
Expired activity
Please go to the PowerPak
homepage and select a course.
Evidence-Based Treatment of Hypercholesterolemia: Patient-Centered Evaluation and Management
INTRODUCTION
Cardiovascular (CV) disease has been the leading cause of death in the United States for decades. Managing hypercholesterolemia, specifically with medications that lower low-density lipoprotein cholesterol (LDL-C) is an evidence-based treatment strategy to reduce risk of atherosclerotic cardiovascular disease (ASCVD). Statin medications specifically lower LDL-C and are the primary agents used to treat patients with hypercholesterolemia. Cholesterol-lowering treatment has increased substantially among adults from 8% (1999-2000) to 18% (2011-2012), with the use of statins more than doubling (7% to 17%) during this time.1 Moreover, newer evidence about non-statin medications should increase the overall use of lipid-lowering medications.
Statin therapy lowers LDL-C and is proven to lower the risk of ASCVD based on numerous clinical trials.2 Because this evidence base is so robust, prescribing of a statin in patients with clinical ASCVD or high-risk primary prevention patients (e.g., patients with diabetes) is a clinical metric to describe quality among various health care organizations. Moreover, some patients are at high risk for developing ASCVD despite having “normal” cholesterol values. These patients are also candidates for statin therapy.
Pharmacists can be directly involved with the implementation of evidence-based hypercholesterolemia treatment. Evidence demonstrates improved control and treatment of patients with hypercholesterolemia through pharmacy intervention programs.3-6 As such pharmacists should know about and be able to apply updated evidence-based consensus recommendations for the management of hypercholesterolemia. Knowledge of lipid-lowering medications, treatment of special populations, and strategies to optimize medication management can improve patient outcomes.
EVIDENCE-BASED GUIDELINES
The National Cholesterol Education Program (NCEP) was the first to publish evidence-based guidelines for the management of hypercholesterolemia. The last NCEP guideline, the Adult Treatment Panel III, was published in 2001 with a focused update in 2004.7,8 The NCEP guidelines were sponsored by the National Heart Lung and Blood Institute, which decided to not release a subsequent guideline. Instead, the American College of Cardiology/American Heart Association (ACC/AHA) released a comprehensive evidence-based guideline in 2013.9 These 2013 ACC/AHA guidelines recommended treating with statins of fixed intensity in patient groups for whom evidence definitively demonstrated reduction in ASCVD.
This robust change to the management of hypercholesterolemia abandoned the traditional approach of treating to specific LDL-C target values and resulted in significant debate among the medical community. To highlight this point, the National Lipid Association (NLA) published recommendations in 2014 that emphasized use of LDL-C targets, a treatment approach fundamentally similar to NCEP guidelines.10
The New 2018 Cholesterol Guideline
The ACC/AHA convened an multidisciplinary group of experts with representatives from 12 different professional organizations (including the NLA) to create the 2018 Cholesterol Guideline.11 Of note, the American Pharmacists Association was one of these partner organizations. This 2018 Cholesterol Guideline builds off the 2013 ACC/AHA guidelines by recommending statin-based therapy for patients in one of four statin benefit groups.9 However, new evidence from prospective placebo-controlled studies were incorporated.12-15
The 2018 Cholesterol Guideline categorizes patients based on the presence (secondary prevention) or absence (primary prevention) of clinical ASCVD.11 Similar to the 2013 ACC/AHA guideline, four statin benefit groups continue to define patients with proven benefit from statin therapy, as follows:
- Secondary Prevention – Clinical ASCVD
- Primary Prevention – Severe hypercholesterolemia with baseline LDL-C ≥190 mg/dL
- Primary Prevention – Diabetes, age 40–75 years with LDL-C of 70–189 mg/dL
- Primary Prevention – Age 40–75 years, without diabetes, with LDL-C of 70–189 mg/dL and estimated 10-year ASCVD risk of ≥7.5%
Both a class of recommendation (COR) and level of evidence (LOE) accompany each recommendation in the 2018 Cholesterol Guideline. The COR is I, IIa, or IIb (based on degree of benefit outweighing risk) and LOE is A, B, or C (based on quality of supporting clinical trials) with B and C delineating whether the available evidence is randomized (R), nonrandomized (NR), limited data (LD), or expert opinion (EO).
The 2018 Cholesterol Guideline emphasizes that only certain lipid-lowering drug classes have evidence demonstrating reductions in ASCVD. These include statins and, in some circumstances, a cholesterol absorption inhibitor (ezetimibe) and proprotein convertase subtilisin kexin type 9 (PCSK9) inhibitors (alirocumab and evolocumab).
Statin therapy, when recommended, is based on the potency of the statin defined by the average effects of a certain statin on LDL-C levels at a specific dose (Table 1). When high-intensity statin therapy is recommended, the corresponding goal is to reduce LDL-C by 50% or more. Similarly, when moderate-intensity statin therapy is recommended, the corresponding goal is to reduce LDL-C by 30%–49%. If goal is not attained, maximizing or intensifying the statin dose and/or intensity is recommended, followed by addition of a nonstatin agent in some circumstances. Low-intensity statin regimens are not recommended unless an extenuating circumstance (e.g., drug interactions, intolerance) is present.
| Table 1. Intensity Daily Doses of Statins as Defined in the 2018 Cholesterol Guideline |
| High Intensity |
Moderate Intensity |
Low Intensity |
|
| LDL-C loweringa |
≥50% |
30% to 49% |
<30% |
| Primary statinsb |
Atorvastatin 40c–80 mg
Rosuvastatin 20–40 mg |
Atorvastatin 10–20 mg
Rosuvastatin 5–10 mg
Simvastatin 20–40 mg |
Simvastatin 10 mg |
| Other statins d |
Pravastatin 40–80 mg
Lovastatin 40–80 mg)
Fluvastatin XL 80 mg
Fluvastatin 40 mg twice daily
Pitavastatin 1–4 mg |
Pravastatin 10–20 mg
Lovastatin 20 mg
Fluvastatin 20–40 mg |
|
Source: Reference 11.
Abbreviations used: LDL-C, low-density lipoprotein cholesterol. Boldface type indicates specific statins and doses evaluated in randomized controlled trials.2
a LDL-C lowering that should occur with the dosage
b Reductions with atorvastatin, rosuvastatin, simvastatin estimated using median reduction from the VOYAGER database41
c Only one randomized controlled trial used atorvastatin 40 mg as a down-titration option for patients unable to tolerate atorvastatin 80 mg.42
d Expected LDL-C reductions for fluvastatin, lovastatin, pitavastatin, pravastatin according to FDA-approved product labeling. |
Nonstatin medications are not recommended for routine use. However, ezetimibe and the PCSK9 inhibitors have a role in combination with maximally tolerated statin therapy in certain patients.
