
Expired activity
Please go to the PowerPak
homepage and select a course.
Module 13: Analyzing Health Care Quality and Cost: An Overview of MTM Star Ratings
INTRODUCTION
Quality of Health Care
There is an urgent need to improve health care quality in the United States (U.S.). Starting in 1999, the Institute of Medicine (IOM) developed a series of reports that describe the urgent need to improve U.S. health care. These reports are the foundation for recent quality discussions in health care. The first report, entitled To Err is Human: Building a Safer Health System, discussed the economic and clinical consequences of medication errors and misuse and also suggested that many issues in U.S. health care have resulted from ineffective systems.1 The second report, entitled Crossing the Quality Chasm: A New Health System for the 21st Century, called for reinventing the health care system in America to improve the overall quality of care. This included the development of measures for assessing quality of care.2 The third report, entitled Health Professions Education: A Bridge to Quality, identified myriad gaps in U.S. health care education and suggested ways to close those gaps to improve the quality of such education. Several recommendations included training health care professionals to work in teams, use and apply evidence-based information, serve the needs of diverse populations, analyze the root cause of errors and quality issues, and utilize informatics in patient care.3
Quality issues in health care fall into the following three categories: underuse, overuse, and misuse.4 Underuse refers to failure to offer care that would provide favorable patient outcomes. One example of underuse would be failing to provide a controller medication for a person with asthma who has a moderate to severe case and has been overusing rescue medications. Overuse involves providing health care when the risks outweigh the possible benefits. Examples of overuse may include sedatives, hypnotics, and antidepressants, as well as the use of antipsychotics to treat older adult patients.5 Misuse refers to giving appropriate health care, but having avoidable complications occur because of issues similar to those encountered with polypharmacy.
Before continuing, it is important to define quality, both in general and with respect to health care. Merriam-Webster's Dictionary interprets quality as a "degree of excellence."6 While this definition provides a framework for quality in general, it is also helpful to examine the definitions of quality specific to health care. So, what is quality in health care? It can be said that quality in pharmacy practice "represents a degree of excellence, increases the probability of positive outcomes, decreases the probability of negative outcomes, corresponds with current medical knowledge, offers the patient what he or she wants, and provides the patient with what he or she needs."7
Now that we have defined quality and its relationship to health care, how can we measure quality? A commonly used method to measure health care quality is to use the Structure Process Outcome framework developed by Dr. Avedis Donabedian.8 Structure describes the presence of something that is reasonably associated with quality. That is, do the raw materials exist in the right place? For example, state pharmacy regulations may require that a community pharmacy employ a licensed pharmacist in addition to having sufficient counter space in the pharmacy for prescription processing, an ample number of medication references, and a private patient counseling center, to name a few. Process refers to the actions associated with quality. For example, following a standardized operation for prospective drug utilization review, as required by the Omnibus Budget Reconciliation Act of 1990 (OBRA '90), is a process and how often the procedure is followed could be thought of as a process measure.9 Outcomes are the end result attributable to health care products or services. Positive outcomes associated with quality health care include reduced mortality, improved quality of life (QoL), control of disease and pain, and satisfaction with care. Outcomes can be thought of in the framework of the ECHO model (economic, clinical, and humanistic outcomes).10 That is, outcomes for a patient with type 2 diabetes mellitus (T2D) can be clinical, such as the control of the disease as measured by blood glucose (BG) or glycosylated hemoglobin (A1C) in the short-term or by the prevention of end-stage renal failure in the long-term.
BG control in such a patient may have economic outcomes, such as the savings from decreasing the number of hospital stays the patient experiences, and humanistic outcomes, such as improved patient satisfaction or health-related QoL. Structure, process, and outcomes are indicators of quality and each is necessary to fully elucidate health care quality.
For example, having ready access to current clinical guidelines in a pharmacy is more likely to be associated with higher quality care than a pharmacy without such access (i.e., structure). However, it is not sufficient. The clinical guidelines must be accessed and used appropriately. Pharmacists who routinely review current clinical guidelines and who use this information in a proactive manner when assessing care and making recommendations are more likely to provide a higher level of care than those who do not (i.e., process). This, too, is not sufficient. What we are really after is the outcome or result of therapy (i.e., disease control, decreased health care costs, and improved health-related QoL). Optimally, outcomes are what we really should measure because they are the reason for having structures and processes.
In the recent past, U.S. health care costs were considered to be an important outcome. Lately, though, there is more talk of value entering the equation. So, what is value in terms of health care? That type of value is the ratio of quality over cost.11 Thus, to elevate value, one must either increase quality or lower cost or do both. Value-driven health care is a concept that is becoming increasingly important when discussing the quality of health care. "Value-driven health care" is defined as health care that is selected based on relative value to other alternatives, not just on quality. This means that quality can no longer be considered independent of cost because the two are linked. So, when we refer to value-driven health care, we are discussing what is paid for in terms of what is received, compared with alternatives.
Take-home point: Health care quality and value-driven health care are important for pharmacists or pharmacies because pharmacists are being asked by payers and regulators to measure the quality and value of their services. Payers are using quality as a determining factor for inclusion into their pharmacy networks. To be sure your pharmacy is included in the network, it is essential to assess your quality. The health plans are assessing pharmacies, so it is important that pharmacists be aware of this.
