
Expired activity
Please go to the PowerPak
homepage and select a course.
Module 1. Diabetes Defined: An Overview of Prevalence and Pathophysiology
INTRODUCTION
Diabetes mellitus has become a disease state of epidemic proportion. This is evidenced by a worldwide prevalence of at least 8.8%, according to data from the International Diabetes Federation.1 This equates to a current 425 million people affected worldwide. The global burden of this disease state is estimated to cause a substantial financial impact in which treatment and possible prevention strategies will play key roles.
Most simply, diabetes mellitus is characterized by higher than normal levels of glucose in the blood. The American Diabetes Association (ADA) classifies diabetes into the following general categories: 2
- Type 1 diabetes (due to autoimmune beta-cell destruction, usually leading to absolute insulin deficiency)
- Type 2 diabetes (due to a progressive loss of beta-cell insulin secretion frequently on the background of insulin resistance)
- Gestational diabetes mellitus (GDM) (diabetes diagnosed in the second or third trimester of pregnancy that was not clearly present before pregnancy)
- Specific types of diabetes due to other causes, e.g., monogenic diabetes syndromes, diseases of the exocrine pancreas (such as cystic fibrosis and pancreatitis), and drug- or chemical-induced diabetes (such as with glucocorticoid use, etc.)
The two most prevalent forms of diabetes are type 1 diabetes (T1D) and type 2 diabetes (T2D). Both T1D and T2D are heterogeneous diseases where the presentation and course of the disease can vary substantially. 2 As noted above, T1D is characterized as an autoimmune disease in which the body is unable to continue to produce insulin because of the destruction of the insulin-producing beta cells in the pancreas. While traditionally thought of as a disease that occurs primarily in children, T1D can occur in both children and adults. 2 T2D is thought to be caused by a genetic predisposition and a complex interaction of metabolic risk factors, such as poor diet, obesity, and inactivity. T2D, while more common in adults, can occur in younger individuals including children and adolescents. Unfortunately, at this time no interventions have been proven to prevent T1D. However, there is evidence showing that lifestyle interventions with the addition of metformin in select individuals can prevent or at least delay T2D.3,4 Per the ADA classification scheme provided above, other types of diabetes include GDM, monogenic diabetes syndromes, diseases of the exocrine pancreas, and drug- or chemical-induced diabetes2 these types of diabetes are very rare and will only be briefly covered in this module. Pharmacists can play a unique role in the management of diabetes through diabetes screening efforts, risk factor modification (e.g., through counseling on lifestyle interventions), medication counseling, and ensuring that patients diagnosed with diabetes receive the appropriate therapies based on their diagnosis and individualized needs.
PREVALENCE
Currently it is estimated that at least 30.3 million people or 9.4% of individuals in the United States (U.S.) have diabetes.5 In the year 2015 alone, the number of U.S. adults aged 20 years or older newly diagnosed with diabetes was 1.5 million. Additionally, 23.8% of the more than 30 million people in the U.S. with diabetes were not yet diagnosed and another 84 million adults (34% of American adults) had prediabetes. These statistics are staggering, and they are projected to continue to grow; estimates currently suggest that 1 in every 3 Americans born today will develop diabetes. The aging population will be most impacted, both in the U.S. and in other countries.6 In 2015, diabetes was reported to be the seventh leading cause of death in the U.S., but this statistic is likely underreported.5 Economically, $245 billion is spent annually on diabetes in the U.S.1 Our present health care system is likely unprepared to handle the complications associated with this disease and the massive financial burden it is expected to bring. In addition, pharmacists and other health care professionals will most certainly be faced with expanding roles in the management of the symptoms and complications of diabetes to meet the need.
TYPE 1 DIABETES (T1D)
Epidemiology
T1D comprises somewhere around 5% to 10% of all diabetes cases worldwide,1 but accounts for over 90% of diabetes cases in childhood and adolescence in most western countries. 7 T1D was previously referred to as “insulin-dependent diabetes” or “juvenile-onset diabetes,” but these terms are no longer recommended since T1D can occur at any age and a fair number of people with T2D are managed with insulin therapy.
For individuals younger than 20 years of age, T1D accounts for the majority of new diabetes cases diagnosed in the U.S.8 The age of presentation peaks at the following two distinctive points: one peak occurs from 4 to 6 years of age and the other peaks in early puberty (i.e., 10 to 14 years of age).9
Clinical Presentation
Children with T1D most commonly present with the abrupt onset of polydipsia, polyuria, weight loss, and hyperglycemia.10 ADA criteria for the diagnosis of diabetes is provided in Table 1. In addition to the measurements provided in the table below, diabetes can also be diagnosed in a patient with classic symptoms of hyperglycemia or hyperglycemic crisis with a random plasma glucose ≥200 mg/dL.2
| Table 1. Criteria for the Diagnosis of Diabetes.2 |
| Fasting plasma glucose (FPG)* |
≥126 mg/dL |
| 2-hour postprandial glucose |
≥200 mg/dL during OGTT |
| A1C |
≥6.5% |
| *Fasting is defined as no caloric intake for at least 8 hours. OGTT = oral glucose tolerance test. |
Children presenting with hyperglycemia usually appear slightly ill with nonspecific complaints, such as lethargy and weight loss, although weight loss occurs in only half of children diagnosed.11 Polyuria may present as bed-wetting or daytime increased urinary frequency and/or incontinence in a previously potty-trained child. Other symptoms may include blurry vision, drowsiness, poor stamina, frequent skin and bladder infections, and vaginitis. Adults present similarly, but symptoms may not be as abrupt. For adults, longer time frames from the onset of disease to the diagnosis often occur as the result of a decreased rate of beta-cell destruction.2
T1D can in some cases first present as diabetic ketoacidosis (DKA). The reported frequency of children with T1D initially presenting in DKA is approximately 25-30% of cases,12,13 but varies depending on the study. Younger children are generally more likely to present in DKA when compared to older children and adolescents, with more than half of children under the age of 3 years initially presenting in DKA.14 Children are more likely than adults to present in DKA and this syndrome is characterized by nausea and vomiting, breathlessness, and abdominal pain.15 Laboratory values will indicate that hyperglycemia, glucosuria, ketonemia, and ketonuria are present. In addition, patients may also develop a fruity-smelling breath and increased drowsiness and lethargy. DKA also leads to profound dehydration associated with polyuria and sometimes acute vomiting. Children younger than 6 or those from an adverse socioeconomic background are more likely to present in DKA.16 Patients with DKA will require immediate treatment, including rehydration and insulin therapy in the hospital setting.