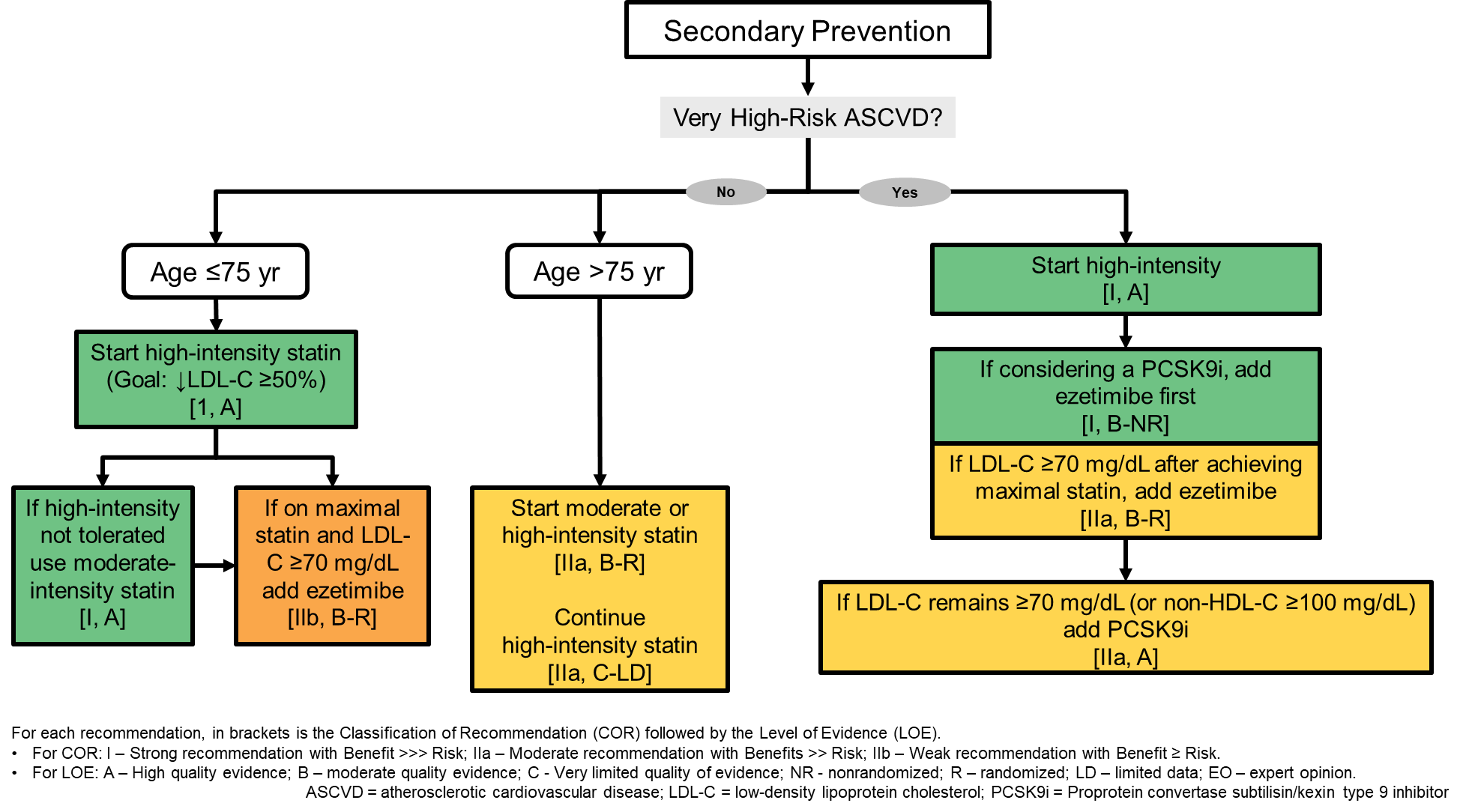
Secondary Prevention
Recommendations for secondary prevention (patients with clinical ASCVD) are outlined in Figure 1.16 The initial step in evaluating this population it to ascertain if the patient has very-high-risk recurrent clinical ASCVD (Table 2). Very-high-risk patients have a history of more than one major ASCVD event or if they have had one major ASCVD event coupled with multiple high-risk conditions.
| Figure 1. 2018 Cholesterol Guideline Recommendations for the Treatment of Secondary Prevention Patients11 |
 |
| Table 2. Very-High-Risk Clinical Atheroscerotic Cardiovascular Disease (ASCVD) |
History of multiple major ASCVD events
or
1 major ASCVD event and multiple high-risk conditions |
Major ASCVD Events |
- Recent acute coronary syndrome (within past 12 months)
- Prior myocardial infarction (other than recent ACS event listed above)
- Prior ischemic stroke
- Symptomatic peripheral arterial disease
|
| High-Risk Conditions |
- Age ≥65 years
- Current smoking
- LDL-C ≥100 mg/dL despite maximally tolerated statin and ezetimibe
- History of:
- Chronic kidney disease (eGFR 15–59 mL/min/1.73 m2)
- Congestive heart failure
- Coronary revascularization other than the initial major ASCVD event(s)
- Diabetes mellitus
- Heterozygous familial hypercholesterolemia
- Hypertension
|
Source: Reference 11.
Abbreviations used: ASCVD, atherosclerotic cardiovascular disease; eGFR, estimated glomerular filtration rate. |
High-intensity statin therapy, with the dose optimized to achieve LDL-C reduction of at least 50%, is the initial recommendation for all patients with clinical ASCVD who are 75 years of age or younger (COR I, LOE A recommendation).11 For patients older than 75 years, clinicians have the option of starting moderate- or high-intensity statin therapy, or continuing high-intensity statin therapy for patients already treated with high-intensity statin therapy.
Most patients with clinical ASCVD are considered very high risk. In the 2018 Cholesterol Guideline, recommendations for this patient population have been expanded based on recent evidence with nonstatin therapy.12,14,15 If LDL-C remains at or above 70 mg/dL during high-intensity statin therapy with the dose/intensity maximized as needed, ezetimibe can be added. Thereafter, if LDL-C continues to remain at or above 70 mg/dL, adding a PCSK9 inhibitor is reasonable.
Ezetimibe is recommended as the first nonstatin add-on medication in this situation based on data from a large Veterans Affairs cohort study. In that trial, ezetimibe added to maximal statin therapy lowered LDL-C to below 70 mg/dL in most patients.17 The recommendation was also influenced by the cost of PCSK9 inhibitors. At the time the 2018 Cholesterol Guideline was written, the list price of PCSK9 inhibitors was approximately $14,000 annually, which correlated to benefit of more than $150,000 per quality-adjusted life-year (QALY). Because of that less-than-optimal ratio, the 2018 Cholesterol Guideline recommended third-line use of PCSK9 inhibitors. The manufacturers of the two PSCK9 inhibitors later reduced their list prices to less than $6,000 annually; this lower price point could make these agents moderate or possibly high value in very-high-risk secondary-prevention patients.
