
Expired activity
Please go to the PowerPak
homepage and select a course.
INVASIVE MYCOSES IN HEMATOLOGIC MALIGNANCIES: OPTIMAL MANAGEMENT STRATEGIES
SECTION 1A: INTRODUCTION
Matthew Lunning, DO
Welcome to Invasive Mycoses in Hematologic Malignancies: Optimal Management Strategies. I’m Matthew
Lunning. I'm an assistant professor in the Division of Oncology and Hematology at the University of Nebraska
Medical Center. By training, I am a lymphoma/myeloma transplanter. My co-panelist, Dr. Alison Freifeld, will help
me moderate this session. She is a professor of internal medicine, also at the Fred & Pamela Buffett Cancer Center
at the University of Nebraska Medical Center in Omaha, Nebraska.
So here's the agenda. This is the introduction component, and Dr. Freifeld will present a little bit of background in
invasive fungal infections. We’ll then turn it over to Dr Maertens and Jim Lewis about invasive fungal infections
diagnosis and therapeutics. And we will get started now with the symposium portion with Dr. Freifeld discussing
the epidemiology of invasive fungal infections in hematologic malignancies.
SECTION 1B: EPIDEMIOLOGY OF INVASIVE FUNGAL INFECTIONS IN HEMATOLOGIC MALIGNANCIES
Alison G. Freifeld, MD
Good afternoon, and welcome to the Invasive Fungal Infection Symposium. I'm Alison Freifeld, colleague of Matt
Lunning. We work together on a daily basis at the Fred & Pamela Buffett Cancer Center in Omaha.
So, as you know, infectious complications have improved in terms of management over the last 60 years that
we've been using cytotoxic chemotherapy. It’s really gratifying to see that we've been able to predict and manage – and in many cases, contain – things like cytomegalovirus, and many of the routine bacterial infections. Of course,
now we're faced with the rising incidence of resistance among many infectious pathogens. And today we are
talking specifically about invasive fungal infections or IFI, especially in hematologic malignancies.
And so, what I’d like to do is first orient you to the epidemiology of IFIs in both hematologic malignancies and
transplant. There are a number of opportunities for invasive fungal infections to occur during the course of
treatment for hematologic malignancies.
And for the most part, we're talking about Aspergillus species, which typically account for about 60% of all the IFIs
documented. Which are far greater in number than Candida infections, accounting for about 30%. Then,
occasionally, we see zygomycoses or Fusarium in a small percentage, but they are, as you know, very difficult to
treat.
if we looked to the course of a patient, starting with the AML population, data have shown us from large
population studies performed prior to the advent of the triazoles that we're going to talk about today – that there
was a baseline rate of about 8% to 12% of invasive fungal infections in that population, comprising all of these
genera: Aspergillus, Candida, and Fusarium and the fungi of the Zygomycota phylum.
Interestingly, in the ALL population the rates are a little lower, about 6.5%. In a study performed in Italy in the early
part of this century, looking at about 150 infectious aspergillosis patients in newly diagnosed AML, about 60% were
diagnosed during induction, about 36% during relapse and refractory disease, as you’d expect. So most episodes of
IFI occur during induction for AML. And only about 3% during consolidation cycles.
If we look at the stem-cell transplant population, we know that the vast majority of IFIs (99%) occur in the
allogeneic setting as opposed to the autologous transplant group. In allogeneics, the cumulative incidence is 2 to
8%, in general. There is a very wide variety of cumulative incidence rates, depending on which population studies
are looked at. But a common finding is that 80% of these typically occur within a hundred days of transplant,
during the neutropenic period and also during periods of acute GvHD.
So before we really go through a lot of the data that my colleagues are going to present, we need to kind of review
the definitions of IFI. And these are definitions that were created by the combined efforts of the EORTC and the
Mycoses Study Group in the United States, just to be able to clarify what we're all talking about.
And the proven definition is very easy – because it requires histology, cytology, or culture data from a sterile site.
So nobody would argue with that and I've shown at the right, some lung histology, H&E section demonstrating
those narrow septate hyphae with acute-angle branching and tissue – very characteristic of aspergillosis. That’s
the kind of data that really is required for a proven infection. And it’s unfortunately, the kind of data that we
rarely are able to achieve.
A probable definition was created so that we could capture IFIs from the vast majority of patients where host
factors, clinical criteria, and mycological criteria are required in order to categorize the infection as probable. The
host factors have to be approximate and show severe immunosuppression, neutropenia, recent allogeneic
transplant, corticosteroids, T cell immunosuppression, etc.
The clinical criteria are largely dependent on the CT appearance of what is thought to be characteristic of an
invasive fungal infection, typically a mold. And in this situation, I’ve shown you a large nodular lesion on a CT scan,
that I think most of us in the right setting and the right host would consider likely to be due to an invasive mold
infection.
These mycologic criteria were first delineated in 2002, and then revised in 2008. They were revised to include not
just mold by cytology or direct microscopy or culture in a non-sterile specimen, but also to include the new antigen
testing methods.
Well, these are not necessarily brand new in 2015 – and we’ll hear more about them from Dr. Maertens. But a
positive galactomannan test from serum, BAL, or CSF, or a β-D-glucan test from serum are considered enough
evidence at the mycologic level to designate a probable infection.
So let's turn first to the incidence of IFI in the hematologic malignancy group—that is, the non-transplant
populations. And I've accumulated here several very large studies that were done in the early part of the century
to show you the splay of data in IFIs in the baseline group, meaning those who received either placebo or
fluconazole prophylaxis.
There are 2 retrospective studies and 3 randomized controlled trials. And I think these will provide to us the best
data, in which the control groups had anywhere between a 2% and 8% incidence of IFI, with the application of a
mold-active agent, itraconazole, as prophylaxis in 2 of these studies.
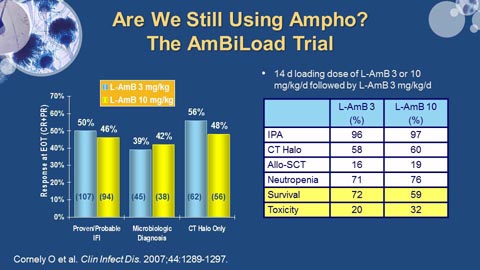
I want to particularly draw your attention to this study in 2007 by Cornely, which really is kind of the basis for most
studies going forward, most information going forward about the azoles and their efficacy for prophylaxis. And in
this large study, many of you may be familiar with – 602 patients with AML were randomized to receive either
fluconazole or itraconazole, which were the standards of care at the time versus posaconazole – in the oral suspension
form, very different from the tablet form that we have today. And they recognized a dramatic decrease from 8%
to 2% in the prophylaxed group with a concomitant decrease in the defined invasive aspergillosis group from 7% to
1%.
And I think this really set the stage for subsequent studies after that. This really has established posaconazole as
the drug of choice for prophylaxis. We can argue a little bit about that in the coming session. But let's just say that
that’s the baseline data.
I also wanted to point out that this study by Gomes was done at a single center, MD Anderson. It’s a retrospective
review of 152 patients with newly diagnosed AML. And they found an actually quite high, sort of outlying
incidence of mold infection in their group. Interestingly, this group found that in patients who are prophylaxed
with the echinocandins, there were more breakthrough infections with mold infections. They also did a lot of
clofarabine treatment with reduced intensity transplants. They ended up having a lot of mold breakthroughs
there, as well, so there were a number of confounders in their population, making definitive interpretation
difficult.
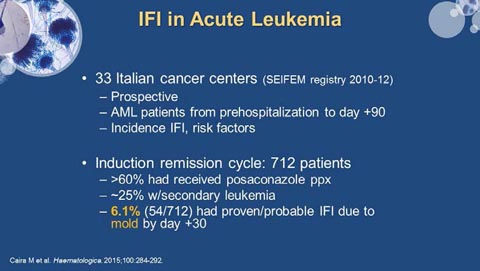 |
So a more contemporary study comes from Italy looking at a registry study from 2010 to 2012, done prospectively
in AML patients who are followed from pre-hospitalization to day +90. They looked at incidence of IFI, as well as
risk factors and found that in 712 patients going through induction remission, about 60% of these patients had
received posaconazole, 25% had a secondary leukemia, and these leukemias are notably difficult to put into
remission. And their overall incidence of proven and probable IFI was 6.1% by day 30. So this is a little bit more
recent data to look at in terms of what the baseline would be.
This is an interesting study because they went on to look at pre- and post-chemotherapy risk factors for IFI,
especially mold infection, in particular.
But they, not surprisingly, found that COPD and ECOG performance status of greater than 2 were linked to proven
and probable mold infections. But they also found that house renovation in the 6 months prior to treatment and a high exposure job, meaning things like farming or working in a floral shop or construction work were also
associated with subsequent IFI due to molds.
This is the most puzzling piece, and that is that having a higher body weight was relatively protective. And by
higher body weight, they meant a BMI of 30, which they really had trouble explaining. So before you reach for the
glazed donuts, I'm not sure how to really interpret that data. But at least, these were not cachectic people
certainly. Post transplant, not surprisingly, they also showed modest association with longer neutropenia
durations, esophagitis, grade 2 or more as being predictive. And then posaconazole prophylaxis, as we've seen
earlier, was relatively protective.
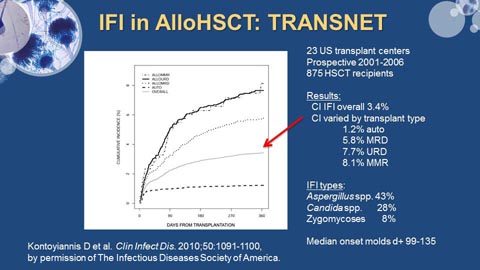 |
In the allogeneic transplant situation, the largest study to date has been from the TRANSNET Group, which was a
consortium of 23 US transplant centers, who prospectively collected data between 2001 and 2006. Again, prior to
the widespread use of triazoles – looking at 875 stem cell transplant recipients. They found overall a 3.4%
incidence of IFI in that group within the first year after transplant. But that, as you'd expect, the incidence varied
by transplant type. And I alluded to this earlier, but autotransplant shown in the dash line at the bottom, 1.2%.
So really this is not an issue, as you well know, of autotransplant patients. But it really varies by what type of
allogeneic transplant is performed, with the unrelated donor and mismatched transplants occurring at rates of
about 8% at 1 year, and 5.8% in those who are matched and related. Again, Aspergillus predominated, accounting
for about 40% of IFIs; Candida representing about a third, not quite; and zygomycoses, 8%.
So again, in a more recent study from Italy, risk factors for IFI after allotransplant. This was a prospective study
amongst 30 Italian centers. Almost 2,000 stem cell recipients, and about 14% received a mold-active agent for
prophylaxis. They found several categories of IFI early in the course before day 40, with a cumulative incidence of 5.1%. And risks were unrelated or cord blood transplant or having a prior IFI or having acute leukemia at
transplant. I think we could have predicted many of these.
And then late IFI, that is after day 40 to day 100 – just a small percentage, not quite 2%. Again related to having
had an unrelated transplant or a cord blood transplant or acute GvHD with concomitant methylprednisolone or its
equivalent. Regarding receipt of a mold-active agent for prophylaxis – and remember, this is in an allotransplant
group, but those who received a mold-active agent had a reduced overall incidence from 9 to 4.6%. Again raising
the question, is that important? In other words, should we be using mold-active agents in the post-transplant
setting? Or is fluconazole enough? And I've listed several of the other risk factors that have emerged, as well,
from other studies.
 |
But I want to go to that question that I just asked. And that is, what about the use of mold-active agents in the
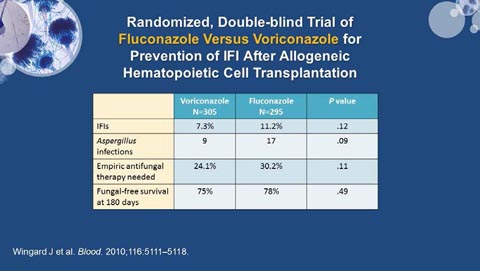
setting of allogeneic stem cell transplant? And here is the classic data that was published by John Wingard in 2010, from a randomized double-blind trial of fluconazole—no activity against invasive molds like Fusarium, etc. versus voriconazole, which does have that anti-mold activity.
For prevention of IFI after allogeneic stem cell transplant, they provided either fluconazole or voriconazole for the
first hundred days after transplant. And in some situations, those who were felt to be at higher risk were able to
continue on their assigned azole therapy, which the hypothesis that if you give people voriconazole, something
that’s a broader spectrum azole, you would decrease the incidence of IFIs. You would presumably decrease the
incidence of Aspergillus infections, have less need for empiric antifungal therapy, and have greater fungal-free
survival. I think that’s sort of an intuitive hypothesis.
The P values and the incidences are shown here. There was no decrease in IFIs. There was a trend toward fewer infections in those who only received fluconazole. There was no difference in terms of empiric
antifungal therapy, and no difference in fungal-free survival. So I think at this stage, most of the transplant centers
in the US and elsewhere use fluconazole primarily for prophylaxis in this setting.
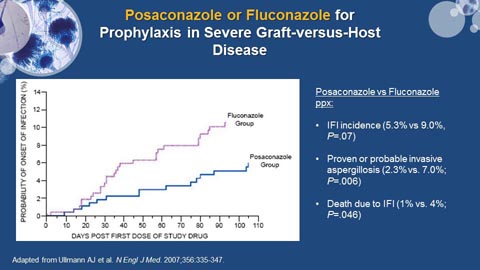 |
I also want to show you another pivotal study for allotransplant patients with GvHD. This was the posaconazole
versus fluconazole study, published by Ullmann in the New England Journal in 2007. And I show it even though it’s
older data; it’s important because it serves as the basis for what we're going to talk about today. And in this study,
patients who had a severe GvHD and were on at least 1 mg/kg of methylprednisolone or equivalent daily were
randomized to receive posaconazole or fluconazole prophylaxis. And as you can see here, in the first 100 days,
those with a greater probability of infection due to invasive fungal infections were in the fluconazole group, with
proven or probable invasive aspergillosis being decreased significantly from 7% to 2.3%, although there was a
trend toward decreased overall IFI. But most importantly, there were mortality benefits seen in this study – 4%
versus 1%, with the benefit seen due to posaconazole.
So talking about mortality, if we look at some of the older data, this is where we really I think all of us become very
nervous about invasive fungal infections. And that is the fact that they tend to be lethal in our patients.
