
Expired activity
Please go to the PowerPak
homepage and select a course.
A Review of Nonsterile Compounding Essentials for Veterinary Patients
INTRODUCTION
In a Guidance for Industry released in May 2015, the US Food and Drug Administration (FDA) estimated that 75,000 pharmacies fill 6,350,000 compounded prescriptions for animals annually.1 A survey of 2015 pharmacy school graduates revealed that only 4% had received any veterinary pharmacotherapy training in pharmacy school.2 At time of writing, the presence of veterinary pharmacotherapy education in pharmacy technician training is also lacking, with only a few training programs offering rotations in veterinary practice settings. A survey of veterinarians’ perceptions found that one-third of respondents were aware of a pharmacist dispensing error for their animal patients, and 10% of respondents knew of incidents when pharmacist errors harmed animals.3 The spectrum of therapeutic need in veterinary medicine is large, and the availability of approved drug products for all veterinary species and indications is small. Consequently, compounding fills therapeutic gaps.
Pharmacist competence in providing pharmaceutical care and compounds for animal patients is critical because they are the only health care providers expected by society and permitted by law to provide pharmaceutical care for all species—humans and nonhumans. Almost two-thirds of US households have pets.4 It behooves all pharmacists to aspire to a high level of competence in providing the expected level of expertise and quality for households with human and nonhuman patients. Pharmacists are also well positioned to collaborate with veterinarians to provide high quality compounded formulations that are safe and have optimal compositions to deliver the intended therapeutic effect. This activity is intended to provide pharmacists and pharmacy technicians with:
- An overview of compounding regulatory requirements for nonhumans
- A working knowledge of species-specific considerations for compounding
- A review of selection of compounding formulas and components for animal patients
- A description of nonsterile compounded dosage forms commonly requested and prescribed for animal patients
- A review of appropriate counseling points and administration devices for pet owners receiving compounded preparations for their companions
GLOSSARY
Perhaps one of the most critical elements for compounded preparations is to interpret prescription abbreviations and instructions correctly. Veterinary medical education evolved independently from human health care education, and classically trained pharmacists and pharmacy technicians often find abbreviations used on veterinary prescriptions unrecognizable. Table 1 lists relevant veterinary abbreviations and acronyms and their translations.
| Table 1. Medical Terminology for Veterinary Prescriptions |
| Term/Abbreviation |
Translation |
| Bolus |
Large, solid, oral dosage form, usually for horses or livestock |
| Divided BID |
The total daily dose is calculated and then administered over 2 equally divided doses 12 hours apart |
| DLH |
Domestic Longhaired (cat) |
| Drench |
Large volume of oral liquid administered as a single dose |
| DSH |
Domestic Shorthaired (cat) |
| EOD |
Every other day |
| Fe - |
Feline or cat |
| FS |
Female spayed |
| K9 |
Canine or dog |
| MN |
Male neutered |
| OD |
Once daily or right eye depending on context |
| Paste |
Viscous oral liquid dosage form |
| QOD |
Every other day |
| SID |
semel in die (once daily) |
| TD |
Transdermal |
| Source: References 5, 6 |
DUE DILIGENCE
Prescription review for nonhuman patients requires a novel dimension of due diligence. While identifying species is the most obvious novelty, the animal’s intended use or “job” is a critical consideration.
Legally, humans may not be consumed as food, but humans may consume almost any other animal species as food if they desire. Currently, it is illegal to eat species that the US Secretary of Interior or Secretary of Commerce designates as endangered, but social and cultural preferences put all other animals at risk of consumption as human food. FDA Center for Veterinary Medicine (CVM) has identified food animal species according to “major” species (cattle, pigs, chickens, and turkeys) or “minor” species (any other species, typically goats, sheep, rabbits, game birds, nonornamental fish, and honeybees).7 Although withdrawn in November 2017, FDA’s Guidance for Industry 230, Compounding with Bulk Drug Substances for Animal Patients prohibited compounding with Active Pharmaceutical Ingredients (bulk drug substances) for cattle, swine, chickens, turkeys, sheep, goats, or ornamental fish. The prioritization of these species as food-producing animals gives clear insight into FDA’s current thinking regarding use of compounded preparations in food-producing animals. The terms “major” and “minor” species are economically derived descriptors and are based on market share for veterinary pharmaceuticals; they do not predict the likelihood of an individual animal being consumed as human food. For this reason, veterinary drug law has evolved quite differently than human drug law and will be discussed at length in the next section. Knowing whether an animal or its byproducts (eg, milk, eggs, and honey) are going to be consumed by humans is a critical consideration prior to preparing compounded medications for animal patients.
Animals may also perform nonfood-related jobs for humans as performance or service animals. Almost every competitive animal performance discipline is ruled by drug use prohibitions that impose strict penalties for violative drug residues detected in animal athletes.8,9 Pharmacists filling veterinary prescriptions should ask whether the animal is used in competition; if so, the pharmacist should include relevant precautions in prescription-related caregiver counseling. Dogs and horses commonly perform service roles for humans (eg, substance or human detection, assistance for challenged humans, animal-assisted therapy, and manual labor). Pharmacists should also ask whether an animal is a service animal and address medical therapy’s potential impact on their ability to perform their jobs when providing caregiver counseling.
Species- and breed-specific differences in drug disposition comprise the bulk of a veterinary pharmacist’s expert knowledge. Differences in anatomy, physiology, metabolic capacity, and genetic predispositions across animal species and breeds determine whether a given drug will be therapeutic or toxic in an animal. A more detailed description of species and breed-specific considerations is offered below.
Health care providers must view drug-dosing metrics differently for veterinary patients. While many dosages for drugs used in humans are empiric and based on the typical adult or pediatric human patient, dosages for animal patients are most frequently weight-based or scaled. Veterinary dosing metrics are typically dosed according to a ratio of drug amount per body weight (actual or ideal body weight) or surface area (eg, milligram per kilogram body weight or milligram per meter2 body surface area).10 For this reason, pharmacists and pharmacy technicians reviewing prescriptions for nonhumans must request the patient’s current weight if it is not indicated on the prescription, and confirm dosages by consulting a veterinary drug information reference or contacting the prescribing veterinarian.