Primary Prevention
Recommendations for use of lipid-lowering therapies for primary prevention are outlined in Figure 2.16 The first step in evaluating patients for primary prevention is to determine if they are in a statin benefit group based on baseline LDL-C or presence of diabetes and/or other risk-enhancing factors.
| Figure 2. 2018 Cholesterol Guideline Recommendations for the Treatment of Primary Prevention Patients11 |
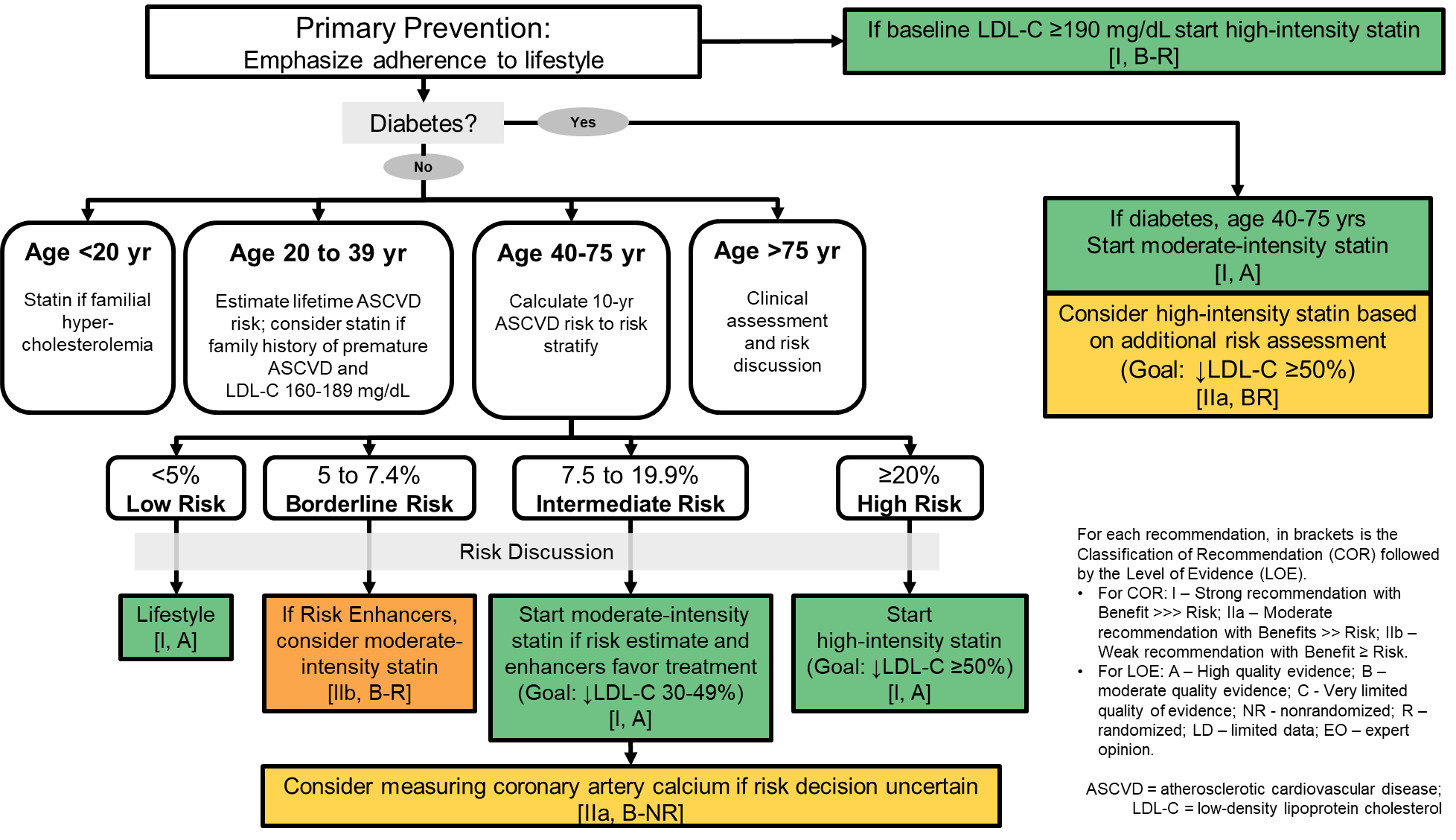 |
Severe Hypercholesterolemia. Patients with baseline LDL-C values of 190 mg/dL or more are considered to have severe hypercholesterolemia. Many of these patients have familial hypercholesterolemia, but genetic testing is not necessary because having severe LDL-C elevation is sufficient to establish a high risk of ASCVD. For patients ages 20–75 years, high-intensity, maximally tolerated statin therapy should be initiated (COR I, LOE B-R recommendation).11 For these patients, a reduction in LDL-C of 50% or more is needed to lower ASCVD risk. If not achieved with maximally tolerated statin therapy, the 2018 Cholesterol Guideline recommends addition of ezetimibe, a bile acid sequestrant, and/or a PCSK9 inhibitor. However, the value of PCK9 inhibitors was considered uncertain in the 2018 Cholesterol Guideline because long-term clinical trials evaluating reduction in ASCVD among primary-prevention patients with severe hypercholesterolemia with PCSK9 inhibitors were not available.
Diabetes Mellitus. Diabetes is a major independent risk factor for ASCVD. Primary-prevention patients should be evaluated on an individual basis by calculating their 10-year risk score using the Pooled Cohort Equations and considering risk-enhancing factors (Table 3). The Pooled Cohort Equations calculator introduced in the 2013 ACC/AHA guideline is also recommended in the 2018 Cholesterol Guideline for risk evaluation in primary-prevention patients with LDL-C less than 190 mg/dL.18 This calculator estimates 10-year risk of ASCVD, which includes coronary heart disease and symptomatic carotid artery disease. The tool used to perform this calculation has been enhanced and calculates lifetime ASCVD risk in patients age 20–59 (ASCVD Risk Estimator Plus; it is available at: http://tools.acc.org/ASCVD-Risk-Estimator-Plus/#!/calculate/estimate/).
| Table 3. Risk-Enhancing Factors as Defined in the 2018 Cholesterol Guideline |
| Patient Characteristics |
- Family history of premature ASCVD (males, age <55 years; females, age <65 years)
- Primary hypercholesterolemia (LDL-C, 160–189 mg/dL or non–HDL-C 190–219 mg/dL)
- Metabolic syndrome (increased waist circumference, elevated triglycerides [>175 mg/dL], elevated blood pressure, elevated glucose, and low HDL-C [<40 mg/dL in men; <50 in women mg/dL])
- High-risk race/ethnicities (e.g., South Asian ancestry)
|
| Medical History |
- Chronic kidney disease (eGFR 15–59 mL/min/1.73 m2 with or without albuminuria, and not dialysis or kidney transplantation)
- Chronic inflammatory conditions (e.g., psoriasis, rheumatoid arthritis, HIV)
- Premature menopause (< 40 years) and pregnancy-associated conditions that increase later ASCVD risk (e.g., preeclampsia)
|
| Lipid/Biomarkers |
- Persistently elevated, primary hypertriglyceridemia (≥175 mg/dL)
- In select individuals, abnormal biomarkers if measured:
- High-sensitivity C-reactive protein ≥2.0 mg/L
- Lipoprotein(a) ≥50 mg/dL (especially higher levels)
- Apolipoprotien B ≥130 mg/dL (corresponds to LDL-C >160 mg/dL)
- Ankle brachial index <0.9
|
| Diabetes-Specific |
- Long duration (≥10 years for type 2 or ≥20 years for type)
- Albuminuria ≥30 mcg of albumin/mg creatinine
- eGFR <60 mL/min/1.73 m2
- Retinopathy
- Neuropathy
- Ankle brachial index <0.9
|
Source: Reference 11.