After diagnosis, many patients enter a honeymoon phase, in which some endogenous insulin production remains and only small amounts of exogenous insulin is required to maintain glycemic control.17 This time period is transient and beta-cell destruction continues, leading to a complete reliance on exogenous insulin to manage glucose.
Pathophysiology
It has long been assumed that T1D results from an interplay between genetics and environment. More specifically, in a person who is genetically predisposed to the disease, environmental triggers are thought to cause an autoimmune response that leads to destruction of pancreatic beta cells (i.e., cells that excrete insulin) and, ultimately, insulin deficiency and metabolic abnormalities.8 Additionally, there does appear to be a common cascade of events in the progression of the immune-mediated illness. These events include a long period of time prior to diagnosis in which immune markers are present and beta-cell destruction is occurring (i.e., reported to be as long as 9 years), high blood glucose levels (during which a majority of pancreatic beta cells are destroyed), a transient period of remission known as the honeymoon phase (during which the individual appears to produce some insulin) and, finally, established disease.15
| Figure 1. Pathophysiology of Type 1 Diabetes Timeline |
 |
| Source: UpToDate.com. Accessed April 14, 2019. |
RISK FACTORS
Family History
Studies show that the lifetime risk of developing T1D is greater for those who have close relatives with T1D.7 The risk of T1D broken down by genetic susceptibility is shown below in Table 2:7,18,19
Table 2. Lifetime Risk of Developing T1D Based on Genetic Susceptibility.
- No family history: 0.4%
- Mother has T1D: 1-4%
- Father has T1D: 3-8%
- Both parents have T1D: Reported as high as 30%
- Non-twin sibling with T1D: 3-6% by age 20; 10% by age 60
- Dizygotic twin with T1D: 8%
- Monozygotic twin with T1D: 30% within 10 year of diagnosis of first twin; 65% by age 60
|
Of note in Table 2, the risk of developing T1D is a bit higher if the father contributes the disease instead of the mother.
Race/Ethnicity
Ethnic differences in the incidence of T1D are also apparent in the U.S. The highest prevalence of T1D was seen in non-Hispanic white youths, according to a 2009 study that sampled large multiethnic populations.20 Non-Hispanic whites younger than 20 years of age seem to have the highest incidence of T1D in the U.S., at 23.6 per 100,000 person-years.9 The incidence for African-Americans, Hispanics, Asian-Pacific Islanders, and American Indians followed in respective order, from rates highest to lowest after non-Hispanic youths. These observations of ethnic-specific risk factors are likely contributed to gene polymorphisms.
Genetic Markers
T1D is most definitely a polygenic disorder and more than 40 genetic polymorphisms that confer susceptibility to T1D have been identified.21 Multiple genes are reported to influence the risk of T1D, including human leukocyte antigen (HLA)-DQalpha, HLA-DQBeta, HLA-DR, preproinsulin, the PTPN22 gene, CTLA-4, interferon-induced helicase, interleukin (IL)-2 receptor (CD25), and many others. The genes most responsible for familial aggregation of diabetes are within the major histocompatibility complex (MHC) located in the HLA region on chromosome-6 and are thought to be responsible for more than 30% to 50% of T1D genetic susceptibility.7,22 Certain combinations of the DQ and DR alleles are associated with a higher risk of T1D. In particular, more than 90% of patients with T1D carry either HLA-DR3, DQB1*0201 or HLA-DR4, DQB1*0302.23 Additionally, DR3/4 heterozygotes are at the greatest susceptibility and carry the DQA1*0501, DQB1*0201, and DQA1*0301, DQB1*0302 gene sequences. These DR3/4 heterozygotes comprise only 2% of the children born in the U.S.; however, these individuals make up 40% of all U.S. children that develop diabetes. In addition, some of the HLA alleles are associated with protection from diabetes including DQA1*0102, DQB1*0602.24 This protective allele occurs in 20% of the general population, but in less than 1% of children who develop T1D.
