
Expired activity
Please go to the PowerPak
homepage and select a course.
Addressing Rising Anemia Rates in Women: What Can Pharmacists Do to Improve Detection and Management?
Abstract
Iron deficiency and anemia are extremely common and serious health problems that affect women disproportionately compared with men.1 At-risk populations include women who are menstruating, pregnant, or postpartum, in addition to those with certain chronic diseases.2-4 Awareness about the impact of iron deficiency and anemia in the female population is low among the general public but also among healthcare providers.5 Many cases of iron deficiency and anemia remain unrecognized, untreated, or ineffectively treated, often with serious consequences.6
There is a need for greater understanding regarding the high prevalence of iron deficiency among women and awareness of current guidelines for evaluation, monitoring, and management. Pharmacists have the potential to expand awareness, improve anemia management, and implement effective patient education.7 This article will provide pharmacists with decision-making tools for management of iron deficiency and anemia in affected and at-risk female populations.
Anemia Incidence and Prevalence Among Women in the U.S.
The World Health Organization (WHO) describes iron deficiency as “the only nutritional deficiency significantly prevalent in virtually all industrialized nations."8 According to the U.S. Department of Health and Human Services (HHS), more than 6 million women who are menstruating are either iron deficient or anemic.9 Data from the 2016 National Health and Nutrition Examination Survey (NHANES) highlight the disproportionate prevalence of anemia in females. Over a 10-year period (2003 to 2012), about 5.6% of the U.S. population (including children and adults) were anemic, and 1.5% had moderate to severe anemia.10 In certain age brackets, the prevalence is significantly higher among women versus men, as shown in Figure 1.10 The gender discrepancy is most pronounced in younger age groups (9 times higher in females ages 15 to 29 and 7 times higher for women in their 30s) and continues until the 6th and 7th decades, when rates among men climb significantly due to chronic health conditions.10
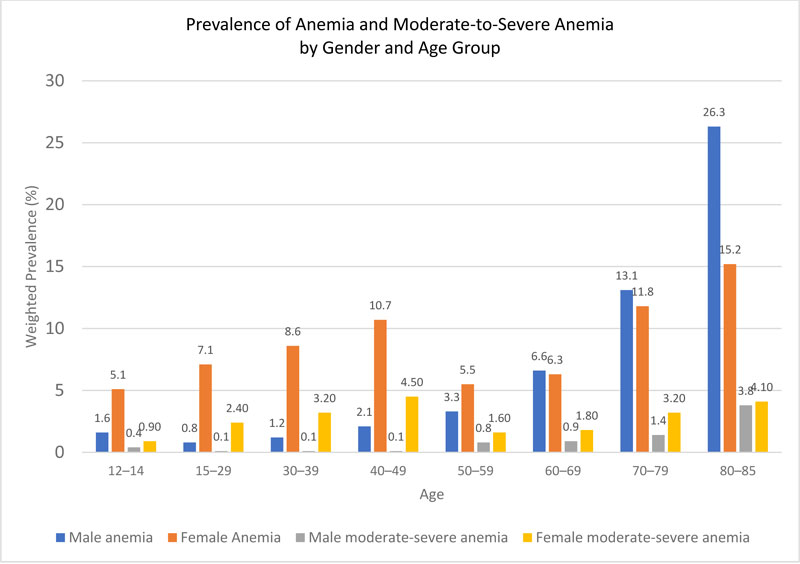 |
Figure 1. Prevalence of Anemia and Moderate-to-Severe Anemia, by Gender and Age Group10
Data from 5 NHANES surveys from 2003 to 2012 yielded a sample of 41,026 individuals between ages 0.5 and 85 years at a roughly equal balance of males and females. (Chart shows data for ages 12 and above.) Outcomes assessed were anemia and moderate-to-severe anemia. Women known to be pregnant (n=776) were excluded from the general analysis and these data examined separately. [Source: Le CHH. PLoS One. 2016;11(11):e0166635. Open Access] |
Race and ethnicity are factors that influence anemia prevalence (Figure 2): 15% of black women have anemia regardless of their age, and this rate climbs to an alarming 35.6% for black women who reach their early 80s.10 Similar patterns are seen among those with moderate-to-severe anemia (Figure 3).10 In the NHANES report, moderate-to-severe anemia was 5 times more common among non-pregnant females relative to men (2.5% vs. 0.5%, P<0.0001).10
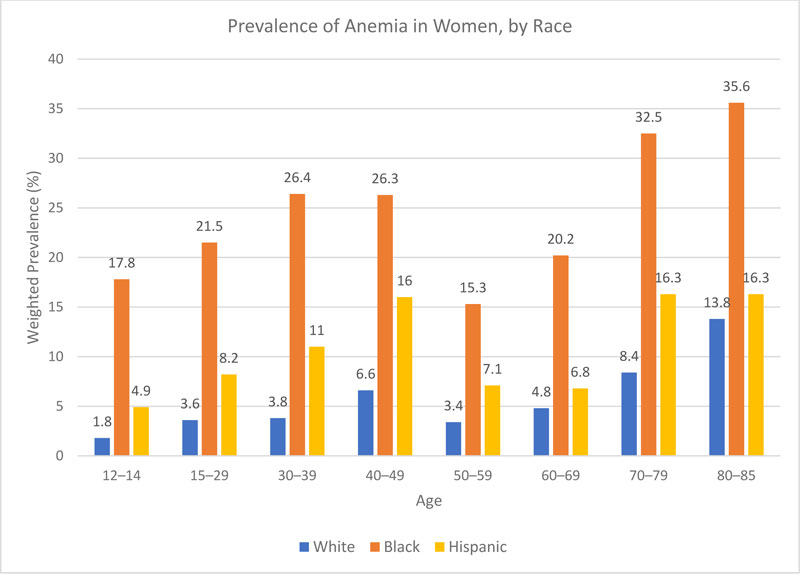 |
Figure 2. Prevalence of Anemia in Women, by Race10
NHANES data from 2003 to 2012 (n=41,026) broken down by race show significantly higher weighted prevalence of anemia among black and Hispanic women across all age ranges. [Source: Le CHH. PLoS One. 2016;11(11):e0166635. Open Access.] |
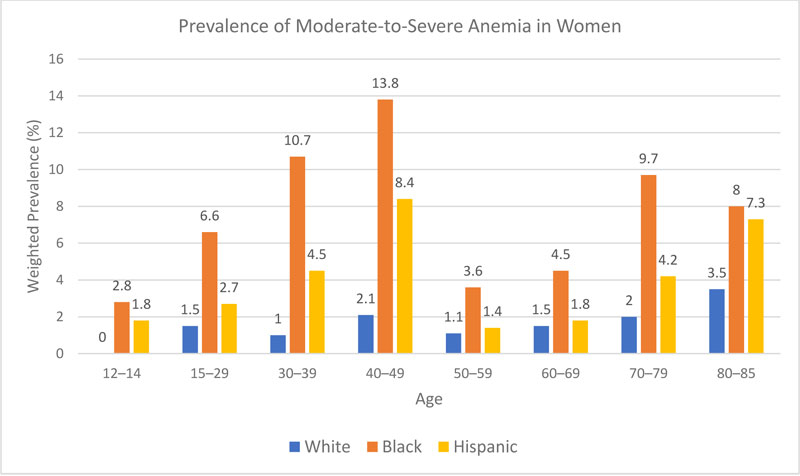 |
Figure 3. Prevalence of Moderate-to-Severe Anemia in Women, by Race10
NHANES data from 2003 to 2012 show disproportionate rates of moderate to severe anemia in women of black or Hispanic racial origin. [Source: Le CHH. PLoS One. 2016;11(11):e0166635. Open Access.] |