In addition, animal weight is very important in determining appropriate sizes and volumes of compounded dosage forms for administration. The amount of oral liquid or solid oral dosage form size that an animal will tolerate or accept correlates directly with its species and body size. While volumes permitted for use in laboratory animals are quite large (10 mL per kg per dose),11,12 many pet owners are unable to manage more than 0.2 mL to 0.3 mL per kg body weight per dose. Additional discussion of this concept is presented in the Species Specifics section below.
CURRENT REGULATORY ENVIRONMENT
Drug law for animal use is based primarily on preventing harm to human health if people consume animal tissues that have drug residues.13 However, the vast majority of veterinary prescriptions presented to pharmacies are for companion animals that will never be consumed as food. To accommodate this wide spectrum of intended use, the US Congress enacted the Animal Medicinal Drug Use Clarification Act (AMDUCA) in 1994.14 The FDA’s CVM regulates the Act. AMDUCA codifies extralabel use of drugs in animals. Extralabel use is use of a drug in a manner not specified on the label or documents provided by the manufacturer; liability for such use rests with the veterinarian, not the manufacturer. Extralabel use is a practice that includes use of compounded drug preparations since they have no FDA-approved label. CVM employs a combination of regulations, rules, and guidance to enforce AMDUCA’s provisions when human public health is at risk from extralabel use of drugs in animals.15 Neither AMDUCA nor promulgated regulations permit or prohibit use of bulk drug substances or active pharmaceutical ingredients (APIs, see Sidebar) in food-producing or nonfood-producing animals.
|
Sidebar: Definition of Active Pharmaceutical Ingredient (API): “Any substance or mixture of substances intended to be used in the manufacture of a drug (medicinal) product and that, when used in the production of a drug, becomes an active ingredient of the drug product. Such substances are intended to furnish pharmacologic activity or other direct effect in the diagnosis, cure, mitigation, treatment, or prevention of disease or to affect the structure and function of the body.”
|
| Source: Reference 16 |
Because AMDUCA and regulations are silent on the use of APIs, FDA has issued a series of guidance documents that date back to 1996 indicating their current thinking on issues that represent high or low regulatory priority. At the time this article was prepared, the most recent FDA guidance document for veterinary compounding, Guidance for Industry (GFI) #230: Use of Bulk Drug Substances in Compounding for Animal Patients, issued in 2015 was withdrawn completely in 2017 after public comments indicated that the guidance was too restrictive to allow veterinarians to properly treat animal patients. Although currently withdrawn, GFI #230 clearly described FDA enforcement priorities for pharmacists compounding with APIs for both food-producing and nonfood-producing animals.17 While current statute requires that compounds for animal patients be prepared from FDA-approved products, ironically, pharmacists are generally unable to obtain veterinary-only approved drug products needed to make compounds. This paradox is a consequence of decisions by the Animal Health Institute (veterinary pharmaceutical industry) that restrict distribution of veterinary products to licensed veterinarians and was closely scrutinized by the Federal Trade Commission in 2014.18 Pharmacists who try to provide legally compliant compounded therapies for animals often find themselves without legally acceptable options when they cannot obtain starting ingredients, or approved veterinary products, but can obtain only technically illegal starting ingredients. At the time of this writing, the Federal Trade Commission continues to examine this restrictive distribution practice and is evaluating whether it is discriminatory.18
Until such rulings become official, pharmacists and pharmacy technicians are encouraged to use approved drugs as starting ingredients when possible and appropriate. A suggested decision tree based in FDA’s historical thinking for compounding for food-producing animals vs companion animals is presented below in Figure 1.17
| Figure 1. Compounding for Food-Producing vs Companion Animals |
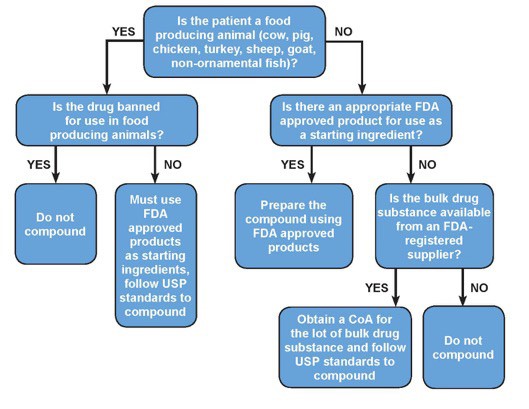 |
Abbreviation: USP, United States Pharmacopeia
Adapted from reference 17. |
SPECIES SPECIFICS
Although pharmacists are recognized experts in the field of human pharmacology and drug therapy, they cannot easily extrapolate human pharmacotherapy concepts to nonhuman medical therapies. Although humans tend to anthropomorphize animals, they are not smaller, larger, furrier, feathered, scaled, or finned versions of humans. Critical evaluation of compounded preparations’ potential safety and efficacy in animals requires pharmacists to be aware of species’ anatomical, physiological, metabolic, behavioral, genetic, dietary, and toxicological differences.
Anatomical differences among species are significant in veterinary pharmacotherapy.10 Comprehensive discussion of significant anatomical differences is beyond the scope of this activity, but the most relevant to preparing compounds are presented.
Body covering and body orientation are important anatomical considerations. Densely furred species may not receive the full benefit of topical therapy, and species covered with feathers primarily used for insulation against heat and cold may be harmed by topical therapies that disrupt feather integrity. For example, topical ointments are rarely used on birds as they may lead to hyperthermia or hypothermia, depending on ambient temperatures. Most veterinary species have a horizontal (rather than vertical) body orientation, and gravity does not facilitate passage of solid dosage forms to the stomach.10 For example, large capsules or medicated treats compounded for dogs and cats may lodge on the esophageal mucosa and cause erosions before reaching the stomach, where dilution and dissolution should occur. Caregivers for animals with horizontal body orientations should be instructed to chase orally administered solids with at least 5 mL to 6 mL of liquid or a small amount of food compatible with the drug being administered.