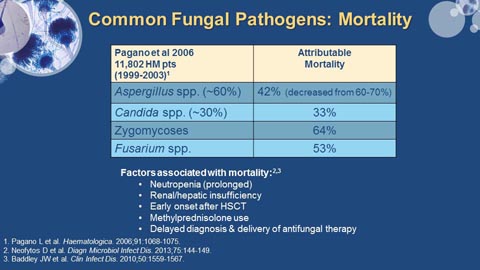 |
These are data again pre-triazoles with having an attributable mortality of about 40%, down from the
1990s when it was more in the 60 to 70% range. And there are some data to suggest that it’s decreased even
further in the current era, certainly. For Candida species, the mortality rate is about 33%; zygomycoses and Fusarium are the ones that we really have most concern about because of the associated very high levels of
mortality. A number of factors are associated with mortality. And so, in our patients with prolonged neutropenia,
some renal or hepatic insufficiency, methylprednisolone use and the idea that delayed diagnosis and delivery of
antifungal therapy contribute to mortality, are all factors that promote the use of voriconazole and posaconazole,
and perhaps isavuconazole – as we’ll see. These are the factors that really have all of us so concerned that we end
up prescribing those agents frequently.
And I want to share with you this kind of apocalyptic quote from some folks who wrote in Clinical Infectious
Diseases about a year ago, including John Wingard:
That’s what we're here today to talk about. How can we better use these drugs to improve the outcomes of IFI in
our hematologic malignancy and allotransplant patients? Specifically, what new diagnostic methods will be available
to us to more accurately and rapidly define IFIs? And how should we use the new triazole drugs so that we avoid
spiraling empiricism? What are the advantages and problems associated with each of the ones that are available?
And finally, is azole resistance really an emerging problem? Is it something that we have to be concerned about in
our patient population?
And so with that, I'm going to turn it over to Dr. Maertens and Dr. Lewis to start answering some of these
questions for you.
SECTION 2: IFI DIAGNOSTICS
Johan Maertens, MD, PhD
Although I'm a hematologist by training and a transplant physician, I've been asked to talk about the currently
available and emerging tools that we have for diagnosing invasive fungal infections in hematology patients. And I
will also address the question of how can we incorporate and how can we integrate these new diagnostic tools
into our diagnostic and therapeutic algorithms.
 |
We’ll talk about fungal diagnostics, what is currently available. I will not discuss radiology, although radiology has
been a key element or has become a key element for diagnosing invasive mold infections. But I will only focus here
on what's available from the mycology or the microbiology lab. And in the interest of time, we will focus on mold
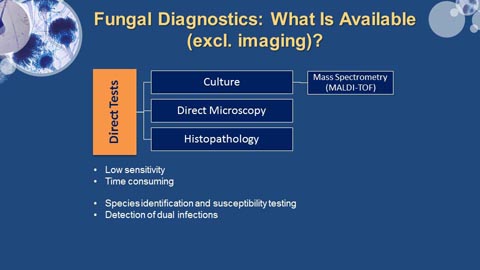
infections and not on yeast infections. So, first of all, we have a number of direct tests or conventional tests. And
these are histopathology, direct microscopy, and culture. Now histopathology has always been one of the key
elements and has always been the gold standard for making the diagnosis of invasive mold infections, also in
hematology patients.
And as already mentioned by Alison in her talk, that has been acknowledged by the EORTC/MSG definitions, where
you see that histopathology is really the tool that we use to make a diagnosis of proven fungal infection. But you
also know that both in clinical practice and in clinical studies, we don’t have that many patients with proven
disease, most of them have probable disease. And then we have culture and direct microscopy. Direct microscopy,
often by the use of optical brighteners, such as Calcofluor.
Now there seems to be some problem with culture. Culture is taken from normal, sterile sites. First of all, culture
has a low sensitivity. This is certainly true for blood cultures, if you talk about invasive mold infections. Usually our
blood cultures are negative, although there are few notable exceptions, like Fusarium and others. But, if we talk
about invasive aspergillosis, in 99% of your cases, blood cultures will certainly be negative. So there is low
sensitivity in hematology population, sensitivity is at best around 30% to 50%. And also the predictive value of a
positive culture depends on the underlying condition of the patient. Another problem with culture is that it is time-consuming. These fungal pathogens grow slowly in the different media that we use. And it takes time to identify
these fungal pathogens.
However, there are also a number of advantages. If you have a positive culture, you can do susceptibility testing.
And this is important in the context of growing resistance or emerging resistance, especially azole resistance. And,
often, culture is the only way to detect multiple fungal infections in a single patient.
Now over the last couple of decades, I have to say, we have seen an increase in the number of nonculture-based
diagnostic tools. Among these indirect tests, some focus on mold infections, others more on yeast infections.
And we have, for instance, galactomannan detection that has become available now. We can look for anti-mannan
for detecting invasive Candida spp. infections. There is a T2 assay that is available in this country as well as 1-3 β-D-glucan, which is more of a panfungal assay. We’ll discuss more about that later. As already mentioned, PCR may
be available – a panfungal PCR or a species-specific PCR. And then there are the new kids on the block, the lateral
flow assays, both for detection of Aspergillus infection, but also other non-Aspergillus mold infections.
As you can see, the list is not complete. You do not see tests for cryptococcal infections on the slide. And also,
important for this country, we will not discuss tests for the endemic mycoses. So again, we will focus here mainly
on the mold infections.
We will discuss what can be routinely available in many centers, that is detection for galactomannan, detection for
1,3-β-D-glucan, and PCR.
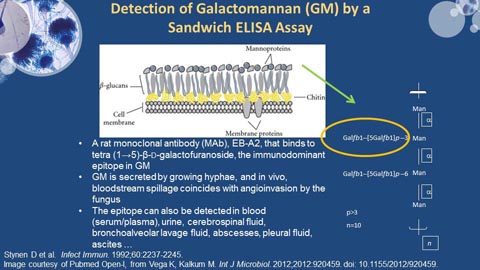 |
Now let's start with galactomannan. If you look at the composition of a fungal cell, first of all you have the fungal
cell membrane, which is composed of a bilayer of phospholipids. And on top of that, there is a fungal cell wall.
And that fungal cell wall has different layers of molecules, be it mannoproteins, glucan, and chitin. Now these
mannoproteins are really consistent of different manno residues held together, and they have different side
chains. The test that we use to detect galactomannan is a commercially available test by Bio-Rad Laboratories. It’s
called the Platelia Assay. And it uses a monoclonal antibody, that’s a rat monoclonal antibody, EB-A2, that binds to
the immunodominant epitope in galactomannan, and that’s basically the side chain. Here you can see the
galactofuranoside chain. Now this side chain is not specific for galactomannan. You will find it also in other
different mannoproteins. So basically what you detect with these tests is not really galactomannan, but
macromolecules containing galactofuranoside as a side chain.
We know that galactomannan is secreted only by growing hyphae. It’s not secreted by resting conidia, only by
growing hyphae. And so, galactomannan is really released into the circulation when the fungus becomes invasive.
The epitope can be found on many different body fluids. Usually we use blood samples, be it serum or plasma
samples, for testing for galactomannan. But it can also be performed on urine. It can be performed on
cerebrospinal fluids. It can also be performed on BAL fluids, abscesses, pleural fluid, etc. So basically any body fluid
can be tested for the presence of galactomannan.
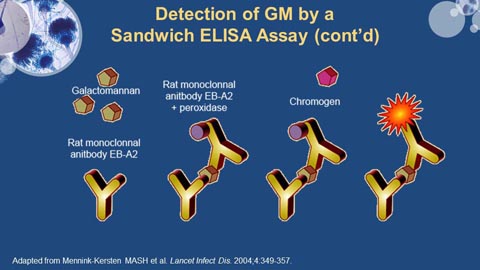 |
Now this is how the test works. It’s basically a sandwich ELISA. You have a microplate that is coated by the rat
monoclonal antibody. And that is used as a capture antibody. If you add a clinical specimen, and if there is
galactomannan present in that specimen, galactomannan will bind to the monoclonal antibody. And we use that
same antibody as a detector antibody. So now the galactomannan is really sandwiched in between the two
monoclonal antibodies. And then we add a chromogenic substrate, and then the test can be read by optical
reader.
What the test gives you is a ratio. So it doesn’t give you the actual amount of galactomannan, but it gives you a
ratio. And this is calculated by dividing the optical density of the patient sample by the mean optical density of a
control sample that is provided by the manufacturer. And so, it gives you an optical density index.
What do we know about the specificity of the galactomannan assay? Well, it’s rather specific for Aspergillus spp.
But there is some cross-reactivity. Patients having invasive Fusarium spp. infections, for instance, may be
galactomannan positive. The same is true for Acremonium and for Histoplasma spp. We don’t have Histoplasma in
Europe, but I know that you see it in this country.
So you have to take that into account, that patients with Histoplasma infection can be GM positive. And also the
patient infected with Alternaria and Penicillium spp. can be GM positive, although Penicillium is usually considered
a contaminant coming from the lab, and not really a human pathogen. And there are fewer exceptions listed over
here.
Usually GM is negative when you have a patient with a Mucorales infection. I say usually because we've seen a
number of patients that were, indeed, galactomannan-positive. And the difficulty here is to see or to assess
whether this is cross-reactivity between Mucorales, or whether these patients really have dual infection –
Mucorales with Aspergillus. The tests will always be negative in case of invasive Candida spp. infections, invasive
cryptococcal infections, or pneumocystis infections.
Now before you start using this test or before you start ordering the test, you have to know that the performance
of the assay is influenced by a number of biological and epidemiological factors. And without going into too much
detail, not looking at all the elements here listed, we list some of the biological factors that clearly play a role in the
performance of the GM test is the site of infection.
If you have an encapsulated infection, like an abscess, then there may be no release of galactomannan in the
circulation. So you may have what is called a false-negative assay, even with a patient with documented infection. Clearly there is an impact of exposure to antifungal agents. And I have to say, an exposure to
mold-active antifungal agents. Many of them are mold-active azoles, but also the mold-active polyenes – and even
the echinocandins. If there is exposure, be it prophylactically or empirically, that will decrease the sensitivity of
the assay.
And you also have to look at the underlying condition. The performance of this test is best in severely neutropenic
patients. It performs less well in the non-neutropenic hematology patients. And it performs poorly in the non-hematology population. So if you use this test in solid organ transplant recipients, in HIV patients, in ICU patients,
sensitivity will be poor. However, if you focus on the prolonged neutropenic hematology patients, then the
sensitivity is around 80 to 90%. And there are a number of epidemiological factors that play a role, such as your
sampling strategy. Do you ask for the test only once a week? Or do you ask for it twice or three times a week?
That will have a major impact. Your underlying prevalence of invasive fungal disease, and of course, the cutoff that
you use for positivity will have an impact on sensitivity and specificity of the test.
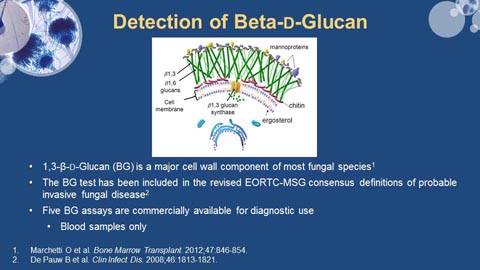 |
Looking at β-D-glucan, as already mentioned by Alison, 1,3-β-D-glucan has been included in the revised EORTC-MSG
Consensus definitions, as well as the microbiological criteria for diagnosing probable invasive fungal disease. And it
is a major cellular component of most fungal species, not of all fungal species – and I’ll come back to the specificity
in a minute.
There are a number of different commercially available assays that can be used. We normally detect 1,3-β-D-glucan using blood samples. It can also be performed on cerebrospinal fluids. But you have to remember that, for
instance, a BAL sample is not suitable for this assay.
Now different tests are commercially available. However, if you look in Europe and in the US, only the Fungitell
test, which was formally called the Glucatell test, and is manufactured by Associates of Cape Cod, is now approved
by the FDA and is also available in Europe.
All the tests, such as the Fungitell-G, the Wako test, and the Maruha test are mainly – not to say exclusively— used
in Japan. They are not available in this country, nor in Europe. Importantly, if you read the literature on this test, you have to know that a cutoff that is used to define a positive assay is different for all these different assays. And
it’s around 60 to 80 pg/mL for the Fungitell assay, and significantly lower for the Japanese assays.
Now this is looking at the specificity with 1,3-β-D-glucan assay. You will detect Aspergillus cases, Candida cases, but
a lot of other fungal pathogens will be detected, as well, including Fusarium, Trichosporon, Acremonium spp., and
all these listed here on the slide. Also, Pneumocystis jiroveci will be picked up by this panfungal assay. And it’s
actually a very nice test to make a diagnosis or to improve the diagnosis for Pneumocystis jiroveci pneumonia.
The test is usually negative for cryptococcal infections. In the early days, we said that infections with Cryptococcus spp. always yielded negative 1,3-β-D-glucan results. Now we've seen a number of cases that tested positive. So
that’s why I said it’s usually negative. And you will not pick up infections caused by Zygomycetes with this test.
Now, for both the β-D-glucan assay and the galactomannan assay, there are a number of false-positive assays –
false-positive, but also false-negative assays. I've listed the reasons here.
The use of some β-lactam antibiotics, such as piperacillin/tazobactam or amoxicillin/clavulanic acid, can result in
false-positive galactomannan assays, as well as false-positive β-D-glucan assays. So, you have to remember that if
you use BAL fluid, and if it is very sticky, and you add a mucolytic agent before you use it in the lab, some of these
mucolytic agents can result in false-negative galactomannan assays.
Now only one word about PCR. You have seen on the slide presented by Alison regarding the EORTC-MSG
definitions, that PCR is still not added to one of the microbiological criteria. And that’s because PCR is really not
standardized. Many of us use PCR. There are a number of commercially available PCRs for detecting Candida, for
detecting Aspergillus spp. They are not really popular, at least not in Europe. And many of us use in-house
developed PCRs, but as already mentioned, they are not standardized. And as such, they have not been included
as microbiological criteria.
However, there is a great initiative, at least in Europe. But there is collaboration also with centers in the United
States and in Australia. It’s called the Europe Aspergillus PCR Initiative. That was launched in 2006 under the
umbrella of the International Society of Human and Animal Mycology. And the aim of that initiative is really trying
to standardize the whole procedure of PCR.