Centers for Medicare & Medicaid Services (CMS) Star Ratings
Quality advocates indicate there are four major ways to improve that factor: 1) regulation, 2) continuous quality improvement (CQI), 3) marketplace competition, and 4) payment incentives.4 Regulation can be used to mandate minimum standards by health care providers and insurers. Regulation alone, however, often fails to achieve the intended results. For example, the OBRA'90 legislation did not achieve the desired impact of improving rational and safe medication use.
CQI is a management philosophy indicating system improvement can be achieved by : 1) monitoring quality, 2) simplifying and improving the system, 3) eliminating waste and duplication, and 4) preventing errors. Although underutilized in health care, CQI offers tremendous promise.
Marketplace competition is advocated because providing credible information about health care quality and value to patients and payers is believed to encourage provider (e.g., pharmacists, hospitals, and physicians) competition and, in turn, lead to higher health care quality and value. An example of marketplace competition by publicly presenting quality metrics in health care is the Hospital Compare Web site (https://www.medicare.gov/hospitalcompare/search.html), with which consumers can directly compare the quality of hospitals in their geographic area. Publicly reported quality metrics are not yet used in pharmacies, but it seems possible in the near future.
Payment incentives (to health plans, hospitals, or physicians) are advocated to encourage greater efforts to improve quality. Payment incentives, which are often called pay-for-performance (P4P), are evident in pharmacy practice and this will be discussed in more detail later. The current health care payment structure does not make performance-based payment easy; however, all of these methods are being tested in various ways throughout the health care system. Some are being encouraged through health reform legislation at the Federal and local levels, while others are being initiated by providers and insurers.
The Patient Protection and Affordable Care Act (ACA) was signed into law in 2010.12 The goal of the ACA is to expand and change insurance coverage while improving health care accessibility, affordability, efficiency, quality, and value. Several elements of the ACA that are likely to influence the quality of pharmacy services will be touched on briefly below. Accountable Care Organizations (ACOs) are networks of health care providers who are incentivized to work together to provide coordinated, comprehensive patient care across settings. Payments to ACOs are tied to health outcomes (i.e., value-driven health care) rather than to the number of services provided (i.e., fee for service). Therefore, ACOs emphasize quality of care over quantity of care. Pharmacists in ACOs are encouraged to work with inter-professional teams to provide medication therapy management (MTM), medication adherence counseling, and other services. The Center for Medicare and Medicaid Innovation (CMMI) is a part of the CMS established by the ACA to test new ways of delivering and paying for health care. Innovations of interest to pharmacists include MTM services, transition of care programs, hospital readmission reduction programs, and cost-reduction strategies. Health Insurance Exchanges are marketplaces for buying health insurance offered by private companies, where individuals, families, and small businesses can choose a plan based on costs, benefits, and other features.
CMS Star Ratings are a quality rating system encouraged by the ACA. CMS Star Ratings, were formed in 2006 as part of the Medicare Part D legislation.13 The CMS Star Ratings is a 5-Star rating system designed to grade health plans that sponsor a Medicare Part C or D benefit. In this grading system 1 Star is the lowest quality and 5 Stars is the highest quality. The Star Rating system is designed to provide consumers with data about the quality of Parts C and D in any given plan and it can be useful when choosing from among the plans currently available. These annual ratings, which are made available on Medicare Plan Finder (www.medicare.gov/find-a-plan/questions/home.aspx), are similar to other rating systems you may find on the Internet (e.g., www.amazon.com). Star Ratings provide a way to measure, monitor and compare the quality performance of Medicare plans. Medicare Advantage Prescription Drug Contracting (MAPD) plans are rated on performance measures for Medicare Parts C and D. A subset of the Healthcare Effectiveness Data and Information Set (HEDIS), a measure set from the National Committee for Quality Assurance (NCQA), is used for Part C evaluation. Medicare Part D Stars are applicable to MAPDs and stand-alone Prescription Drug Plans (PDPs). The Stars are assigned based on performance measures across four domains. The four Part D domains are:
1) Drug Plan Customer Service;
2) Member Complaints and Changes in the Drug Plan's Performance;
3) Member Experience with Drug Plan;
4) Drug Safety and Accuracy of Drug Pricing.14
There are 14 individual measures of quality in the 2019 Part D ratings. Medication safety and adherence measures are in the domain of Drug Safety and Accuracy of Drug Pricing. The quality of drug plans and pharmacy benefits are an important element of the Star Ratings and pharmacies that exceed quality benchmarks can receive bonuses (i.e., P4P as previously described). MAPD plans with higher Star ratings qualify for bonus payments. Bonuses of 5% are awarded to 4, 4.5, and 5-Star-rated Medicare Advantage Plans which leads to a significant revenue boost. For example, if an additional 5% equates to $36 per member per month, a 4-star plan with 100,000 members would receive an additional $72 million increase in revenue. In 2018, there was an estimated $6.3 billion in quality bonus payments to MAPD plans alone. There is a 2 year lag between measurement and payment, so 2019 payments are based on 2017 Star ratings performance.15,16 Medicare Advantage and Prescription Drug Plans that earn a 5-Star rating benefit from year-round plan enrollment and are recognized by a high-performing icon in the Medicare Plan Finder. Plans with a rating of 2.5 or fewer stars for 3 consecutive years are labeled with a low-performer icon.16 Star rating has been associated with beneficiaries' enrollment decisions, both among first-time enrollees and those switching plans.17 A 2018 analysis showed the additional impact of MAPD star ratings improvements on plan enrollment and revenue. According to the analysis of 500 MAPD contracts:
- For plans with 3 or less stars, a 1-star rating improvement could, on average, lead to a year-over-year 8 percent to 12 percent increase in plan enrollment.