Species’ metabolic, and consequently, toxicological differences are also important considerations for nonhuman compounding.10 Glomerular filtration rate, hepatic drug-metabolizing enzymes, protein transporters, and efflux pumps in nonhuman species vary widely. Understanding nonhuman drug metabolism limitations is critical to preparing compounds for animal species.
Cats perform glucuronyl transferase conjugations inefficiently; drugs, excipients, flavors, and dyes cleared by this mechanism often are metabolized by alternate pathways to metabolites that can be toxic and are often deadly in cats. Pharmacists should evaluate any drug, excipient, preservative, flavor, or dye carefully before using it in a feline preparation. Alcohols, benzoic acid derivatives, and azo dyes are particularly problematic. If a colored tracer (eg, a colored powder added to inspect homogeneity visually) is required when triturating powders to make capsules for cats, a naturally colored powder such as cyanocobalamin should be used instead of an artificially colored dye. It is also very important to note that cats groom themselves and other cats, so these same principles should also be applied to all topical therapies to prevent unintended systemic adverse effects from topically administered compounds.
Dogs are relatively deficient in the enzymes that acetylate drugs, and pharmacists should beware of this deficiency before compounding for dogs. Dogs also have significant genetic anomalies that predispose them to unique toxicities. While the artificial sweetener, xylitol, is generally recognized as safe in most species, it is rapidly and completely absorbed across the gastrointestinal–blood barrier in dogs. It acts like glucose, causing insulin release and a corresponding profound, often fatal, hypoglycemia. Chronic xylitol exposure can also cause severe hepatic necrosis in dogs.19 Many drugs approved for use in humans contain xylitol as an inactive ingredient, and pharmacists may be asked to compound a copy of a commercially available drug that does not contain xylitol, such as gabapentin (Neurontin) oral solution.20
Canine mast cells are reactive to surfactants and preservatives commonly used in humans drugs (eg, polysorbate 80 and Cremophor EL) and can result in serious, life-threatening anaphylactic reactions in dogs.21,22 While a comprehensive discussion of species-specific metabolic differences is beyond the scope of this activity, Table 2 illustrates excipients, flavors, preservatives, and dyes that should be avoided in select species.
| Table 2. Toxic Drugs/Excipients/Foods by Species |
| Drug/Excipient/Food |
Species Affected |
Toxicity |
| Alcohols |
Dogs, cats, birds |
Central nervous system toxicity |
| Avocado |
Birds |
Pulmonary congestion, nonsuppurative inflammation of the liver, kidney, pancreas, skin, and proventriculus |
| Benzocaine, benzoic acid derivatives |
Cats |
Red blood cell oxidative injury, hemolytic anemia |
| Chocolatea |
Dogs, birds |
Cardiovascular and central nervous system stimulation |
| Cremophor |
Dogs |
Histamine release, anaphylaxis |
| Fat, fatty foods |
Dogs |
Increased risk of pancreatitis |
| Garlic, onionsa |
Dogs, cats |
Hemolytic anemia |
| Grapes, raisinsa |
Dogs |
Renal toxicity |
| Macadamia nutsa |
Dogs |
Lethargy, hyperthermia, ataxia, vomiting |
| Pennyroyal |
Cats |
Hepatotoxicity |
| Polysorbate 80 |
Dogs |
Histamine release, anaphylaxis |
| Raw yeast dough |
Dogs |
Alcohol poisoning, gastrointestinal dilatation and volvulus |
| Xylitol |
Dogs, birds |
Profound hypoglycemia and hepatocellular necrosis |
Source: Reference 23
a Artificial flavors that mimic the natural substance are not toxic but encourage an attraction to the natural substance. |
Dietary and behavioral considerations are also important when providing safe, palatable compounds for nonhuman patients. Animal flavor preferences correlate strongly with their natural diets.24 For example, cats are obligate carnivores (depend on the nutrients found only in animal flesh for their survival), typically preying on small rodent species, birds, and fish. They are relatively uninterested in flavors associated with carbohydrates (eg, sweet or aromatic). Cats also lack sweet taste receptors on their tongues25 and primarily prefer meat-based or organ flavors, such as tuna, salmon, chicken, or liver. Dogs evolved with a more omnivorous dietary habit after preying on species with large quantities of herbivorous matter in their gastrointestinal tracts. As a result, dogs have a wider spectrum of flavor preferences, including sweet, salty, and meat-based flavors.
Birds’ wide variety of flavor and texture preferences are related to their species and natural diets. Herbivorous and omnivorous birds, such as caged birds and poultry, often prefer color and movement over flavor and texture.26 For example, chickens usually prefer a colorful, wiggly medicated gummy worm offered by hand over a flavored, colorless, oral suspension delivered from an oral syringe.
Horses’ carbohydrate-rich diets lead them to prefer sweet and aromatic flavors. Horses select food based on visual cues, odor, taste, texture, availability, and variety. A flavor-preference study performed at the University of Southampton identified some surprising favorite flavors for horses, with the top-ranked favorite being fenugreek (a spice with a maple fragrance and bitter-to-sweet taste).27
Comprehensive reviews of animal taste preferences have been published for companion animals.28,29 Table 3 describes flavor preferences by species; however, the pharmacist and pharmacy technician should always consult the animal’s caregiver to confirm which flavors are most likely to be accepted.
Finally, pharmacists must consider impact on drug stability and bioavailability when adding flavors to compounds. They need to evaluate flavors that change pH, alter solubility or suspendibility, or risk binding of active ingredients carefully before including them in compounded preparations.