And then finally, there is the lateral flow device, which is really a point-of-care test if you use BAL samples. It’s not
a point-of-care test if you use serum samples or plasma samples because there is a pre-heating test that needs to
be performed in the lab. But if you use BAL samples, it really is a point-of-care test that can be done at the bedside.
And it takes about 15 minutes to have a positive or a negative answer.
This test also uses a monoclonal antibody. In this case a murine monoclonal antibody, different from the rat
monoclonal antibody that is used in the galactomannan assay, recognizing a constitutive glycoprotein antigen.
That antigen is secreted during active growth of the hyphae, so it’s not secreted by resting conidia. And as you can
see, it displays superior specificity to the rat monoclonal antibody that is used in the galactomannan assay. And
this test has been developed as a rapid, and certainly user-friendly, diagnostic test.
Here you see some aspects of the specificity. So this is what the assay looks like. And here we've tested 5
different fungal pathogens. This is the assay that was specific for Aspergillus fumigatus. And if the test is positive,
then you see a second band appearing in the assay.
Now the question is how can all these diagnostic tools help us in our clinical practice?
These assays can help us in different ways. They can help us to exclude the diagnosis of invasive fungal disease.
And if you want to use the tests for excluding the diagnosis of invasive fungal disease, you certainly rely on the
negative predictive value of these assays. And you use the negative predictive value either to stop the antifungal
treatment that was started empirically or prophylactically, or to withhold antifungal therapy. Most of the time we
use the assays in this way in our clinical practice.
The assays can also help us to support the diagnosis of invasive fungal disease and this is the way we use the assay
mostly in clinical studies. To support the diagnosis, we rely on the positive predictive value, either to ask for
additional diagnostics—for instance, to ask for a CT scan, or to start early antifungal therapy. And these assays can
help us to predict outcome. And in that case, we rely on the baseline values or we look at the kinetics of the assay
to choose or to modify our antifungal therapy.
Now there are a number of conditions that we have to take into account. And the first one and probably the most
important one is that for a given sensitivity and specificity of the assay, the test performance is mainly driven by
the pre-test prevalence of the target condition. And this is a common theme, and we’ll come back later when I talk
about prophylaxis.
We should also look at the importance of antifungal prophylaxis—again, something I will discuss within a minute.
There is the importance of the strategy of using these assays in a surveillance strategy or for early diagnosis. The
importance of the sample that we are going to use, a serum sample or plasma sample, or a BAL fluid. And the
number of samples that we use will have importance, as well.
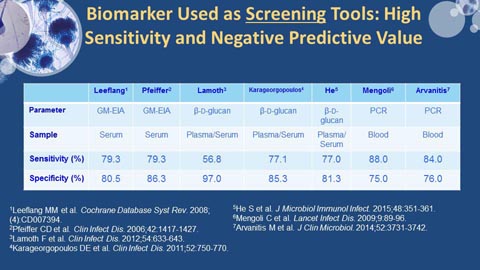 |
So if you use these biomarkers as screening tools—again we rely on the negative predictive value. So you are
looking for tests with a high sensitivity. You don’t want to have false negative assays. Now this is looking at a
number of different meta-analyses that have evaluated performance of the galactomannan assay, the β-D-glucan
assay, and PCR. And you see that for the galactomannan, the sensitivity is around 80% in meta-analysis. For PCR,
it’s around 85%. It’s important to note that we have a high sensitivity, despite the fact that this is not the
standardized assay. And if you look at β-D-glucan, it’s somewhat low. It’s around 70%.
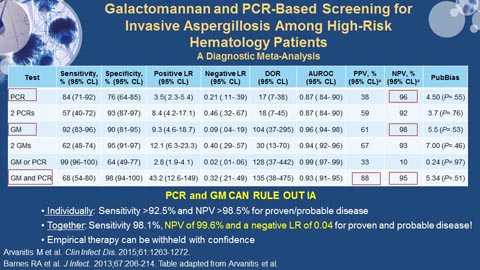 |
However, if we start combining these assays, then clearly you have different results. This is again a meta-analysis
looking at GM and PCR as used as screening tools in high-risk hematology patients. PCR alone has a negative
predictive value of around 96%. For GM, it’s 98%. If we start combining GM and PCR as screening tools, the
negative predictive value is 95%. But as you can see, you clearly increase the positive predictive value up to 88%.
Now these are data taken from meta-analyses. If you look at probably the most important study that has been
done, it was published by Rosemary Barnes in the Journal of Infection a couple of years ago. In that study, they
looked at high-risk hematology patients. These patients were screened weekly for galactomannan and PCR, twice
weekly. And the results of the study are that if you look at these tests individually, the sensitivity and the negative
predictive value are OK. But if you start combining these tests, when you take the results together, GM and PCR,
then you have a negative predictive value of almost 100% with a very good negative likelihood ratio. Clearly,
saying that you can rely on the negative predictive value of this combination to withhold empirical antifungal
therapy.
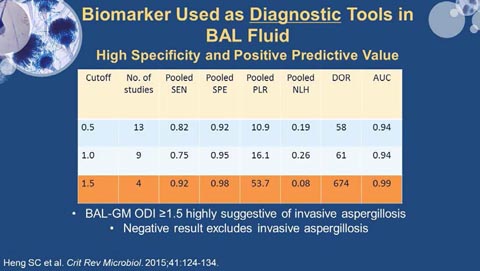 |
Now we can also use these biomarkers as a diagnostic tool. And if you use them as diagnostic tools, they are
mostly performed on BAL fluid. And in that case, you want to have a high positive predictive value. So you're
looking for a test with a high specificity. You want to be sure that a positive test result really means that you have
invasive aspergillosis.
Again looking at different meta-analyses here – and here, the question is what is the cutoff that you are going to
use? Is it 0.5? Is it 1.0 or 1.5? And if you look at the meta-analysis, 1.5 seems to be the most appropriate cutoff,
resulting in a high diagnostic odds ratio of 674. So the conclusion of this meta-analysis was that a BAL
galactomannan optical density index of 1.5 or higher is highly suggestive of invasive aspergillosis, whereas a
negative result virtually always excludes invasive aspergillosis.
So if you use an assay, you have to know that the same assay – that maybe you have to use different thresholds.
Clearly if you use galactomannan for screening purposes, your threshold will be 0.5. If you use it for diagnostic
purposes, your threshold will be 1.5.
One final word about antifungal prophylaxis. Kieren Marr clearly showed in a study published in 2005, that if you
use mold-active agents— azoles, polyenes, and even echinocandins—you decrease the sensitivity of the
galactomannan assay. And the same is true for β-D-glucan and probably also true for PCR. And why is that? Well
first of all, because mold-active agents decrease the baseline incidence, and so they will also decrease your
positive predictive value.
Now one of the questions is can you still rely on serum galactomannan if you give mold-active agents to your
patients? And we just heard from Alison that many of us use posaconazole prophylaxis now. So can you still rely
on serum galactomannan in posaconazole prophylaxed patients?
Well, yes you can. But then you have to use it not as a screening tool, but as a diagnostic tool when you have a
high suspicion of invasive fungal disease. And that’s very nicely shown by a recent study published by Rafael
Duarte, a study from Spain looking at the performance of serum galactomannan in high-risk patients receiving
mainly posaconazole or voriconazole.
If you use it as a screening tool in these patients, as already mentioned, the incidence of invasive aspergillosis is
going to be 2% or lower. You still have a high negative predictive value, but the positive predictive value is only
12%. However, if you have a high suspicion of invasive fungal infection—so a breakthrough fungal infection in a
patient on mold-active azole, then you use it as a diagnostic tool—your baseline incidence then is going to be
much higher; it’s around 50%. And then your positive predictive value rises from 12% to 90%. So it can still be
used—not as a screening assay, but as a diagnostic tool.
So finally we have to try to incorporate these new diagnostic tools or these biomarkers into our antifungal
management strategies. We know that we can give an antifungal prophylactically or empirically. Empirically really
means that you have a fever-driven approach and that you give it to your patients with unresponsive fever.
Also we have directed treatment if you have proven probability cases. But now with the new treatment
approaches, we start relying on these new diagnostic tools, we incorporate them and we may have more
diagnostic-driven approaches where we decide to start an antifungal agent on the basis of a positive biomarker, or
on the basis of a positive biomarker in combination with non-typical pulmonary infiltrates seen on a chest CT scan
or on a standard radiology.
SECTION 3: IFI THERAPEUTICS
James S. Lewis, II, PharmD
One of the things that has gotten really interesting is that any time I wade into the oncology area—because I'm
kind of an ID person normally—I get serious drug envy. And as a pharmacist, you can kind of see where this comes
from. I get drug envy very easily. I want to tell you guys—I got off the plane last night, went down to baggage
claim. I walk out to baggage claim, there is a sign there for a TKI. I drive down the highway, there are two
billboards on the way here for a TKI. You guys are getting new drugs weekly.
We in the ID world, we're lucky if we get a new drug once every year or two. And so, we're still going to be talking
about data with drugs that’s a few years old here, and that’s probably mind blowing for you guys in the oncology
world. We're still talking about voriconazole from 2002.
This is the FDA indication list for the antifungal agents that we currently have available on the market. And I note
the key phrase here: FDA approved. This is not how they're necessarily used clinically. But this is what they are
approved for by the agency. And what you notice really quickly here is that there are some marked differences
with regards to what these agents are actually approved for. We know at this point, as it’s already been shown a
little bit, voriconazole has prophylaxis data. But it’s in no way, shape, or form indicated for that by the FDA.
The other thing to know about voriconazole now—and one of the reasons that this is going to be important is—
insurance companies. Voriconazole is now generic in the United States. And what that has done to your price is
roughly drive it down by about 75%. So now voriconazole is way cheaper than the other azoles that you see up
here on this slide. And you'll see why that’s important as we move forward a little bit.
Posaconazole has only got prophylaxis data. You'll notice you've not seen treatment data up on this slide really
anywhere. There's a little bit of retrospective treatment data. But again, this is with the oral suspension. The FDA
in the package insert says that the tablets are the preferred formulation. When does the agency do that? Never,
okay. So one of the things that you need to realize is that a lot of the data that you're seeing up there with
posaconazole is with an oral suspension formulation, that it had to be the third Tuesday of the month after 4 pm to
get reliable absorption. That’s how dodgy this stuff was. So we have really good data, even with an inferior
product. And we're going to come back again to the different formulations with posaconazole.
That brings us to the new kid on the block – isavuconazole. But with isavuconazole, what you'll notice really
quickly is there's no prophylaxis data yet. But the spectrums of these agents are so darned similar, guys, let me tell
you, I really think that pretty much these drugs can be used for one another in different places.
And so, what you're going to see, I think going forward, is going to be largely driven by financial implications:
voriconazole being generic, being a big one. These two (isavuconazole and posaconazole) are going to be branded
for a while. And so, I think you're going to see a bit of a price dogfight potentially break out between the two of
them.
Alright, so what about amphotericin B? We're talking a whole lot about azoles up here and on the previous slide.
Why are we spending so much time on azoles? Well again, coming back to ancient data circa 2002, I just want to
remind you really quick that voriconazole took amphotericin B out and kicked it around the block for invasive
aspergillosis.
So basically we woke up on Thursday morning before the New England Journal of Medicine was published. And if I
walked up behind you in the hall of your medical center and said invasive aspergillosis, you would have
immediately said AmB. That’s what you would have done. That night, we went to bed after the publication of this
data and the answer switched immediately to voriconazole. The interesting thing was how fast the change
occurred. It says how much all of you in this room hated AmB. Because I have never seen uptake of clinical data
so quickly in my life. Our hematologist ran screaming from the room with regards to AmB. And there was a party
now that they had something else to use for invasive aspergillosis. So we don’t talk a whole lot about AmB
because voriconazole flat out whooped it, to use a term that we would use in Texas a lot.
 |
But what about liposomal amphotericin B? It’s still out there. It’s still the broadest spectrum game in town. And
we know it’s better tolerated than the old school, which should be put in a box and dropped in the middle of the
ocean. So are we still using it? Yes, we are—especially in people who can't tolerate the newer generation azoles,
or God forbid, have breakthrough infections while on one of these newer azoles. And we're not supposed to do
this, but we all do it. When you look at the comparison of response numbers across the different groups here,
these numbers, as far as response rates go for liposomal amphotericin B, look very similar to voriconazole.
We've not seen head-to-head data between liposomal AmB and any of the current generation of azoles out there.
But these response rates pretty much look in line. So we do still use some liposomal AmB, but more so in an
intolerance or salvage role than probably anything else.
What about echinocandins? We all absolutely love echinocandins. And the reason for that is that they're so darn
well tolerated. From a pharmacist's standpoint, the lack of drug interactions, these drugs are almost boring
sometimes. I mean, they don’t quite give me enough to do as a pharmacist. And so, the echinocandins are really awesome, but the downside of them is the spectrum is atrocious. They get Candida and they get Aspergillus spp.,
and that’s about it.
So they're being used a lot more by you guys for prophylaxis in the intense AML induction chemotherapy setting,
in order to get away from some of the drug interactions with these azoles. And guys, that’s really, as you're well
aware, the major problems with the azoles—we're seeing a lot more echinocandin use pop up.
The slide shows data out of MD Anderson that looked at people who are receiving induction chemotherapy. And
what they saw was they got a lot more breakthrough fungal infections when they got an echinocandin than they
did with one of the newer generation azoles. Now when you really drill down on this data, one of the things that's
very interesting is that a lot of the breakthrough data, especially on the echinocandin side, was yeast based, which
really surprised me. I expected it to be more driven by mold breakthrough. But this difference is largely driven by
a lot of yeast breakthrough. So I think that’s something to kind of think about. And again, as was mentioned
previously, this is single center data. So we need to see a little bit more of this. But this really kind of gives me a
little bit of reason for concern. And I’ll tell you, our group in Oregon, we really try to keep the new generation
azoles out there as much as we can in this situation.
 |
So when you're talking about what you want to see from a perfect antifungal agent, you've got a long shopping list
here. And the problem is that when you go through the shopping list you realize very quickly, we don’t have the
perfect antifungal available to us.