Non-HLA genes identified as possibly contributing to the development of T1D include the insulin gene (INS) region on chromosome 11, polymorphisms of a promoter of the insulin gene, and an amino acid change of a lymphocyte specific tyrosine phosphatase (PTPN22).25 The association between these genes and the development of diabetes is not as strong as the HLA association. However, MHC susceptibility genes are not sufficient to induce T1D alone, suggesting that polygenic inheritances of non-MHC genes are essential to the development of the disease.24
Autoimmunity
The natural progression of T1D is hypothesized to occur as the result of a combination of genetic susceptibility factors and environmental triggers causing autoimmunity.7 Autoimmunity in T1D is described as the presence of circulating antibodies to islet and/or beta-cell antigens, often long before the disease state becomes evident.26 The exact mechanism as to how beta-cell autoimmunity is initiated after the precipitating environmental factor is not yet fully understood. Several specific autoantigens have been identified that may play important roles in the initiation of injury to the beta cells, including insulin autoantibodies (IAA), tyrosine phosphatase islet antigen 2 (IA2A), islet-specific-glucose-6-phosphatase catalytic-subunit-related protein (IGRP), glutamic acid decarboxylase 65 (GAD65), zinc transporter of islet beta cells (ZnT8) and others.27 The presence of specific autoantibodies can be a useful tool in establishing diagnosis because the risk of developing T1D is strongly correlated with the number of positive antibodies. However, the absence of pancreatic autoantibodies does not rule out the possibility of developing T1D and it is estimated that 5% to 10% of all patients with T1D are not positive for islet autoantibodies.8 This indicates that other islet autoantigens may exist.
Additionally, patients with T1D are also more likely to be diagnosed with other autoimmune disorders, including celiac disease, thyroid disorders (e.g., Graves’ disease and Hashimoto’s thyroiditis), Addison’s disease, multiple sclerosis, and others.2 This suggests that simply having an autoimmune disorder may put a person at greater risk for T1D as well.
Environmental Associations
Despite multiple research efforts aimed at identifying specific environmental triggers for T1D, no clear factor has been linked to islet autoimmunity.28
Geographic location may play a role in predicting the development of T1D. Although the incidence of childhood diabetes is quite variable across the world, specifically in Europe, the risk appears to rise in accordance with one’s distance from the equator.29 The highest reported incidences of T1D occur in Finland and Sardinia, with rates almost 400 times higher than those of children in China and Venezuela, which have the lowest incidence.30,31 However, wide variations in incidence among locations of similar latitude suggest that other factors, besides location, are major contributors.
Perinatal factors, such as maternal age older than 25 years, preeclampsia, maternal diet, maternal infections, jaundice, and neonatal respiratory disease, have been shown to be associated with small increases in risk for developing T1D.32 The observation that T1D autoantibodies often develop early in infancy suggests that fetal exposures may play a role in future disease development. More research is needed in this area for definitive causation to be proven.
Both specific childhood virus exposures and a low overall rate of infection in childhood have been proposed as possible environmental causes of T1D.33 However, this evidence is not conclusive and it is not certain that viruses are involved in causation of the disease. To further confuse the issue, there is evidence that other viruses may protect against the development of T1D, which was suggested by a study that showed increased rates of diabetes in mice that were raised in pathogenic-free environments.34 This theory is similar to the “hygiene hypothesis” and may have to do with the gut microbiome.
It has also been suggested that proteins in cow’s milk may trigger an autoimmune response.35 This is either as a result of early exposure to some component of albumin in the milk or from a cell-mediated response to beta-casein. Longer duration of breast-feeding and supplementation with Vitamin D have been reported to provide partial protection against beta cell autoimmunity and T1D. This research is ongoing as other studies have not found an association between increased rates of T1D and early exposure to cow’s milk or lesser duration of breast-feeding.36
TYPE 2 DIABETES (T2D)
Epidemiology
T2D makes up the majority of diabetes diagnoses and represents approximately 90% to 95% of all diabetes cases worldwide.1 T2D has previously been referred to as “adult-onset diabetes” or “non-insulin-dependent diabetes,” but these terms are no longer recommended for use as children and adolescents can be diagnosed with T2D and people with T2D are sometime managed on intensive insulin therapy. The epidemic of T2D is most certainly linked to increasing rates of overweight and obesity persons in the U.S. The prevalence of T2D is 3 to 7 times higher for obese adults compared with adults at an optimal body weight.37 T2D appears to be most common in both the older and non-white population of the U.S. As much as 25% of Americans older than 65 years or older are shown to have T2D.5 As mentioned above, additional data suggest that the diagnosis of T2D is increasing for the younger population as well. Of the children diagnosed with T2D, 94% are of minority descent, and having overweight or obesity especially increases the risk.
Clinical Presentation
T2D is a disease characterized by hyperglycemia. However, unlike T1D, the onset of T2D tends to progress more gradually over time. Typical first symptoms in adults include fatigue, dry skin, poor wound healing, dry mouth, blurred vision, or sometimes there are no symptoms at all.38 Symptoms tend to be poorly differentiated, but can also present overtly, similar to those of T1D, especially if the disease has gone undetected for longer periods of time. The wide range of symptoms at presentation reflects, in part, the level of insulin resistance and degree of beta-cell damage that has occurred. Many people already experience long-term complications at the time of diagnosis and this has led scientists to estimate that diabetes may typically be present for many years prior to diagnosis. Examples of these complications include neuropathies, retinopathies, cardiovascular issues, and other microvascular complications. Because symptoms at presentation vary so widely and are often not recognized, screening of high-risk persons is critical for identifying those with prediabetes or undiagnosed diabetes and preventing the disorder if possible. Hyperglycemia that is pronounced enough to diagnose diabetes is the same criteria used to diagnosing T1D (see Table 1).2 Hyperlipidemia and hypertension are common metabolic comorbidities in these patients and screening all patients with T2D for blood pressure and lipid abnormalities at diagnosis is recommended.