| Table 3. Flavor Preferences by Species |
| Species |
Preference |
| Cat |
Meat, organ meat, fish |
| Dog |
Meat, salty, sweet |
| Horse |
Sweet, fruit, aromatic herbs/grasses |
| Bird |
Dietary dependent |
| Cow |
Sweet, aromatic herbs/grasses |
| Rabbit |
Herb, vegetable, sweet |
| Pig |
Sweet, fruit, vegetable |
| Ferret |
Meat, fish, sweet |
| Reptiles |
Dietary dependent |
FORMULA AND COMPONENT SELECTION
While many verified and peer-reviewed formulas are available for compounded dosage forms intended for humans, these formulas may be inappropriate for use in nonhuman species. The United States Pharmacopeia (USP) has developed dozens of verified compounded preparation formulas specifically for veterinary use.31 USP nomenclature identifies these formulas in its compendia by the following format: Drug Generic name, Compounded, Dosage Form, Veterinary (eg, Enrofloxacin, Compounded, Oral Suspension, Veterinary). USP has tested its veterinary-compounded preparation monographs for stability to the published beyond-use-dates (BUDs) and includes specific instructions describing how to prepare, package, test, and label each compound. Many of the almost 200 USP compounded preparations not specified for veterinary use may also be used in animal patients if the criteria presented above are used to evaluate species-specific concerns. In addition to the USP-National Formulary (USP-NF) hard copy books, USP now offers an electronic USP Compounding Compendium that contains all standards and formulas related to compounding.31
When a USP formula monograph is unavailable, drug manufacturers may sometimes provide extemporaneous compounding information for their products; however, this information is rarely available, and manufacturers—concerned about liability—are often unwilling to share this information. Pharmacists can locate other compounding formulas by searching secondary source collections of published peer-reviewed compounded preparation stability studies,32 again with the caveat that they must review species-specific considerations for each component used. If peer-reviewed evidence cannot be located in secondary resources, a search of primary peer-reviewed literature may reveal a stability-tested formula suitable for use in animal patients. The International Journal of Pharmaceutical Compounding is a bimonthly scientific and professional journal that frequently features stability-tested formulas for veterinary compounds.33
When no evidence is available to support stability and ingredient compatibility for a compounded preparation, pharmacists should apply USP compounding defaults. They must consider the active drug’s inherent stability, suitability of components for the target patient/species, and potential adverse effects if the compound is not stable throughout the labeled BUD and intended therapy period. USP General Chapter <795> Pharmaceutical Compounding-Non-sterile Preparations default BUDs for nonsterile compounds, which are listed in Table 4. An illustrative example for applying USP defaults to a nonevidence-based compounded preparation for animals follows in Box 1.
| Table 4. United States Pharmacopeia <795> Beyond-use-Date |
| Type of Preparation |
Beyond-use Date
(days) |
Storage Temperaturea |
Examples |
Non-preserved aqueous
dosage formsa |
14 |
Refrigerator |
Tablets crushed in distilled water |
Preserved aqueous
dosage formsa |
35 |
Controlled room temperature or refrigerator |
Tablets crushed and suspended in a preserved oral suspending vehicle |
| Nonaqueous dosage formsb |
90 |
Controlled room temperature or refrigerator |
Tablets crushed and suspended in an oil vehicle |
| Solid dosage formsc |
180 |
Controlled room temperature or refrigerator |
Capsules, tablets, granules, powders |
a An aqueous preparation is one that has a water activity (Aw) of > 0.6 (eg, emulsions, gels, creams, solutions, sprays, or suspensions)
b Any preparation other than solid dosage forms that have a reduced Aw of ≤ 0.6 (eg, suppositories, ointments, fixed oils, or waxes)
c Capsules, tablets, granules, powders |
| Source: Reference 30 |
|
Box 1. Compounding Clinical Pearl: Pharmacy Case Study
A veterinarian would like to prescribe torsemide for a small Chihuahua with chronic heart failure. He consults the pharmacist and asks how he can provide a 0.5 mg dose orally twice daily to the canine patient. Torsemide is available as a 5 mg tablet, so fractionating the tablet is not an option. After consulting USP, primary and secondary literature, and calling the manufacturer, the pharmacist determines that no verified formula for torsemide suspension exists. She turns to USP defaults in USP <795>. Her BUD options are 30 days refrigerated if she uses a preserved aqueous vehicle, and 90 days room temperature if she uses an anhydrous vehicle such as fixed corn oil. The dog has a cough and pulmonary effusion due to its congestive heart failure, so the pharmacist decides that aspiration of an anhydrous vehicle (eg, fixed oil) would be very dangerous. She also discusses with the veterinarian the fact that this is a novel therapy for the dog and that to ensure drug efficacy, drug stability must be assumed throughout the treatment period. The veterinarian tells her that the follow-up appointment for the dog is scheduled in 10 days and the dosage may be adjusted at that time based on clinical response. The pharmacist then reasons that it is best to compound torsemide as a 5 mg/mL oral suspension in simple syrup and assign a 30-day refrigerated BUD. The resultant volume of administration for the dog is 0.1 mL orally twice daily, and the dog’s caregiver feels this is a manageable dosing volume and will continue to allow for reasonable volumes if the dose is increased at the follow-up visit.
Abbreviations: BUD, beyond-use-date; mg, milligram; mL, milliliter; USP, United States Pharmacopeia.
|
COMPOUNDED VETERINARY DOSAGE FORMS
The majority of compounded prescriptions presented to community pharmacists by the animal’s caregiver will be for nonsterile compounded preparations. such as oral suspensions, capsules, and medicated treats. Less often, community pharmacists will be asked to perform more complex nonsterile compounding, which includes transdermal gels and core-coated targeted-release tablets. A discussion of considerations for the most commonly prescribed compounded dosage forms is presented below.
Oral Suspensions
Pharmacists compound oral suspensions most often for animal patients.34 This dosage form allows concentration or dilution of strength as compared to manufactured products and allows flexible dose adjustment necessitated by growth or desired therapeutic effect. Many cat, horse, and exotic animal pet owners also prefer oral suspensions as they are easier to administer than other forms.
When preparing oral suspensions, pharmacists should consider 2 concerns about drugs particle size in suspension (from API or manufactured tablets or capsules):
- Particle size should be small enough to keep the drug sufficiently suspended to allow caregivers to withdraw uniform doses.
