oler A, Whooley MA, Oler J, Grady D. Adding heparin to aspirin reduces the incidence of myocardial infarction and death in patients with unstable angina. A meta-analysis. 1996;276:811-815.
- Linkins LA, Dans AL, Moores LK, et al. Treatment and prevention of heparin-induced thrombocytopenia: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. 2012;141:e495S-e530S.
- Ferguson JJ, Califf RM, Antman EM, et al. Enoxaparin vs unfractionated heparin in high-risk patients with non-ST-segment elevation acute coronary syndromes managed with an intended early invasive strategy: primary results of the SYNERGY randomized trial. 2004;292:45-54.
- Fifth Organization to Assess Strategies in Acute Ischemic Syndromes I, Yusuf S, Mehta SR, et al. Comparison of fondaparinux and enoxaparin in acute coronary syndromes.N Engl J Med.2006;354:1464-1476.
- Yusuf S, Mehta SR, Chrolavicius S, et al. Effects of fondaparinux on mortality and reinfarction in patients with acute ST-segment elevation myocardial infarction: the OASIS-6 randomized trial. 2006;295:1519-1530.
- Stone GW, McLaurin BT, Cox DA, et al. Bivalirudin for patients with acute coronary syndromes.N Engl J Med.2006;355:2203-2216.
- Stone GW, Witzenbichler B, Guagliumi G, et al. Bivalirudin during primary PCI in acute myocardial infarction.N Engl J Med.2008;358:2218-2230.
- Kastrati A, Neumann FJ, Mehilli J, et al. Bivalirudin versus unfractionated heparin during percutaneous coronary intervention.N Engl J Med.2008;359:688-696.
- Schulz S, Richardt G, Laugwitz KL, et al. Prasugrel plus bivalirudin vs. clopidogrel plus heparin in patients with ST-segment elevation myocardial infarction.Eur Heart J.2014;35:2285-2294.
- Shahzad A, Kemp I, Mars C, et al. Unfractionated heparin versus bivalirudin in primary percutaneous coronary intervention (HEAT-PPCI): an open-label, single centre, randomised controlled trial. 2014;384:1849-1858.
- Dobesh PP, Varnado S, Doyle M. Antiplatelet agents in cardiology: a report on aspirin, clopidogrel, prasugrel, and ticagrelor.Curr Pharm Des.2016;22:1918-1932.
- Current-Oasis Investigators. Dose comparisons of clopidogrel and aspirin in acute coronary syndromes.N Engl J Med.2010;363:930-942.
- Yusuf S, Zhao F, Mehta SR, et al. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation.N Engl J Med.2001;345:494-502.
- Wiviott SD, Braunwald E, McCabe CH, et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes.N Engl J Med.2007;357:2001-2015.
- Tantry US, Bonello L, Aradi D, et al. Consensus and update on the definition of on-treatment platelet reactivity to adenosine diphosphate associated with ischemia and bleeding.J Am Coll Cardiol.2013;62:2261-2273.
- Yusuf S, Zhao F, Mehta SR, et al. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation.N Engl J Med.2001;345:494-502.
- Current-Oasis Investigators. Dose comparisons of clopidogrel and aspirin in acute coronary syndromes.N Engl J Med.2010;363:930-942.
- Chen ZM, Jiang LX, Chen YP, et al. Addition of clopidogrel to aspirin in 45,852 patients with acute myocardial infarction: randomised placebo-controlled trial. 2005;366:1607-1621.
- Sabatine MS, Cannon CP, Gibson CM, et al. Addition of clopidogrel to aspirin and fibrinolytic therapy for myocardial infarction with ST-segment elevation.N Engl J Med.2005;352:1179-1189.
- Brunton LL, Hilal-Dandan R, Knollmann BC, eds. Goodman & Gilman's : the Pharmacological Basis of Therapeutics, 13e. McGraw-Hill's AccessMedicine. 13th ed. New York, N.Y.: McGraw-Hill Education LLC.; 2018. Available athttp://accesspharmacy.mhmedical.com.proxy.cc.uic.edu/content.aspx?bookid=2189§ionid=170270669. Accessed 2019, May 30.