T2D in children most often occurs in those with overweight or obesity and in those with a family history of the disease. As many as 85% of children diagnosed with T2D have overweight or obesity and as many as 74% to 100% of these children have a first-degree relative with T2D.39 As mentioned before, many of these children are of non-European descent. In general, children present with glycosuria but no evidence of ketonuria, mild thirst complaints, possible slight increase in urination, and little or no weight loss.38 Polycystic ovary syndrome (PCOS) and acanthosis nigricans (thickening and darkening of skin in the neck, groin, or armpit region) are disorders associated with insulin resistance and these are commonly seen in children and adolescents presenting with T2D as well. The onset of childhood T2D typically occurs around puberty, when insulin sensitivity declines. Metabolic disturbances are also seen in children newly diagnosed and include hypertension, dyslipidemia, and microalbuminuria.
Pathophysiology
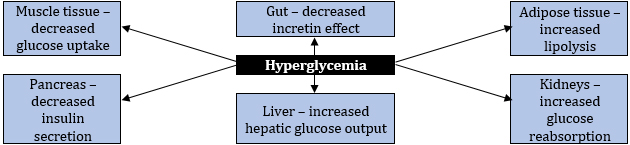
T2D is a progressive disease caused by multiple complex metabolic factors that result from defects of specific organ sites. While the mechanism of this process is not completely understood, it is clear that the following abnormalities are occurring: insulin resistance in muscle and adipose tissue, a progressive decline in pancreatic insulin secretion, higher glucagon levels, which cause increased hepatic glucose production, diminished production of gastrointestinal incretins, and increased renal glucose reabsorption in the kidneys, among other factors.40 This process occurs in a progression of clinically defined phases.
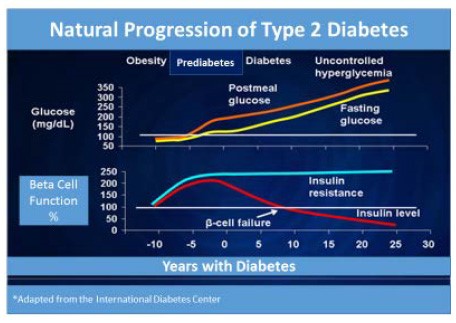
In the initial stage of the disease insulin resistance first occurs, along with impaired insulin sensitivity, and is soon followed by compensatory insulin hypersecretion.38 Almost all patients are asymptomatic at this stage and clinicians are unaware of the disease process. Over time, pancreatic beta-cell secretion of insulin is impaired even further, so that an abnormal rise of blood sugar occurs after meal intake and fasting glucose levels also rise. This phase is typically called prediabetes. Fasting blood glucose typically rises to 100 mg/dL or higher (100 to 125 mg/dL) and this is referred to as impaired fasting glucose. Upon observation, 2-hour postprandial readings climb to 140 mg/dL or higher (140 to 199 mg/dL) when impaired glucose tolerance occurs and hemoglobin A1C readings can be found slightly elevated to 5.7% or greater (5.7% to 6.4%).2 Lastly, overt diabetes occurs as the result of a progressive decline in beta-cell function as well as additional decreases in insulin production. Lack of insulin sensitivity is accompanied by increased hepatic glucose production as well.38 This phase is sufficient enough to produce fasting glucose levels diagnostic of diabetes (126 mg/dL or greater); however, most will still not experience any of the symptoms of diabetes. It is important to remember that progression to diabetes among those with risk factors for diabetes is not inevitable. Several studies, including the Diabetes Prevention Program Research Group, have shown that people with prediabetes who exercise regularly and lose weight can at least delay, if not prevent T2D.4
| Figure 2 – Natural Progression of Type 2 Diabetes.41 |
 |
Insulin Resistance
T2D is a complex syndrome characterized by the following 2 defective insulin-mediated processes: impaired glucose metabolism into insulin-sensitive tissues and the decreased effectiveness of insulin to suppress glucose production by the liver.42 Multiple cellular defects in insulin action have been discovered, including impairment of glucose transport, glucose phosphorylation, glycogenesis, and glucose oxidation. Central obesity appears to be one of the most important causes of insulin resistance development. Insulin resistance also contributes to lipid abnormalities, as evidenced by elevations in triglyceride-rich lipoproteins and decreases in high density lipoprotein (HDL) cholesterol levels for those individuals with hyperinsulinemia. When a patient possesses multiple risk factors for heart disease, including central obesity, elevated lipids, increased blood glucose, and/or hypertension; this myriad of risk factors is called metabolic syndrome.43 These patients are at especially high risk for diabetes and end organ complications. Epidemiological studies suggest that high insulin levels may be associated with coronary artery disease, as well, and that insulin resistance correlated with carotid intimal medial wall thickness.43 A more precise measure of insulin action is critical for defining the relation between insulin resistance and coronary artery disease.
Beta-Cell Dysfunction
Normally, pancreatic beta cells respond to changes in blood glucose and food intake in a complex fashion that maintains normal blood glucose levels throughout the day. T2D impairs beta cell function in several ways. When insulin resistance and increased hepatic glucose output are present, initially pancreatic insulin secretion is increased to compensate for these impairments temporarily. However, persistent fasting hyperglycemia does not allow this compensatory mechanism to continue forever and eventually insulin secretion declines. About 70% of beta-cell function is already lost by the time the 2-hour postprandial glucose level is 120-140 mg/dL.44 Some studies show that a decrease in the beta-cell mass and an increase in beta-cell apoptosis may be the causation of impaired insulin secretion and an overall decrease in beta-cell function.45 Individuals with prediabetes and T2D have been shown to have decreased beta-cell mass compared with their counterparts without diabetes, regardless of weight status.