Each of the three classes, the polyenes, the echinocandins, and the azoles, all have significant challenges when you
look at this wish list on this slide. And so, really we're in an area where we're having to kind of give-and-take a little
bit with regards to the strengths and weaknesses of each of the compounds we have available to us.
 |
So with that being said, let's talk a little bit about the azoles. And we're going to spend the bulk of our time for the
remainder here talking about azole therapy. Now LFTs drive us all nuts. I think everybody in here has seen the
person who you started on whatever “aconazole,” and then a couple of days later their LFTs start to move. But the
problem is that you guys specialize in using drugs that cause LFT abnormalities. And then you do things to these
patients that cause this lovely disease state called graft-versus-host disease, which I've seen also do some very fun
things to LFTs. So it’s really kind of a multifactorial problem. But we know that within the class, all of these azoles
do it. And it’s not necessarily dose related. And that’s really beautifully and best laid out in the fluconazole
package insert.
The million-dollar question is here in bullet 3. What's the cross reactivity? We don’t know. And so I think it is
certainly worthwhile if someone’s LFTs are moving—especially this means you, voriconazole—to try a different
azole and see if you can back down the LFTs a little bit. And when and where do you discontinue this? Again, it’s
kind of a pain threshold issue because there's really no clear guidance out there as to at what elevation of LFTs
should we be thinking about moving to the potentially nephrotoxic LAmB, or to the much more narrow-spectrum
echinocandins? So it really does become a very, very challenging dance to do. And we really think voriconazole is
probably the worst of the bunch with regards to LFT abnormalities. But again, the new formulation of
posaconazole—I would argue that a lot of the reason that we never saw LFT abnormalities with the oral
suspension was because of variable absorption. You're not going to see LFT abnormalities with an undetectable
posaconazole level when there's no drug there. So I think we're about to learn a lot more with the new tablet and
IV formulations of posaconazole about what the true incidence of LFT abnormalities with posaconazole really is.
And we're really going to get a good snapshot here really quick with the isavuconazole versus voriconazole data to
look at how those two stack up head-to-head.
 |
This is a big moment in my life. I grew up as a Star Wars geek. So imagine my pure excitement when several years
ago I walked into ICAAC and saw two of my favorite things in the same place—fungal infections and Star Wars.
Sitting in the middle of the poster at ICAAC is Chewbacca. And the reason that Chewbacca was sitting in the
middle of the poster: this was a case series out of the NIH, talking about hallucinations due to voriconazole.
The paper, which was later published, and the poster that really did a nice job of laying this out, talked about a
gentleman at the NIH medical branch who was receiving voriconazole. The medical team walks in and he’s like—
guys, there's something I need to tell you. At least this is how I pictured this conversation going. There's
something I need to tell you. Chewbacca is on the ceiling. I know Chewbacca is not on the ceiling; he’s not really
there. But Chewbacca is on the ceiling. And this is really one of the issues with voriconazole. We've learned over
time at these higher serum concentrations, especially over about 5.5 mcg/mL, patients start to hallucinate.
We had a guy at UT San Antonio thank us for the lovely artwork at the foot of his bed and tell us how the artwork
changed every day and wanted to know if he was going to be charged for that, by the way. But there was no
artwork at the foot of his bed. His voriconazole level was 9 mcg/mL. This is the kind of stuff that we have seen.
We've also seen an increasing discussion of skin cancer, fluoride problems, LFT abnormalities, and—the always
awesome—erratic pharmacokinetics that you see with voriconazole. So let's talk a little bit more about the
voriconazole tolerability issue.
This skin cancer issue is bothering me more and more the more I look at this. And really, it appears to be dose and
duration dependent. And what they think – although they're not totally sure – is that it may be driven by the
voriconazole main metabolite, which is voriconazole N-oxide. And the issue I think is that a lot of this data has
been in the dermatologic literature. Some of it has been in the oncology literature. But it’s not all been focused in
an area where a lot of ID and oncology people are necessarily seeing it all the time.
The other thing that we have had to deal with a lot more is this fluoride issue. We learned a lot with the Exserohilum outbreak after the contaminated steroids out of Boston, where they had shot steroids full of fungus
into people’s central nervous system. We learned a lot about high-dose voriconazole over the long term. And one
of the things that we saw is with this trifluorinated structure, that you were getting fluoride serum levels in
patients that were considerably higher than you would have liked. This was associated with a lot of bone pain and
a lot of periostitis, especially in the ulna and in the ribs.
So we've got skin cancer issues. We've now got some fluoride issues. And we certainly have the hallucination stuff
that we talked about earlier. One of the things also that came out was that there's also a lot of alopecia that
occurred in the patients who were getting higher doses of voriconazole during the Exserohilum outbreak. I want
you to stop for a minute and think about Chewbacca with a little alopecia.
Then finally, as if this isn't getting complicated enough, Pascual and colleagues come out a couple of years ago and
said everything that you know about the bioavailability of voriconazole is wrong.
When voriconazole came out in 2002, one of the strengths of the compound was that it was supposed to have
100% oral bioavailability. But I think as increasingly a lot of us have used this drug, we've realized that it’s not one-to-one. And Pascual was really the group that came out and clearly showed us that the bioavailability, especially in
sick oncologic patients, is probably in the 60 to 80% range. And so that bioavailability difference makes the dosing
again a little bit dicey. And we haven’t even gotten in to all of the P-450 issues with regards to voriconazole yet.
Look at this study if you've not looked at this before because, the bioavailability is not as good as many people
think. And that bioavailability issue, especially when you're doing therapeutic drug monitoring, really comes back
to get you.
 |
Now posaconazole, I want to say a couple of things about posaconazole. First – thank you. The IV and the tablets
are awesome. It is so nice to have a drug that finally gets in, that you don’t have to mix it with olive oil, orange
juice, and stand the patient on their head in order to get them to absorb it.
The new tablets are flat out awesome. Albeit a little bit big for some patients. And the IV is also awesome, but it
did come with cyclodextrin – but beggars can't be choosers, right? Now the major problem with posaconazole at
this point in time is that it’s costly compared to voriconazole (which has become generic): $155 a day for tablets,
or $500 a day for IV. By comparison, you start talking about voriconazole being at about $40 a day, the IV is up
around $100 a day. You're talking about considerably more expensive when it comes to the posaconazole
formulations that are out there.
Also, there have been an increasing number of reports of dose confusion. Realize with posaconazole that the
tablets and the IV are dosed 300 mg once a day. Not the 200 mg 3 to 4 times a day that you guys are used to with
the old oral suspension. As a matter of fact, the package insert for posaconazole was re-updated to kind of remind
you of that fact. And there have been a couple of case reports. One in a kid where the oral suspension dosing was
given using the tablets and you got crazy high levels and some toxicity. So I think this dose confusion thing with
posaconazole is really something you want to be aware of and remember that it’s once a day now with the tablets
and the IV formulation.
 |
The issue with isavuconazole at this point in time is that we don’t know what we don’t know. If you go backwards
about 15 years ago and look at the development of posaconazole and voriconazole, what we were told at that
point in time was, “Nope, no, nope. No need for therapeutic drug monitoring.” We've all heard this story right
around 2000. We're hearing the same story on isavuconazole. But we've not really had a really great look at all of
the pharmacokinetic data yet. And so, I'm going to withhold judgment on what type of therapeutic drug
monitoring is really going to be necessary here. Because again, this is going through P-450 systems just like
posaconazole and voriconazole. There's variability in those P-450 systems just like posaconazole and voriconazole.
It does appear that it’s possibly a little bit better tolerated than voriconazole. And again, it’s once daily after two
days of loading. The nice thing about isavuconazole is it’s got a crazy long half-life of about 380 hours, I believe.
And so it allows you to really get on that once-daily dosing. But that load goes over two days.
It’s again IV and oral. And again, it’s 200 mg both IV and oral with the 1:1 bioavailability. The interesting thing
here though is to be aware, this comes as a pro drug. The pro drug on this is isavuconazonium sulfate. There's also
again no cyclodextrin in the IV, which is a nice advantage because the pro drug is very water soluble. And it only
has the treatment indication at this point. Remember it’s indicated for the treatment of invasive aspergillosis, as
well as the treatment of invasive mucormycosis, albeit with only about 37 patients in that Mucor treatment data
set.
So here again, coming back to one of the questions that we had earlier is the voriconazole versus isavuconazole
phase 3 data in invasive aspergillosis. What you see is really no difference around a lot of the major endpoints
down here. But where you do see it is the drug-related adverse events.
What's really different as far as the adverse drug events go is really areas that you would kind of expect. We know
historically that voriconazole has had issues with skin. Again we're talking about the skin cancer thing here.
Again coming back to voriconazole really quick – the FDA updated the package insert in February of this year.
Again kind of beefing up the wordage on skin abnormalities, visual abnormalities, as well as some of the LFT stuff.
So really I think the challenge with voriconazole continues to be the tolerability of the compound. And really the
issues within the variability of the PK.
So when you look at isavuconazole head-to-head with voriconazole, you would hope to see these kind of three
common problem areas look a little bit better for isavuconazole. And at this point, they really kind of do. It’s
important to note though, and thank you to Johan for pointing this out to me prior to today, was that the
hallucinations are not included in the visual disorders at all. That’s a separate breakout. And there really didn't
appear to be a huge difference there, but that may be due to how the voriconazole was dosed, that you weren't
really seeing super-high voriconazole levels there.
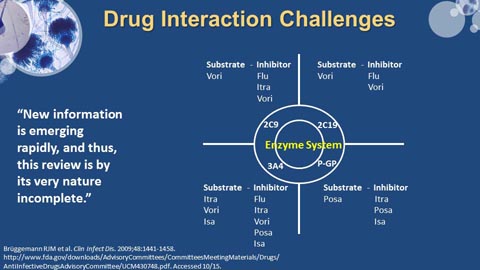 |
Now job security for me is on this slide. The drug interaction stuff with the azoles is one of the major limitations to
the use of this compound. And really what you've got here are some of the major enzyme systems that are out
there from a P-450 standpoint. Notice 3A4. Okay, 3A4 and 3A5 are really where the vast majority of drugs go
through, including a lot of your oncologic drugs. And notice that all of these—look at all of them—are inhibitors.
Now some of them are more potent inhibitors than others, with itraconazole and voriconazole being extremely
potent inhibitors. With voriconazole, interactions are more likely with drugs metabolized via 2C9 and 2C19, but
also with 3A4 inhibitors.
Posaconazole is a pretty good inhibitor, as is isavuconazole. So all of these are going to shut down your P-450
system and are going to push up the levels of anything that is being metabolized through those P-450 systems. So I
think that Brüggemann, who's done a ton of work with this, really says it very nicely in a review that they published
in CID going on about six years ago.
You've really got to stay on top of this, especially in your world. Because you're getting so many new drugs so fast
that a lot of times the drug interaction really is not that well understood when a lot of these new drugs are coming
to market. And when you start shutting down the metabolism of some of these fun-filled compounds that you
guys are using, you can see some very substantial toxicities associated with them. And again, really trying to
remember which drugs are living in which group. And I want to point out, notice that voriconazole is all over the
place. Really voriconazole does multiple enzyme systems, and is all kinds of fun. But for P-glycoprotein, which I
think is really underappreciated—posaconazole and isavuconazole are sitting out there. So, really, irrespective of
where you go within the azole class, the drug interactions are a major challenge.
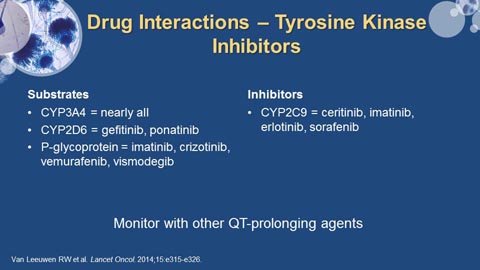 |
Regarding the tyrosine kinase inhibitors – again I am blown away by the number of these new molecules that are
on the market. And what's really interesting – if you haven’t seen it, there's a great review on drug interactions
with tyrosine kinase inhibitors. It was published in Lancet Oncology last year. And it’s really a good one to keep
stuck in a filing cabinet somewhere. But when you look at these, a ton of these things— almost all of them—are
going through 3A4. And when you're going through 3A4, you are going to bump into those azoles. You are going
to do it. And so really, I think this is an area that you've got to pay huge attention to.
The other thing that’s very, very clear – when you look at a lot of the package inserts, the drug interaction work
was done mostly against ketoconazole. Who cares? Nobody uses ketoconazole, and it behaves differently than
the other azoles that we're playing with now. But it’s unfortunately kind of a gold standard in drug development.
So really watch this.
I also want to shout out – always look at the package inserts, always look at your LexiComps, your Micromedex’s.
Put your pharmacist in a headlock and drag them to go to drug interaction review with you. But also there's a very
nice new website. It’s fungalpharmacology.org. There's a nice explanation of it in Journal of Antimicrobial
Chemotherapy this month. And I played around with that website quite a bit. It’s really slick. But I think really
having to stay up on the drug interactions with these new compounds is going to be a challenge for all of us.
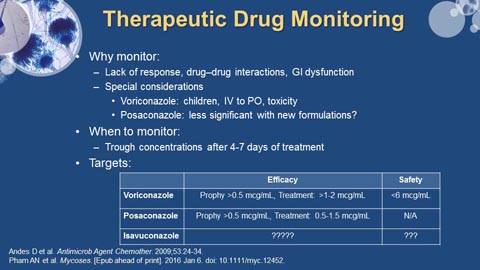 |
Therapeutic drug monitoring – to wrap up really quick. If your patient is on voriconazole, you need therapeutic
drug monitoring – period, end of discussion. And the reason for that is the variability of the compound. And also
the fact that we know that below a serum level of about 1 to 1.5 mcg/mL, the drug doesn’t work. And above a
serum level of about 5 mcg/mL to 5.5 mcg/mL, everybody sees Chewbacca. So you have efficacy issues and you
have tolerability issues. And you have a narrow therapeutic index. Guys, that is the definition of a drug that needs
therapeutic drug monitoring.
What about posaconazole? Posaconazole, it depends. If you're using it for prophylaxis and you're using the new
tablet formulations, I think you can make a very strong argument for no therapeutic drug monitoring. We just
finished an article on this– and it’s actually in press at Mycoses right now. Several other groups have done similar work. When
you're using the tablet formulation, the incidence of patients having a posaconazole serum level that’s less than 0.7 mcg/mL is very low. Now if you're really worried about somebody’s GI integrity – they're throwing everything
up, they’ve got rip-roaring mucositis, it might still be worth a look. But regarding routine TDM for posaconazole in
the era of the tablet formulation, I'm not sure is necessary anymore. When it comes to treatment, I think I would
definitely want them up around 1.0 mcg/mL, okay. But again, the volume of distribution for posaconazole is so
high, it gets out in the tissue so well. And I think we're a little bit less clear because really posaconazole is just not
been used for treatment that much. We don’t know a lot about it from a treatment standpoint.