Abbreviations used: ASCVD, atherosclerotic cardiovascular disease; eGFR, estimated glomerular filtration rate; HDL-C, high-density lipoprotein cholesterol; HIV, human immunodeficiency virus; LDL-C, low-density lipoprotein cholesterol. |
The strongest and most foundational recommendation for primary-prevention patients with diabetes (type 1 or type 2) is moderate-intensity statin therapy for those aged 40 to 75 years, regardless of 10-year ASCVD risk score (COR I, LOE A recommendation).11 If a patient is at higher ASCVD risk (determination based on clinical judgment), it is reasonable to use high-intensity statin therapy with a goal LDL-C reduction of 50% or more (COR IIa, LOE B-R recommendation).11 The 2018 Cholesterol Guideline highlights multiple ways for clinicians to use their judgment to identify higher risks in diabetes:
- Multiple ASCVD risk factors
- Multiple risk factors or age 50 to 75 years
- Men >50 years of age and women >60 years of age
- As patients age or develop risk modifiers
- 10-year ASCVD risk ≥20%
It is reasonable to continue statin therapy in primary-prevention patients with diabetes when they reach 75 years of age. Moreover, it may be reasonable to begin statin therapy in adults in this age group after a clinician–patient discussion of potential benefits and risks.
In patients ages 20 to 39 years, statin therapy can be initiated when diabetes-specific risk enhancers are present (Table 3).
Other Patients. For patients without severe hypercholesterolemia or diabetes who are candidates for primary prevention, the 10-year ASCVD risk score should be used to assess the need for therapy. Age is an important consideration in this decision (Figure 2).
For those 20–39 years of age, lifestyle interventions can be recommended based on lifetime ASCVD risk. For patients age 40–75 years, the 10-year ASCVD risk score can be categorized as depicted in Figure 2 as low risk (<5%), borderline risk (5%–7.4%), intermediate risk (7.5%–19.9%), or high risk (≥20%), and a patient–clinician discussion of these risks should guide therapy.11
This discussion should cover risk factors, adherence to healthy lifestyle, potential for ASCVD risk-reduction benefits, and potential for adverse effects and drug–drug interactions, as well as patient preferences. Individualized treatment decisions should consider these recommendations in cholesterol guidelines:
- Low Risk: Lifestyle modification only.
- Borderline Risk: Moderate-intensity statin therapy may be considered, but only if risk-enhancing factors are present, and only after a patient-clinician discussion of risk (COR IIb, LOE B-R recommendation).11
- Intermediate Risk: Moderate-intensity statin therapy should be started, with LDL-C reduced 30%–49%, when risk-enhancing factors are present because risk-enhancing factors favor initiation or intensification of statin therapy (COR I, LOE A recommendation).11 Coronary artery calcium (CAC) scoring should be considered if the decision to treat is uncertain. If the CAC score is 0, it is reasonable to withhold statin therapy and reassess in 5 to 10 years if higher risk conditions are absent (diabetes mellitus, family history of premature ASCVD, cigarette smoking). If CAC is 1 to 99, it is reasonable to start moderate-intensity statin therapy if patients have reached age 55 years. If CAC is 100 or greater (or in the 75th percentile) it is reasonable to start moderate-intensity statin therapy regardless of age.
- High Risk: High-intensity statin therapy should be started, with LDL-C reduced by 50% or more (COR I, LOE A recommendation).11
In primary-prevention patients older than 75 years of age whose LDL-C is 70–89 mg/dL, the 2018 Cholesterol Guidelines recommend moderate-intensity statin therapy as reasonable. However, when these patients have functional decline (physical or cognitive), multimorbidity, frailty, or reduced life expectancy, statin therapy can reasonably be stopped; potential benefits are limited in these situations.
Implementing Evidence-Based Therapy
Several implementation strategies are recommended in the 2018 Cholesterol Guidelines to optimize the use of evidence-based recommendations and therapies and enhance patient adherence.11 A patient–clinician discussion should occur to promote shared decision-making before therapy is prescribed (Table 4).
| Table 4. Checklist for Clinician–Patient Shared Decision Making for Initiating Therapy |
| Items |
Recommendations |
| ASCVD risk assessment |
- Determine if in a statin treatment group; use ASCVD Risk Estimator Plusa if
- Primary-prevention adults age 40–75 years with LDL-C ≥70 mg/dL
- Not needed if secondary prevention, LDL-C ≥190 mg/dL, or diabetes age 40–75 years
- Assess for presence of risk-enhancing factors
- Assess coronary artery calcification if risk decision is uncertain
- Use decision tools to explain risk (e.g., ASCVD Risk Estimator Plus,a Mayo Clinic Statin Choice Decision Aid)
|
| Lifestyle modifications |
- Review lifestyle habits (e.g., diet, physical activity, body mass index, tobacco use)
- Endorse a healthy lifestyle and provide relevant advice, materials, or referrals
|
| Potential net clinical benefit from pharmacotherapy |
- Recommend and explain statins as first-line therapy
- Consider combination statin/nonstatin therapy in selected patients
- Discuss potential risk reduction from lipid-lowering therapy
- Discuss the potential for adverse effects or drug–drug interactions
|
| Cost considerations |
- Discuss potential out-of-pocket cost of therapy (e.g., insurance plan coverage, tier level, copayment)
|
| Shared decision making |
- Encourage the patient to verbalize what was heard
- Invite the patient to ask questions, express values and preferences, and state ability to adhere to lifestyle changes and medications
- Refer patients to trustworthy materials to aid in their understanding of issues regarding risk decisions
- Collaborate with the patient to determine therapy and follow-up plan
|
Source: Reference 11.
Abbreviations used: ASCVD, atherosclerotic cardiovascular disease; LDL-C, low-density lipoprotein cholesterol.
ahttp://tools.acc.org/ASCVD-Risk-Estimator-Plus/#!/calculate/estimate/ |
Prospective interventions focused on improving adherence to prescribed therapy are recommended. These include telephone reminders, calendar reminders, integrated multidisciplinary educational activities, and pharmacist-led interventions. Pharmacist-led interventions should focus on optimizing medication regimens.
Population health interventions involving clinicians, health systems, and health plans are recommended to identify patients who are not receiving guideline-directed medical therapy. After identifying these gaps in care, appropriate guideline-directed medical therapy should be implemented using multifaceted strategies. Importantly, evaluating the effects of therapy on LDL-C levels at 4 to 12 weeks after the start or any change in therapy is essential to identify patients needing intensification of therapy.