- Improving from a 3-star to 4-star rating could increase revenue between 13.4 percent and 17.6 percent.18
The medication-use (adherence) Star Ratings measures were all triple-weighted in recent years. In 2016, a new medication therapy management (MTM) process measure (Completion Rate for Comprehensive Medication Reviews (CMRs), with a weighting of 1, was added to the Star Ratings set.14 An additional measure in 2019 with a weighting of 1 is the Statin Use in Persons with Diabetes (SUPD) measure.14 Nearly 40% of a Part D plan's Star Rating in 2020 will be based on performance on the 3 medication-use metrics and the CMR completion rate and SUPD.19 Because medication-related measures make up such a large proportion of a health plan's Star Rating, pharmacies will continue to play a very important role in quality measure performance improvement for Part C and D plans. Health plans will continue to watch pharmacies to see which systems are helping to achieve better Star Measures and which ones are bringing down their ratings.
Take-home point: It is important for pharmacists or pharmacies to know about the CMS Star measures because the quality bonus payments may become increasingly important to continued profitability for those plans and perhaps for pharmacies.
Organizations That Create Pharmacy Quality Measures
To improve the health care system, measuring health care quality and safety is of the utmost importance. When measurements are taken, people will often recognize problematic areas and work to improve systems with a new or improved method or process. For example, if a professor tells her students that she is going to test them on how to apply the most recent guidelines for diabetes mellitus (DM) pharmacotherapy, they will usually make an effort to know what to do. The same response can be seen with health care. If we tell physicians that we will assess and publicly report their DM pharmacotherapy guideline adherence, they will likely implement processes and systems to help ensure that patients with DM are treated appropriately. So, as we focus on quality improvement in the health care system, performance must be assessed. Measurements provide information about whether a problem exists or not. We know that such data drive improvement, accountability, research, and payment. Pharmacies are trying to reduce medication errors, improve care, and receive reimbursement for patient care services, so, it is quite important that we measure pharmacy quality.
In recent years, the dimensions of pharmacy and pharmacist performance have changed. In the past, most measures of pharmacy performance focused on providing a drug to the patient. The drawback to such measures is that good performance based on this data may not always result in positive health outcomes. For instance, dispensing a large number of prescriptions in a short period of time can lead to negative health outcomes if the medications prescribed are wrong for the patient's condition or if patients do not know how to appropriately take the medications. Thus, these pharmacy performance measures tended to underemphasize important elements of professional service, such as communication and MTM. Some traditional pharmacy performance measures include the number of prescriptions dispensed, a desirable location, customer satisfaction that revolves around convenience, competitive prices, labor costs per prescription, the ratio of new prescriptions to refills, and prescription sales. New measures are being developed that better represent the changing practice of pharmacy. Some of the new performance measures encompass adherence rates with chronic medications; medication error rates; numbers of patients achieving therapeutic goals; levels of patients receiving immunizations; disease-, population-, and medication-specific standards; and patient satisfaction with counseling about new prescriptions, verbal and written information about medicines, and other elements of pharmacy-related care. These new performance measures seek to assess elements of care more closely related to positive health outcomes.
Governmental and nongovernmental organizations are trying to create measures that assess the multidimensional nature of medication therapy and pharmacist care. One organization that develops quality measures for medication use is the Pharmacy Quality Alliance (PQA) (www.pqaalliance.org). The PQA was established in 2006 because the founders recognized that, while there were myriad quality-performance measures for hospitals, health plans, nursing homes, and physicians (as well as others), good pharmacy quality data to assess the multidimensional nature of medication therapy and pharmacist care were not readily available. The founders encouraged those in the industry to band together and, through a transparent, consensus-based process, determine how medication use should be measured. PQA is a nonprofit organization with more than 250 member organizations that span healthcare quality, including healthcare payers, health plans, community pharmacies, physician providers, life sciences organizations, state and federal government agencies, academic institutions, standard setting/accreditation organizations, health information technology (HIT) partners, and other stakeholders interested in improving medication-use quality.20
As a recognized leader in quality measure development, PQA is dedicated to its mission to optimizing health by advancing the quality of medication use.2 The PQA team convenes multiple stakeholders to collaboratively promote appropriate medication use, develop strategies for measuring and reporting performance, research quality measurement impact, and provide education on quality-based healthcare. Visit the PQA website (https://www.pqaalliance.org/) and explore the different activities that the PQA is currently pursuing, as well as the process of measurement creation.
Take-home point: Pharmacists and pharmacies must know about and be able to name an organization that creates medication use quality measures (e.g., The Pharmacy Quality Alliance or the PQA). This is important because the PQA is dedicated to improving the safe and appropriate use of medications by collaboratively defining how the multidimensional nature of medication therapy should be measured.