And isavuconazole, who knows? You've got a massive volume of distribution. There's no signal in the phase 3
data. But then again, there's never a signal in the phase 3 data. It’s always as this stuff percolates out more. So
we don’t really know with isavuconazole yet what the TDM requirement is going to be. We need to see a lot more
PK data on isavuconazole to really help us make that decision.
In conclusion, the issue with the azoles is the drug interactions and the therapeutic drug monitoring considerations
remain there. With isavuconazole, be aware that we don’t know what we don’t know about the pharmacology.
SECTION 4: PROPHYLACTIC, PRE-EMPTIVE, EMPIRICAL, AND DIRECTED ANTIFUNGAL THERAPY...
STRATEGIES THAT ARE MUTUALLY EXCLUSIVE, OR...?
Eric J. Bow, MD, MSC, D. Bacteriol, FRCPC
Thank you very much. I would like to present an approach consistent with that one might take as an oncologist or
as a transplanter, looking at the patient’s journey through the course of their illnesses. So, with that in mind, let
me begin with a review of recent changes in medical mycology that may be relevant to clinicians.
First, the introduction and refinement of consensus-based definitions for invasive fungal infection gives us a
common language around the robustness of the diagnosis. The term “possible invasive fungal infection” implies
something different than “proven infection,” with implications for prognosis. These definitions were designed
specifically for clinical trial use. Notwithstanding, clinicians have been applying them at the bedside.
Second, the availability of a wider spectrum of imaging techniques (high-resolution CT, magnetic resonance
imaging, and PET scanning) has added to our abilities to use radiological features to define clinical syndromes
involving body sites. Recognition of these syndromes is important because it helps direct microbiological and non-microbiological test strategies toward a more robust mycological diagnosis and therapeutic intervention.
Third, the diagnostic process has been enhanced by the availability of nonculture-based biological markers about
which Johan just spoke. There is the galactomannan assay for species; however, a limitation is the
production of this antigen by other molds in varying amounts. The β-D-glucan test for both molds and yeast,
including Pneumocystis jirovecii, is nonspecific. The genomic techniques for mold and yeast based upon PCR may
be more sensitive but remain nonstandardized. The use of mannan/anti-mannan for Candida spp. has limited
usefulness.
Fourth, there are a limited number of classes of available antifungal agents for invasive infection. Each class has a
different molecular target. Accordingly, there has been a renewed interest in the use of combinations, analogous
to the principles employed for oncology regimens. Fifth, we have learned about the practical importance of drug-drug interactions, particularly with the azoles. The importance of the role of therapeutic drug monitoring in
maintaining a balance between efficacy and safety has been discussed. Sixth, the recognition of risk factors for
invasive fungal infection has served to target populations of patients for prevention strategies to mitigate those
risks. The relevant risks are not continuous over a patient’s journey. The spectrum of patients at risk for invasive
fungal infection has been expanded. We are transplanting a broader spectra of patients than in the past. The pre-test probabilities of invasive fungal infection, as Johan has indicated, have increased.
Four broad strategies of management have been developed; preventative strategies such as chemoprophylaxis;
early therapy based on the detection of biological markers of infection, the pre-emptive approach; the empirical
approach for clinical syndromes suspected but not proven to be of fungal origin; and directed therapies for fungal
syndromes based upon the hierarchical classification of possible, probable, or proven infection. These approaches
are not mutually exclusive. There is a great deal of overlap in how the available therapeutics are deployed. It begs
the question about the value encompassed in these strategies for the resources that must be expended in their
deployment.
This is a conceptual paradigm to help understand the relationships among burden of invasive fungal infection, the
probabilities of infection control, and time. Oncologists are very mindful of the inverse impact of tumor burden
upon prognosis. The relationship between fungal burden and outcome is similar.
The detection of surrogate biological markers based upon PCR or antigen detection techniques, together with
high-resolution CT, may enhance the likelihood of early detection. Traditional bedside diagnostic tools based on
signs and symptoms and conventional X-rays arguably detect invasive infection in patients late in the natural
history of the disease, consistent with all-cause mortality rates in the range of 6-8 out of every 10 patients. The
paradigm of early pathogen marker detection with therapeutic intervention has been employed for
cytomegalovirus infection in solid organ and stem-cell transplant recipients as a standard of practice. The
administration of antiviral therapy at the time of detection of CMV DNAemia prevents progression to clinical
disease and the associated excess morbidity and mortality. This principle, based upon biological marker detection,
is now being explored for invasive fungal infection in high-risk patients.
 |
Chemoprophylaxis strategies are deployed among patients at high risk for invasive fungal infection but in whom
there is no mycological evidence of fungal infection or clinical evidence of fungal disease.
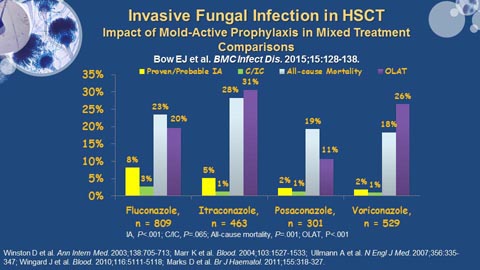
A number of published studies in high-risk stem-cell transplant recipients, summarized in this mixed treatment
comparisons meta-analysis, have demonstrated similar protective effects of the azoles against invasive candidiasis,
but differential protection against invasive mold infections such as invasive aspergillosis. Second generation mold-active agents such as voriconazole and posaconazole appear to be more efficacious in the prevention of proven or
probable invasive aspergillosis and for reducing all-cause mortality compared to either fluconazole or itraconazole.
These treatment effects are encouraging; however, they remain imperfect since breakthrough fungal infections
still occur despite these strategies.
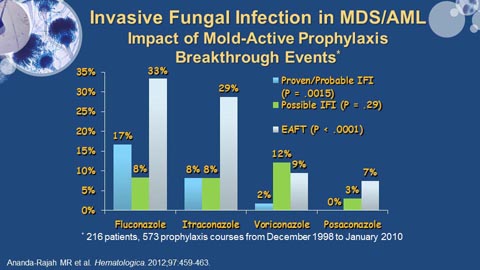 |
The results of systematic reviews notwithstanding, it is encouraging that single center experiences continue to
demonstrate similar treatment effects. Such is the case in this example in AML patients from Melbourne, Australia,
where the mold-active second-generation azoles appear to have not only similar potent protective effects against
proven and probable invasive fungal infection, but also a differential impact compared with fluconazole and
itraconazole on the use of empirical antifungal therapy for the persistent neutropenic fever syndrome.
Adult patients with acute lymphoblastic leukemia who are receiving dose-intense multi-agent multi-cycle
chemotherapy is a population at risk for invasive fungal infection that is often overlooked in clinical trials.
In this example from 4 hospitals in Melbourne, Australia, the anti-leukemic regimen–related event rates for
proven/probable/possible invasive fungal infection seem similar to those reported for AML patients. These anti-leukemic regimens, like the childhood ALL regimens, are corticosteroid-intensive, are administered over many
months, and are designed to be very immunosuppressive, enhancing the risk for invasive mold infections.
Although the numbers illustrated in the slide are not statistically different, there may be a signal in these
observations regarding the magnitude of this risk.
These observations are not sufficient to warrant consideration of routine deployment of mold-active prophylaxis;
however, they do reinforce the need for more robust assessment of the actual event rates for invasive fungal
infection among adult ALL patients receiving dose-intensive chemotherapy regimens.
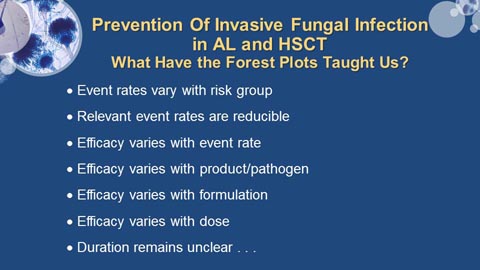 |
There have been a number of antifungal prophylaxis studies published over the years. There are a number of
lessons to be gleaned from the systematic reviews of these experiences. First, the risk for invasive fungal infection
is not uniform across all patient groups, and the risks are discontinuous over time. For example, the risk for
invasive fungal infection during remission induction in AML is higher than that associated with post-remission
consolidation. Accordingly, antifungal prophylaxis may be appropriate for the former but not the latter situation.
Second, clinical trials have demonstrated that relevant event rates such as proven and probable invasive fungal
infection are reducible by chemoprophylaxis strategies.
Third, the efficacy of chemoprophylaxis also varies with the event rate. The lowest event rate for invasive fungal
infection among control patients in comparative clinical trials appears to be of the order of 5 to 6%. The protective
benefit of antifungal prophylaxis applied to a population where the baseline event rate is below this may be
negligible, or at least not be detectable. It may not be worth our while to apply an antifungal prophylactic strategy
in that patient population, given the expense of the drug, the toxicities of the drug, and the increasing concerns
over antifungal drug resistance.
Fourth, efficacy varies with product and the pathogen. For example, an anti-aspergillosis prophylaxis strategy
based upon fluconazole would be expected to fail based upon the lack of activity of this agent against Aspergillus spp. Accordingly, the clinician must choose the antifungal prophylaxis agent on the basis of the pathogen to be
targeted and the antifungal activity of the agent. Fifth, the choice of formulation may impact upon antifungal
efficacy. For example, systematic review of clinical trials evaluating the role of itraconazole to prevent invasive
aspergillosis demonstrated relative lack of efficacy of the oral capsules compared with the oral solution. Sixth,
efficacy varies with the dose of antifungal agent. Experience has suggested that lower doses may result in lower
drug exposures and increased risk for treatment failures and breakthrough fungal infection.
Lastly, the optimal duration of prophylaxis remains unclear. Many pundits argue that antifungal therapy should
continue until the end-of-risk. End-of-risk may be defined by recovery from myelosuppression, as in the
circumstances of AML therapy-induced neutropenia, or by the discontinuance of immunosuppressive therapy as in
the case of allogeneic stem cell transplant recipients treated successfully for acute graft-versus-host disease. The
optimal duration for prophylaxis in adult ALL, where intensive treatments may last 8 or more months, remains
undefined.
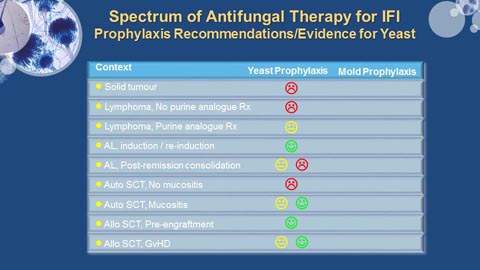 |
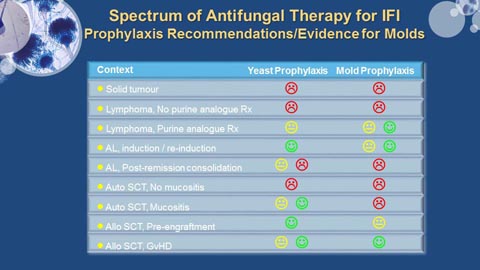
This is an illustrated summary of the circumstances in which published guidelines suggest yeast and mold
prophylaxis should be considered. The green and red faces indicate recommendations for and against antifungal
prophylaxis, respectively. The yellow face indicates insufficient evidence to support a recommendation (clinical
equipoise). Yeast prophylaxis is not recommended in patients undergoing primary treatment for solid tumors or
lymphoma. The use of purine analogue therapy enhances the immunosuppressive effect of chemotherapy in
lymphoreticular malignancies; however, it remains unclear whether this effect translates into an enhanced risk for
invasive fungal infection. There is evidence supporting yeast prophylaxis in the setting of primary and salvage
induction therapy in AML (AI), but not post-remission consolidation. Similarly, the duration of the
myelosuppression-driven risk for invasive candidiasis is sufficiently short among stem-cell autograft recipients,
particularly where hematopoietic growth factors are being employed to hasten engraftment, such that anti-yeast
prophylaxis is not recommended. There may be an argument for such prophylaxis among stem cell autograft
recipients receiving myeloablative conditioning regimens without hematopoietic growth factor support and who
are expected to have grade 3-4 mucositis. Yeast prophylaxis may be considered for stem-cell allograft recipients
during the pre-engraftment phase post transplant and during the post-engraftment phase that is punctuated by
graft-versus-host disease.
 |
Mold-active prophylaxis is not recommended for patients receiving cyclical cytotoxic chemotherapy for solid
tumors or lymphoma. There is a suggestion from case series that the risk of invasive mold infection among purine
analogue recipients (eg, patients with advanced chronic lymphocytic leukemia) may be sufficiently high to warrant
consideration of anti-mold prophylaxis. The evidence base to support this is not robust, however (CII). AML
patients undergoing primary or secondary remission-induction may benefit from anti-mold prophylaxis if they are
being treated outside a high-efficiency particulate air-filtered protected environment (AI). As for the
considerations for yeast prophylaxis after post-remission consolidation, mold-active prophylaxis is not
recommended for consolidation in AML; nor is it recommended in the setting of stem cell autografting. Although
many clinicians prescribe anti-mold prophylaxis in the pre-engraftment setting post stem cell allografting, there is
little clinical trial–based evidence to support this practice. It seems to be largely extrapolated from the AML
induction experience. Lastly, mold-active prophylaxis is recommended in the circumstance of graft-versus-host
disease post stem cell allografting.
This can be modified if your institution event rate is unacceptably high, that is above 8% or 9%; then that would
justify reconsidering some of these guidelines.
Let me address pre-emptive therapy for just for a few moments. There are a number of studies that have tried to
address how we should execute this strategy using the diagnostic technologies that we have available.
An early retrospective trial, a single arm trial from France examined the role of serial high resolution CT screening.
Another nonrandomized study in AML patients, published by Johan Maertens, demonstrated a 78% reduction in
the prescription of empirical anti-fungal therapy through serial serum galactomannan testing. A randomized-controlled German trial of serial serum Aspergillus PCR in stem cell transplant recipients, observed 56% strategy-driven increase in the use of empirical antifungal therapy, but no impact upon all-cause mortality.