Hepatic Glucose Production
A secondary cause of increasing blood glucose levels is excessive hepatic glucose production.40 In fasting conditions, glucose is produced by the liver; however, the liver of a person with diabetes will produce substantially more glucose and burden the circulation with extra glucose. This is caused by the excess glucagon levels of people with T2D. Reduced insulin/incretin hormones cannot allow for the normal suppression of glucagon levels in hyperglycemic conditions. In addition, insulin normally causes glucose uptake into the muscle and adipose tissue and a decrease in hepatic glucose production. Insulin is needed to signal the liver to stop glucose production; so, as insulin levels decline, the liver produces more glucose than the body can use and glucose levels in the plasma continue to rise.
Incretin Effect
Incretin hormones in the gastrointestinal tract have been implicated as a factor in the development of T2D. Incretins are naturally occurring hormones that the gut releases throughout the day to facilitate the response of the pancreas and liver to variations in blood glucose.46 The main incretins responsible for this are thought to be glucose-dependent insulinotropic peptide (GIP) and glucagon-like peptide-1 (GLP-1). The activity level of these incretins is increased substantially when food is ingested. When blood glucose rises, both GIP and GLP-1 stimulate beta cells to secrete insulin and the alpha cells of the pancreas to suppress glucagon release from the liver. Patients with prediabetes and T2D are deficient in GLP-1. This deficiency contributes to excess hepatic glucose production, failure to suppress production of hepatic glucagon after meal intake, and increased appetite. These same people also show increases in dipeptidyl peptidase-4 activity (DPP-4) in the fasting state. DPP-4 enzymes break down GLP-1 hormones in the body and this may explain why GLP-1 secretion is impaired after meal intake in those with T2D.40
Increased Renal Glucose Reabsorption
Under normal to mildly hyperglycemic conditions, the kidneys reabsorb almost all glucose in the glomerular filtrate. 47 Glucose is facilitated through SGLT2 and SGLT1 transporters. Experimental data indicate that SGLT2 is expressed on the luminal surface of the epithelial cells of the proximal convoluted tubule, and is a low-capacity, high-affinity glucose transporter. As such, SGLT2 is responsible for the reabsorption of ~90% of filtered glucose in the kidney. SGLT1 is expressed in the late proximal tubule and reabsorbs most of the remaining (~10%) filtered glucose.
In humans, glycosuria occurs when blood glucose reaches a threshold of about 180 mg/dL. Diabetes increases this threshold to somewhere around 200-240 mg/dL, and in this way, exacerbates hyperglycemia. 47 The exact mechanism behind this response is unclear, but most likely includes increased expression of SGLTs. The SGLT2 inhibitor class of medications specifically addresses this increased renal glucose reabsorption noted in people with T2D to treat hyperglycemia.
| Figure 3. Contributing Factors in the Pathophysiology of Type 2 Diabetes.40 |
 |
RISK FACTORS
Family History/Ethnicity
The development of T2D is clearly linked to family history. In fact, individuals with a family history in a first degree relative have a two- to three-fold increased risk of developing T2D.48,49 Additionally, T2D prevalence in the U.S. varies tremendously among groups with individuals of African-American, Native American, and Hispanic origin having greater risk for developing T2D.50
Genetics
The genetics of T2D is quite complex and not completely understood. Most cases of T2D involve many genes contributing small parts to the overall condition. More than 36 genes have been identified as contributing to risks for T2D, but only 10% of the heritability of T2D can be explained.37 For most patients, it is impossible to identify a genetic abnormality and environmental factors are more predominate. Some genes that have been associated with T2D include transcription factor 7-like 2 (TCF7L2), peroxisome proliferator-activated receptor gamma (PPARG), potassium inwardly rectifying channel - subfamily J - member 11 (KCNJ11), the sulfonylurea urea receptor (ABCC8), Calpain 10, glucose transporter 2 (GLUT 2), the glucagon receptor (GCGR), and many others.51 Defects at TCF7L2 impact beta-cell development and function and studies show that carriers of one risk allele have an approximate risk of T2D that is 40% higher than carriers with a protective allele. Additionally, one genetic variant of the PPARG gene causes decreased insulin sensitivity and increases the risk for T2D by several-fold. This gene is thought to be more common in Caucasians. Calpain 10 and ABCC8 variations contribute to decreased insulin secretion and, thus, increase risk for diabetes. Interestingly, most of the genes identified impact insulin secretion and regulation mediated from the pancreas. In contrast, genes that have been linked to insulin resistance, obesity, and other aspects of glucose metabolism are much less common.
Environmental Factors
Obesity, aging, a longer life span, smoking history, and physical inactivity are all examples of environmental factors that can affect the progression of T2D.52 Central or visceral obesity seems to be specifically problematic and a major contributor to insulin resistance. Decreased daily activity related to modern technology and changes in the American diet, including increased fat intake, increased simple sugar intake, and a decrease in dietary fiber intake, have all contributed to the obesity epidemic as well. Even mild obesity can contribute to glucose intolerance. Those of Japanese origins are especially prone to central obesity and, thus, a lower body mass index (BMI) target has been recently suggested for them (23 BMI).2 Smoking has been shown to be especially detrimental to health and increases the risk for diabetes by 30% to 40%, along with the long-term complications risk.53
Medications that may impair glucose tolerance by decreasing beta-cell insulin secretion, increasing glucose production in the liver, or causing insulin resistance are vast. Glucocorticoids, oral contraceptives, beta-blockers, thiazide diuretics, statins, protease inhibitors, atypical antipsychotics, cyclosporine, tacrolimus, and others comprise this list.54 Pharmacists should be especially vigilant to review all medications for patients with diabetes, or those at risk for diabetes, for possible hyperglycemia adverse reactions.