Quality Measures in the Pharmacy
PQA has been developing quality standards for medication use that mainly focus on measures in the areas of adherence, safety, and appropriateness. Table 1 includes an overview of the PQA Performance Measures developed over the years by various PQA measure development teams (MDTs). These have been grouped into five domains: Adherence, Appropriate Medication Use, Medication Safety, Medication Therapy Management, and Quality Improvement Indicators. PQA also has two core measure sets focused on opioid prescribing and specialty medications.22 The metrics were developed through broad stakeholder participation from across PQA's diverse membership and have been field tested by a number of PQA member organizations (e.g., Optum, Inc., Inovalon, CMS, Merck & Co., Inc.). Specific details about how they were developed can be found on the PQA website. PQA measures currently used in the 2019 CMS Star Ratings have been bolded and italicized.19,22,23
It its CY 2020 Final Call Letter, the mechanism by which changes to the Medicare Part D program are annually announced, no new Star Rating measures are being proposed for addition in 2020.19 CMS did indicate some new Display Page measures. Display measures are not included in plan ratings and are used to monitor plan performance for quality improvement. New for 2020 are:
- Transitions of Care (Part C) – NCQA Steward
- Follow-up after Emergency Department Visit for Patients with Multiple Chronic Conditions – NCQA Steward
CMS also indicated some forthcoming changes to the medication-related Star Ratings for 2021. New measures that will be lining up for the 2021 Display Page with intent to become Star Ratings measures include:
- Concurrent Use of Opioids and Benzodiazepines (COB; (NQF 3389));
- Polypharmacy: Use of Multiple Anticholinergic Medications in Older Adults (POLY-ACH); and,
- Polypharmacy: Use of Multiple CNS-Active Medications in Older Adults (POLY-CNS).19
CMS also indicated it will likely retire the High Risk Medication Use in the Elderly Measure from the Display Page in 2021.19
Taking a closer look at the adherence to diabetes medications measure, we see that Proportion of Days Covered (PDC) is the PQA-endorsed method for estimating medication adherence for those using chronic medications. PQA PDC metrics are also endorsed by the National Quality Forum (NQF). The diabetes medication PDC metric identifies the percentage of patients taking medications in a particular drug class who have high adherence (i.e., PDC of more than 80% for the individual). Let's examine how the diabetes all-class measure is calculated below. (See Table 2 and Figure 1 for additional information.) When health plans evaluate pharmacies, they assess quality at the pharmacy level—not the pharmacist level—and Part D health plans are measured at the plan level (i.e., depending on who is being measured and who is doing the measuring).
A higher rate of patients meeting the PDC metric threshold may indicate a higher quality of care. Pharmacies with higher rates are judged as providing better care. Measuring pharmacy quality can be employed for a variety of purposes, including the development and design of quality improvement programs for the pharmacy. Payers and other entities may use them to develop report cards to be utilized by consumers who are actively choosing pharmacy providers. The measures can be used by pharmacy benefit managers (PBMs) and others to determine which pharmacies may be in a network or to establish compensation in P4P programs. These criteria can assist with benchmarking pharmacies and pharmacists and with identifying quality deficiencies, as well as to assess the impact of interventions. Finally, these standards may help outcomes researchers examine quality trends and conduct comparative effectiveness research.
| Table 1. Pharmacy Quality Alliance (PQA) Performance Measures22 |
| Adherence |
Proportion of Days Covered (PDC) Metrics: The percentage of patients who met the PDC threshold of 80%* during the measurement period for each of the following:
- Diabetes All Class (PDC-DR) (NQF #0541)
- Renin Angiotensin System Antagonists (PDC-RASA) (NQF #0541)
- Statins (PDC-STA) (NQF #0541)
- Beta-blockers (PDC-BB)
- Calcium Channel Blockers (PDC-CCB)
- Biguanides (PDC-BG)
- Dipeptidyl Peptidase (DPP)-4 Inhibitors (PDC-DPP)
- Sulfonylureas (PDC-SFU)
- Thiazolidinediones (PDC-TZD)
- Non-Warfarin Oral Anticoagulants (PDC-NOAC)
- Long-Acting Inhaled Bronchodilator Agents in COPD (PDC-COPD)
- Antiretrovirals (this measure has a threshold of 90% for ≥3 medications)* (PDC-ARV-2019)
- Non-infused Disease Modifying Agents used to Treat Rheumatoid Arthritis (PDC-RA)
- Non-infused Disease Modifying Agents used to Treat Multiple Sclerosis (MS) (PDC-MS)
Adherence and Persistence Metrics that do not utilize PDC:
- Treatment of Chronic Hepatitis C: Completion of Therapy (HCV)
- Primary Medication Nonadherence (PMN)
|
Appropriate Medication
Use |
- Diabetes Medication Dosing (DOS)
- Statin Use in Persons with Diabetes (SUPD; NQF #2712)
- Medication Therapy for Persons with Asthma (MTPA)
|
| Medication Safety |
Medication Safety in Older Adults:
- Use of High-Risk Medications in the Elderly (2017 Update) (HRM-2017)
- Use of Benzodiazepine Sedative Hypnotic Medications in the Elderly (BSH)
- Polypharmacy: Use of Multiple Anticholinergic Medications in Older Adults (POLY-ACH)
- Polypharmacy: Use of Multiple CNS-Active Medications in Older Adults (POLY-CNS)
Medication Safety for Opioid Use:
- Concurrent Use of Opioids and Benzodiazepines (COB; (NQF 3389))
- Use of Opioids at High Dosage in Persons Without Cancer (OHD; NQF #2940)
- Use of Opioids from Multiple Providers in Persons Without Cancer (OMP; NQF #2950)
- Use of Opioids at High Dosage and from Multiple Providers in Persons Without Cancer (OHDMP; NQF#2951)
Additional Medication Safety Measures:
- Drug-drug Interactions (DDI-2017)
- Antipsychotic Use in Persons with Dementia (APD; NQF #2111)
- Antipsychotic Use in Persons with Dementia: MDS (APD-MDS)