|
The most recent NHANES report on anemia prevalence in the U.S. identified a large jump in overall anemia prevalence—from 4% at the beginning of study (2003) to 7.1% in 2012, and a near doubling of moderate-to-severe anemia rates. This was especially notable in segments of the female population, for example, an increase from 3.7% in 2003 to 6.1% in 2009 among white women.10
|
Despite efforts to raise awareness, the prevalence of anemia has increased steadily in the overall population, from 4% in 2003 to 7.1% in 2012, along with a near-doubling of moderate-to-severe anemia. This was especially notable in some segments of the population (e.g., an increase from 3.7% in 2003 to 6.1% in 2009 among white women).10 The cause of this steadily increasing prevalence across populations remains unclear.10
Causes, Signs, and Symptoms of Anemia
Women at highest risk for iron deficiency and anemia include those who are menstruating, pregnant, or postpartum.4 Women have the potential to lose a significant amount of iron through menstruation—about 16 mg of iron for the average menstrual period (35 mL), which may increase to 36 mg or more for women with abnormal uterine bleeding.11 If the body's iron stores contain an average of 3,000–4,000 mg, average menstrual blood loss equals about 0.4 to 0.5% of total body iron.11 Studies show that women with heavy menstrual cycles (abnormal uterine bleeding) are at higher risk for iron deficiency and anemia.5,11 Some causes of abnormal uterine bleeding include:5
- fibroids
- miscarriage or ectopic pregnancy
- intrauterine device (IUD) and related complications
- pelvic inflammatory disease
- uterine, ovarian, and cervical cancers
Women who are competitive athletes are at increased risk for iron deficiency, as are those who are dieting or who consume a primarily vegetarian diet.12 Anemia may be caused or exacerbated by occult blood loss from the gastrointestinal (GI) tract, thus increasing the risk in non-menstruating women with GI diseases or dysfunction.13 Gastritis, celiac disease, and Helicobacter pylori infection are causes of anemia related to gastric malabsorption of iron. An increasingly common cause of gastric malabsorption is gut resection or bypass surgery for weight loss.14 Bariatric surgery also leads to vitamin B12 and/or folate deficiency, which can contribute to anemia. Aside from iron deficiency, other causes of anemia include blood loss, hemolysis, bone marrow disease, use of medications that suppress bone marrow function, kidney disease, malignancy, hemoglobinopathy, and vitamin B12 or folate deficiency.15
Anemia develops slowly and insidiously and is frequently confused with other causes of fatigue, especially among adolescent and teenage girls.5,16 Patients with chronic health conditions such as kidney failure or congestive heart failure are usually monitored carefully for anemia, but detection is often missed in otherwise-healthy women.15 Similarly, progression from iron deficiency to anemia is slow and insidious. When symptoms develop, they are often nonspecific and may be blamed on an overly busy or stressful lifestyle. Some symptoms of iron deficiency are shown in Figure 4.17,18
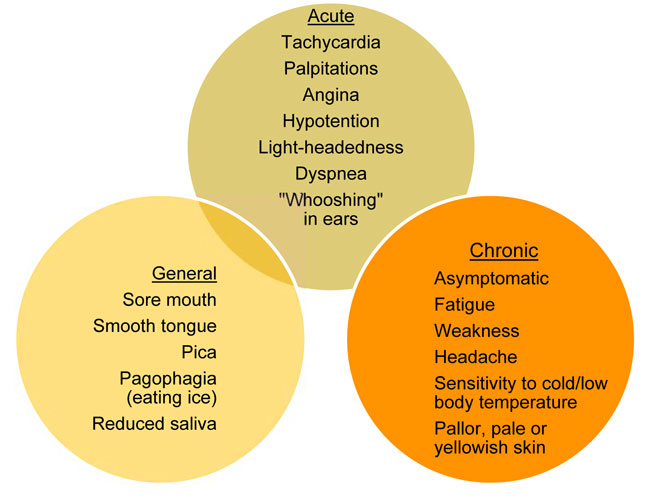 |
| Figure 4. Signs and Symptoms of Iron Deficiency17,18 |
Iron deficiency anemia is associated with significant health effects including altered mental development and learning capacity, shortened attention span, irritability, fatigue, weakness, and susceptibility to infection.19,20 Women with anemia are more likely to need blood transfusions, require emergency room visits, and generate higher hospitalization costs.5 Anemia causes particular complications during pregnancy, childbirth, and in the postpartum period, as discussed later in this article.