LIPID-LOWERING PHARMACOTHERAPY
Several different lipid-lowering medications are described in Table 5. Statins, ezetimibe, bile acid sequestrants, and the PCSK9 inhibitors are used to lower LDL-C. Fibric acid derivatives and omega-3 fatty acids are used to lower elevated triglycerides (TGs).
| Table 5. Description of Lipid-Lowering Medications |
| Drug Class |
Agents |
Mechanism of Action |
Lipoprotein
Changes 10,33 |
Evidence-Based Reductions in ASCVD11 |
Safety considerations |
| Statin |
- Atorvastatin
- Fluvastatin
- Lovastatin
- Pitavastatin
- Pravastatin
- Rosuvastatin
- Simvastatin
|
Competitively inhibits HMG-CoA reductase to inhibit cholesterol synthesis in the liver, resulting in increased expression of LDL-receptors that accelerates uptake of LDL from blood to liver |
LDL-C: ↓ 18%–55%
HDL-C: ↑ 5–15%
TGs: ↓ 7–30% |
Numerous clinical trials demonstrate proven reductions in primary and secondary prevention |
- Muscle-related side effects
- Small increase in risk of new onset diabetes
- Drug–drug interactions (agent specific)
|
| Cholesterol absorption inhibitor |
|
Blocks the Niemann-Pick C1-Like 1 receptor to inhibit absorption of cholesterol, leading to decreased delivery of intestinal cholesterol to the liver reducing hepatic cholesterol stores and increasing cholesterol clearance from the blood |
LDL-C: ↓ 13%–20%
HDL-C: ↑ 3%–5%
TGs: ↓ 5%–11% |
One clinical trial in secondary prevention showing reduced CV events in combination with moderate-intensity statin12 |
- Small increased risk of elevated hepatic transaminases when used with a statin
|
| Bile acid sequestrant |
- Colesevelam
- Colestipol
- Cholestyramine
|
Binds intestinal bile acids, impeding reabsorption, upregulating cholesterol 7-α-hydroxylase, which increases conversion of cholesterol to bile acids with the increased cholesterol demand in the liver increasing hepatic LDLRs and increasing cholesterol clearance from the blood |
LDL-C: ↓ 15%–30%
HDL-C: ↑ 3%–5%
TGs: ↓ 0%–10% |
One clinical trial in primary prevention men showed reduced CV events with cholestyramine |
- Can raise serum TG values
- Gastrointestinal side effects
|
| PCSK9 inhibitor |
|
Binds PCSK9, which normally binds to LDLRs to promote LDLR degradation (LDLR is the primary receptor that clears circulating LDL); by inhibiting PCSK9 binding to LDLRs, there are increased number of LDLRs and results in increased cholesterol removal |
LDL-C: ↓ 40%–72%
HDL-C: ↑ 0%–10%
TGs: ↓ 0%–17% |
Two clinical trial in very-high-risk secondary-prevention patients showing reduced CV events in combination with maximally tolerated statins14,15 |
|
| Fibric acid derivative |
- Fenofibrate
- Fenofibric acid
- Gemfibrozil
|
Activates PPARα to increase lipolysis and elimination of triglyceride-rich particles from plasma by activating lipoprotein lipase, reducing Apo CIII production, and increasing synthesis of HDL-C and Apo AI and AII |
LDL-C: ↓ 5%-↑ 20%
HDL-C: ↑ 10%-20%
TGs: ↓ 20%-50% |
One clinical trial in primary prevention and one clinical trial in secondary prevention showed reduced CV events with gemfibrozil vs. placebo One primary prevention clinic trial in diabetes of fenofibrate in combination with a statin failed to show differences in CV events |
- Adjust dose in renal dysfunction
- Small increase in serum creatinine concentrations (especially fenofibrate or fenofibric acid)
- Gallstones
- Increase risk of myopathy when used with a statin (especially with gemfibrozil)
|
| Omega-3 fatty acids |
- Icosapent ethyl (EPA only)
- Omega-3-acid ethyl esters
- Omega-3 carboxylic acid
|
Not been well defined; EPA reduces VLDL TG synthesis and/or secretion and enhances TG clearance from circulating VLDL particles. May also increase β-oxidation; inhibit DGAT, decrease lipogenesis, and increase lipoprotein lipase activity. |
LDL-C: ↓ 6%-↑ 25%
HDL-C: ↓ 5%-↑ 7%
TGs: ↓ 19%-44% |
One clinical trial (EPA only) in patients with triglycerides values of 135-499 mg/dL who were secondary prevention or primary prevention with diabetes and additional risk factors, showing reduced CV events in combination maximally tolerated statin34 |
- DHA containing products may increase LDL-C concentration
|
| Abbreviations used: CV, cardiovascular; DGAT, diacylglycerol acyltransferase; DHA, docosahexaenoic acid; EPA, eicosapentaenoic acid; HDL-C, high density lipoprotein cholesterol; HMG-CoA, 3-hydroxy-3-methylglutaryl-coenzyme A; LDL-C, low density lipoprotein cholesterol; LDLR, LDL receptor; PCSK9, proprotein convertase subtilisin kexin type 9; PPARα, peroxisome proliferator activated receptor α; TG, triglycerides; VLDL, very low density lipoprotein. |
Statins
Statins have the best evidence of effectiveness for reducing both LDL-C and risk of ASCVD. All statins except pitavastatin are available as less expensive generic alternatives. Most statins should be administered in the evening so that they can maximally inhibit 3-hydroxy-3-methylglutaryl-coenzyme A (HMG CoA) reductase. However, atorvastatin, pitavastatin, and rosuvastatin can be administered at any time of the day due to their long half-lives.
Adverse Effects
Most patients tolerate statin therapy well. Some patients experience “intolerance” to this class of drugs, primarily because of statin-associated muscle symptoms (SAMS). The 2018 Cholesterol Guideline and a 2019 AHA Scientific Statement both address statin safety and conclude that in patients for whom statin treatment is recommended, the benefits greatly outweigh the risks.11,19 The prevalence of statin “intolerance” is unknown but is estimated to as high as 10%.20
The 2018 Cholesterol Guidelines concluded that SAMS, new-onset diabetes, and transaminase elevations are rare but do occur with statin use.11 However, the association between statin use and memory/cognition changes, cancer, renal dysfunction, tendon rupture, interstitial lung disease, low testosterone, cataracts, and hemorrhagic stroke lack requisite data to confirm their association based on the extensive review of evidence by the 2018 Cholesterol Guideline group.
Statin-Associated Muscle Symptoms. The constellation of SAMS includes myalgia, myositis/myopathy, rhabdomyolysis, and the very rare statin-associated autoimmune myopathy.11
Myalgia is unexplained muscle discomfort; it can present as aches, soreness, stiffness, tenderness, or cramping during or after exercise.21 Patients with myalgia have normal serum creatine kinase (CK) values. The incidence of myalgia is up to 10% in observational studies, but is 1%–5% in prospective randomized controlled trials.11 Predisposing factors include age, female sex, low body mass index, concomitant use of high-risk medications (cytochrome P450 3A4 inhibitors, organic anion transporting polypeptide 1B1 inhibitors), comorbidities (human immunodeficiency virus [HIV] infections; renal, liver, thyroid disorders; preexisting myopathy), Asian ancestry, excessive alcohol intake, high levels of physical activity, and trauma.
Myositis/myopathy is weakness not attributed to pain that is associated with elevated serum CK values above the upper limit of normal. Myositis implies muscle inflammation, with the extent of myonecrosis correlating with the degree of serum CK elevation.21 Myositis/myopathy is considered rarely associated with statin therapy.
Rhabdomyolysis is considered very rare, yet is the most serious adverse effect associated with statin therapy.11,21 Patients typically present with myalgia and serum CK of more than 10 times the upper limit of normal (typically more than 50 times the upper limit of normal).
Management strategies for addressing SAMS depend on the clinical presentation. For patients with myositis/myopathy or rhabdomyolysis, statin therapy should be stopped and patients triaged for immediate medical care, especially for rhabdomyolysis. For patients with myalgia, a thorough assessment of symptoms is recommended, along with evaluation for nonstatin causes and predisposing factors.11 Secondary causes of SAMS that can be mitigated include changes in exercise, drug–drug interactions, hypothyroidism, or vitamin D deficiency.