- Particle size should not be so small that it settles on the bottom of the container and forms a hard, nondispersible cake.31
Appropriate vehicle viscosity is critical. Aqueous vehicles such as methylcellulose or simple syrup are usually employed; anhydrous vehicles include corn oil, NF, and cod liver oil, NF. Silica gel can be used as a suspending agent. Note that silica gel should be avoided in animals with a propensity to develop silicate uroliths, a condition that can be confirmed with the prescriber prior to compounding. Pharmacists should also assess microbial preservative systems, pH, vehicle compatibility with drug, excipient compatibility with drug, and container compatibility with drug if a verified, evidence-based formula is not available. The preparation of oral suspensions is generally accomplished by the steps listed in Table 5.
| Table 5. Preparing Oral Suspensions for Veterinary Patients |
| 1. Comminute dry ingredients to a fine, uniform powder in a mortar and pestle. |
| 2. Wet the powder with the smallest volume of vehicle to accomplish a thick paste (too much liquid at this point defeats the high shear necessary to reduce particle size further and completely wet the powder). |
| 3. Geometrically add vehicle and triturate to a pourable liquid. |
| 4. Add any flavoring at this point. |
| 5. Transfer the pourable liquid to a calibrated dispensing container. |
| 6. Rinse the mortar with vehicle and bring forward to the dispensing container to bring to final volume. |
| 7. Shake well before dispensing. |
| Source: Reference 30 |
If the oral suspension needs flavoring, it is usually added at no more than 3% of the final volume prepared; however, specific proportions for each flavor should be confirmed with the flavoring’s manufacturer. It is also important to note that water-miscible flavors should only be used in water-containing vehicles, and oil-miscible flavors should only be used in anhydrous vehicles. Many commercially available suspending vehicles contain preservatives, sweeteners (some sugar-free), flavors, or artificial color. As previously stated, it is critical to confirm that these additives are not toxic to the particular species for which the compound is being prepared.
Oral Pastes
As mentioned in the glossary, veterinarians always classify pastes as oral dosage forms and never administer them topically. Oral pastes are moderately complex nonsterile dosage forms. Veterinarians frequently prescribe them for horses or other animals where a high viscosity is desired (to keep the drug from running back out of a patient’s mouth), but dosing flexibility is still required. Pharmacists compound pastes using a process almost identical to that for oral suspensions. However, the suspending vehicle’s viscosity must be high enough to prevent drug settling, and the pharmacist must ensure that the drug remains completely suspended in the vehicle before dispensing. Anhydrous paste bases include various concentrations of polyethylene bases, and aqueous bases are generally made from high concentrations (4% to 5%) of methylcellulose. Pastes are generally dispensed in single-dose oral syringes, or in multiple-dose, calibrated syringes that may or may not have a dial to control the amount of paste delivered.
Oral Capsules
Compounded capsules offer significant advantages over liquid dosage forms as they contain an exact dose and clients have fewer measuring tasks than with liquids or pastes. Capsules also may contain powders or liquids, and since they can be sealed and locked, may mask the taste of drugs that animals find unpalatable. Caregivers may also open capsules and sprinkle the contents on moist food, or mix them with a small amount of palatable compatible liquid in an oral dosing syringe immediately before administration.
The USP default stability BUD for capsules is 180 days or the manufacturer’s API expiration date, whichever is shorter, so capsules are ideal for chronic conditions that require only occasional rechecks with the attending veterinarian.30 Capsules are available in many inert and dissolvable materials (gelatin, vegetable cellulose) and colors, making them pharmaceutically elegant and appealing to pet owners. Pharmacists can prepare capsules from approved solid dosage forms (tablets and capsules) or API powders. Instead of a liquid vehicle, the diluent vehicle is usually an inert powder such as lactose, USP, or hypromellose, USP. For capsules that will be opened by pet owners and sprinkled on the pet’s food, pharmacists can comminute finely ground dried kibble (pet food) to a fine powder and use it as the capsule diluent (provided the drug is compatible with ingredients in the kibble). The typical procedure for compounding capsules is explained below in Table 6.
| Table 6. Preparing Oral Capsules for Veterinary Patients |
| 1. Calculate the total amount of active ingredient required using commercially available tablets, capsules, or API powder. Remember to account for any inert ingredients in starting tablets or capsules, and waters of hydration, salt forms, and percentagestrength from the certificate of analysis for API powders. |
| 2. Calculate total amount of diluent powder required to mix with active drug ingredients to ensure that finished weight completely occupies the calibrated volume of the empty capsule. |
| 3. Working in a powder hood with appropriate protective clothing, weigh all calculated components and place in mortar using geometric dilution of API powders with excipients. |
| 4. Comminute dry ingredients into a uniformly fine particle size. |
| 5. Using a capsule machine or packing individually by hand, fill the long end of each capsule to the calibrated capacity. |
| 6. Replace the capsule tops. |
| 7. Weigh at least 20 capsules or 10% of the final number of capsules (whichever is less) to ensure that they are within ± 10% of the target filled capsule weight range, remembering to account for the weight of the empty capsule before it was filled. |
| 8. Capsules should be dispensed in light- and moisture-resistant childproof containers and pet owners instructed to store capsules at controlled room temperature (or under refrigeration if required for the active drug). |
Source: Reference 30
Abbreviation: API, active pharmaceutical ingredient. |
Chewable Treats
Many manufactured veterinary medications are available in chewable tablet forms. Because pets tend to like them, pet owners and veterinarians often ask pharmacists to prepare a similar dosage form when compounded therapies are needed. Medicated treat bases may be prepared using semi-moist pet treats as the base, or by mixing glycerin, gelatin, and polyethylene base with powdered flavors that the pet prefers.
Pharmacists prepare medicated treats similarly to capsules. They use a mold with a known calibrated final weight (similar to the known calibrated final weight of an empty capsule) and an appropriate ratio of drug-to-treat base to achieve the desired final dose. Used less often, another method is to calibrate the weight of a punched shape (eg, like a cookie cutter) cut from a sheet of treat base rolled to a uniform thickness and proceed with calculations similar to the molded treat process.