Diagnosing Iron Deficiency and Anemia
Iron deficiency and anemia are typically diagnosed by measuring serum hemoglobin (Hb) and serum ferritin (Table 1).21 Checking ferritin levels may allow for early detection of iron deficiency when hemoglobin is within normal range.14 As the cellular storage protein for iron, ferritin is present in small concentrations in blood, so its concentration typically correlates with total body iron stores. However, ferritin is released from damaged hepatocytes, so its levels may be falsely elevated in the presence of chronic or acute inflammation, liver disease, renal failure, metabolic syndrome, or malignancy.14,17,22
| Table 1. Hemoglobin and Ferritin Thresholds for Anemia in Women21 |
| Population |
Anemia
Hemoglobin
(g/dL) |
Moderate-to-severe anemia
Hemoglobin (g/dL) |
Anemia
Serum ferritin (ng/mL) |
| Women (age over 15 years, non-pregnant) |
<12 |
<11 |
<15–30 |
| Pregnant women (first and third trimester) |
<11 |
<10 |
<30 |
| Men (age over 15 years) |
<13 |
<11 |
<15–30 |
| Data adapted from: World Health Organization. Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. 2011. Available at: http://apps.who.int/iris/bitstream/10665/85839/3/WHO_NMH_NHD_MNM_11.1_eng.pdf |
Anemia in Pregnancy
Pregnancy and the postpartum period are associated with high risk for anemia. Of the approximately 4 million women who give birth each year, about 2 million become iron deficient and more than 1 million develop postpartum anemia.23 During pregnancy, iron intake must increase to meet heightened demand, which includes red blood cell (RBC) volume increases of 20% to 30% and increased iron requirements of 5 to 7 mg per day.24
NHANES data from 1999–2006 showed the prevalence of iron deficiency among U.S. women was 7% in the first trimester of pregnancy, 14% in the second, and 30% in the third.25 Some factors that increase the risk during pregnancy include:26
- having a heavy menstrual flow prior to becoming pregnant
- low dietary consumption of iron
- multiple fetuses
- frequent vomiting
- pregnancies close together
Iron deficiency and anemia during pregnancy carry significant health risks for the mother and the infant, including preterm delivery, low birth weight, excessive blood loss during labor, need for blood transfusion, infection, and intensive care admission.25,26 Especially in low- and middle-income countries, maternal anemia is associated with heightened risk for both perinatal mortality and neonatal mortality.27 Improved education is needed to increase awareness among healthcare professionals about the occurrence of iron deficiency and anemia in pregnancy, so at-risk patients can be properly screened and treated.
Screening in Pregnant Women
Screening for iron deficiency and anemia in pregnant women is recommended by organizations including the American College of Obstetricians and Gynecologists (ACOG), WHO, and the Centers for Disease Control and Prevention (CDC), as summarized in Table 2.28,29 In addition to standard blood tests, vitamin B12 and folate levels may be checked to explore potential causes of anemia.13
| Table 2. Recommended Screening and Evaluation of Iron Deficiency in Pregnant Women |
| Hemoglobin (Hb) and hematocrit (Hct) at first prenatal visit and early in third trimester28 |
| Anemia in pregnancy defined as Hb <11 g/dL or Hct <33% in the first and third trimesters29 |
| Serum ferritin measured at first prenatal visit and early in third trimester to assess maternal iron stores28 |
| Pregnant women with anemia: iron deficiency is present if ferritin is <30 ng/mL (if iron levels are sufficient, check for other causes of anemia)17 |
| Pregnant woman who are not anemic: iron deficiency is present if ferritin is <15 ng/mL, or between 15 and 30 ng/mL30 |
|
"There is an epidemic of iron deficiency in pregnant women in the United States. In an era of high technology medicine, it is surprising that iron deficiency remains an unsolved obstetric problem in our country."31
|
Oral Iron Supplements in Pregnancy
Interventions to prevent iron deficiency and anemia in pregnant women include supplementing iron and folic acid and ensuring sufficient dietary intake of iron along with other vitamins and minerals. The CDC recommends supplementing with 30 mg elemental iron orally per day for most pregnant women.29 An exception is women who have hemochromatosis, a metabolic disorder associated with excess iron. Pharmacists should be aware that not all prenatal vitamins contain iron; those that do typically contain 17 to 28 mg elemental iron per dose. Oral iron supplementation should begin when pregnancy is confirmed and be maintained throughout the duration. More detail on oral iron supplementation can be found in the Treatment section.
Intravenous Iron in Pregnancy
For women in their second or third trimesters of pregnancy who require iron supplementation, IV iron is recommended for those who cannot tolerate or have an insufficient response to oral iron. When anemia is treated later in the pregnancy (e.g., third trimester) there may be insufficient time to make up iron stores with dietary sources or oral iron supplements.24,32 Gastric bypass surgery may result in severe impairment of intestinal iron absorption, so pregnant women with a history of these procedures often require IV iron.18 IV iron is associated with fewer GI side effects compared with oral iron, which is usually a benefit for pregnant women. For more detail on IV iron, see the Treatment section.