- Antipsychotic Use in Children under 5 Years (APC; NQF #2337)
|
Medication Therapy
Management |
- Completion Rate for Comprehensive Medication Review (CMR)
|
Quality Improvement
Indicators |
These metrics are used by organizations solely for internal quality improvement:
- Provision of Medication Therapy Management Services Post Hospital Discharge
- Readmission of Patients Provided Medication Therapy Management Services Post Hospital Discharge
- Medication Synchronization: Program Acceptance and Initial Synchronization
- Medication Synchronization: Patient Contact Rate
- Medication Synchronization: Completeness
- Medication Synchronization Continuation: 2 Rates
|
| Table 2. Proportion of Days Covered (PDC)—Diabetes (All class) |
| Measure Title |
Measure Description/Definition |
| PDC—Diabetes (All class) |
The percentage of patients 18 years of age and older who met the
PDC threshold of 80% during the measurement year for the therapeutic medication class |
Is Your Pharmacy Contributing to the Part D Star Ratings?
Value-based health care is important and positioned to become even more so. Medication-use quality metrics are being used to rate Medicare Part D health plans, with these metrics weighted heavily when calculating Star Ratings. Pharmacies have become quite important to health plans because of the heavy weighting on medication-use measures, so much so that pharmacies have become very influential in whether a Part D plan receives the coveted 5-Star rating. Health plans pay increasingly close attention to pharmacy performance on medication use metrics.
One way for pharmacists and pharmacies to keep pace is to utilize the Electronic Quality Improvement Platform for Plans & Pharmacies (EQuIPP) created by Pharmacy Quality Solutions (PQS). The EQuIPP platform helps you determine how your pharmacy is performing on these and other metrics. (http://www.pharmacyquality.com) EQuIPP, to which most community pharmacies have access at the managerial level, if not the store level, is the first national pharmacy quality measurement, benchmarking, and reporting platform.23 It connects plans and pharmacies to quality metric performance data in a more real-time fashion (i.e., updated approximately monthly) allowing both to more rapidly respond to changes in performance versus the 2−year lag in the Star Ratings program. Because this platform provides benchmark data, pharmacies can compare their performance with that of others in their chain and state, making this information easily understandable. By doing so, EQuIPP facilitates an environment in which prescription drug plans and community pharmacies can engage in strategic relationships to address improvements in the quality of medication use.23
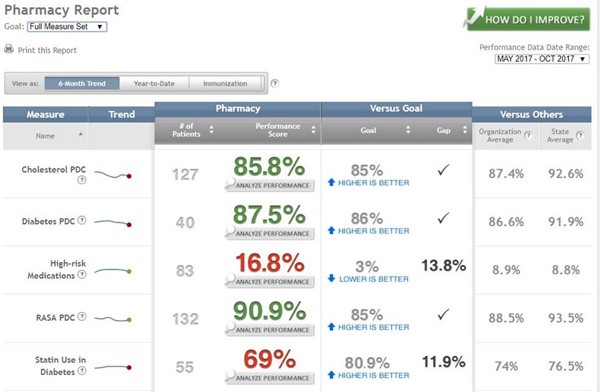
Figure 2 provides a screen shot of the EQuIPP pharmacy report view. As you can see, EQuIPP lists the PQA medication-use measures that are in the Star Ratings program (along with additional metrics) in the far-left column (labeled "Measure"). More quality measures can be added to align with CMS, NCQA, URAC (formerly the Utilization Review Accreditation Commission), or other initiatives. A user can click on the question mark beside each measure for more detailed information concerning the numerator and the denominator. The next column, marked "Trend," offers a trend line on that measure. Further to the right, labeled "# of Patients", this column tells the user how many of their patients are included in each measure calculation. The next column to the right, entitled "Performance Score" provides the pharmacy's score on each measure. Note that some rates are green indicating that the pharmacy is at or exceeds the goal on this measure, while others are red, which show s that the score is not at goal. There is also a hot link below the rate that helps the user analyze the pharmacy’s' scores. The next column, labeled "Goal," indicates the goal for each measure. This can be modified to reflect the program for which the goal is stated (e.g., Star Ratings) or to reflect internal pharmacy organization goals. Reminders are provided to allow the user to easily understand whether a higher or lower score on each measure is "better". For example, on a Diabetes PDC measure, a better score is higher, which indicates better adherence to therapy. However, on a measure such as "High-Risk Medications," a lower score reveals that fewer patients from the pharmacy are taking potentially harmful medications, thus indicating better quality. The next column, entitled "Gap", lets the user know at a glance if the pharmacy is at goal or not. If not, the data show how much of a gap there is before goal is reached. For example, in Figure 2, the "Statin Use in Diabetes" goal is 80.9% or higher, but the pharmacy's score is 69%, indicating that there is a significant divide (11.9%), with much work necessary to get the pharmacy to goal on this measure. The final two columns on the right, labeled "Versus Others," provide the user with an understanding of how the pharmacy is performing compared with the "Organizational Average" and the "State Average." Above these columns, there is a green icon with an arrow and the words "How do I improve?" This link, when clicked on, takes the user to instruction and information about how to better the pharmacy's quality measure performance.23 Because EQuIPP is a neutral intermediary that favors collaboration of health plans, PBMs, and pharmacies in CQI activities related to medication use, EQuIPP supports multitier views of pharmacy organization performance – from the individual pharmacy, through districts/regions, to the corporate roll-up. Because EQuIPP data are updated on a near monthly basis, there is a consistent, standardized assessment of community pharmacy performance on Medicare Part D Star Ratings and other quality measures, as well as faster, more-refined benchmarking performance in key market areas. This, then, provides the foundation for performance-based contracts and payment systems for pharmacy networks.