It is important to note that many semi-moist treats marketed for dogs contain propylene glycol. Propylene glycol has been banned for addition to cat food or treats since 1996, as concentrations of 5% to 10% propylene glycol have caused Heinz body anemia in cats.35 Medicated chewable treats are ideally packaged in closed troche molds or in individual blister packs to prevent exposure to mold and moisture loss. Moisture loss changes treats’ texture, and many pets will reject treats if this occurs. The procedure for compounding medicated treats is illustrated below in Table 7.
| Table 7. Preparing Chewable Treats for Veterinary Patients |
| 1. Calculate the total amount of active ingredient required using commercially available tablets, capsules, or API powder. Remember to account for any inert ingredients in starting tablets or capsules, and waters of hydration, salt forms, and percentage strength from the certificate of analysis for API powders. |
| 2. Calculate total amount of treat base required to mix with active drug ingredients to achieve the total weight of the calibrated mold or cutout. |
| 3. Working in powder hood with appropriate protective clothing, weigh all calculated components and place in mortar. |
| 4. Comminute ingredients into a uniformly mixed dough. |
| 5. Using a treat mold, fill each mold evenly to capacity or roll out dough uniformly and cut to appropriate size. |
| 6. Weigh at least 10% of the final number of treats to ensure that they are within ± 10% of the target weight range. |
Source: Reference 30
Abbreviation: API, active pharmaceutical ingredient. |
Transdermal Gels
Transdermal gels areformulated in penetration-enhancing percutaneous vehicles intended to achieve systemic bioavailability after topical application to intact skin. Veterinary transdermal gels are used most often in cats, and the most common application site is the hairless pinna inside the cat’s ear.36 To accomplish transdermal penetration, drugs are usually compounded in concentrations that deliver doses in volumes of 0.1 mL to 0.2 mL. For example, methimazole transdermal gel is compounded in a concentration of 50 milligrams (mg) per mL to allow delivery of 5 mg in 0.1 mL.37
Veterinarians will frequently consult compounding pharmacists for advice as to whether a drug is a good candidate for transdermal administration. While a comprehensive discussion of the use of transdermal gels in veterinary medicine is beyond the scope of this activity, note that drugs with narrow therapeutic indices, drugs with known safety issues for humans, and drugs that are listed as contact irritants in the Material Safety Data Sheet are generally considered inappropriate candidates for transdermal administration. Transdermal gels are generally prepared as shown in Table 8.
| Table 8. Preparing Transdermal Gels for Veterinary Patients |
| 1. Weigh or measure the appropriate amount of API powder required to prepare the prescribed volume of the transdermal gel. |
| 2. In a suitable container (syringe or mortar) wet the API with a suitable solvent, such as propylene glycol or diethylene glycol, to a smooth paste. |
| 3. Add the appropriate percutaneous penetration enhancing vehicle (eg, lecithin:isopropyl palmitate solution and Pluronic F127) to volume. |
| 4. Mix using a shearing action by using an ointment mill or with a sufficient number of syringe-to-syringe transfers to accomplish uniform mixing. |
Source: Reference 30
Abbreviation: API, active pharmaceutical ingredient. |
Transdermal gels are typically dispensed in 1 mL amber dosing syringes with 0.1 mL calibration marks so each syringe contains approximately 10 doses. Twist-and-click delivery systems are available for delivery of transdermal gels, but these administration devices must be calibrated carefully to ensure uniform dose delivery. Since transdermal drugs do not discriminate between patient skin and caregiver skin, pharmacists should counsel caregivers to use protective gloves or finger cots when applying transdermal medications and to wash hands thoroughly after.
Suppositories
Used infrequently in veterinary species, suppositories provide local or systemic effects. They contain 1 or more drug substances dispersed in a suitable base and molded into a shape and size suitable for insertion into the rectum. The most common use of suppositories in animal patients is for local effects in the rectum (eg, constipation) or when the oral route is inaccessible (eg, patient is experiencing status epilepticus or when the patient refuses oral medications). Because nonhumans cannot be commanded to retain suppositories voluntarily, the suppository’s size and shape must facilitate retention without prolonged manual occlusion of the anal sphincter by the caregiver. No authoritative references are available on the subject of appropriate size and shape for nonhuman rectal suppositories, so pharmacists must consult with prescribing veterinarians to determine specific needs for individual patients.
Suppositories may be prepared by mixing an appropriate amount of active drug substance with a compatible suppository base and then forming into shapes by hand-rolling, compression molding, or fusion molding. Suppositories are generally made from solid ingredients and drugs that are measured by weight. When they are mixed, melted, and poured into suppository mold cavities, they occupy the volume of the mold cavity. Since the components are measured by weight but compounded by volume, pharmacists will need to perform density and mold calibrations to provide accurate doses. Density factors to determine drug displacement by volume are available in pharmaceutical reference texts.38
Compounded Sterile Preparations
Sterile compounds are also used in veterinary patients but are beyond the scope of this activity. Pharmacists interested in providing sterile compounded preparations for animal patients are encouraged to apply the legal considerations and species-specific concepts presented for nonsterile veterinary compounding and to follow USP General Chapter <797> Pharmaceutical Compounding—Sterile Preparations.
QUALITY ASSURANCE OF VETERINARY COMPOUNDS
USP compounding standards require subjective and objective assessments of quality for compounds before they are dispensed to patients.39 In compounded preparation monographs, USP lists specific tests that must be performed on a compound to determine its quality. Determination of final pH, as described by USP General Chapter <791>, is required for all water-containing USP compounded preparation monographs.40 Sterility testing is not required for nonsterile compounded preparations, but antimicrobial effectiveness testing may be useful for nonsterile compounds that have the potential for microbial or fungal growth over the lifetime of their stated BUD. Quality assessment of a finished nonsterile liquid might include determination of correct volume, uniform dispersion of suspended solids, particulate matter for solutions, pH, osmolality, osmolarity, resuspendibility, color, odor, and “syringeability” in an oral-dosing syringe. Quality assessment of a solid nonsterile compounded dosage form might include dosage form target weight, uniformity, capsule integrity, color, and dissolution.