Postpartum Anemia
Iron deficiency and anemia are common in the postpartum period and represent significant health problems in women of reproductive age. Postpartum anemia is defined as:33,34
- Hb <10 g/dL within 24 to 48 hours after delivery
- Hb <11 g/dL at 1 week postpartum
- Hb <12 g/dL at 8 weeks postpartum
Postpartum anemia is surprisingly common. In developing countries, the prevalence may be as high as 50%–80% and the condition is associated with high rates of maternal morbidity and mortality.34 European studies have reported rates of 22% to 24%. In the U.S., higher rates of postpartum anemia (27%) have been observed in low-income populations.35 Interestingly, in a Danish study of healthy women, the prevalence of postpartum anemia at 1 week following normal delivery was 14% for women who took an iron supplement and 24% among those not taking a supplement.16
Prevention of Postpartum Anemia
Ideally, efforts should be made to identify and address anemia prior to delivery. International guidelines recommend that pregnant women, especially those with antenatal anemia, have their hemoglobin levels screened and anemia corrected prior to delivery if possible.34 Hemoglobin concentrations also should be checked in women who experience significant peripartum bleeding.34 Those with moderate-to-severe anemia or high risk for hemorrhage should be advised to deliver in a hospital setting.34 Pregnant women should by typed for blood groups (ABO and Rh factor) and screened for the presence of red cell antibodies early in pregnancy and at 28 weeks' gestation. In women who are Rh negative, the 28-week sample should be taken before the administration of routine antenatal anti-D Ig prophylaxis.34
Treatment: Oral Iron Supplementation
Dietary Sources of Iron
Iron is absorbed from the diet in two forms: nonheme iron from plants and fortified foods and heme iron from animal sources. In people who consume meat, heme iron contributes at least 10% to 15% of total absorbed iron.36 Nonheme iron is usually much less well absorbed than heme iron. Iron absorption is inhibited by phytates and polyphenols in beverages such as tea and coffee beverages. Iron bioavailability may be reduced by calcium found in foods. Absorption of iron can be enhanced by supplementation of ascorbic acid, which may counteract the effects of all dietary inhibitors of iron absorption. Foods highest in iron content include fortified breakfast cereals such as cream of wheat, canned white beans, dark chocolate, beef liver, lentils, spinach and tofu.36
Some commonly used oral iron formulations are summarized in Table 3.24,37 Oral iron supplementation of 60 mg to 120 mg elemental iron daily is the preferred initial treatment for iron deficiency and anemia in most patients.14,29,38 A potential disadvantage of oral iron supplementation is its tendency to produce a slow and often suboptimal response. Heme iron is better absorbed than non-heme iron, but it will not be accepted if the person is vegetarian.39 Oral iron may be insufficient to resolve severe anemia in certain patient groups due to factors such as poor absorption, poor patient adherence, gastrointestinal side effects of oral iron (which occur in up to 70% of patients), and premature discontinuation of treatment.18 Ferritin and hemoglobin levels should be rechecked about 4 weeks after initiation of oral iron therapy to determine whether expected increases (1 g/dL hemoglobin) occurred.31
| Table 3. Commonly Available Oral Iron Formulations40 |
Agent
(% elemental iron) |
Dosage form |
Elemental
irondose |
| Ferrous gluconate (12%) |
325 mg tablet |
38 mg |
| Ferrous sulfate (20%) |
220 mg/5mL oral solution
325 mg immediate-release tablet
160 mg extended-release tablet |
44 mg
65 mg
50 mg |
| Ferrous fumarate (33%) |
325 mg tablet
150 mg extended-release tablet |
107 mg
107 mg |
| Polysaccharide iron complex (100%) |
150 mg capsule |
150 mg |
GI effects from oral iron include nausea, constipation, diarrhea, epigastric distress, metallic taste, and greenish/black stool.18 To increase tolerability, pharmacists may recommend reducing the dose, or intermittent administration. Alternate-day oral dosing has been shown to allow for a higher fraction of the iron dose to be absorbed while reducing the incidence of nausea.41 GI tolerability can also be improved by taking the supplement with food or at bedtime, although combining oral iron with food can significantly decrease iron absorption.36 If swallowing pills is the issue, a liquid iron supplement can be taken in juice or other liquids. There are many iron salts and different oral iron supplements available, but minimal data exist to suggest advantages of one over another. Sustained-release preparations may result in fewer adverse GI effects, but due to their release further down the GI tract they may also result in reduced iron absorption.18
Oral Iron in Pregnancy
For pregnant women with low ferritin levels and anemia, recommended oral iron doses range from 30 to 120 mg daily.29 Optimal absorption has been shown with daily doses of 40 to 80 mg elemental iron.42 Higher iron doses do not necessarily allow for greater iron absorption and may worsen adverse effects (AEs). Absorption of oral iron is enhanced by vitamin C derived from diet or supplements. Many pregnant women discontinue oral iron due to GI effects, especially those who are on doses greater than 30 mg daily.12 Tolerability problems are heightened for women who experience nausea, constipation, or exaggerated gag reflexes during pregnancy.43
Oral Iron in the Postpartum Period
Oral iron supplementation, either alone or in combination with folic acid, is recommended for a period of 6 to 12 weeks following childbirth to reduce the risk of anemia, especially in areas where gestational anemia is a public health concern.34 For women with mild-to-moderate postpartum anemia (Hb 9–11 g/dL) who are hemodynamically stable and asymptomatic or mildly symptomatic, an oral daily dose of 80 to 100 mg elemental iron is recommended for a period of 3 months.17,33
Oral iron supplementation should be continued for 3 months after normalization of RBC indices, to ensure replenishment of iron stores. Hb and ferritin levels should be monitored every 3 months for the first year and after 1 year, or if signs or symptoms of anemia recur.13
Treatment: IV Iron Supplementation
Although some healthcare professionals may assume that only critically ill patients need IV iron, IV iron therapy is the recommended approach for treatment of anemia in many women under certain circumstances.31 Indications for IV iron are summarized in Table 4.14 For women who are pregnant, IV iron can be useful in the antenatal period to correct iron deficiency anemia and elevate hemoglobin levels prior to delivery, with the goal of reducing hemorrhage risk and the need for peripartum transfusions.44 In addition, studies have shown that IV iron may be more effective than oral iron when treating women with abnormal uterine bleeding.44
| Table 4. Indications for Intravenous Therapy In Patients with Iron Deficiency Anemia14 |
|
IV administration of iron should be considered in patients with confirmed iron deficiency anemia and 1 or more of the following:
- Demonstrated intolerance, nonadherence, or lack of efficacy with oral iron therapy, despite modification of dose, timing and frequency;
- Pregnancy (beyond the first trimester) and postpartum women, for the above reasons or to avoid imminent decompensation/transfusion (e.g., in women who present late and/or display severe anemia);
- Intestinal malabsorption (e.g., inflammatory bowel disease);
- Ongoing iron losses (i.e., from blood) exceeding absorptive capacity;
- Clinical need for rapid iron supply (i.e., in patients where optimization of erythroid response is important to prevent physiological decompensation/ transfusion);
- Chronic renal impairment receiving concomitant erythropoietin-stimulating agent therapy.