Figure 2. Electronic Quality Improvement Platform for Plans & Pharmacies (EQuIPP) Pharmacy Report View
 |
PQA-supported demonstrations in Pennsylvania showed that Rite Aid pharmacies were capable of achieving substantial improvement in PDC rates over 1 year while remaining efficient; so the Highmark Medicare plan's PDC measures increased by 1 star during the demonstration period. In addition, there are economies of scale: for example, thousands of pharmacists in a plan's network frequently meet with Medicare patients which means there are many pharmacist touch points to achieve a positive impact. Most Medicare Part D plans could move from 3 Stars to 4 Stars on each PDC measure if every pharmacy in the network helped just one more patient on an angiotensin-converting enzyme inhibitor/angiotensin receptor blocker, one more person with DM, and one more individual on a statin become highly adherent.24
Take-home point: It is important for pharmacists or pharmacies to determine how the pharmacy is contributing to the Medicare Part D Star Ratings using the EQuIPP dashboard to ensure optimal performance in network status and to improve patient care.
Medication Therapy Management (MTM) and Comprehensive Medication Review (CMR)
Before discussing how pharmacists can use the information in this article to improve pharmacy quality and to assist patients, a review of definitions is in order. According to CMS, a Medicare Part D sponsor must incorporate a Medication Therapy Management Program (MTMP) into its plan benefit structure. The MTMP should: 1) ensure optimum therapeutic outcomes for targeted beneficiaries through improved medication use; 2) reduce the risk of adverse events; 3) be developed collaboratively with licensed and practicing pharmacists and physicians; 4) describe the resources and time needed to implement the MTMP; and 5) include a description of any care coordination management plans established for targeted individuals.25 MTM services can be independent of or may occur in conjunction with medication dispensing. Specific services included in MTM can be comprehensive or targeted to an individual medication problem or disease state. Table 3 lists specific MTM services.26 Note: these reviews can be comprehensive or focused based on individual patient needs and can specifically involve any of the following activities: overall pharmacotherapy consults, disease management coaching/support, pharmacogenomics applications, anticoagulation management, medication safety surveillance, immunization, and other clinical services.26
Note that recent consensus on the definition and title of MTM has been a hot topic lately. The Joint Commission of Pharmacy Practitioners recently redefined the practices as Medication Management Services (MMS) which encompass "a spectrum of patient-centered, pharmacist-provided, collaborative services that focus on medication appropriateness, effectiveness, safety, and adherence with the goal of improving health outcomes". This definition has been developed through a pharmacy-based multi-stakeholder consensus.27 A CMR specifically has not been defined by this group; however, CMS defines it as an MTM encounter designed to: 1) improve patients' knowledge of their medications and supplements; 2) identify and address their issues or concerns; and 3) empower people's self-management of medications and health conditions.28
| Table 3. Specific services Included in Medication Therapy Management (MTM)26 |
According to the individual needs of the patient, MTM services include, but are not limited to, the following:
- Collecting patient-specific information
- Assessing medication therapies to identify medication-related problems
- Developing a prioritized list of medication-related problems
- Creating a plan to address identified medication-related problems
|
Take-home point: Pharmacists should understand the definitions and intent of MTM and CMRs so they can develop programs that meet the intent of these services. This is important because one of the medication-use Star Ratings metrics addresses CMR completion rate.