Intrauterine developmental causes have also been implicated in the development of T2D recently. The theory of the thrifty genotype suggests that insulin resistance is both beneficial and detrimental by improving survival during states of caloric deprivation, but leading to negative consequences in states of caloric excess.55 This theory has been hypothesized to occur during early life in the womb if intrauterine growth restriction and low birth weight are caused by malnutrition. Thus, those infants born with low birth weights (less than 3.5 kg) are at greater risk for developing diabetes in adulthood. Conversely, high birth weight is also a risk factor for diabetes (greater than 4 kg).56 It has been shown that prenatal exposure to hyperglycemia can cause higher birth weights and may increase the risk for T2D, regardless of genetic predisposition. Other studies indicate that premature children may also be at greater risk for diabetes.56 More research is needed to confirm these findings. However, it is apparent that prenatal influences may have great determinants for the risk of developing diabetes in the future.
OTHER TYPES OF DIABETES
Idiopathic Type 1 Diabetes (T1D)
Idiopathic T1D is a form of diabetes with no known etiology.2 Patients with this disorder are prone to ketoacidosis and exhibit varying degrees of insulin deficiency, but have no evidence of ß cell autoimmunity. This form of the disease appears to be strongly tied to family inheritance and most of those affected by it are of Asian or African ancestry.
Gestational Diabetes Mellitus (GDM)
GDM is defined by the ADA as diabetes diagnosed in the second or third trimester of pregnancy that was not clearly present before pregnancy. The incidence of gestational diabetes varies among populations and ethnicities; but, it is estimated that of the 6% to 7% of pregnancies affected by diabetes, 90% of them are GDM. The rate of GDM is increasing and this is most likely a result of the increasing number of women with overweight and obesity in their childbearing years.57 Physical activity and a well-balanced diet are key counseling points when discussing how to reduce newborn complications for patients with GDM. In addition, some expectant mothers may have glycemic levels sufficient enough to warrant use of medication. The American Diabetes Association (ADA) recommends insulin as the preferred medication for treating hyperglycemia in GDM.58 While sometimes used clinically, the ADA states that metformin and glyburide should not be used as first-line agents because both drugs cross the placenta to the fetus. Women who are diagnosed with GDM are also at greater risk for subsequent T2D in their lifetime and should be monitored regularly after delivery of the child.
Monogenic Diabetes Syndromes
Monogenic defects that contribute to beta-cell dysfunction include MODY and neonatal diabetes. Together, monogenic diabetes syndromes account for <5% of all cases of diabetes.2
Maturity-onset diabetes of the young (MODY) is a relatively rare form of diabetes that results from a defect in a single gene.2,37 MODY is frequently characterized by the onset of hyperglycemia at an early age and is characterized by impaired insulin secretion with minimal or no defects in insulin action. MODY is inherited in an autosomal dominant fashion with abnormalities in at least 13 genes identified to date.2 People with MODY are usually not overweight and do not present with other risk factors for diabetes. MODY can be treated with oral antihyperglycemic agents (low dose sulfonylureas) and in some cases may not require insulin.
Neonatal diabetes occurs within the first 6 months of life and is quite rare.2 This type of diabetes can be transient or permanent depending on the genetic defect. If it is permanent, treatment options depend on the genetic defect and include sulfonylurea options and/or insulin therapies.
Cystic Fibrosis-Related Diabetes (CFRD)
CFRD is the most common comorbidity for people with cystic fibrosis.2 Partial destruction of the islet mass causes decreased insulin production in this population and nearly 40% to 50% of adults with cystic fibrosis are affected by this condition. These patients are generally treated with insulin.
Posttransplantation Diabetes Mellitus (PTDM)
PTDM denotes the presence/development of diabetes following organ transplantation.2 Use of corticosteroids and immunosuppressive agents contribute to the development of PTDM. Because immunosuppressive agents are required to prevent organ rejection, hyperglycemia management may be required long-term.
SUMMARY
Diabetes is an increasing concern within the U.S., as well as the world. Its remarkable growth rate has reached an epidemic proportion in recent years. Regardless of the etiology, all types of diabetes are associated with the potential for long-term complications. Disappointing data show that hemoglobin A1C values tend to increase by 1% every 2 years, even with the most aggressive interventions.59 Patients with diabetes require repeated intervention and education to maximize treatment success. Pharmacists in clinical roles can be advocates for evidence-based practices to decrease the clinical inertia related to diabetes treatment as well as an important point of contact to patients for medication counseling and adherence assistance. Additionally, future attempts to prevent and/or reverse diabetes are most likely to succeed if they include the most recent advances in the understanding of the complex pathogenesis of the disease. Pharmacists play an important role in communicating medical information to patients about diabetes and need to stay updated on new prevention techniques, treatment devices, and therapies.
| Potential Counseling Tips for Pharmacists |
| Category |
Potential Counseling Tips |
| Prevention |
· Research has shown that the development of type 2 diabetes can be delayed or prevented by eating healthier foods, exercising, or losing weight if necessary.
· Preventing diabetes in you and your loved ones will not only lead to better health, but will also help you avoid hassle (i.e., less visits to the physician and less time in the hospital) and costs (i.e., costs of medical care and lost work).
· You can potentially prevent diabetes complications by maintaining in good control of your diabetes and other risk factors. This is a great point to bring out to your patients. |
| Screening |
· Because symptoms at presentation vary so widely and are often not recognized, screening of high-risk persons is critical. The pharmacist can then offer to screen the patient or refer him/her to the next health fair, during which screenings will be performed at low or no cost.
· Patients diagnosed with type 2 diabetes should also receive screenings for high cholesterol and blood pressure.