|
| Adapted from: Pasricha SR, et al. Diagnosis and management of iron deficiency anaemia: a clinical update. Med J Aust. 2010;193:525-532.14 |
IV iron doses are highly individualized. Many severely iron deficient patients need over 1000 mg (with an average of 1500 mg or greater) of iron to resolve their deficit. In order to avoid giving multiple standard doses, an FDA-approved regimen is administration of 2 doses of 750 mg for a total cumulative dose of 1500 mg of iron per course..18 Some practices administer multiple smaller doses of IV iron, such as IV iron sucrose (300 mg) every 2 weeks for 3 doses. See Table 5 for IV iron formulations and dosing.
Concerns about serious AEs have historically caused practitioners to hesitate in prescribing high-dose IV iron, and some providers still hesitate today, despite advances in available IV iron formulations.14,44 These safety concerns stemmed mainly from the risk of serious allergic reactions attributed primarily to earlier formulations of high molecular weight (HMW) iron dextran, which are no longer available in the U.S.45 Low molecular weight (LMW) iron dextran carries a lower risk of serious AEs. Ferric carboxymaltose is an IV iron formulation approved in 2013 that allows for administration of high doses over a short period of time, without the need for a test dose.44,46
| Table 5. Parenteral Iron Agents, Adult Doses47-51 |
| Iron sucrose injectable solution, 20 mg Fe/mL (Venofer®) |
| Indication |
Dose |
Dosage Notes/Precautions |
| CKD, Non-dialysis |
200 mg IV per dose (over 2-5 min or via infusion over 15 min); 5 doses over 14 days |
Cumulative 1,000 mg in 14 days |
| CKD, Dialysis dependent |
100 mg (over 2–5 min or via infusion over 15 min) per dialysis session |
Do not exceed cumulative total dose of 1,000 mg divided in 3 doses/week |
| CKD, Peritoneal dialysis-dependent |
300 mg IV over 1.5 hr for 2 doses, 14 days apart. Then, 400 mg IV over 2.5 hr 14 days later |
|
| LMW iron dextran injectable solution, 50 mg Fe/mL (INFeD®) |
| Indication |
Dose |
Dosage Notes/Precautions |
| Iron deficiency |
0.0442 (desired Hgb–observed Hgb) x LBW + (0.26 x LBW) |
Give test dose of 0.5 mL and observe patient for 1 hour prior to giving remainder of therapeutic dose
Refer to labeling for boxed warning on precautions against anaphylactic reactions including test dose |
| Blood loss |
Total dose (mg)= blood loss (mL) x HCT |
See formula in labeling for dose calculation |
| Ferric gluconate injectable solution, 12.5 mg Fe/mL (Ferrlecit®) |
| Indication |
Dose |
Dosage Notes/Precautions |
| Iron deficiency/anemia |
125 mg IV infusion over 1 hr |
Most patients require 250 mg/infusion for 8 dialysis sessions
Do not exceed 12.5 mg/min administration rate |
| Ferric carboxymaltose injectable solution, 50 mg Fe/mL (Injectafer®) |
| Indication |
Dose |
Dosage Notes/Precautions |
Iron deficiency/anemia
Patient weight < 50 kg |
2 doses of 15 mg/kg body weight separated by at least 7 days. Administer as IV infusion (over at least 15 min) or a slow IV push (100 mg/min) |
Do not exceed 1,500 mg elemental iron per course |
| Patient weight ≥ 50 kg |
2 doses of 750 mg separated by at least 7 days, for a cumulative dose of 1,500 IV iron per course. Administer as 15-minute IV infusion or a slow IV push (100 mg/min) |
Do not exceed 1,500 mg per course |
| Ferumoxytol, 30 mg Fe/mL (Feraheme®) |
| Indication |
Dose |
Dosage Notes/Precautions |
| Iron deficiency/anemia |
510 mg IV over at least 15 minutes, followed by 510 mg IV infusion over at least 15 minutes 3 to 8 days later |
No data in pregnancy
Boxed warning for anaphylactic reactions. No test dose recommended. |
| Fe=iron; CKD=chronic kidney disease; IV=intravenous; LMW= low molecular weight; Hgb=hemoglobin; LBW= lean body weight; HCT=hematocrit |
IV Iron in the Postpartum Period
Postpartum women with moderate-to-severe anemia (Hb <9 g/dL) should receive IV iron rather than oral supplements. Severely anemic patients with blunted erythropoiesis due to infection and/or inflammation who do not respond adequately to IV iron treatment (and severely anemic patients who refuse blood transfusions) may require treatment with an erythropoiesis-stimulating agent (ESA) in consultation with the hematologist.34
Safety Aspects of IV Iron
Parenteral iron therapy provides a greater and more rapid iron supply compared with oral iron supplementation.13 It is important for pharmacists to be aware of the available formulations and indications for use of IV iron. For each IV iron formulation, the pharmacist should be aware of:
- Need for pre-dose testing (recommended with low-molecular weight iron dextran)
- Product-specific administration instructions including infusion and bolus dosing recommendations
- Potential infusion-related adverse effects
Premedication with antihistamines is not indicated for IV iron, except for test doses of LMW iron dextran, and may cause adverse effects if used.52 Acute AEs usually present during the test dose, but can occur during infusion.53 IV iron should be administered in a setting where AEs can be managed. Possible mild-to-moderate adverse effects of IV iron are hypotension, transient self-limiting infusion reactions (mild chest discomfort or flank or facial flushing), abdominal pain, nausea, headache, or diarrhea.52 Risks of serious AEs are low with newer formulations of IV iron. A retrospective analysis of FDA adverse drug event data showed that LMW iron dextran had a significantly lower rater of serious AEs than HMW iron dextran.54 Iron sucrose and ferric gluconate and must be given in lower doses due to risk of infusion reactions above 300 mg and 250 mg, respectively.18