Another randomized-controlled French study, from Cordonnier and colleagues, in acute leukemia and stem cell
autograft patients using clinical signs and symptoms along with a serum galactomannan, observed a 36% reduction
in the use of empirical amphotericin B therapy and an increase in the IFI detection rate, but no strategy-driven
impart upon all-cause mortality.
A Swedish study examined a once-weekly pan-fungal PCR-based pre-emptive strategy for invasive fungal infection
among reduced-intensity conditioned (RIC) stem cell allograft recipients during the first 100 post-transplant days.
No impact of the monitoring strategy was detected before day 100. Most of the cases of IFI occurred after day 100,
consistent with the period of greatest risk among RIC-conditioned allograft recipients.
Lastly, a randomized-controlled multicenter study in acute leukemia and stem-cell transplant recipients in Australia
examined the impact of serial screening using both serial galactomannan and PCR-based assays. There was a
strategy-driven 53% reduction in the use of empirical antifungal therapy but no impact on directed antifungal
therapy or all-cause mortality.
These studies illustrate proof of principle that diagnostics-driven testing for biological markers of invasive fungal
infection can impact on the empirical use of antifungal therapy and also reduce the time to treatment.
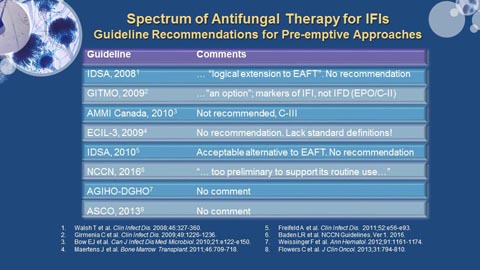 |
What do our guidelines say about this? The IDSA guidelines saw pre-emptive as a logical extension to empirical
antifungal therapy, but no recommendations could be offered on the basis of the available information at the
time. The Italian guidelines recommend a “surveillance strategy and/or an active diagnostic approach.” The
Canadian guidelines could not make a recommendation based upon the information available in 2009-2010. The
2009 European Conference on Infections in Leukaemia–3 was unable to make any recommendation because of a
lack of standardized definitions. The 2010 IDSA guidelines on the use of antimicrobial agents in neutropenic
patients suggested that a diagnostics-driven pre-emptive approach may become an acceptable alternative to
empirical antifungal therapy strategies, but couldn’t make a firm recommendation at that time.
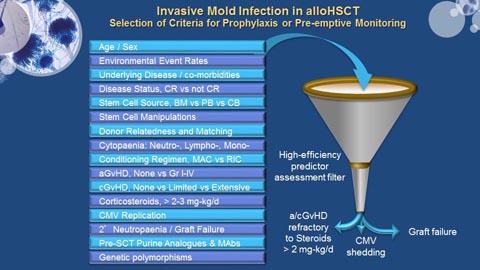 |
There are a number of risk factors that have been identified for invasive fungal infection among patients
undergoing hematopoietic stem cell transplantation. Many of these are listed on the left hand side of the slide.
Some are dependent upon one another, and others are independent predictors of IFI. Some may even interact
with one another with synergistic or additive effects.
After review, some of these factors such as steroid-refractory graft-versus-host disease, cytomegalovirus
DNAemia, and graft failure have been prominent in the literature as variables linked to enhanced risk for IFI.
The above figure is offered as a model of how these predictor variables might be used to decide which patients
might be candidates for mold-active chemoprophylaxis or a diagnostics-driven pre-emptive strategy.
For example, the onset of GvHD among stem cell allograft recipients is a known risk factor for IFI (see the pathway
at the top of the figure). Among the sub-group who prove to have steroid-refractory GvHD and for whom
augmented immunosuppression is required, the risk for IFI may be even greater. Such patients may be candidates
for a mold-active prophylaxis approach, whereas a diagnostics-driven pre-emptive monitoring approach may be
appropriate for those whose GvHD responds to primary steroid-based therapy.
Among patients who shed Cytomegalovirus (CMV, a known risk for IFI in stem cell transplant recipients – see the
middle pathway in the figure), a mold-active prophylaxis approach might be considered for those who also develop
GvHD, but a pre-emptive monitoring approach may be considered for those who remain free of GvHD.
Similarly, among those transplant recipients who develop graft failure, a mold-active prophylaxis approach may be
considered if there is concomitant CMV DNAemia, and pre-emptive monitoring may be considered for those
without CMV DNAemia.
These possibilities would limit the exposure of mold-active triazole prophylaxis to very selected sub-groups of
patients at risk for IFI. Such strategic management pathways will require validation in prospective trials before they
can be accepted and deployed for routine use, however.
Empirical antifungal therapies are administered to patients at risk for IFI and who have a febrile illness that could
be driven by an invasive fungal infection, but for whom there is no mycological and very limited clinical evidence to
support an IFI diagnosis. A persistent neutropenic fever (PNF) syndrome occurring in the setting of broad-spectrum
antibacterial therapy is an example of such a circumstance (the case definition for which appears on the slide that
follows).
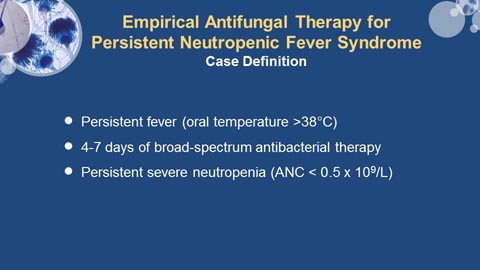 |
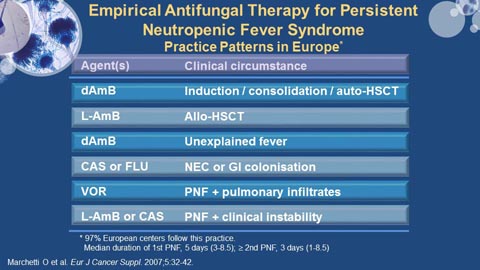 |
The approaches clinicians have employed for the PNF have varied depending upon the clinical circumstances (see
the above figure). For example, a survey of European clinicians’ antifungal prescriptions demonstrated a
preference for conventional amphotericin B deoxycholate for empirical antifungal therapy for the PNF syndrome in
the setting of unexplained fever during acute leukemia induction or post-remission consolidation. However,
liposomal amphotericin B was preferred in the setting of allogeneic stem cell transplantation, or in the setting of
PNF with clinical instability. A mold-active azole, voriconazole, was preferred if the PNF syndrome was
accompanied by pulmonary infiltrates. An echinocandin or fluconazole was preferred in the setting of neutropenic
enterocolitis.
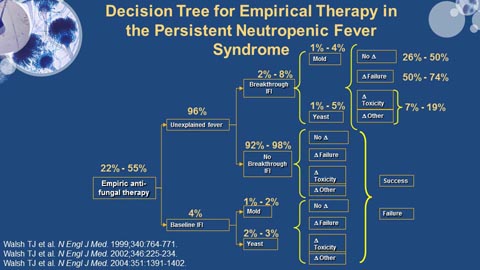 |
Based upon published experience (see the above figure), the PNF syndrome may be seen in approximately one-in-five to one-in-two neutropenic subjects. Most (96%) of these neutropenic fevers remain unexplained (that is, no
focus and no pathogen identified). Of these febrile events, a smaller proportion of PNF syndromes (2-8%) may be
associated with breakthrough IFI, whilst the patient continues to receive the empirical antifungal agent. These
breakthrough IFIs are divided between invasive candidiasis and an invasive mold infection. A small proportion (~4%) of PNF syndromes may be explained by a baseline IFI, either a mold or an invasive yeast infection. Treatment
of these events must take into consideration the antifungal agents received by the patient as either antifungal
prophylaxis or as empirical antifungal therapy. Such patients will be treated until response or until a change is
required primarily for treatment failure or for toxicity.
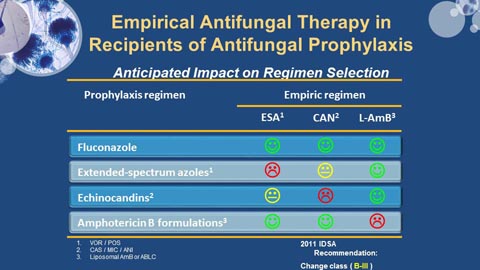 |
The choice of prophylactic antifungal agent influences the choice of the class of antifungal agent to be used for
empirical or directed therapy. For example, breakthrough IFIs in patients receiving fluconazole-based anti-fungal
prophylaxis may be salvaged using an extended-spectrum mold-active azole (ESA) such as voriconazole, or an
echinocandin such as caspofungin, or a polyene such as liposomal amphotericin B. Given the similarities in
antifungal spectrum among ESAs and echinocandins, salvage therapy for breakthrough IFI for patients receiving
ESAs or echinocandins as prophylaxis is limited to liposomal amphotericin. However, salvage antifungal therapy for
systemic amphotericin-based prophylaxis failures is limited to ESAs or echinocandins, the similarities of activity
spectra notwithstanding.
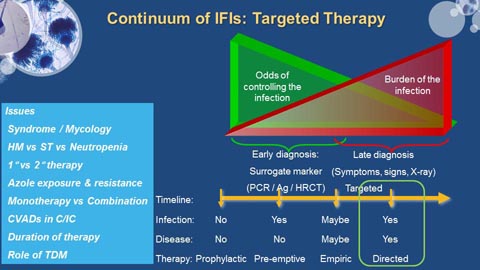 |
Directed antifungal therapy is based upon a hierarchical classification of diagnostic robustness; that is, possible,
probable, or proven IFI. The clinician must consider the syndrome and the possible mycological etiologies, the
context of the underlying cancer and treatment for that cancer, prior exposure to azoles and the possibility of drug
resistance, the role of monotherapy and combination antifungal therapy, the role of risk factors such as the
presence of central venous access devices that may be amenable to modification, the duration of antifungal
treatment required for a given syndrome, and the role of therapeutic drug monitoring for azole therapy to
optimize efficacy and minimize toxicity.
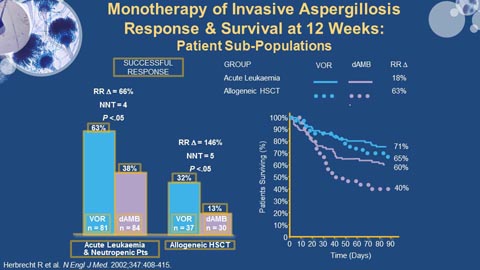 |
Voriconazole has become the accepted standard of practice for the treatment of invasive aspergillosis in high-risk
patients. Based on the seminal study of Herbrecht and colleagues in 2002 comparing voriconazole to the then-standard, amphotericin B deoxycholate, a significant clinical response and survival advantage was demonstrated
among the voriconazole recipients. Moreover, the treatment effect was observed among different diagnostic sub-groups of patients (see the above figure for the relative responses among acute leukemic neutropenic patients and
stem-cell transplant patients). It was noted that response rates among stem-cell transplant recipients was significantly lower than among other risk groups, suggesting that more work was needed to improve these
outcomes for this group of patients.
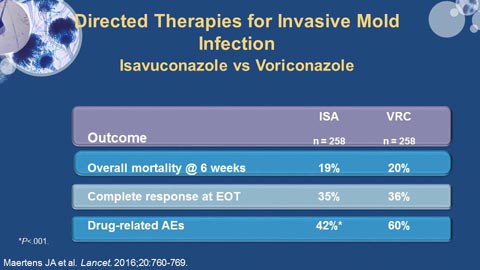 |
Newer agents such as isavuconazole have been studied for invasive aspergillosis. The results of a recent
comparative trial with voriconazole have suggested similar efficacy but a modest toxicity advantage for
isavuconazole.
A recent blinded, randomized-controlled trial by Marr and colleagues (see the above figure) of combination
antifungal therapy for invasive aspergillosis in stem-cell transplant recipients and patients under treatment for
hematological malignancy demonstrated a survival advantage for a combination of voriconazole and an
echinocandin, anidulafungin, among patients with galactomannan-based probable invasive aspergillosis who had a
moderate burden of infection (as measured by serum galactomannan – see figure below).
The published guidelines for invasive aspergillosis (IA) do not support combination antifungal therapy for the
primary treatment of IA. There is more support for the use of combination strategies in salvage IA therapy.
The issue of extended-spectrum azole resistance among Aspergillus spp. has been raised by several investigators.
The above map from the group in Nijmegen, the Netherlands, demonstrating the wide distribution of resistant
strains (in the shaded areas) that have been identified. This phenomenon is raised as a cautionary note.
Let me just summarize what I have learned.
- Antifungal prophylaxis strategies may have a protective treatment effect against molds and yeasts; but, ...
- It remains unclear - who gets the most benefit and the best value for the dollar spent?
- Whilst the reported experience with diagnostics-based pre-emptive therapy looks promising, we don’t yet
know the optimal drivers. In some clinical circumstances this strategy may replace antifungal prophylaxis.
- Persistent neutropenic fever–driven empirical antifungal therapy has limited utility. It adds cost and certainly
over-treats and adds to the risk of toxicity.
- Based on the available evidence, voriconazole today represents the monotherapy of choice for
proven/probable invasive aspergillosis. The fungal disease burden also influences the outcome and prognosis
for patients.
- Combination antifungal therapy for invasive aspergillosis infections is experimental but looks very promising.
The one study that we have discussed is promising but in a very distinct subgroup of patients for whom the
diagnosis was established by the use of serum galactomannan.
- Azole-based mold-active prophylaxis will likely preclude the use of azole-based combination antifungal
therapy. It is unclear whether the efficacy of azole:liposomal amphotericin B combination therapy is
equivalent to azole:echinocandin therapy.
- The ever-present threat of resistance among fungi may represent a limiting factor in treatment success.
Increasing antifungal resistance may threaten the effectiveness of the strategies that have recently been
developed. Antifungal stewardship in the form of a disciplined approach to the deployment of these agents
may limit, at least in part, the impact of this phenomenon.
SECTION 5: PANEL DISCUSSION
QUESTION:
To the panel, can you comment on some of the major flaws in the Gomes study? Namely the use of IFI incidence
per prophylactic days (where echinocandins were only used in the first 30 days, the highest risk period and
likely) in the patients receiving hepatotoxic chemo, ie, clofarabine. Fluconazole actually had the lowest rate of
IFIs per their definition. Basically how comfortable are you in using echinocandin prophylaxis and treatment in
various setting?