In the absence of a reversible secondary cause of SAMS that is not considered severe, recommendations are to reassess and rechallenge to achieve maximal LDL-C lowering using a modified dosing regimen, an alternative statin, or a statin–nonstatin combination regimen.11 For severe myalgia, the patient evaluation should always include measuring serum CK and evaluating objective muscle weakness. If symptoms suggest hepatotoxicity, liver transaminases (including total bilirubin and alkaline phosphatase) should be measured. It is important to note that serum CK and liver transaminases should not be routinely measured in the absence of SAMS.11 Moreover, the 2018 Cholesterol Guidelines state that coenzyme Q10 (a dietary supplement) is not recommended for routine use in patients treated with statins or to treat SAMS.11
New-Onset Diabetes: Statin therapy has been associated with a dose-dependent but modest 10%-12% increase in risk of developing type 2 diabetes.11,22-25 This possibility is included in statin product labeling. However, the risk of new-onset diabetes is offset by the 25%–35% reduction in CV events. Based on the Cholesterol Treatment Trialist data, treating 255 patients with statin therapy for over 4 years would result in 1 case of new-onset diabetes but would prevent 5.4 cases of death or nonfatal myocardial infarction.26,27
Patients at risk for new-onset diabetes are those who have additional risk factors for diabetes, including body mass index of 30 kg/m2 or more, fasting blood glucose of 100 mg/dL or more, metabolic syndrome, or glycosylated hemoglobin of 6% or more).11,25 The 2018 Cholesterol Guideline recommends statin therapy even in such patients because benefits of treatment outweigh their risks.11
Hepatic Effects: Transaminase elevations of more than 3 times the upper limit of normal have been reported with statin therapy.11 However, this is rare and does not require routine evaluation of serum hepatic transaminases. Importantly, the incidence of hepatic failure with statin therapy is so rare that it is comparable to the risk of idiopathic hepatic failure.20
Cognitive Effects: Several years ago, the Food and Drug Administration (FDA) issued a warning about mild impaired cognition (memory loss, forgetfulness, and confusion) with statin therapy.28 While the onset of symptoms is variable, symptoms are reported to be reversible within a few weeks of stopping statin therapy.
The FDA warning implies that these adverse effects can occur with all statins; however, a 2014 NLA safety report states that most published case reports of cognitive adverse effects are with simvastatin and atorvastatin, both lipophilic statins.29 Similarly, the 2018 Cholesterol Guideline and other published analyses did not identify convincing data to confirm the association between statin therapy and cognitive side effects.11,30,31
Reducing the statin dose, stopping the statin, or rechallenge with a hydrophilic statin (e.g., pravastatin or rosuvastatin) are possible options for patients complaining of cognitive side effects.29
Ezetimibe
Ezetimibe modestly lowers LDL-C without effects on other lipid parameters. It is well tolerated without major drug–drug interactions.
In the IMPROVE-IT trial, ezetimibe reduced the risk of ASCVD events when used in combination with a moderate-intensity statin therapy in patients with very-high-risk clinical ASCVD.12 IMPROVE-IT also provided evidence demonstrating reductions in CV events with statin–ezetimibe combination therapy, and recommendations for use were incorporated into the 2018 Cholesterol Guideline.11 However, overall benefits were modest in relation to the relative ASCVD risk reduction, and it was studied in combination with moderate-intensity statin therapy, not high-intensity statin therapy.
PCSK9 Inhibitors
The PCSK9 inhibitors are bioengineered monoclonal antibodies. Alirocumab and evolocumab are administered as subcutaneous injections every 2 to 4 weeks. They are expensive agents, but both have had significant price reductions (from their original list price of approximately $14,000 annually to $5,850 annually). These agents are available only through specialty pharmacies, but with the price reduction, they may become available in other pharmacies.
The primary side effects that patients may experience with PCSK9 inhibitors are injection site reactions; otherwise, the agents are relatively well tolerated. Neurocognitive side effects were initially thought to occur with PCSK9 inhibitors. However, ongoing safety analyses did not show changes in neurocognitive function with PCSK9 inhibitors in comparison with placebo.14,15,32
The PCSK9 inhibitors reduce LDL-C levels up to 72%.33 Two large placebo-controlled randomized clinical trials, the FOURIER with evolocumab and ODDYSEY-Outcomes with alirocumab, both demonstrated that adding a PCSK9 inhibitor to statin therapy in patients with very-high-risk clinical ASCVD further reduces the risk of ASCVD events.14,15The magnitude of ASCVD event reductions were greater than what was seen with ezetimibe in IMPROVE-IT. Most patients in FOURIER and ODDYSEY-Outcomes were also treated with high-intensity statin therapy. Based on these results, the addition of a PCSK9 inhibitor to maximally tolerated statin therapy in very-high-risk clinical ASCVD was incorporated into the 2018 Cholesterol Guideline, but addition of ezetimibe first is recommended.11
The primary role of PCSK9 inhibitors is for very-high-risk patients with ASCVD or with very high baseline LDL-C values (patients with familial hypercholesterolemia). The FDA indication for alirocumab and evolocumab is as an adjunct to diet and maximally tolerated statin therapy for the treatment of adults with heterozygous familial hypercholesterolemia (HeFH) or ASCVD who require additional LDL-C lowering. Evolocumab is also indicated for homozygous familial hypercholesterolemia (HoFH).
Bile Acid Sequestrants
The only lipid-lowering medications that are not systemically absorbed are bile acid sequestrants. These agents modestly lower LDL-C and are ideally used in combination with a statin. While these agents have no known systemic adverse effects, many patients experience gastrointestinal side effects (bloating, cramping, constipation).
Moreover, these drugs can have drug–drug interactions that result in decreased absorption of other drugs when administered concurrently; this is less frequent with colesevelam. Other less common side effects include decreased absorption of fat-soluble vitamins and increased triglycerides.
Other Agents
Fibric acid derivatives and omega-3 fatty acids are primarily used to treat hypertriglyceridemia. These agents are summarized in Table 5. For the treatment of hypertriglyceridemia, the 2018 Cholesterol Gguideline recommends consideration of intensifying or starting a statin for patients with persistently moderate or severe hypertriglyceridemia (fasting triglyceride values ≥150 mg/dL) in patients age 40–75 years when 10-year ASCVD risk is 7.5% or more.11 Because the primary health risk associated with very high triglycerides is pancreatitis, these guidelines also recommend fibric acid derivatives or omega-3 fatty acids in patients with elevated triglycerides (500–999 mg/dL), especially in those whose serum triglycerides exceed 1000 mg/dL.
Two omega-3 fatty acids, eicosapentaenoic acid (EPA) and docosapentaenoic acid (DPA), are useful for lowering triglycerides. Three omega-3 fatty acid products are approved by FDA for hypertriglyceridemia (triglycerides ≥500 mg/dL). One product, icosapent ethyl, contains only EPA, while the other two contain both EPA and DPA.