· Know how to identify the symptoms of diabetes in your patients. Some common symptoms to watch out for are increased thirst, increased urination, and unexplained weight loss. |
REFERENCES
- Cho NH, Shaw JE, Karuranga S, et al. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract. 2018;138:271-281.
- American Diabetes Association. 2. Classification and diagnosis of diabetes: Standards of Medical Care in Diabetes – 2019. Diabetes Care. 2019;42(Suppl. 1):S13-S28.
- The Diabetes Control and Complications Trial (DCCT) Research Group. The effect of intensive treatment of diabetes on the development and progression of long term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329(14):977-986.
- Knowler WC, Barrett-Connor E, Fowler SE, et al; for the Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med.2002;346(6):393-403.
- Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2017. Atlanta, GA: Centers for Disease Control and Prevention, U.S. Dept of Health and Human Services; 2017.
- Whiting DR, Guariguata L, Weil C, Shaw J. IDF Diabetes atlas: global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res Clin Pract.2011;94(3):311-321.
- Mayer-Davis EJ, Kahkoska AR, Jefferies C, et al. ISPAD Clinical Practice Consensus Guidelines 2018: Definition, epidemiology, and classification of diabetes in children and adolescents. Pediatr Diabetes. 2018;19(Suppl. 27):7-19.
- Duncan GE. Prevalence of diabetes and impaired fasting glucose levels among US adolescents: National Health and Nutrition Examination Survey, 1999-2002. Arch Pediatr Adolesc Med. 2006;160(5):523-528.
- Dabelea D, Bell RA, D'Agostino RB Jr, et al; and the Writing Group for the SEARCH for Diabetes in Youth Study Group. Incidence of diabetes in youth in the United States. 2007;297:2716-2724.
- Banion C, Valentine V. "Type 1 diabetes throughout the life span." In: Mensing CE, Cornell S, Halstenson C. The Art and Science of Diabetes Self-Management Education Desk Reference. 3rd ed. Chicago, IL: American Association of Diabetes Educators (AADE); 2014.
- Silverstein J, Klingensmith G, Copeland K, et al; American Diabetes Association. Care of children and adolescents with type 1 diabetes. Diabetes Care. 2005;28(1):186-212.
- Wolfsdorf J, Glaser N, Sperling MA. Diabetic ketoacidosis in infants, children and adolescents: A consensus statement from the American Diabetes Association. Diabetes Care. 2006;29(5):1150-1159.
- Agus MS, Wolfsdorf JI. Diabetic ketoacidosis in children. Pediatr Clin North Am.2005;52(4):1147-1163.
- Klingensmith GJ, Tamborlane WV, Wood J, et al. Diabetic ketoacidosis at diabetes onset: still an all too common threat in youth. J Pediatr. 2013;162(2):330-334.
- Beisswenger PJ. "Type 1 diabetes." In: Leahy JL, Clark NG, Cefalu WT. Medical Management of Diabetes Mellitus. New York, NY: Marcel Dekker; 2000.
- Rewers A, Chase HP, Mackenzie T, et al. Predictors of acute complications in children with type 1 diabetes. 2002;287(19):2511-2516.
- Chiang JL, Kirkman MS, Laffel LM, et al; and the Type 1 Diabetes Sourcebook Authors. Type 1 diabetes through the life span: a position statement of the American Diabetes Association. Diabetes Care.2014;37(7):2034-2054.
- Steck AK, Barriqa KJ, Emery LM, et al. Secondary attack rate of type 1 diabetes in Colorado families. Diabetes Care. 2005;28(2):296-300.
- Tillil H, Köbberling J. Age-corrected empirical genetic risk estimates for first-degree relatives of IDDM patients. Diabetes. 1987;36(1):93-99.
- Dabelea D, Mayer-Davis EJ, Saydah S, et al; and the SEARCH for Diabetes in Youth Study. Prevalence of type 1 and type 2 diabetes among children and adolescents from 2001 to 2009. 2014;311(17):1778-1786.
- Barrett JC, Clayton DG, Concannon P, et al; and the Type 1 Diabetes Genetics Consortium. Genome-wide association study and meta-analysis find that over 40 loci affect risk of type 1 diabetes. Nat Rev Genet.2009;41(6):703-707.
- Redondo MJ, Eisenbarth GS. Genetic control of autoimmunity in Type 1 diabetes and associated disorders. 2002;45(5):605-622.
- Tisch R, McDevitt H. Insulin dependent diabetes mellitus. 1996;85(3):291-297.
- Erlich H, Valdes AM, Noble J, et al; and the Diabetes Genetics Consortium. HLA DR-DQ haplotypes and genotypes and type 1 diabetes risk: analysis of the type 1 diabetes genetics consortium families. 2008;57(4):1084-1092.
- Polychronakos C, Li Q. Understanding type 1 diabetes through genetics: advances and prospects. Nat Rev Genet.2011:12(11):781-792.
- Atkinson MA, Maclaren NK. Mechanisms of Disease: the pathogenesis of insulin-dependent diabetes mellitus. N Engl J Med.1994;331(21):1428-1436.
- Watkins RA, Evans-Molina C, Blum JS, DiMeglio LA. Established and emerging biomarkers for the prediction of type 1 diabetes: a systematic review. Transl Res.2014;164(2):110-121.
- Simmons K, Michels AW. Lessons from type 1 diabetes for understanding natural history and prevention of autoimmune disease. Rheum Dis Clin North Am.2014;40(4):797-811.
- Rosenbauer J, Herzig P, von Kries R, et al. Temporal, seasonal, and geographic incidence patterns of type 1 diabetes mellitus in children under 5 years of age in Germany.1999;42(9):1055-1059.