ANSWER:
JAMES LEWIS, II, PharmD:
I think the author of the question really hits a lot of the nails on the head with regards to the limitations of that
study. And I think the fact that it’s a single-center experience with a very high attack rate are 2 other limitations to
the data set that I would certainly add.
That being said, though, the fact of the matter is that there's still something of a signal there. And it is one of
those things where I will certainly use the echinocandin in a prophylaxis setting when there is a good reason not to
be using the azole.
And I think what that data says to me is that I will do that, but I will try to get them back to the azole as quickly as I
can for a more prolonged prophylaxis-type setting. Again it’s anecdotal single-center experience, but we certainly
seem to see more breakthroughs with echinocandins, as well. Again, limitation, single-center, anecdotal response
to the question.
But it does give me a little bit of pause. So I think long story short, I would still do it if absolutely necessary in a
situation where the azole therapy is not optimal, for whatever reason, but will try to get back to an azole as quickly
as I can.
QUESTION FROM AUDIENCE MEMBER:
As I go through the slides, I see one of the highest incidence of fungal infection is in patients with acute
lymphoblastic leukemia. And one of the problems in prophylaxis over there is if you use azole, there is an
interaction with vincristine, which is the mainstay of therapy – and there is an interaction between vincristine
and azoles. And if you use something like micafungin, it’s an intravenous therapy and you cannot do this in the
outpatient setting.
So let me ask, in each of your institutions, how do you deal with that? And sometimes the toxicity is really bad if
you're using azoles that you have to stop their ALL therapy. And that has affected their outcomes.
ANSWER:
MATTHEW LUNNING, DO:
That’s an excellent question. In fact, that was something that we spent I think a good 10 minutes on before the
actual symposium discussing about it. Because internally in our own ALL use, whether it’s with HyperCVAD in ALL,
or trying to use some of the earlier BFM regimens and AYAs, we struggle with this concept. And I don't know that
there's definitely a right answer.
ALISON FREIFELD, MD:
I don’t think there is a very good answer. And I will say that, for example, the NCCN guidelines suggest an
echinocandin. And I know that’s very burdensome for the patient. But we also try to avoid the azoles in that
situation. There's not a great answer for that because of the severe neurotoxicity.
MATTHEW LUNNING, DO:
And I think that sometimes, if you will, people try to use echinocandins as an outpatient in a different dosing and
schedule. I think it’s 300 Monday, Wednesday, Friday is something that I have seen be done.
But where is the data for that? Well, it’s often single institution; this is how we try to do it, rather than, “There's a
paper to be referenced.”
JAMES LEWIS, II, PharmD:
But again I think to follow up, that was exactly the point I was going to make. There's a very nice supplement that
was—I believe it was sponsored by Astellas—that was in Clinical Infectious Diseases not too long ago.
Really, when you look at echinocandin half-life and you look at the fact that those are concentration-dependent
drugs, or at least they appear to be in vitro, some of these extended dosing interval uses of the echinocandins I
think really do make a lot of sense pharmacologically. And while I understand that there are definite limitations,
the currently available data, I think that again given the risk of the azoles with the vincristines and whatnot of the
world, that those types of regimens make a lot of sense.
ERIC BOW, MD:
Again I think what you've done is identified an unmet need for research. And again, many individuals—at least in
the Canadian centers—have chosen to go back to the old school of using amphotericin B in intermittent dosing.
And again, I know of no specific data in adult ALL using HyperCVAD-like regimens that gives us confidence in that
strategy. I’ll have to argue, just as an aside, I don't know that we actually know what the event rates for invasive
fungal disease—and mold disease in particular—is in that patient population as an ambulatory type of population.
AUDIENCE MEMBER:
At our own center, we have been doing it for the first cycle they are usually inpatient, so we use an
echinocandin. But for the subsequent cycles, for the Part B, we go to an azole. And for the third cycle, we try to
start an azole 48 hours after vincristine and give a break. But I'm not sure...
ALISON FREIFELD, MD:
That’s reasonable.
MATTHEW LUNNING, DO:
And I think the risk probably changes as you get further along in ALL management obviously. Upfront they're at
much higher risk because you can never tell how long they’ve been immunosuppressed functionally from their
disease, leading into cycles 1a and 1b, or induction and intensification from that standpoint. Johan, did you have a
comment?
JOHAN MAERTENS, MD:
Yeah, I wanted to comment on Eric’s suggestion of using a polyene. You have to know that Gilead just did a study
looking at adult ALL patients, where they randomized them between either placebo or a liposomal amphotericin B
given twice weekly at 5 mg/kg during the first cycle.
And it’s quite a large study, it’s around 300 patients. The incidence of invasive fungal infection was much higher
than what we saw in the Italian study, that was 7.5%. In the Gilead study, it’s 12%. So it’s really almost the same
size in what we see in the AML population.
But the key message of the study was that there was no difference between the placebo arm and the liposomal
amphotericin B arm. Now that may be because the dose was too low, or maybe you have to give it 3 times a week
instead of twice. That we don’t know.
But if you look at the study results, there was no real difference between placebo or liposomal amphotericin B
during the first cycle of ALL treatment.
ALISON FREIFELD, MD:
And I think that’s a good point. And also to follow up on what Matt is saying, if we use AML as the paradigm, what
I showed was that the incidence of invasive fungal disease is maybe 3% during consolidation cycle.
So as you control the underlying disease, your rates of invasive fungal infection are markedly declined. So the first
cycle is the one obviously that—especially as you're underscoring—probably makes the most sense in which to do
the most intensive prophylaxis.
QUESTION: This will be for Johan to give you some time to think. How often do you see false positive makers, ie
(1→3)-β-D-glucan when patients are dialysis?
ANSWER:
JOHAN MAERTENS, MD:
Oh, a lot. If you have a patient on dialysis and (1→3)-β-D-glucan is quite difficult to use. So let's say that most of
the false positives we see in the ICU setting, patients receiving hemoglobins, lots of blood products, being on
dialysis, being post surgery—it’s a difficult assay to handle in the ICU setting or in the critical outpatient
population.
We don’t see that many false positives in let's say the neutropenic hematology population. But as you mentioned
on dialysis, it really is a problem.
QUESTION FROM AUDIENCE:
Hi, John Wilson from Mayo Clinic. And we've been wrestling with the use of isavuconazole in our hematology
patients, whether prophylactically or therapeutically and looking at the potential, just because of cost issues and
looking at the potential role for patients that have underlying QTc prolongation or drug interactions in that
capacity.
But we're also looking at the long half-life of isavuconazole and the potential use of antineoplastics with CYP3A4
drug interactions in that regard, and given that long terminal half-life I think of 130-140 hours, should we
potentially be looking at a washout period of stopping isavuconazole, looking at another potential anti-mold
agent for a period of time before embarking on other agents with CYP3A4 drug interactions, or additional
antineoplastic chemotherapy options that go down that route?
ANSWER:
JAMES LEWIS, II, PharmD:
I sure as heck would. I completely agree with you that that long half-life, while it’s of benefit from a therapeutic
and ease of dosing standpoint, in the situations you're describing, it really represents a challenge. That inhibition
of the P-450 system does not go away for at least the first 2 to 3 half-lives. And it’s probably even a little bit further
out than that. So I really agree with your comments and your concerns.
References
- Allen KC, Sanchez CJ Jr, Niece KL, Wenke JC, Akers KS. Voriconazole enhances the osteogenic activity of human
osteoblasts in vitro through a fluoride-independent mechanism. Antimicrob Agents Chemother. 2015;59:7205-7213.
- Ananda-Rajah MR, Grigg A, Downey MT, et al. Comparative clinical effectiveness of prophylactic
voriconazole/posaconazole to fluconazole/itraconazole in patients with acute myeloid leukemia/myelodysplastic
syndrome undergoing cytotoxic chemotherapy over a 12-year period. Haematologica. 2012;97:459-463.
- Andes D, Pascual A, Marchetti O. Antifungal therapeutic drug monitoring: established and emerging indications. Antimicrob Agents Chemother. 2009;53:24-34.
- Arvanitis M, Anagnostou T, Mylonakis E. Galactomannan and polymerase chain reaction-based screening for
invasive aspergillosis among high-risk hematology patients: a diagnostic meta-analysis. Clin Infect Dis.
2015;61:1263-1272.
- Arvanitis M, Ziakas PD, Zacharioudakis IM, Zervou FN, Caliendo AM, Mylonakis E. PCR in diagnosis of invasive
aspergillosis: a meta-analysis of diagnostic performance. J Clin Microbiol. 2014;52:3731-3742.
- Astellas Anti-Infective Drugs Advisory Committee. Briefing Document: Isavuconazonium Invasive Aspergillosis and
Invasive Mucormycosis. Northbrook, IL: Astellas Pharma US, Inc.; 2014.
http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/
AntiInfectiveDrugsAdvisoryCommittee/UCM430748.pdf. Accessed 10/15.
- Baddley JW, Andes DR, Marr KA, et al. Factors associated with mortality in transplant patients with invasive
aspergillosis. Clin Infect Dis. 2010;50:1559-1567.
- Barnes RA, Stocking K, Bowden S, Poynton MH, White PL. Prevention and diagnosis of invasive fungal disease in
high-risk patients within an integrative care pathway. J Infect. 2013;67:206-214.
- Blennow O, Remberger M, Klingspor L, et al. Randomized PCR-based therapy and risk factors for invasive fungal
infection following reduced-intensity conditioning and hematopoietic SCT. Bone Marrow Transplant.
2010;45:1710-1718.
- Bow EJ, Evans G, Fuller J, et al. Canadian clinical practice guidelines for invasive candidiasis in adults. Can J Infect
Dis Med Microbiol. 2010;21:e122-e150.
- Brüggemann RJ, Alffenaar JW, Blijlevens NM, et al. Clinical relevance of the pharmacokinetic interactions of azole
antifungal drugs with other coadministered agents. Clin Infect Dis. 2009;48:1441-1458.
- Bueid A, Howard SJ, Moore CB, et al. Azole antifungal resistance in Aspergillus fumigatus: 2008 and 2009. J
Antimicrob Chemother. 2010;65:2116-2118.
- Caillot D, Casasnovas O, Bernard A, et al. Improved management of invasive pulmonary aspergillosis in neutropenic
patients using early thoracic computed tomographic scan and surgery. J Clin Oncol. 1997;15:139-147.
- Caira M, Candoni A, Verga L, et al; SEIFEM Group (Sorveglianza Epidemiologica Infezioni Fungine in Emopatie
Maligne). Pre-chemotherapy risk factors for invasive fungal diseases: prospective analysis of 1,192 patients with
newly diagnosed acute myeloid leukemia (SEIFEM 2010-a multicenter study). Haematologica. 2015;100:284-292.
- Cordonnier C, Pautas C, Maury S, et al. Empirical versus preemptive antifungal therapy for high-risk, febrile,
neutropenic patients: a randomized, controlled trial. Clin Infect Dis. 2009;48:1042-1051.
- Cornely O, Maertens J, Bresnik M, et al; AmBiLoad Trial Study Group. Liposomal amphotericin B as initial therapy
for invasive mold infection: a randomized trial comparing a high-loading dose regimen with standard dosing
(AmBiLoad trial). Clin Infect Dis. 2007;44:1289-1297.
- Cornely OA, Maertens J, Winston DJ, et al. Posaconazole vs. fluconazole or itraconazole prophylaxis in patients
with neutropenia. N Engl J Med. 2007;356:348-359.
- Cresemba prescribing information. Northbrook, IL: Astellas Pharma; 2015.
- De Pauw B, Walsh TJ, Donnelly JP, et al; European Organization for Research and Treatment of Cancer/Invasive
Fungal Infections Cooperative Group; National Institute of Allergy and Infectious Diseases Mycoses Study Group
(EORTC/MSG) Consensus Group. Revised definitions of invasive fungal disease from the European Organization for
Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of
Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin Infect Dis. 2008;46:1813-1821.
- Diflucan prescribing information. New York, NY: Pfizer; 2014.
- Doan TN, Kirkpatrick CM, Walker P, et al. Primary antifungal prophylaxis in adult patients with acute lymphoblastic
leukaemia: a multicentre audit. J Antimicrob Chemother. 2015;71:497-505.
- Donnelly JP, Leeflang MM. Galactomannan detection and diagnosis of invasive aspergillosis. Clin Infect Dis.
2010;50:1070-1071.
- Duarte RF, Sánchez-Ortega I, Cuesta I, et al. Serum galactomannan-based early detection of invasive aspergillosis in
hematology patients receiving effective antimold prophylaxis. Clin Infect Dis. 2014;59:1696-1702.
- Flowers CR, Seidenfeld J, Bow EJ, et al. Antimicrobial prophylaxis and outpatient management of fever and
neutropenia in adults treated for malignancy: American Society of Clinical Oncology clinical practice guideline. J
Clin Oncol. 2013;31:794-810.
- Freifeld AG, Bow EJ, Sepkowitz KA, et al; Infectious Diseases Society of America. Clinical practice guideline for the
use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the Infectious Diseases Society of
America. Clin Infect Dis. 2011;52:e56-e93.
- Girmenia C, Barosi G, Aversa F, et al. Prophylaxis and treatment of invasive fungal diseases in allogeneic stem cell
transplantation: results of a consensus process by Gruppo Italiano Trapianto di Midollo Osseo (GITMO). Clin Infect
Dis. 2009;49:1226-1236.
- Girmenia C, Raiola AM, Piciocchi A, et al. Incidence and outcome of invasive fungal diseases after allogeneic stem
cell transplantation: a prospective study of the Gruppo Italiano Trapianto Midollo Osseo (GITMO). Biol Blood
Marrow Transplant. 2014;20:872-880.
- Glasmacher A, Cornely O, Ullmann AJ, et al; Itraconazole Research Group of Germany. An open-label randomized
trial comparing itraconazole oral solution with fluconazole oral solution for primary prophylaxis of fungal infections
in patients with haematological malignancy and profound neutropenia. J Antimicrob Chemother. 2006;57:317-325.
- Gomes MZ, Jiang Y, Mulanovich VE, Lewis RE, Kontoyiannis DP. Effectiveness of primary anti-Aspergillus prophylaxis during remission induction chemotherapy of acute myeloid leukemia. Antimicrob Agents Chemother.
2014;58:2775-2780.