There is not strong evidence to support significant differences in safety or efficacy among the commercially available IV iron products.18 Newer IV iron formulations available in the U.S. include ferumoxytol and ferric carboxymaltose. Ferric carboxymaltose has a nearly neutral pH (5.0 to 7.0) and physiologic osmolarity, making it possible to administer higher single doses over shorter time periods compared with other parenteral preparations.55 Because it releases elemental iron more slowly than iron sucrose or ferric gluconate, it allows for complete replacement dosing in a time period of 15 to 60 minutes without the need for a test dose.52 A head-to-head study comparing IV iron sucrose and IV ferric carboxymaltose in a group of 200 women with iron-deficiency anemia showed a more rapid restoration of hemoglobin levels and higher quality of life measures for the latter agent.56 Ferumoxytol has been shown to be effective and well tolerated in patients with GI disorders, cancer, CKD, and iron deficiency anemia.57,58 In a safety evaluation in patients with varying degrees of kidney function, IV ferumoxytol was shown to have comparable safety profile to iron sucrose.59
Pharmacist Involvement in the Management of Anemia
Pharmacists are well positioned to improve diagnosis and management of anemia in women. Roles of the pharmacist may include:60
- recommendation of screening or testing for patients
- selection of oral or IV therapies
- evaluation of formulary options
- education of healthcare professionals and patients
- development of dosing and monitoring protocols
- promoting quality improvement
- reducing costs of care61
Several studies have validated the role of pharmacists in improving patient outcomes in the management of anemia.60-63 In hospital and health-system settings, responsibilities of pharmacists may include screening patients for anemia, developing guidelines for selection and use of therapies, providing patient education, and reducing costs of care.61 In hospitals, pharmacists need a clear understanding of the important distinctions between different formulations of oral and IV iron supplementation and how to select the dose and administer these agents.
Community pharmacists are often called upon to advise patients about selection of oral iron products, minimizing GI adverse effects and optimizing iron absorption, and when to contact their physician for further evaluation and treatment. Because oral iron can be difficult to tolerate, pharmacists may advise patients to take them at bedtime or on alternate days. Forms of supplemental iron other than ferrous or ferric salts—including heme iron polypeptides, carbonyl iron, iron amino-acid chelates, and polysaccharide-iron complexes—might have fewer GI side effects.64 Some patients find that liquid preparations are easier to tolerate than iron tablets.
Pharmacists should be aware of potential absorption issues resulting from co-administration of oral iron with other medications and foods (see Table 6).4,64 Patients should be made aware of the potential toxicity of oral iron supplements and be advised to take necessary precautions around young children.64
| Table 6. Oral Iron Absorption Interactions4,6,40 |
| Iron absorption decreased by coadministration with: |
Gastric acid suppressants:
Antacids
Proton pump inhibitors
H2 receptor blockers
Tetracycline/doxycycline
Dairy products (calcium)
Tea (tannins, polyphenols)
Some vegetables (polyphenols)
Bran cereals (phytates) |
| Iron absorption increased by coadministration with: |
Ascorbic acid (Vitamin C) |
| Drugs whose absorption/efficacy are decreased by coadministration with iron |
Levodopa/methyldopa
Levothyroxine
Bisphosphonates
Fluoroquinolones
Tetracycline/doxycycline |
Patients who exhibit symptoms of iron deficiency, have a history of anemia, or who have difficulty tolerating oral iron should be referred for further medical evaluation. By being aware of the prevalence, groups at highest risk, and signs and symptoms of iron deficiency and anemia, pharmacists can make recommendations for screening or monitoring of iron levels and other causes of anemia. In addition, pharmacists in the community need to be aware of the available forms of iron replacement and appropriate dosage and administration.
Conclusion
Iron deficiency and anemia are often overlooked and can cause serious health problems. Abnormal uterine bleeding, pregnancy, and the postpartum period place women at significantly higher risk for anemia relative to men. There is a need for greater understanding regarding the high prevalence of iron deficiency among women and awareness of current guidelines for evaluation, monitoring, and management. Pharmacists in the community are often in a position to educate patients about iron supplementation. In hospital and infusion center settings, pharmacists may be involved in the selection, preparation, administration and monitoring of IV iron doses. Thus pharmacists have the potential to expand awareness, improve anemia management, and implement effective patient education.