- Yang Z, Wang K, Li T, et al. Childhood diabetes in China. Enormous variation by place and ethnic group. Diabetes Care.1998;21(4):525-529.
- Harjutsalo V, Sund R, Knip M, Groop PH. Incidence of type 1 diabetes in Finland. 2013;310(4):427-428.
- Stene LC, Magnus P, Lie RT, et al; Norwegian Childhood Diabetes Study Group. Birth weight and childhood onset type 1 diabetes: population based cohort study.2001;322(7291):889-892.
- Bortell R, Pino SC, Greiner DL, et al. Closing the circle between the bedside and the bench: Toll-like receptors in models of virally induced diabetes. Ann N Y Acad Sci.2008;1150:112-122.
- Bach JF. The effect of infections on susceptibility to autoimmune and allergic diseases. N Engl J Med. 2002;347(12):911-920.
- Knip M, Akerblom HK. Early nutrition and later diabetes risk. Adv Exp Med Biol. 2005;569:142-150.
- Sipetic S, Vlajinac H, Kocev N, et al. Early infant diet and risk of type 1 diabetes mellitus in Belgrade children. 2005;21(4):474-479.
- Bardsley JK, Magee MF. "Pathophysiology of the metabolic disorder." In: Mensing C, Cornell S, Halstenson C. The Art and Science of Diabetes Self-Management Education Desk Reference. 3rd ed. Chicago, IL: American Association of Diabetes Educators (AADE); 2014.
- Vivian EM. "Type 2 diabetes throughout the life span." In: Mensing C, Cornell S, Halstenson C. The Art and Science of Diabetes Self-Management Education Desk Reference. 3rd ed. Chicago, IL: American Association of Diabetes Educators (AADE); 2014
- American Diabetes Association. Type 2 diabetes in children and adolescents (consensus statement). Diabetes Care.2000;23(3)381-389.
- Defronzo RA. Banting Lecture. From the triumvirate to the ominous octet: a new paradigm for the treatment of type 2 diabetes mellitus. Diabetes. 2009;58(4):773-795.
- Bergenstal R. "Natural History of Type 2 Diabetes" diagram. In: Translating Diabetes Medications into Protocol. The Many Faces of Community Health International Diabetes Center (IDC) Web site. http://www.manyfacesconference.org/conference2008/Bergenstal%20Many%20Faces.pdf. Accessed April 14, 2019.
- Leahy JL. "Type 2 diabetes mellitus." In: Leahy JL, Clark NG, Cefalu WT. Medical Management of Diabetes Mellitus. New York, NY: Marcel Dekker; 2000.
- Cefalu WT. "Insulin resistance." In: Leahy JL, Clark NG, Cefalu WT. Medical Management of Diabetes Mellitus. New York, NY: Marcel Dekker; 2000.
- Nichols GA, Hilliar TA, Brown JB. Progression from newly acquired impaired fasting glucose to type 2 diabetes. Diabetes Care.2007;30(2):228-233.
- Butler AE, Janson J, Bonner-Weir S, et al. Beta-cell deficit and increased beta-cell apoptosis in humans with type 2 diabetes. 2003;52(1):102-110.
- Deacon CF. What do we know about the secretion and degradation of incretin hormones? Regul Pept. 2005;128(2):117-124.
- Alicic RZ, Neumiller JJ ,Johnson EJ, et al. Sodium-glucose cotransporter 2 inhibition and diabetic kidney disease. Diabetes. 2019;68(2):248-257.
- Klein BE, Klein R, Moss SE, Cruickshanks KJ. Parental history of diabetes in a population-based study. Diabetes Care. 1996;19(8):827-830.
- Meigs JB, Cupples LA, Wilson PW. Parental transmission of type 2 diabetes: the Framingham Offspring Study. Diabetes. 2000 29(12):2201-2207.
- Carter JS, Pugh JA, Monterrosa A. Non-insulin-dependent diabetes mellitus in minorities in the United States. Ann Intern Med. 1996;125(3):221-232.
- Herder C, Roden M. Genetics of type 2 diabetes: pathophysiologic and clinical relevance. Eur J Clin Invest. 2011;41(6):679-692.
- Sullivan PW, Morrato EH, Ghushchyan V, et al. Obesity, inactivity, and the prevalence of diabetes and diabetes-related cardiovascular comorbidities in the U.S., 2000-2002. Diabetes Care. 2005;28(7):1599-1603.
- S. Department of Health and Human Services. 2014 Surgeon General's Report: The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General.Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention (CDC), National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2014. CDC Web site. http://www.cdc.gov/tobacco/data_statistics/sgr/50th-anniversary/index.htm. Accessed April 14, 2019.
- Luna B, Feinglos MN. Drug induced hyperglycemia.JAMA. 2001;286(16):1945-1948.
- Phillips DI, Barker DJ, Hales CN, et al. Thinness at birth and insulin resistance in adult life. Diabetologia. 1994;37(2):150-154.
- Harder T, Rodekamp E, Schellong K, et al. Birth weight and subsequent risk of type 2 diabetes: a meta-analysis. Am J Epidemiol. 2007;165(8):849-857.
- American College of Obstetricians and Gynecologists. Committee opinion no. 504: Screening and diagnosis of gestational diabetes mellitus: College publications retraction. Obstet Gynecol.2013;122(2 pt 1):405.
- American Diabetes Association. 14. Management of diabetes in pregnancy: Standards of Medical Care in Diabetes – 2019. Diabetes Care. 2019;42(Suppl. 1):S165-S172.
- Fonseca VA. Defining and Characterizing the progression of type 2 diabetes. Diabetes Care.2009;32(suppl 2):S151-S156.
Back to Top