The EPA-only product, icosapent ethyl, was studied in the REDUCE-IT trial, a large prospective randomized placebo-controlled trial. In REDUCE-IT, icosapent ethyl was added to statin therapy in patients with either clinical ASCVD (secondary prevention) or diabetes (primary prevention) whose triglyceride values were 135–499 mg/dL. After multiple years, icosapent ethyl significantly reduced the risk of ischemic events, including cardiovascular death.34
These data were not available when the 2018 Cholesterol Guideline was created, but they will certainly influence therapy in the future in patients with persistently elevated triglycerides.
OTHER POPULATIONS
The 2018 Cholesterol Guideline includes many recommendations for racial/ethnic populations at risk for ASCVD, women, patients with chronic kidney disease, adults with chronic inflammatory disorders or HIV infections. Detailed recommendations are provided in the complete guideline.11
Children and Adolescents
Healthy lifestyles and behavior modification are primary risk reduction approaches to prevent abnormalities in children and adolescents. Moreover, certain pediatric patients are at high risk for ASCVD, including those with HoFH, in whom ASCVD is evident in the first and second decades of life.35,36
Previous NCEP guidelines recommended cholesterol screening in select patients aged 2–19 years.37,38 The 2018 Cholesterol Guideline recommends more specific screening based on a family history.11 Measuring fasting or nonfasting lipid panel is recommended as early as 2 years of age in children with a family history of premature ASCVD or significant hypercholesterolemia. It is reasonable to measure a fasting or nonfasting lipid panel once between the ages of 9 and 11 years, and again between the ages of 17 and 21 years for children and adolescents without such family history.
Lipid-lowering drug therapy —generally statins — may be considered in this age group when lifestyle therapy is insufficient. Lipid-lowering drug therapies have been studied primarily in pediatric patients with either HoFH or HeFH. Many agents are approved for use in pediatric patients, with differences in approved ages and doses (see Table 6).
| Table 6. Lipid-Lowering Drug Therapies in Pediatric Patientsa |
| |
Approved Age (yr) |
Approved Starting Dose |
Approved Maximum Daily Dose |
| Statins |
|
|
|
· Atorvastatin
· Fluvastatin
· Lovastatin
· Pravastatin
· Simvastatin
· Rosuvastatin |
10–17
10–16
10–17
8–13/14-18
10–17
7–17 |
10 mg
20 mg
10 mg
20 mg/40 mg
10 mg
5–20 mg |
20 mg
80 mg
20 mg
20 mg/40 mg
40 mg
20 mg |
| Ezetimibe |
≥10 |
10 mg |
10 mg |
| Bile Acid Sequestrants |
|
|
|
· Colesevelam
· Cholestyramine |
10–17
NA |
3.75 g
240 mg/kg/db |
3.25 g
8 g |
a Information is from FDA-approved product labeling for these medications. Safety and efficacy not established in pediatric patients for pitavastatin, PCSK9 inhibitors, fibric acid derivatives, omega-3 fatty acids, niacin, lomitapide, and mipomersen.
Abbreviation used: NA, not applicable.
b In three divided doses. |
Older Patients
With age, people have increasing risk of ASCVD. In fact, advanced age (45 years or older for men, 55 years or older for women) is considered a major independent risk factor for ASCVD regardless of medical history.
There is general consensus that older adults who need secondary prevention should be treated with statin therapy.11,39 Other lipid-lowering drug therapies have not been as well studied. The 2018 Cholesterol Guideline has age-specific recommendations to limit adverse effects and recommends moderate-intensity statin therapy (instead of high-intensity) for secondary-prevention patients older than 75 years.11 Although the precise benefits of statin therapy are less clear in older patients who need primary prevention, the Cholesterol Treatment Trialist data suggest benefit outweighs risk but not to the degree as in secondary prevention.39
Clinicians should feel comfortable in using statin-based therapy in older patients, but should always use clinical judgment to assess risk and benefits. For older adults who require lipid-lowering drug therapy, factors such as risk of drug–drug interactions, adverse effects, decreased drug elimination, and cost should be considered. Statins have the strongest evidence in older patients with hypercholesterolemia. However, adverse effects and drug–drug interactions can be potentially more common in the older adult. Pharmacokinetic changes with statins have been demonstrated in older patients, but statins generally do not require an empiric dose adjustment that is based on age (Table 7).40
| Table 7. Summary of FDA Product Label Dosing Recommendations for Statins in Older Patients |
| Statins |
Pharmacokinetic Changes |
Recommendations for Older Patients |
| Fluvastatin |
· Plasma levels not significantly changed |
· No dose adjustment |
| Lovastatin |
· Mean plasma level ~45% higher in older patients (70–78 years of age) |
· No dose adjustment |
| Pravastatin |
· Mean AUC 25%–50% higher in older patients
· Mean Cmax, Tmax, and t½ similar |
· No dose adjustment |
| Atorvastatin |
· Cmax 40% and AUC 30% higher in healthy older patients (≥65 years) |
· No dose adjustment
· Greater sensitivity of some older adults cannot be ruled out |
| Rosuvastatin |
· No different in plasma concentrations between younger and older patients (≥ 65 years) |
· No dose adjustment
· Greater sensitivity of some older adults cannot be ruled out |
| Simvastatin |
· Mean plasma level ~45% higher in older patients (70–78 years) |
· No dose adjustment
· Greater sensitivity of some older adults cannot be ruled out |
| Pitavastatin |
· Cmax 10% and AUC 30% higher in the older patients (≥65 years) |
· No dose adjustment
· Greater sensitivity of some older adults cannot be ruled out |
Source: Reference 40.
Abbreviations used: AUC, area under the serum concentration–time curve; Cmax, maximum serum concentration; Tmax, time of maximum serum concentration. |
CONCLUSION
The 2018 Cholesterol Guideline recommends evidence-based approaches to treating most patients with hypercholesterolemia. These recommendations carry forward the approach of starting fixed-intensity statin therapy in patients in one of the four 2013 ACC/AHA blood cholesterol guideline–defined groups. However, intensifying therapy is now recommended when goal percentage reduction in LDL-C is not achieved. Moreover, nonstatin medications are recommended add-on therapies, primarily in patients with clinical ASCVD or baseline LDL-C values of 190 mg/dL or more. For other patients requiring primary prevention, clinicians should consider the 10-year risk of ASCVD and the presence of risk-enhancing features when determining need for statin therapy. For all patients, shared decision-making is strongly recommended.
REFERENCES
- Benjamin EJ, Muntner P, Alonso A, et al. Heart disease and stroke statistics—2019 update: a report from the American Heart Association. Circulation. 2019:CIR0000000000000659.
- Baigent C, Blackwell L, Emberson J, et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376:1670-1681.
- Chisholm-Burns MA, Kim Lee J, Spivey CA, et al. US pharmacists' effect as team members on patient care: systematic review and meta-analyses. Med Care. 2010;48:923-933.
- Sandhoff BG, Nies LK, Olson KL, Nash JD, Rasmussen JR, Merenich JA. Clinical pharmacy cardiac risk service for managing patients with coronary artery disease in a health maintenance organization. Am J Health Syst Pharm. 2007;64:77-84.
- Santschi V, Chiolero A, Paradis G, Colosimo AL, Burnand B. Pharmacist interventions to improve cardiovascular disease risk factors in diabetes: a systematic review and meta-analysis of randomized controlled trials. Diabetes Care. 2012;35:2706-2717.