Part D plans are required to offer an MTM program in their benefit structure, with a CMR specifically listed as part of the MTM process in the consensus statement. Also, the CMR completion rate is among the five medication-related Part D Star Ratings measures. Other CMS Star Ratings measures work synergistically with MTM services. The intent of MTM is to ensure quality medication outcomes for patients and to decrease medication issues. This directly mirrors the other medication-related PDC Star Rating measures, which specifically assess the PDC of diabetes medications, statins, and Renin Angiotensin System (RAS) Antagonists, and use of statins in patients with diabetes. These medication-use measures were created by a PQA transparent, consensus-based, multi-stakeholder process (i.e., developed by the broader healthcare quality profession including community pharmacy) and adopted by CMS in their Star Ratings set, because medication use is key to patient health and safety and to the quality of health care. In addition, the heavy weighting of the adherence metrics (PDC) in the Part D Star Ratings measures further link to pharmacists' role in health care quality in an unprecedented manner. The EQuIPP platform presents an opportunity for pharmacists to assess and improve their contributions to Part D medication-use quality measurement and provides a business opportunity as well. Pharmacists can help patients improve medication adherence by interacting with those who have not been optimally adherent to such therapy by developing interventions that address patient-reported reason(s) for nonadherence (reason to which community pharmacists are intimately exposed).
If the patient is having difficulty affording his or her medication, the pharmacist can facilitate a switch to a lower-cost generic or a combination medication. This may work well for the person who is taking two medications for which there is a reasonably priced combination product. If an individual is experiencing an adverse event, the pharmacist can help by recommending a move to an alternate choice that would achieve the same therapeutic objective with a lower incidence of the bothersome side effect. If a patient is having trouble remembering to take his or her medications, the pharmacist can suggest compliance aids or memory devices. If the patient has trouble getting to the pharmacy several times a month, the pharmacy can offer medication synchronization and the appointment-based model; in this way, patients may only have to visit the pharmacy once a month or home delivery can be initiated. If a patient is more adherent to his/her chronic medication, positive outcomes, such as better disease control, decreased end-stage complications, and lower heath care utilization and costs, should result. In fact, the Congressional Budget Office once estimated that a 1% increase in the number of prescriptions filled by beneficiaries would cause Medicare's spending on medical services to decrease by about one-fifth of 1%—that is approximately a $1.7 billion savings.29
In addition, helping improve medication adherence presents a business opportunity for pharmacies. Improving PDC (adherence) means patients will fill their medications more often, which will result in additional revenue for the pharmacy30 and better Star Ratings for the health plan. When Part D health plans increase their Star Ratings, they effectively increase their revenue. Pharmacies are influential because of the heavily weighted medication-use measures for Medicare Part D plans; so, pharmacies would be justified in asking to receive contracts that financially reward them for helping increase plan Star Rating performance (which can be tracked on a more real-time basis via EQuIPP). A few health plans have already implemented P4P for pharmacies. As an example, Inland Empire Health Plan (IEHP) launched a P4P plan for pharmacies in October 2013. Pharmacies were evaluated on Star Ratings measures plus the PQA asthma measure and generic dispensing rate. They received bonus payments every 6 months, depending on their performance on each of the following measures: 3-Star attainment = small bonus; 5-Star attainment = large bonus. The bonus is based on the number of patients at each pharmacy and the score on each measure. IEHP also publicly recognizes top performers.31 Other insurers have also instituted P4P programs or pilots, including Healthfirst of NY, Caremark-SilverScript and Humana.32
Take-home point: Pharmacists or pharmacies should offer MTM services and improve their quality measure performance because both situations present opportunities for pharmacists/pharmacies to ameliorate the quality of patient care, store revenue, and health plan Star Ratings. This provides pharmacies with an opportunity to negotiate pay-for-performance (P4P) or other incentive-based programs.
REFERENCES
- Kohn LT, Corrigan JM, Donaldson MS, eds. To Err Is Human: Building a Safer Health System. Washington, DC National Academies Pr; 2000.
- Committee on Quality of Health Care in America, Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academies Pr, 2001.
- Institute of Medicine, Greiner AC, Knebel E, eds. Health Professions Education: A Bridge to Quality. Washington, DC: National Academies Pr, 2003.
- Chassin MR. Galvin RW; and the National Roundtable on Health Care Quality. The urgent need to improve health care quality. JAMA. 1998; 280(11):1000-1005.
- The 2019 American Geriatrics Society Beers Criteria® Update Expert Panel. American Geriatrics Society 2019 Updated AGS Beers Criteria® for Potentially Inappropriate Medication Use in Older Adults. J Am Geriatr Soc. 2019;67(4):674-694.
- Simple definition of quality. http://www.merriam-webster.com/dictionary/quality. Accessed April 20, 2019.
- Warholak TL. Ensuring quality in pharmacy operations. In: Pharmacy Management. Desselle S, Zgarrick D, eds. 3rd ed. McGraw Hill Companies, Inc. 2011:97-121.
- Donabedian A. Evaluating the quality of medical care. Milbank Mem Fund Q. 1966;44(3): Suppl:166-206.
- S. Congress. H.R. 5385, Omnibus Budget Reconciliation Act of 1990. https://www.congress.gov/bill/101st-congress/house-bill/5835 Accessed April 20, 2019.
- Kozma CM, Reeder CE, Schulz RM. Economic, clinical, and humanistic outcomes: a planning model for pharmacoeconomic research. Clin Ther. 1993;15(6):1121-1132; discussion 1120.
- S. Department of Health and Human Services, Value-Driven Health Care Initiative. Washington, DC, U.S. Department of Health and Human Services; https://wayback.archive-it.org/3909/20131218183643/http://archive.hhs.gov/valuedriven/news/20070228.html. Accessed April 20, 2019.