ANIMAL-FRIENDLY DISPENSING AND ADMINISTRATION DEVICES
Oral liquids for humans are often labeled and dosed in concentrations that reflect imperial system spoon measurements (eg, teaspoonfuls and tablespoonfuls.) While imperial units may be useful for dosing human patients when pouring liquid doses into a spoon, they are impractical for dosing animal patients who do not ingest medications or foods in this manner. Animal patients also vary greatly in size, making spoon measurements even less relevant when delivering accurate doses for very small or very large animals. For this reason, veterinary compounded liquids should be dispensed with oral dosing syringes and special adapter caps or inserts to allow liquids to be removed accurately and cleanly. The hub of an oral dosing syringe is inserted into the adapter cap aperture, the bottle inverted, and liquid withdrawn to the desired dosing mark. Figure 2 demonstrates this procedure. Pharmacists can wrap “dose mark” auxiliary labels around the oral dosing syringe, clearly indicating the intended dose with a black line.
| Figure 2. Appropriately using an oral dose syringe with special adapter cap. The hub of an oral-dosing syringe is inserted into the adapter cap aperture, the bottle inverted, and liquid withdrawn to the desired dosing mark. |
 |
| Photo by Gigi Davidson |
COUNSELING POINTS FOR VETERINARY COMPOUNDS
Comprehensive, appropriate caregiver counseling should accompany dispensing of any compound prepared for use in animals. Important counseling points are listed in Table 9.
| Table 9. Counseling Points for Veterinary Compounded Prescriptions |
| 1. Drug name, indication, and route of administration |
| 2. Frequency of administration |
| 3. Demonstration of administration devices and accurate dose markings |
| 4. Storage and handling of medication including any caregiver precautions |
| 5. Proper disposal of unused compound |
| 6. Observation of compound for any change in physical characteristics (color, consistency, odor) or pet refusal to take compound after initial acceptance |
| 7. Remind the caregiver to check for any performance drug rules for animal athletes |
| 8. Emphasize importance of returning to veterinarian for recheck appointment |
| 9. Describe monitoring signs for efficacy, toxicity, or compound failure |
| 10. Report adverse events associated with compound to both veterinarian and pharmacist |
ADVERSE EVENTS AND REPORTING SYSTEMS
Pharmacists should instruct caregivers to monitor both their pet and the compounded medication for any unexpected changes. Monitoring for the pet should include:
- Signs that might indicate an adverse effect related to the drug (eg, tachycardia, gastrointestinal upset, or diarrhea)
- Signs of compound failure, including worsening of bacterial infection from an antibiotic compound that is not stable
- Development of vomiting or hypersalivation over time from a compound that has degraded
- Signs of toxicity from vehicles, preservatives, or excipients
Caregivers should also monitor the compound itself for changes in consistency, odor, color, or phase change, and should contact the pharmacist or veterinarian immediately if the pet suddenly refuses to take a compound that was initially well accepted. Caregivers should be asked to return any remaining portion of a suspect compound to the pharmacy for analysis and corrective actions if needed. Pharmacists should report adverse events associated with compounded drug therapy to the prescribing veterinarian as well as to FDA CVM within 15 days of the adverse event. The adverse event should be reported on FDA Form 1932a, which can be found by using the following link: http://www.fda.gov/downloads/AboutFDA/ReportsManualsForms/Forms/AnimalDrugForms/ucm048817.pdf.
CONCLUSION
Pharmacists and pharmacy technicians are expected by society to provide the same level of expertise in preparing compounds for animal patients as they do for human patients. Pharmacists and pharmacy technicians who prepare compounds for nonhumans should be thoroughly familiar with regulatory boundaries for use of drugs in animals as well as knowledgeable of all of the unique tolerances and toxicities for individual species. Pharmacists and pharmacy technicians should also be familiar with veterinary prescription abbreviations and commonly compounded veterinary dosage forms to avoid potential misunderstandings when filling compounds for veterinary patients. Finally, to maintain confidence and competence in preparing compounds for veterinary patients, pharmacists and pharmacy technicians must keep abreast of changes in veterinary drug laws and stay informed regarding new therapeutic trends in veterinary medicine.
REFERENCES
- Guidance for Industry; Availability; Withdrawal of Compliance Policy Guide; Section 608.400 Compounding of Drugs for Use in Animals. Federal Register website. https://www.federalregister.gov/documents/2015/05/19/2015-11982/compounding-animal-drugs-from-bulk-drug-substances-draft-guidance-for-industry-availability. Accessed June 10, 2019.
- Arnish CE, Davidson GS, Royal K. Veterinary pharmacy education: prevalence and perceptions. Poster presented at: Society of Veterinary Hospital Pharmacists, 34th Annual Meeting; June 14-17, 2015; Portland, ME.
- Cima G. Substitution errors: surveys describe harm from differences between prescriptions and drugs dispensed. J Am Vet Med Assoc. 2014;245(5):462-482.
- S. pet ownership statistics. American Veterinary Medical Association website. https://www.avma.org/KB/Resources/Statistics/Pages/Market-research-statistics-US-pet-ownership.aspx. Accessed June 4 2019.
- Herren RV, Amundson Romich J. Delmar’s Veterinary Technician Dictionary. Albany, NY: Delmar Thomson Learning; 2000.
- Studdert VP, Gay CC, Blood DC. Saunders Comprehensive Veterinary Dictionary. 3rd ed. Edinburgh, Scotland: Saunders Elsevier; 2012.
- Minor use/minor species. U.S. Food and Drug Administration website. http://www.fda.gov/animalveterinary/developmentapprovalprocess/minoruseminorspecies/default.htm. Accessed June 4, 2019.
- United States Equine Federation. 2019 Guidelines for Drugs and Medications. Columbus, OH: United States Equine Federation, Equine Drugs and Medications Program; 2019. https://www.usef.org/forms-pubs/2Zp2C_YKs4s/drugs-medications-guidelines. Accessed July 10, 2019.
- 2019 Uniform Classification Guidelines for Foreign Substances and Recommended Penalties and Model Rule. Lexington, KY: Association of Racing Commissioners International, Inc; 2009. http://arci.com/wp-content/uploads/2019/01/2019-01-07-Classification-Substances.pdf. Accessed June 10, 2019.
- Baggot JD. The Physiological Basis of Veterinary Clinical Pharmacology. Malden, MA: Blackwell Publishing Inc; 2001.
- Morton DB, Jennings M, Buckwell A, et al; Joint Working Group on Refinement. Refining procedures for the administration of substances. Report of the BVAAWF/FRAME/RSPCA/UFAW Joint Working Group on Refinement. British Veterinary Association Animal Welfare Foundation/Fund for the Replacement of Animals in Medical Experiments/Royal Society for the Prevention of Cruelty to Animals/Universities Federation for Animal Welfare. Lab Anim. 2000;35(1):1-41.