- Santschi V, Chiolero A, Burnand B, Colosimo AL, Paradis G. Impact of pharmacist care in the management of cardiovascular disease risk factors: a systematic review and meta-analysis of randomized trials. Arch Intern Med. 2011;171:1441-1453.
- Expert Panel on Detection, Evaluation Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA. 2001;285:2486-2497.
- Grundy SM, Cleeman JI, Merz CN, et al. Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III guidelines. Circulation. 2004;110:227-239.
- Stone NJ, Robinson JG, Lichtenstein AH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129:S1-S45.
- Jacobson TA, Ito MK, Maki KC, et al. National Lipid Association recommendations for patient-centered management of dyslipidemia: part 1 — executive summary. J Clin Lipidol. 2014;8:473-488.
- Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2018 Nov 3. pii: S0735-1097(18)39033-8. doi: 10.1016/j.jacc.2018.11.002. [Epub ahead of print]
- Cannon CP, Blazing MA, Giugliano RP, et al. Ezetimibe added to statin therapy after acute coronary syndromes. N Engl J Med. 2015;372:2387-2397.
- Yusuf S, Bosch J, Dagenais G, et al. Cholesterol lowering in intermediate-risk persons without cardiovascular disease. N Engl J Med. 2016;374:2021-2031.
- Sabatine MS, Giugliano RP, Keech AC, et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. 2017;376:1713-1722.
- Schwartz GG, Steg PG, Szarek M, et al. Alirocumab and cardiovascular outcomes after acute coronary syndrome. N Engl J Med. 2018;379:2097-2107.
- Grundy SM, Vega GL, McGovern ME, et al. Efficacy, safety, and tolerability of once-daily niacin for the treatment of dyslipidemia associated with type 2 diabetes: results of the assessment of diabetes control and evaluation of the efficacy of Niaspan trial. Arch Intern Med. 2002;162:1568-1576.
- Virani SS, Akeroyd JM, Nambi V, et al. Estimation of eligibility for proprotein convertase subtilisin/kexin type 9 inhibitors and associated costs based on the FOURIER trial (Further Cardiovascular Outcomes Research With PCSK9 Inhibition in Subjects With Elevated Risk): insights from the Department of Veterans Affairs. Circulation. 2017;135:2572-2574.
- Goff DC Jr, Lloyd-Jones DM, Bennett G, et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129:S49-S73.
- Newman CB, Preiss D, Tobert JA, et al. Statin safety and associated adverse events: a scientific statement from the American Heart Association. Arterioscler Thromb Vasc Biol. 2019;39:e38-e81.
- Jacobson TA. NLA Task Force on Statin Safety—2014 update. J Clin Lipidol. 2014;8:S1-S4.
- Rosenson RS, Baker SK, Jacobson TA, Kopecky SL, Parker BA. An assessment by the Statin Muscle Safety Task Force: 2014 update. J Clin Lipidol. 2014;8:S58-S71.
- Sattar N, Preiss D, Murray HM, et al. Statins and risk of incident diabetes: a collaborative meta-analysis of randomised statin trials. Lancet. 2010;375:735-742.
- Preiss D, Seshasai SR, Welsh P, et al. Risk of incident diabetes with intensive-dose compared with moderate-dose statin therapy: a meta-analysis. JAMA. 2011;305:2556-2564.
- Waters DD, Ho JE, Boekholdt SM, et al. Cardiovascular event reduction versus new-onset diabetes during atorvastatin therapy: effect of baseline risk factors for diabetes. J Am Coll Cardiol. 2013;61:148-152.
- Ridker PM, Pradhan A, MacFadyen JG, Libby P, Glynn RJ. Cardiovascular benefits and diabetes risks of statin therapy in primary prevention: an analysis from the JUPITER trial. Lancet. 2012;380:565-571.
- Maki KC, Ridker PM, Brown WV, Grundy SM, Sattar N, The Diabetes Subpanel of the National Lipid Association Expert Panel. An assessment by the Statin Diabetes Safety Task Force: 2014 update. J Clin Lipidol. 2014;8:S17-S29.
- Baigent C, Keech A, Kearney PM, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet. 2005;366:1267-1278.
- U.S. Food and Drug Administration. FDA Drug Safety Communication: important safety label changes to cholesterol-lowering statin drugs. Updated July 3, 2012, Available at: http://www.fda.gov/Drugs/DrugSafety/ucm293101.htm.
- Rojas-Fernandez CH, Goldstein LB, Levey AI, Taylor BA, Bittner V, The National Lipid Association's Safety Task Force. An assessment by the Statin Cognitive Safety Task Force: 2014 update. J Clin Lipidol. 2014;8:S5-S16.
- Richardson K, Schoen M, French B, et al. Statins and cognitive function: a systematic review. Ann Intern Med. 2013;159:688-97.
- Ott BR, Daiello LA, Dahabreh IJ, et al. Do statins impair cognition? A systematic review and meta-analysis of randomized controlled trials. J Gen Intern Med. 2015;30(3):348-358.
- Giugliano RP, Mach F, Zavitz K, et al. Cognitive function in a randomized trial of evolocumab. N Engl J Med. 2017;377:633-643.
- Shimada YJ, Cannon CP. PCSK9 (proprotein convertase subtilisin/kexin type 9) inhibitors: past, present, and the future. Eur Heart J. 2015;36(36):2415-2424.
- Bhatt DL, Steg PG, Miller M, et al. Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia. N Engl J Med. 2019;380:11-22.
- de Jongh S, Lilien MR, Bakker HD, Hutten BA, Kastelein JJ, Stroes ES. Family history of cardiovascular events and endothelial dysfunction in children with familial hypercholesterolemia. Atherosclerosis. 2002;163:193-197.
- Ose L. Diagnostic, clinical, and therapeutic aspects of familial hypercholesterolemia in children. Sem Vascular Med. 2004;4:51-7.
- McCrindle BW, Urbina EM, Dennison BA, et al. Drug therapy of high-risk lipid abnormalities in children and adolescents: a scientific statement from the American Heart Association Atherosclerosis, Hypertension, and Obesity in Youth Committee, Council of Cardiovascular Disease in the Young, with the Council on Cardiovascular Nursing. Circulation. 2007;115:1948-1967.
- American Academy of Pediatrics. National Cholesterol Education Program: report of the Expert Panel on Blood Cholesterol Levels in Children and Adolescents. Pediatrics. 1992;89:525-584.
- Cholesterol Treatment Trialists Collaboration. Efficacy and safety of statin therapy in older people: a meta-analysis of individual participant data from 28 randomised controlled trials. Lancet. 2019;393:407-415.
- Lowe RN, Vande Griend JP, Saseen JJ. Statins for the primary prevention of cardiovascular disease in the elderly. Consult Pharm. 2015;30:20-30.
- Karlson BW, Wiklund O, Palmer MK, Nicholls SJ, Lundman P, Barter PJ. Variability of low-density lipoprotein cholesterol response with different doses of atorvastatin, rosuvastatin, and simvastatin: results from VOYAGER. Eur Heart J Cardiovasc Pharmacother. 2016;2:212-217.
- Pedersen TR, Faergeman O, Kastelein JJ, et al. High-dose atorvastatin vs usual-dose simvastatin for secondary prevention after myocardial infarction: the IDEAL study: a randomized controlled trial. JAMA. 2005;294:2437-2445.
Back to Top