- Wiviott SD, Braunwald E, McCabe CH, et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes.N Engl J Med.2007;357:2001-2015.
- Roe MT, Armstrong PW, Fox KA, et al. Prasugrel versus clopidogrel for acute coronary syndromes without revascularization.N Engl J Med.2012;367:1297-1309.
- Dobesh PP, Oestreich JH. Ticagrelor: pharmacokinetics, pharmacodynamics, clinical efficacy, and safety. 2014;34:1077-1090.
- Wallentin L, Becker RC, Budaj A, et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes.N Engl J Med.2009;361:1045-1057.
- Mahaffey KW, Wojdyla DM, Carroll K, et al. Ticagrelor compared with clopidogrel by geographic region in the Platelet Inhibition and Patient Outcomes (PLATO) trial. 2011;124:544-554.
- Berwanger O, Nicolau JC, Carvalho AC, et al. Ticagrelor vs clopidogrel after fibrinolytic therapy in patients with ST-elevation myocardial infarction: a randomized clinical trial.JAMA Cardiol. 2018;3:391-399.
- Angiolillo DJ, Rollini F, Storey RF, et al. International expert consensus on wwitching platelet P2Y12 receptor-inhibiting therapies. 2017;136:1955-1975.
- Wiggins BS, Rodgers JE, DiDomenico RJ, Cook AM, Page RL, 2nd. Discharge counseling for patients with heart failure or myocardial infarction: a best practices model developed by members of the American College of Clinical Pharmacy's Cardiology Practice and Research Network based on the Hospital to Home (H2H) Initiative.Pharmacotherapy. 2013;33:558-580.
- Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2018. 2018;139(25):e1082-e1143.
- Cannon CP, Blazing MA, Giugliano RP, et al. Ezetimibe added to statin therapy after acute coronary syndromes.N Engl J Med. 2015;372:2387-2397
- Schwartz GG, Steg PG, Szarek M, et al. Alirocumab and cardiovascular outcomes after acute coronary syndrome.N Engl J Med.2018;379:2097-2107.
- Garg R, Yusuf S. Overview of randomized trials of angiotensin-converting enzyme inhibitors on mortality and morbidity in patients with heart failure. Collaborative Group on ACE Inhibitor Trials. 1995;273:1450-1456.
- Rodrigues EJ, Eisenberg MJ, Pilote L. Effects of early and late administration of angiotensin-converting enzyme inhibitors on mortality after myocardial infarction.Am J Med.2003;115:473-479.
- Lee VC, Rhew DC, Dylan M, Badamgarav E, Braunstein GD, Weingarten SR. Meta-analysis: angiotensin-receptor blockers in chronic heart failure and high-risk acute myocardial infarction.Ann Intern Med.2004;141:693-704.
- Bossard M, Binbraik Y, Beygui F, et al. Mineralocorticoid receptor antagonists in patients with acute myocardial infarction - A systematic review and meta-analysis of randomized trials.Am Heart J. 2018;195:60-69.
- Levine GN, Bates ER, Bittl JA, et al. 2016 ACC/AHA guideline focused update on duration of dual antiplatelet therapy in patients with coronary artery disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines.J Am Coll Cardiol. 2016;68:1082-1115.
- Yeh RW, Secemsky EA, Kereiakes DJ, et al. Development and validation of a prediction rule for benefit and harm of dual antiplatelet therapy beyond 1 year after percutaneous coronary intervention. 2016;315:1735-1749.
- Bonaca MP, Bhatt DL, Cohen M, et al. Long-term use of ticagrelor in patients with prior myocardial infarction.N Engl J Med. 2015;372:1791-800.