- Diehl KH, Hull R, Morton D, et al. A good practice guide to the administration of substances and removal of blood, including routes and volumes. J Appl Toxicol. 2001;21(1):15-23.
- The Animal Drug Amendment of 1968. 21 U.S.C. 301. Public Law 90-399, July 13, 1968.
- Animal Medicinal Drug Use Clarification Act (AMDUCA) of 1994, 21 CFR 530.2. Public Law 103-396, October 22, 1994.
- Extralabel Drug Use in Animals. 21 CFR 530. (2105).
- Guidance for industry, Q7A good manufacturing practice guidance for active pharmaceutical ingredients. U.S. Food and Drug Administration website. http://www.fda.gov/ICECI/ComplianceManuals/CompliancePolicyGuidanceManual/ucm200364.htm#P1354_106112. Accessed June 4, 2019.
- Draft Guidance for Industry: Compounding Animal Drugs from Bulk Substances. Rockville, MD: U.S. Dept of Health and Human Services, U.S. Food and Drug Administration, Center for Veterinary Medicine; 2015. Archive-It.org. FDA.gov archives. https://www.archive-it.org/collections/7993?q=Guidance+for+industry+230&show=ArchivedPages&hitsPerDupe=0&go=Search+the+Archive. Accessed May 23, 2019.
- Gavil AI, Koslov TI, Wilkinson SA, et al; Federal Trade Commission. Competition in Pet Medications Industry—Prescription Portability and Distribution Practices: Federal Trade Commission Staff Report. Washington, DC: Federal Trade Commission; 2014. https://www.ftc.gov/system/files/documents/reports/competition-pet-medications-industry-prescription-portability-distribution-practices/150526-pet-meds-report.pdf. Accessed June 4, 2019.
- Piscitelli CM, Dunayer EK, Aumann M. Xylitol toxicity in dogs. Compend Contin Educ Vet. 2010;32(2):E1-E4.
- Neurontin (Gabapentin) Oral Solution [package insert]. New York, NY: Pfizer, Inc; 2009.
- Lorenz W, Reimann HJ, Schmal A, et al. Histamine release in dogs by Cremophor E1 and its derivatives: oxethylated oleic acid is the most effective constituent. Agents Actions. 1977;7(1):63-67.
- Varma RK, Kaushal R, Junnarkar AY, et al. Polysorbate 80: a pharmacological study. Arzneimittelforschung. 1985;35(5):804-808.
- United States Pharmacopeial Convention. USP Pharmacists’ Pharmacopeia: 3 Supplement (2008-2009). 2nd ed. Rockville, MD: United States Pharmacopeial Convention; 2009. https://www.academia.edu/15791278/USP_Pharmacists_Pharmacopeia_P_S_Notice_and_Warning_Concerning_U.S._Patent_or_Trademark_Rights?auto=download. Accessed May 23, 2019.
- Bradshaw JW. The evolutionary basis for the feeding behavior of domestic dogs (canis familiaris) and cats (felis catus). J Nutr. 2006;136(7 suppl):1927S-1931S.
- Xia Li, Weihua Li, Hong Wang, et al. Cats lack a sweet taste receptor. J Nutr. 2006;136(7 suppl):1932S-1934S.
- Gamberale-Stille G, Tullberg B. Fruit or aposematic insect? Context dependent colormetric preferences in domestic chicks. Proc Biol Sci. 2001;268(1485):2525-2529.
- Goodwin D, Davidson HPB, Harris P. Selection and acceptance of flavours in concentrate diets for stabled horses. Appl Anim Behav Sci. 2005;95(3-4):223-232.
- Thombre AG. Oral delivery of medications to companion animals; palatability considerations. Adv Drug Deliv Rev. 2004;56(10):1399-1413.
- Koppel K. Sensory analysis of pet foods. J Sci Food Agric. 2014; 94(11):2148-2153.
- United States Pharmacopeial Convention. USP General Chapter <795> Pharmaceutical Compounding—Nonsterile Preparations. In: United States Pharmacopeia 43/National Formulary 38. Rockville, MD: United States Pharmacopeial Convention; 2019.
- United States Pharmacopeia Compounding Compendium. United States Pharmacopeial Convention website. http://www.usp.org/store/products-services/usp-compounding-compendium. Accessed June 4, 2019.
- Trissel LA; American Pharmacists Association. Trissel’s Stability of Compounded Formulations. 6th ed. Washington, DC: American Pharmacists Association; 2018.
- International Journal of Pharmaceutical Compounding (IJPC). IJPC website. https://www.ijpc.com. Accessed June 4, 2019.
- United States Pharmacopeial Convention. USP General Chapter <1151> Pharmaceutical Dosage Forms. In: United States Pharmacopeia 38/National Formulary 33.Rockville, MD: United States Pharmacopeial Convention; 2015.
- Christopher MM, Perman V, Eaton JW. Contribution of propylene glycol-induced Heinz body formation to anemia in cats. J Am Vet Med Assoc. 1989;194(8):1045-1056.
- Davidson G. Evaluating transdermal medication forms for veterinary patients, part 1. Int J Pharm Compd. 2001;5(2):95-96.
- Lécuyer M, Prini S, Dunn ME, Doucet MY. Clinical efficacy and safety of transdermal methimazole in the treatment of feline hyperthyroidism. Can Vet J. 2006;47(2):131-135.
- Allen LV, Adeboye A, Desselle SP, Felton LA, eds. Remington: The Science and Practice of Pharmacy. 22nd ed. London, England: Pharmaceutical Press; 2012.
- United States Pharmacopeial Convention. USP General Chapter <1163> Quality Assurance in Pharmaceutical Compounding. In: United States Pharmacopeia 38/National Formulary 33. Rockville, MD: United States Pharmacopeial Convention; 2015.
- United States Pharmacopeial Convention. USP General Chapter <791> pH. In: United States Pharmacopeia 38/National Formulary 33.Rockville, MD: United States Pharmacopeial Convention; 2015.
Back to Top