- Goyal RK. Voriconazole-associated phototoxic dermatoses and skin cancer. Expert Rev Anti Infect Ther.
2015;13:1537-1546.
- Harousseau JL, Dekker AW, Stamatoullas-Bastard A, et al. Itraconazole oral solution for primary prophylaxis of
fungal infections in patients with hematological malignancy and profound neutropenia: a randomized, double-blind, double-placebo, multicenter trial comparing itraconazole and amphotericin B. Antimicrob Agents
Chemother. 2000;44:1887-1893.
- He S, Hang JP, Zhang L, Wang F, Zhang DC, Gong FH. A systematic review and meta-analysis of diagnostic accuracy
of serum 1,3-β-D-glucan for invasive fungal infection: focus on cutoff levels. J Microbiol Immunol Infect.
2015;48:351-361.
- Hebart H, Klingspor L, Klingebiel T, et al. A prospective randomized controlled trial comparing PCR-based and
empirical treatment with liposomal amphotericin B in patients after allo-SCT. Bone Marrow Transplant.
2009;43:553-561.
- Heng SC, Morrissey O, Chen SC, et al. Utility of bronchoalveolar lavage fluid galactomannan alone or in
combination with PCR for the diagnosis of invasive aspergillosis in adult hematology patients: a systematic review
and meta-analysis. Crit Rev Microbiol. 2015;41:124-134.
- Herbrecht R, Flückinger U, Gachot B, Ribaud, Thiebaut A, Cordonnier C. Treatment of invasive Candida and invasive Aspergillus infections in adult haematological patients. Eur J Cancer Suppl. 2007;5:49-59.
- Herbrecht R, Denning DW, Patterson TF, et al; Invasive Fungal Infections Group of the European Organisation for
Research and Treatment of Cancer and the Global Aspergillus Study Group. Voriconazole versus amphotericin B for
primary therapy of invasive aspergillosis. N Engl J Med. 2002;347:408-415.
- Hou TY, Wang SH, Liang SX, Jiang WX, Luo DD, Huang DH. The screening performance of serum 1,3-beta-D-glucan in
patients with invasive fungal diseases: a meta-analysis of prospective cohort studies. PLoS One. 2015;10:e0131602.
- Karageorgopoulos DE, Vouloumanou EK, Ntziora F, Michalopoulos A, Rafailidis PI, Falagas ME. β-D-glucan assay for
the diagnosis of invasive fungal infections: a meta-analysis. Clin Infect Dis. 2011;52:750-770.
- Kontoyiannis DP. Invasive mycoses: strategies for effective management. Am J Med. 2012;125(1 Suppl):S25-S38.
- Kontoyiannis DP, Marr KA, Park BJ, et al. Prospective surveillance for invasive fungal infections in hematopoietic
stem cell transplant recipients, 2001-2006: overview of the Transplant-Associated Infection Surveillance Network
(TRANSNET) Database. Clin Infect Dis. 2010;50:1091-1100.
- Krishna G, Ma L, Martinho M, Preston RA, O'Mara E. A new solid oral tablet formulation of posaconazole: a
randomized clinical trial to investigate rising single- and multiple-dose pharmacokinetics and safety in healthy
volunteers. J Antimicrob Chemother. 2012;67:2725-2730.
- Lamoth F, Cruciani M, Mengoli C, et al; Third European Conference on Infections in Leukemia (ECIL-3). β-Glucan
antigenemia assay for the diagnosis of invasive fungal infections in patients with hematological malignancies: a
systematic review and meta-analysis of cohort studies from the Third European Conference on Infections in
Leukemia (ECIL-3). Clin Infect Dis. 2012;54:633-643.
- Leeflang MM, Debets-Ossenkopp YJ, Visser CE, et al. Galactomannan detection for invasive aspergillosis in
immunocompromized patients. Cochrane Database Syst Rev. 2008;(4):CD007394.
- Maertens J, Marchetti O, Herbrecht R, et al; Third European Conference on Infections in Leukemia. European
guidelines for antifungal management in leukemia and hematopoietic stem cell transplant recipients: summary of
the ECIL 3--2009 update. Bone Marrow Transplant. 2011;46:709-718.
- Maertens J, Theunissen K, Verhoef G, et al. Galactomannan and computed tomography-based preemptive
antifungal therapy in neutropenic patients at high risk for invasive fungal infection: a prospective feasibility study. Clin Infect Dis. 2005;41:1242-1250.
- Maertens JA, Nucci M, Donnelly JP. The role of antifungal treatment in hematology. Haematologica. 2012;97:325-327.
- Maertens JA, Raad II, Marr KA, et al. Isavuconazole versus voriconazole for primary treatment of invasive mould
disease caused by Aspergillus and other filamentous fungi (SECURE): a phase 3, randomised-controlled, non-inferiority trial. Lancet. 2016;387:760-769.
- Malani AN, Kerr L, Obear J, Singal B, Kauffman CA. Alopecia and nail changes associated with voriconazole therapy. Clin Infect Dis. 2014;59:e61-e65.
- Marchetti O, Lamoth F, Mikulska M, Viscoli C, Verweij P, Bretagne S; European Conference on Infections in
Leukemia (ECIL) Laboratory Working Groups. ECIL recommendations for the use of biological markers for the
diagnosis of invasive fungal diseases in leukemic patients and hematopoietic SCT recipients. Bone Marrow
Transplant. 2012;47:846-854.
- Marchetti O, Cordonnier C, Calandra T. Empirical antifungal therapy in neutropaenic cancer patients with
persistent fever. Eur J Cancer Suppl. 2007;5:32-42.
- Marks DI, Pagliuca A, Kibbler CC, et al. Voriconazole versus itraconazole for antifungal prophylaxis following
allogeneic haematopoietic stem-cell transplantation. Br J Haematol. 2011;155:318-327.
- Marr KA, Crippa F, Leisenring W, et al. Itraconazole versus fluconazole for prevention of fungal infections in
patients receiving allogeneic stem cell transplants. Blood. 2004;103:1527-1533.
- Marr KA, Schlamm HT, Herbrecht R, et al. Combination antifungal therapy for invasive aspergillosis: a randomized
trial. Ann Intern Med. 2015;162:81-89.
- Marr KA, Laverdiere M, Gugel A, Leisenring W. Antifungal therapy decreases sensitivity of the Aspergillus
galactomannan enzyme immunoassay. Clin Infect Dis. 2005;40:1762-1769.
- Mengoli C, Cruciani M, Barnes RA, Loeffler J, Donnelly JP. Use of PCR for diagnosis of invasive aspergillosis:
systematic review and meta-analysis. Lancet Infect Dis. 2009;9:89-96.
- Mennink-Kersten MASH, Donnelly JP, Verweij PE. Detection of circulating galactomannan for the diagnosis and
management of invasive aspergillosis. Lancet Infect Dis. 2004;4:349-357.
- Miceli HM, Maertens J. Role of non-culture-based tests, with an emphasis on galactomannan testing for the
diagnosis of invasive aspergillosis. Semin Respir Crit Care Med. 2015;36:650-661.
- Moon WJ, Scheller EL, Suneja A, et al. Plasma fluoride level as a predictor of voriconazole-induced periostitis in
patients with skeletal pain. Clin Infect Dis. 2014;59:1237-1245.
- Morrissey CO, Chen SC, Sorrell TC, et al; Australasian Leukaemia Lymphoma Group and the Australia and New
Zealand Mycology Interest Group. Galactomannan and PCR versus culture and histology for directing use of
antifungal treatment for invasive aspergillosis in high-risk haematology patients: a randomised controlled trial. Lancet Infect Dis. 2013;13:519-528.
- National Comprehensive Cancer Network. Prevention and Treatment of Cancer-Related Infections. NCCN
Guidelines Version 1.2016. Fort Washington, PA: National Comprehensive Cancer Network, Inc.; 2016.
- Neofytos D, Lu K, Hatfield-Seung A, et al. Epidemiology, outcomes, and risk factors of invasive fungal infections in
adult patients with acute myelogenous leukemia after induction chemotherapy. Diagn Microbiol Infect Dis.
2013;75:144-149.
- Noxafil prescribing information. Whitehouse Station, NJ: Merck; 2015.
- Obayashi T, Yoshida M, Mori T, et al. Plasma (1-->3)-beta-D-glucan measurement in diagnosis of invasive deep
mycosis and fungal febrile episodes. Lancet. 1995;345:17-20.
- Odabasi Z, Paetznick VL, Rodriguez JR, Chen E, McGinnis MR, Ostrosky-Zeichner L. Differences in beta-glucan levels
in culture supernatants of a variety of fungi. Med Mycol. 2006;44:267-272.
- Pagano L, Caira M, Candoni A, et al. The epidemiology of fungal infections in patients with hematologic
malignancies: the SEIFEM-2004 study. Haematologica. 2006;91:1068-1075.
- Pagano L, Caira M, Candoni A, et al. Invasive aspergillosis in patients with acute myeloid leukemia: a SEIFEM-2008
registry study. Haematologica. 2010;95:644-650.
- Pascual A, Csajka C, Buclin T, et al. Challenging recommended oral and intravenous voriconazole doses for
improved efficacy and safety: population pharmacokinetics-based analysis of adult patients with invasive fungal
infections. Clin Infect Dis. 2012;55:381-390.
- Perfect JR, Hachem R, Wingard JR. Update on epidemiology of and preventive strategies for invasive fungal
infections in cancer patients. Clin Infect Dis. 2014;59(suppl 5):S352-S355.
- Pfeiffer CD, Fine JP, Safdar N. Diagnosis of invasive aspergillosis using a galactomannan assay: a meta-analysis. Clin
Infect Dis. 2006;42:1417-1427.
- Pham AN, Bubalo JS, Lewis JS 2nd. Comparison of posaconazole serum concentrations from haematological cancer
patients on posaconazole tablet and oral suspension for treatment and prevention of invasive fungal infections. Mycoses. [Epub ahead of print]. 2016 Jan 6. doi: 10.1111/myc.12452.
- Pini P, Bettua C, Orsi CF, et al. Evaluation of serum (1 → 3)-β-D-glucan clinical performance: kinetic assessment,
comparison with galactomannan and evaluation of confounding factors. Infection. 2015 Oct 16. [Epub ahead of
print].
- Stynen D, Sarfati J, Goris A, et al. Rat monoclonal antibodies against Aspergillus galactomannan. Infect Immun.
1992;60:2237-2245.
- Sulahian A, Porcher R, Bergeron A, et al. Use and limits of (1-3)-β-d-glucan assay (Fungitell), compared to
galactomannan determination (Platelia Aspergillus), for diagnosis of invasive aspergillosis. J Clin Microbiol.
2014;52:2328-2333.
- Thornton CR. Development of an immunochromatographic lateral-flow device for rapid serodiagnosis of invasive
aspergillosis. Clin Vaccine Immunol. 2008;15:1095-1105.
- Ullmann A, Lipton JH, Vesole DH, et al. Posaconazole or fluconazole for prophylaxis in severe graft-versus-host
disease. N Engl J Med. 2007;356:335-347.
- Van Leeuwen RW, van Gelder T, Mathijssen RH, Jansman FG. Drug-drug interactions with tyrosine-kinase
inhibitors: a clinical perspective. Lancet Oncol. 2014;15:e315-e326.
- Vega K, Kalkum M. Chitin, chitinase responses, and invasive fungal infections. Int J Microbiol. 2012;2012:920459.
- Vermeulen E, Lagrou K, Verweij PE. Azole resistance in Aspergillus fumigatus: a growing public health concern. Curr
Opin Infect Dis. 2013;26:493-500.
- Vfend prescribing information. New York, NY: Pfizer; 2003.
- Walsh TJ, Anaissie EJ, Denning DW, et al; Infectious Diseases Society of America. Treatment of aspergillosis: clinical
practice guidelines of the Infectious Diseases Society of America. Clin Infect Dis. 2008;46:327-360.
- Walsh TJ, Finberg RW, Arndt C, et al. Liposomal amphotericin B for empirical therapy in patients with persistent
fever and neutropenia. National Institute of Allergy and Infectious Diseases Mycoses Study Group. N Engl J Med.
1999;340:764-771.
- Walsh TJ, Pappas P, Winston DJ, et al. Voriconazole compared with liposomal amphotericin B for empirical
antifungal therapy in patients with neutropenia and persistent fever. N Engl J Med. 2002;346:225-234.
- Walsh TJ, Teppler H, Donowitz GR, et al. Caspofungin versus liposomal amphotericin B for empirical antifungal
therapy in patients with persistent fever and neutropenia. N Engl J Med. 2004:351:1391-1402.
- Weissinger F, Auner HW, Bertz H, et al. Antimicrobial therapy of febrile complications after high-dose
chemotherapy and autologous hematopoietic stem cell transplantation—guidelines of the Infectious Diseases
Working Party (AGIHO) of the German Society of Hematology and Oncology (DGHO). Ann Hematol. 2012;91:1161-1174.
- White PL, Perry MD, Loeffler J, et al; European Aspergillus PCR Initiative. Critical stages of extracting DNA from Aspergillus fumigatus in whole-blood specimens. J Clin Microbiol. 2010;48:3753-3755.
- Williams K, Mansh M, Chin-Hong P, Singer J, Arron ST. Voriconazole-associated cutaneous malignancy: a literature
review on photocarcinogenesis in organ transplant recipients. Clin Infect Dis. 2014;58:997-1002.
- Wingard JR, Carter SL, Walsh TJ, et al; Blood and Marrow Transplant Clinical Trials Network. Randomized, double-blind trial of fluconazole versus voriconazole for prevention of invasive fungal infection after allogeneic
hematopoietic cell transplantation. Blood. 2010;116:5111-5118.
- Winston DJ, Maziarz RT, Chandrasekar PH, et al. Intravenous and oral itraconazole versus intravenous and oral
fluconazole for long-term antifungal prophylaxis in allogeneic hematopoietic stem-cell transplant recipients: a
multicenter, randomized trial. Ann Intern Med. 2003;138:705-713.
- Wojenski DH, Bartoo GT, Merten JA, et al. Voriconazole exposure and the risk of cutaneous squamous cell
carcinoma in allogeneic hematopoietic stem cell transplant patients. Transpl Infect Dis. 2015;17:250-258.
- Zonios DI, Gea-Banacloche J, Childs R, Bennett JE. Hallucinations during voriconazole therapy. Clin Infect Dis.
2008;47:e7-e10.
Back to Top