References
- Iron deficiency--United States, 1999-2000. MMWR Morb Mortal Wkly Rep. 2002;51(40):897-899.
- Markova V, Norgaard A, Jorgensen KJ, et al. Treatment for women with postpartum iron deficiency anaemia. Cochrane Database Syst Rev. 2015(8):Cd010861.
- Barroso F, Allard S, Kahan BC, et al. Prevalence of maternal anaemia and its predictors: a multi-centre study. Eur J Obstet Gynecol Reprod Biol. 2011;159(1):99-105.
- Coad J, Pedley K. Iron deficiency and iron deficiency anemia in women. Scand J Clin Lab Invest Suppl. 2014;244:82-89; discussion 89.
- Morrison J, Patel ST, Watson W, et al. Assessment of the prevalence and impact of anemia on women hospitalized for gynecologic conditions associated with heavy uterine bleeding. J Reprod Med. 2008;53(5):323-330.
- Mirza FG, Abdul-Kadir R, Breymann C, et al. Impact and management of iron deficiency and iron deficiency anemia in women's health. Expert Rev Hematol. 2018;11(9):727-736.
- Debenito JM, Billups SJ, Tran TS, et al. Impact of a clinical pharmacy anemia management service on adherence to monitoring guidelines, clinical outcomes, and medication utilization. J Manag Care Spec Pharm. 2014;20(7):715-720.
- World Health Organization (WHO). Iron deficiency anaemia: assessment, prevention and control. A guide for programme managers. World Health Organization: Geneva, Switzerland;2001.
- U.S. Department of Health and Human Services (HHS). Office on Women’s Health. Iron-deficiency anemia. www.womenshealth.gov. Accessed July 30, 2018.
- Le CH. The Prevalence of Anemia and Moderate-Severe Anemia in the US Population (NHANES 2003-2012). PLoS One. 2016;11(11):e0166635.
- Miller EM. The reproductive ecology of iron in women. Am J Phys Anthropol. 2016;159(Suppl 61):S172-195.
- McClung JP. Iron status and the female athlete. J Trace Elem Med Biol. 2012;26(2-3):124-126.
- Goddard AF, James MW, McIntyre AS, et al. Guidelines for the management of iron deficiency anaemia. Gut. 2011;60(10):1309-1316.
- Pasricha SR, Flecknoe-Brown SC, Allen KJ, et al. Diagnosis and management of iron deficiency anaemia: a clinical update. Med J Aust. 2010;193(9):525-532.
- Miller JL. Iron deficiency anemia: a common and curable disease. Cold Spring Harb Perspect Med. 2013;3(7).
- Milman N. Anemia--still a major health problem in many parts of the world! Ann Hematol. 2011;90(4):369-377.
- Api O, Breyman C, Cetiner M, et al. Diagnosis and treatment of iron deficiency anemia during pregnancy and the postpartum period: Iron deficiency anemia working group consensus report. Turk J Obstet Gynecol. 2015;12(3):173-181.
- Auerbach M, Adamson JW. How we diagnose and treat iron deficiency anemia. Am J Hematol. 2016;91(1):31-38.
- Kordas K, Lopez P, Rosado JL, et al. Blood lead, anemia, and short stature are independently associated with cognitive performance in Mexican school children. J Nutr. 2004;134(2):363-371.
- McCann JC, Ames BN. An overview of evidence for a causal relation between iron deficiency during development and deficits in cognitive or behavioral function. Am J Clin Nutr. 2007;85(4):931-945.
- World Health Organization. Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity, 2011. Available at: http://apps.who.int/iris/bitstream/10665/85839/3/WHO_NMH_NHD_MNM_11.1_eng.pdf.
- Breymann C, Honegger C, Hosli I, et al. Diagnosis and treatment of iron-deficiency anaemia in pregnancy and postpartum. Arch Gynecol Obstet. 2017;296(6):1229-1234.
- Pasricha SR. Should we screen for iron deficiency anaemia? A review of the evidence and recent recommendations. Pathology. 2012;44(2):139-147.
- Bothwell TH. Iron requirements in pregnancy and strategies to meet them. Am J Clin Nutr. 2000;72(1 Suppl):257S-264S.
- Mei Z, Cogswell ME, Looker AC, et al. Assessment of iron status in US pregnant women from the National Health and Nutrition Examination Survey (NHANES), 1999-2006. Am J Clin Nutr. 2011;93(6):1312-1320.
- Cao C, O'Brien KO. Pregnancy and iron homeostasis: an update. Nutr Rev. 2013;71(1):35-51.
- Rahman MM, Abe SK, Rahman MS, et al. Maternal anemia and risk of adverse birth and health outcomes in low- and middle-income countries: systematic review and meta-analysis. Am J Clin Nutr. 2016;103(2):495-504.
- Guidelines for Perinatal Care. 8th ed. Washington DC: American Academy of Pediatrics, American College of Obstetricians and Gynecologists (ACOG); 2017.
- Centers for Disease Control and Prevention (CDC). Recommendations to prevent and control iron deficiency in the United States. MMWR Recomm Rep. 1998;47(RR-3):1-29.
- Guyatt GH, Oxman AD, Ali M, et al. Laboratory diagnosis of iron-deficiency anemia: an overview. J Gen Intern Med. 1992;7(2):145-153.
- Schantz-Dunn J, Barbieri RL. Recognize and treat iron deficiency anemia in pregnant women. OBG Manag. 2017;29(12):8-11,16.
- Milman N. Prepartum anaemia: prevention and treatment. Ann Hematol. 2008;87(12):949-959.
- Milman N. Postpartum anemia II: prevention and treatment. Ann Hematol. 2012;91(2):143-154.