- Furtado RHM, Bhatt DL, Steg PG, et al. Long-Term Secondary Prevention with Ticagrelor for Prior Myocardial Infarction in Patients with no Coronary Stenting: a sub-analysis from PEGASUS TIMI 54; presented at: AHA Scientific Sessions 2018, 2018 Nov 10-12, Chicago, Illinois. Available at http://www.abstractsonline.com/pp8/#!/4682/presentation/51815.
- Bonaca MP, Storey RF, Bhatt DL, et al. Patient Selection for Long-Term Secondary Prevention with Ticagrelor: Insights from PEGASUS-TIMI 54; presented at: AHA Scientific Sessions 2018, 2018 Nov 10-12, Chicago, Illinois. Available at http://www.abstractsonline.com/pp8/#!/4682/presentation/45643.
- January CT, Wann LS, Calkins H, Chen LY, Cigarroa JE, Cleveland Jr JC, Ellinor PT, Ezekowitz MD, Field ME, Furie KL, Heidenreich PA, Murray KT, Shea JB, Tracy CM, Yancy CW, 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation,JAmColl of Cardiol.2019;74(1):104-132. Available at . https://www.sciencedirect.com/science/article/pii/S0735109719302098?via%3Dihub.
- Cannon CP, Bhatt DL, Oldgren J, et al. Dual antithrombotic therapy with dabigatran after PCI in atrial fibrillation.N Engl J Med. 2017;377: 1513-1524.
- Gibson CM, Mehran R, Bode C, et al. Prevention of bleeding in patients with atrial fibrillation undergoing PCI.N Engl J Med. 2016; 375: 2423-2434.
- Lopes Rd, Heizer G, Aronson R, et al. Antithrombotic Therapy after Acute Coronary Syndrome or PCI in Atrial Fibrillation.N Engl J Med. 2019;380:1509-1524.
- Kumbhani DJ, Steg PG, Cannon CP, et al. Adherence to secondary prevention medications and four-year outcomes in outpatients with atherosclerosis.Am J Med. 2013;126:693-700 e1.
- Wiggins BS, Rodgers JE, DiDomenico RJ, Cook AM, Page RL, 2nd. Discharge counseling for patients with heart failure or myocardial infarction: a best practices model developed by members of the American College of Clinical Pharmacy's Cardiology Practice and Research Network based on the Hospital to Home (H2H) Initiative.Pharmacotherapy. 2013;33:558-80.
- Faridi KF, Peterson ED, McCoy LA, Thomas L, Enriquez J, Wang TY. Timing of first postdischarge follow-up and medication adherence after acute myocardial infarction.JAMA Cardiol. 2016;1:147-55.
- Krumholz HM, Merrill AR, Schone EM, et al. Patterns of hospital performance in acute myocardial infarction and heart failure 30-day mortality and readmission.Circ Cardiovasc Qual Outcomes.2009;2(5):407-413..
- Ho PM, Spertus JA, Masoudi FA, et al. Impact of medication therapy discontinuation on mortality after myocardial infarction.Arch Intern Med.2006;166(17):1842-1847.
- Hume AL, Kirwin J, Bieber HL. Improving Care Transitions: Current Practice and Future Opportunities for Pharmacists.Pharmacotherap2012;32(11):e326–e337.
- Hess EP, Coylewright M, Frosch DL, Shah ND. Implementation of shared decision making in cardiovascular care: past, present, and future.Circ Cardiovasc Qual Outcomes.2014;7(5):797-803.
- Hess EP, Hollander JE, Schaffer JT, et a. Shared decision making in patients with low risk chest pain: prospective randomized trial. 2016;355:i6165.
- Wilson T, Miller J, Teare S, et al. Patient perspectives on engagement in decision-making in early management of non-ST elevation acute coronary syndrome: a qualitative study.BMC Medical Informatics and Decision Making. 2017;17:153.
- Doll JA, Jones WS, Lokhnygina Y, et al. PREPARED Study: A study of shared decision-making for coronary artery disease.Circ Cardiovasc Qual Outcomes.2019;12:e005244.
Back to Top