- Patient Protection and Affordable Care Act (ACA). Read the Affordable Care Act. https://www.healthcare.gov/where-can-i-read-the-affordable-care-act/ Accessed April 20, 2019.
- Medicare Part D legislation. Available at gpo.gov/fdsys/pkg/PLAW-108publ173/pdf/PLAW-108publ173.pdf.Accessed April 20, 2019.
- PQA Measure Use in CMS’ Part D Quality Programs. Medicare Part D Star Ratings. https://www.pqaalliance.org/medicare-part-d Accessed April 19, 2019.
- Jacobson G, Damico A, Neuman T. A dozen facts about Medicare Advantage. November 13, 2018. Kaiser Family Foundation Website. https://www.kff.org/medicare/issue-brief/a-dozen-facts-about-medicare-advantage/. Accessed April 22, 2019.
- Advance Notice of Methodological Changes for Calendar Year (CY) 2019 for Medicare Advantage (MA) Capitation Rates, Part C and Part D Payment Policies and 2019 Call Letter. Centers for Medicare and Medicaid Services. https://www.cms.gov/MEDICARE/HEALTH-PLANS/MEDICAREADVTGSPECRATESTATS/DOWNLOADS/ANNOUNCEMENT2019.PDFAccessed April 22, 2019.
- Reid RO, Deb P, Howell BL, Shrank WH. Association between Medicare Advantage plan Star Ratings and Enrollment. JAMA. 2013;309(3):267-274.
- Bajner R, Meinkow E, Munroe J, et.al. Impact of star ratings on Medicare advantage plan success. March 15, 2018. https://www.beckershospitalreview.com/finance/impact-of-star-ratings-on-medicare-advantage-plan-success.html. Accessed April 22, 2019.
- PQS Summary of Pharmacy/Medication-Related Updates in the CY 2020 Final Call Letter. Pharmacy Quality Solutions Website. April 2019. https://www.pharmacyquality.com/wp-content/uploads/2019/04/PQSCY2020FINALcallletter.pdf. Accessed April 20, 2019.
- Pharmacy Quality Alliance Member Organizations. PQA Website. https://www.pqaalliance.org/index.php?option=com_mcsearchresults&view=search&uuid=8aa051ba-fecf-4bb7-b6ba-f53e78f5dea9#/. Accessed April 22, 2019.
- The Pharmacy Quality Alliance (PQA) Story. PQA Website. https://www.pqaalliance.org/our-story. Accessed April 22, 2019.
- Put PQA Measures To Work. PQA Website. https://www.pqaalliance.org/pqa-measures. Accessed April 22, 2019.
- Electronic Quality Improvement Platform for Plans and Pharmacies. EQuIPP Website. https://www.equipp.org/. Accessed April 22, 2019.
- Arya V, Nau D. EQuIPP and Pharmacy Quality Reporting. In: Educating Pharmacists in Quality. Module 3: Session 13. 2014.
- Medication Therapy Management (MTM). Prescription Drug Coverage Contracting. Centers for Medicare and Medicaid Services. cms.gov/medicare/prescription-drug-coverage/prescriptiondrugcovcontra/mtm.html.Accessed April 22, 2019.
- Medication Therapy Management. American Pharmacists Association. http://www.pharmacist.com/medication-therapy-management-services.Accessed April 22, 2019.
- Joint Commission of Pharmacy Practitioners. Medication management services (MMS) definition and key points. March 14, 2018. Available at: https://jcpp.net/wp-content/uploads/2018/05/Medication-Management- Services-Definition-and-Key-Points-Version-1.pdf. Accessed April 22, 2019.
- CY 2019 Medication Therapy Management Program Guidance and Submission Instructions. Centers for Medicare and Medicaid Services. https://www.cms.gov/Medicare/Prescription-Drug-Coverage/PrescriptionDrugCovContra/Downloads/Memo-Contract-Year-2019-Medication-Therapy-Management-MTM-Program-Submission-v-040618.pdf. Accessed April 22, 2019.
- Congressional Budget Office. Report Offsetting Effects of Prescription Drug Use on Medicare's Spending for Medical Services. November 29, 2012.https://www.cbo.gov/sites/default/files/cbofiles/attachments/43741-MedicalOffsets-11-29-12.pdf. Accessed April 22, 2019.
- Holdford D, Inocencio T. Appointment-Based Model (ABM) Data Analysis Report. Prepared for Thrifty White Pharmacy. Virginia Commonwealth University School of Pharmacy. https://www.ncpanet.org/pdf/adherence/thriftywhitemedadherencestudy.pdf. Accessed April 22, 2019.
- Inland Empire Health Plan (IEHP) Pay for Performance Program. https://ww3.iehp.org/en/providers/pharmaceutical-services/pharmacy-p4p-program. Accessed April 22,2019.
- Pay for Performance & the Changing Landscape for Pharmacy: A Panel Discussion. PQA Website. https://www.performrx.com/sites/default/files/Panel-Pay%20for%20Performance%20and%20the%20Changing%20Landscape%20for%20Pharmacy.pdf. Accessed April 22, 2019.
Back to Top