- Munoz M, Pena-Rosas JP, Robinson S, et al. Patient blood management in obstetrics: management of anaemia and haematinic deficiencies in pregnancy and in the post-partum period: NATA consensus statement. Transfus Med. 2018;28(1):22-39.
- Bodnar LM, Scanlon KS, Freedman DS, et al. High prevalence of postpartum anemia among low-income women in the United States. Am J Obstet Gynecol. 2001;185(2):438-443.
- Hurrell R, Egli I. Iron bioavailability and dietary reference values. Am J Clin Nutr. 2010;91(5):1461S-1467S.
- Melamed N, Ben-Haroush A, Kaplan B, et al. Iron supplementation in pregnancy--does the preparation matter? Arch Gynecol Obstet. 2007;276(6):601-604.
- Taylor CL, Brannon PM. Introduction to workshop on iron screening and supplementation in iron-replete pregnant women and young children. Am J Clin Nutr. 2017;106(Suppl 6):1547s-1554s.
- West AR, Oates PS. Mechanisms of heme iron absorption: current questions and controversies. World J Gastroenterol. 2008;14(26):4101-4110.
- Iron Preparations, Oral. Drugs.com. Available at: https://www.drugs.com/monograph/iron-preparations-oral.html.
- Stoffel NU, Cercamondi CI, Brittenham G, et al. Iron absorption from oral iron supplements given on consecutive versus alternate days and as single morning doses versus twice-daily split dosing in iron-depleted women: two open-label, randomised controlled trials. Lancet Haematol. 2017;4(11):e524-e533.
- Moretti D, Goede JS, Zeder C, et al. Oral iron supplements increase hepcidin and decrease iron absorption from daily or twice-daily doses in iron-depleted young women. Blood. 2015;126(17):1981-1989.
- Nguyen P, Thomas M, Koren G. Predictors of prenatal multivitamin adherence in pregnant women. J Clin Pharmacol. 2009;49(6):735-742.
- Gozzard D. When is high-dose intravenous iron repletion needed? Assessing new treatment options. Drug Des Devel Ther. 2011;5:51-60.
- Hayat A. Safety issues with intravenous iron products in the management of anemia in chronic kidney disease. Clin Med Res. 2008;6(3-4):93-102.
- Auerbach M, Ballard H. Clinical use of intravenous iron: administration, efficacy, and safety. Hematology Am Soc Hematol Educ Program. 2010;2010:338-347.
- Venofer (iron sucrose) injection [package insert]. Shirley, NY: American Regent, 2019.
- InFed (iron iron dextran) injection [package insert]. Madison, NJ: Allergan, 2018.
- Ferrlecit (ferric gluconate complex in sucrose) injection [package insert]. Bridgewater, NJ: Sanofi-Aventis, 2015.
- Injectafer (ferric carboxymaltose) injection [package insert]. Shirley, NY: American Regent, 2018.
- Feraheme (ferumoxytol) injection [package insert]. Waltham, MA: Amag Pharmaceuticals, 2018.
- Auerbach M, Macdougall IC. Safety of intravenous iron formulations: facts and folklore. Blood Transfus. 2014;12(3):296-300.
- Goldberg ND. Iron deficiency anemia in patients with inflammatory bowel disease. Clinical and experimental gastroenterology. 2013;6:61-70.
- Chertow GM, Mason PD, Vaage-Nilsen O, et al. On the relative safety of parenteral iron formulations. Nephrol Dial Transplant. 2004;19(6):1571-1575.
- Breymann C, Gliga F, Bejenariu C, et al. Comparative efficacy and safety of intravenous ferric carboxymaltose in the treatment of postpartum iron deficiency anemia. Int J Gynaecol Obstet. 2008;101(1):67-73.
- Naqash A, Ara R, Bader GN. Effectiveness and safety of ferric carboxymaltose compared to iron sucrose in women with iron deficiency anemia: phase IV clinical trials. BMC Womens Health. 2018;18(1):6.
- Ford DC, Dahl NV, Strauss WE, et al. Ferumoxytol versus placebo in iron deficiency anemia: efficacy, safety, and quality of life in patients with gastrointestinal disorders. Clin Exp Gastroenterol. 2016;9:151-162.
- Macdougall IC, Strauss WE, McLaughlin J, et al. A randomized comparison of ferumoxytol and iron sucrose for treating iron deficiency anemia in patients with CKD. Clin J Am Soc Nephrol. 2014;9(4):705-712.
- Strauss WE, Dahl NV, Li Z, et al. Ferumoxytol versus iron sucrose treatment: a post-hoc analysis of randomized controlled trials in patients with varying renal function and iron deficiency anemia. BMC Hematol. 2016;16:20.
- Bacchus S, O'Mara N, Manley H, et al. Meeting new challenges in the management of anemia of chronic kidney disease through collaborative care with pharmacists. Ann Pharmacother. 2009;43(11):1857-1866.
- Gilmartin C. Pharmacist's role in managing anemia in patients with chronic kidney disease: potential clinical and economic benefits. Am J Health Syst Pharm. 2007;64(13 Suppl 8):S15-22; quiz S23-15.
- Clapp SE, Bardo JA, Chrymko MM. Implementation of a pharmacist-managed clinic for patients receiving erythropoietin-stimulating agents. Am J Health Syst Pharm. 2008;65(15):1458-1463.
- Gebara SN, Moubayed H. The role of the pharmacist in optimizing the use of erythropoietin stimulating agents. J Oncol Pharm Pract. 2010;16(1):33-37.
- National Institutes of Health (NIH), Office of Dietary Supplements. Iron: Fact Sheet for Health Professionals. Dec 7, 2018. Available at: https://ods.od.nih.gov/factsheets/Iron-HealthProfessional/.
Back Top